
Abstract
This study examined the use of complementary and medical treatments, both individually and in combination, to address common general and upper respiratory symptoms. Data for the analysis were collected from a series of 18 daily diary questionnaires administered to community-living older African American and white adults living in rural counties in North Carolina. Participants reported symptoms experienced on each diary day and the treatment strategies they used each day in response to the particular symptom(s). Older adults used diverse categories of strategies to treat symptoms; treatment strategies were used inconsistently across symptoms. Use of only complementary strategies, only medical conventional strategies, or both complementary and medical strategies to treat any one symptom rarely corresponded to the use of the same strategy to address other symptoms. Future research would benefit from analyzing how older adults use health care strategies across symptom categories.
Introduction
Our knowledge about the use of treatment strategies, including use of medicine, complementary therapies, medical office visits, and self-care strategies, among older adults has increased during the past few decades (Andersen, 2008; Arcury et al., 2011; Barnes, Bloom, & Nahin, 2008; Calnan, Wainwright, O’Neill, Winterbottom, & Watkins, 2005). However, research examining whether individuals use the same categories of treatment strategies when they experience different symptoms is limited. This omission restricts our ability to understand how older adults integrate multiple treatment strategies into their symptom management repertoire. This article focuses on the current use of treatment strategies among older adults to treat common general symptoms, such as fever or chills, headache, fatigue, and common upper respiratory symptoms, such as runny or stuffy nose, sore throat or hoarse voice, and cough. It compares the use of treatment strategies to respond to a set of general symptoms that affect multiple parts of the body and are unlikely to be associated with one illness, to the use of treatment strategies to respond to a specific system of the body.
A substantial body of research has examined a range of treatment strategies that individuals employ to address their health issues. Older adults consult physicians when they think that the symptom is serious, or it fails to respond effectively to self-care strategies (Arcury et al., 2011; Stoller, Forster, & Portugal, 1993). Over-the-counter medicine (OTC) and prescription medicine are both widely used by older adults to treat their symptoms and conditions (Fry et al., 2007; Kaufman, Kelly, Rosenberg, Anderson, & Mitchell, 2002; Patterns of Medication Use in the United States, 2006; Qato et al., 2008; Rolita & Friedman, 2008; Sleath, Rubin, Campbell, Gwyther, & Clark, 2001). Older adults use home remedies, including the ingestion of food and beverages, and herbal supplements, strategies that are considered complementary when used alongside conventional care, to address health concerns (Arcury et al., 2011; Barnes et al., 2008; Eisenberg et al., 1993; Kaufman et al., 2002; Najm, Reinsch, Hoehler, & Tobis, 2003; Ryder, Wolpert, Orwig, Carter-Pokras, & Black, 2008; Shippee, Schafer, & Ferraro, 2012). They also engage in passive strategies, such as reducing activity or resting or waiting to see how symptoms progress (Arcury et al., 2011; Musil et al., 1998; Stoller et al., 1993)
Some researchers have examined treatment strategies that adults draw upon to treat specific symptoms or health conditions. Calnan et al. (2005), for example, analyzed how adults with upper-limb disorders made decisions about how to treat or manage pain with medication, activity modification, and consultation with physicians and complementary medicine providers. Quandt et al. (2012) reported on strategies used by older adults to manage arthritis. Another research team analyzed older adults’ use of several strategies, including calling upon medical professionals, taking OTC or prescription medication, and engaging in self-care, for each of 20 health problems (Musil et al., 1998). Stoller and colleagues (1993) provided detailed analysis of the self-management strategies of older adults who experienced specific symptoms. Together, these studies provide evidence that adults draw upon multiple and diverse strategies to manage particular symptoms.
Understanding how adults combine conventional and complementary treatment strategies to address common ailments remains limited despite substantial inquiry into older adults’ health self-management. This analysis examines patterns of use of both upper respiratory symptoms and general symptoms. Inclusion of upper respiratory symptoms in the analysis enables us to examine whether older adults use similar treatment strategies for symptoms that affect one specific system of the body; however, upper respiratory symptoms could be associated with more than one illness on any one day or over a series of days. Colds, allergies, and asthma can result in multiple overlapping upper-respiratory symptoms. The general symptoms of fever and chills, headache, and fatigue are not confined to one region of the body. Inclusion of general symptoms in this analysis enables us to analyze whether older adults generally use similar strategies to treat disparate symptoms experienced in different regions of the body. Other common symptoms that are experienced across the lifespan and would also be appropriate to examine. We are, however, restricting this analysis to general and upper respiratory symptoms.
Leventhal’s self-regulatory model of illness provides a theoretical framework to understand strategies drawn upon by individuals to treat health symptoms (Cameron & Leventhal, 2003; Leventhal, Weinman, Leventhal, & Phillips, 2008). It recognizes that individuals have had previous experiences with illnesses. They draw upon the knowledge they gained from those experiences, through interactions with others, and from other lay and expert health information resources. Leventhal’s model emphasizes the subjective component of individuals’ symptoms and brings individuals’ problem-solving skills to the forefront. Adults interpret the symptoms in the context of their personal understandings of health and illness. The self-regulatory model of illness behavior assumes that individuals may respond to any one symptom in diverse ways, depending on their interpretation of the significance of the symptom, and that individuals may draw upon a range of responses. Beliefs that individuals have about the illness that they associate with a symptom, beliefs about the trajectory of illness signified by the symptom, and the beliefs about the potential effectiveness of specific interventions on the progression of the perceived illness all influence older adults’ responses to symptoms. Future responses to symptoms and illnesses may be influenced by perceived effectiveness of current and past treatments (Cameron & Leventhal, 2003; Leventhal et al., 2008). This model leads us to expect that individuals may not necessarily use consistent strategies to treat the same symptoms at different times and are likely to use inconsistent strategies to treat diverse symptoms at different times.
This study examines conventional medical and complementary strategies employed by older adults in rural North Carolina to treat general and upper respiratory symptoms. It addresses how individuals use diverse strategies, both individually and in combination with other strategies, to address multiple common symptoms. This study identifies the percentage of older adults who reported using each of seven strategies: home remedies, herbs, and supplements; food or beverages; OTCs; prescribed medicine and doctor visits; nonprescribed medicine; ignoring symptoms or waiting; resting or reducing activities in response to general and upper respiratory symptoms. It also determines the percentage of older adults who reported using four categories of treatment strategies: only complementary treatments, only conventional medical strategies, complementary and conventional medical strategies, and only passive responses for distinct general and upper respiratory symptoms. Finally, it indicates the consistency of categories of treatments across symptoms among older adults who reported multiple general or upper respiratory symptoms.
Method
Overview
Data used for this analysis were drawn from a series of 18 daily diary questionnaires that examined complementary care, self-care, and medical care for treatment of specific symptoms reported by participants. Older adults living in three rural counties in south-central North Carolina participated in this study. The daily diary studies were fielded on three consecutive days at 1-month intervals over a period of 6 months. All procedures were approved by the Wake Forest School of Medicine, Institutional Review Board (IRB), and participants gave signed informed consent (Arcury et al., 2011).
Sample
The community-dwelling older adults who participated in this study were aged 64 and older, self-identified as African American or white, and were English speaking. The sample was stratified by ethnicity and gender and included approximately 50 older adults in each ethnicity-gender combination. A site-based strategy was used to recruit representative participants (Arcury & Quandt, 1999). The 34 recruitment sites included, but were not restricted to, county social service departments, senior centers, social clubs, churches, and businesses.
One-hundred and ninety-five African American and white older adults completed one or more daily diary studies, and of those, 181 reported one or more symptoms relevant to our research questions and are included in this analysis. More than 70% (131) completed 6 sets of daily diary studies, 21 completed 5 sets, 5 completed 4 sets, 5 completed 3 sets, 10 completed 2 sets, and 9 completed one set.
Data Collection
Trained interviewers completed data collection of the daily diary studies April 2008 through January 2010. Most interviews were conducted by telephone. Older adults who were unable to speak by telephone or preferred not to communicate by telephone were interviewed in person. Participants were asked whether they had experienced a list of specific symptoms during the past 24 hours. For each symptom reported, participants were asked what action, if any, they had taken in response to the symptom.
Measures
Participants reported actions they had taken in response to seven general symptoms (fever or chills, headache, weakness, feeling tired) and upper respiratory symptoms (runny nose or stuffiness, sore throat or hoarse voice, and cough). For each specific symptom reported, participants were asked whether they had addressed that symptom through use of any of the following strategies: ate or drank something to feel better; used some other type of home remedy; took an herb or supplement; took an OTC medicine; took a medicine prescribed by a doctor for the symptom; took another type of prescription medicine; visited a medical doctor; stayed in bed or rest; cut back on usual activities; or ignored the symptoms or decided to wait and see. Types of treatments were combined to create more general categories to allow for analysis of patterns of management strategies across symptoms, and two treatment categories were collapsed. Complementary therapies in this analysis refer to use of home remedies, herbs and supplements, and use of food or beverages to treat a specific symptom. The medical treatment category includes office visits with physicians, use of prescribed medicine, whether or not it was prescribed for the symptom reported, and use of OTCs. Although OTCs may be purchased without a prescription from a health care professional, many commonly used OTCs, such as aspirin, ibuprofin, and loratadine are an integral part of physician-supported treatment plans and are consistent with conventional treatment plans (Pratter, 2006; Sur & Scandale, 2010). In addition, many adults think that OTCs have been approved by regulatory bodies to treat conditions for which they are advertised and therefore perceive them as risk free (Fry et al., 2007). Older adults who took a “mixed-use” strategy used both complementary therapies and medical treatments to address a particular symptom. Older adults who used one strategy (e.g., only conventional medical strategies) to treat one symptom, such as headache, and used another strategy, (e.g., only complementary therapies) to treat fatigue, were categorized as having inconsistent use of complementary and medical strategies in the context of treating headaches and fatigue. Passive treatments consist of ignoring the symptom or waiting, resting, or reducing activities. Experiencing a specific symptom, yet not engaging in complementary therapy, medical treatment, or passive treatment, represents a nonresponse strategy. Personal characteristics recorded include gender, race and ethnicity (African American and white), age (64-74, 75+), and formal education (any education beyond high school or not), income, and marital status.
Analysis
All calculations were performed using SAS v9.2 (SAS Institute, Cary, NC). Characteristics of participants who experienced at least one general or upper respiratory symptom, as well as treatment used and treatment typology for each symptom, were summarized using counts and percentages. Symptom prevalence and treatment use were aggregated from all 18 daily questionnaires.
Results
Descriptive Analysis
A total of 181 older adults reported that they had experienced one or more upper respiratory or general symptoms on one or more diary days and are included in this analysis. Slightly less than half were male (Table 1). Forty-six percent of the older participants were African American; the remaining older adults were white. Sixty percent were aged 64 to 74, and 40% were aged 75 and older. Approximately half of the participants had education beyond high school. Seventy-two percent had a household income above US $13,700 and 41% were married.
Participant Characteristics of Rural Older Adults, North Carolina.
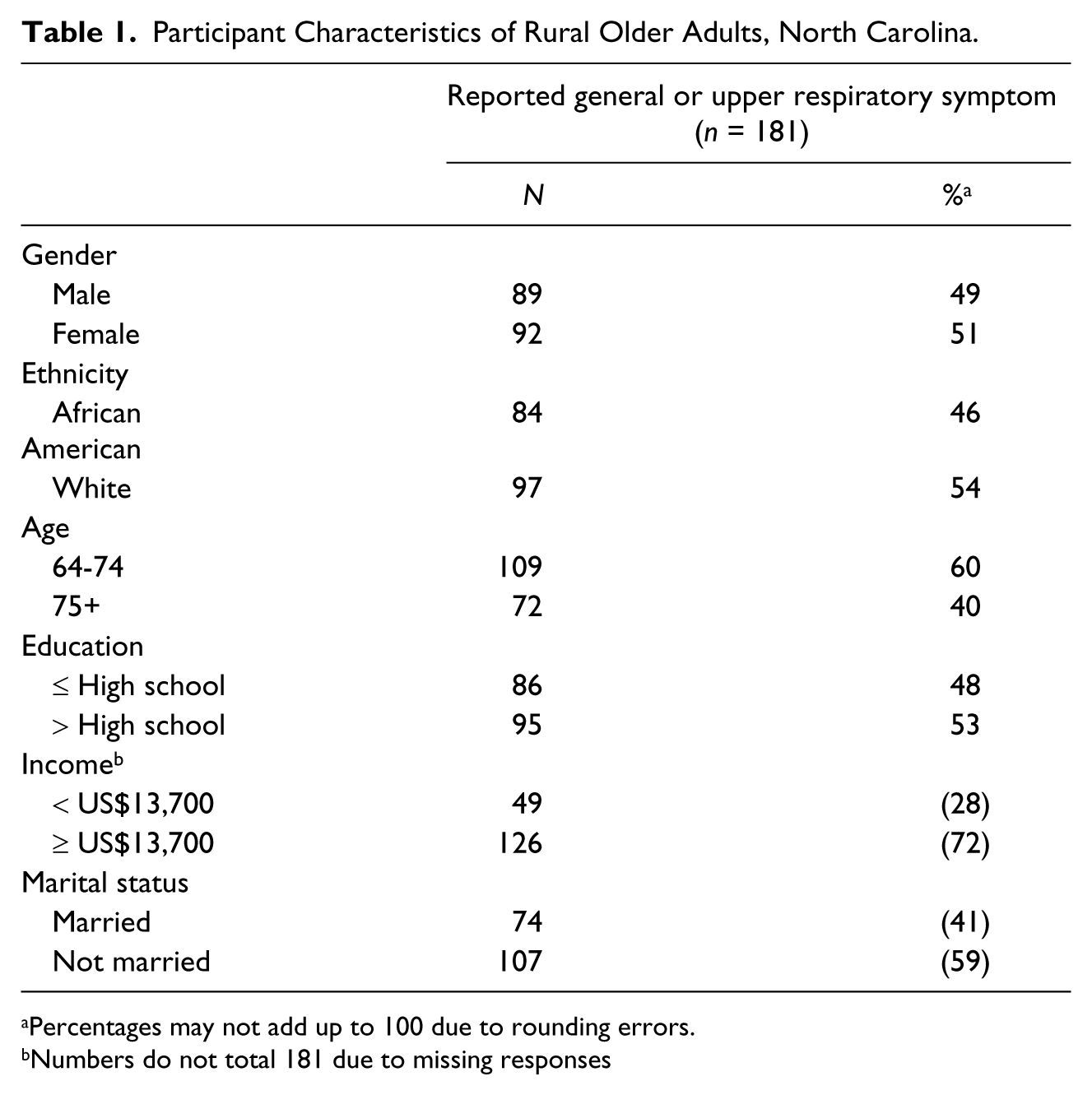
Percentages may not add up to 100 due to rounding errors.
Numbers do not total 181 due to missing responses
Prevalence of Symptoms
The number of older adults who reported they had experienced a general symptom or upper respiratory symptom on one or more days varied substantially by symptom (Table 2). Only 19 participants reported fever or chills on any of the daily diary study days; this analysis therefore gives limited attention to treatment strategy for fever. Ninety-three reported a headache on at least one day. One-hundred and forty older adults experienced fatigue (weakness or tiredness). A runny or stuffy nose, sore throat or hoarse voice, and cough were reported by 128, 60, and 110 older adults, respectively.
Treatment Use Among Participants Who Experienced General or Upper Respiratory Symptoms ≥ 1 Diary Days.

Percentages may not add up to 100 due to rounding errors.
Use of Specific Therapies to Treat General and Upper Respiratory Symptoms
Type of therapy used on at least one diary day varied by symptom experienced (Table 2). Taking an OTC (80%) and resting or reducing activities (68%) were the most common strategies reported to address headache symptoms. Food and beverage (22%), prescribed medicine and doctor’s visits (25%), nonprescribed medicine (20%), and ignoring the symptom or waiting (37%) were used occasionally in response to a headache. Home remedies, herbs, and supplements were rarely used (2%). Among those who had experienced fatigue, a majority reported that they had ignored a symptom or waited to see how the symptom would progress (74%) or rested or reduced their activities (92%); slightly fewer than half had ingested food or beverage (46%) to treat the symptom. Home remedy, herb, and supplement use (14%), OTC use (19%), and taking prescription medicine or visiting a doctor (21%) were less frequently used. Six percent of the older adults took nonprescribed medicine to treat symptoms of fatigue.
Strategies used by older adults to treat upper respiratory symptoms varied widely. The most commonly reported strategies to treat a runny or stuffy nose were to ignore the symptom or wait to see how the symptom progressed (74%) and to use an OTC (61%). Some older adults consumed food or beverages (20%), took prescribed medicine or visited a doctor (27%), or rested or reduced their activities (35%). Few older adults used home remedies, herbs, or supplements (7%) or nonprescribed medicines (9%) to treat a runny or stuffy nose.
More than half of older adults who experienced a sore throat or hoarse voice took an OTC (57%) or ignored the symptom or waited (55%) on one or more daily diary days on which they reported the symptom. Some older adults used a home remedy, herb, or supplement (25%), consumed food or beverages (40%), or rested or reduced their activities (23%) in response to a sore throat. Few took a prescribed medicine or visited a doctor (8%) or took nonprescribed medicine (8%) to treat the symptom.
The majority of older adults who reported a cough took an OTC (63%) or ignored the symptom (70%) on one or more diary days on which they experienced the symptom. Some older adults consumed a food or beverage (30%), took a prescribed medicine or visited a doctor (25%), or rested or reduced their activities (27%) in response to the symptom. Few used home remedies, herbs, or supplements (8%) or took a nonprescribed medicine (6%) to treat a cough on one or more days on which they reported a cough.
Use of Categories of Therapies to Treat General and Upper Respiratory Symptoms
A different perspective of older adults’ care strategies emerges when therapy strategies are broadly categorized (Table 3). A substantial majority (69%) reported that they had used conventional medical strategies on one or more days that they experienced a headache but did not use complementary strategies on any of those days. Twenty percent reported that they had used complementary and conventional medical treatments on at least one day they experienced a headache, although not necessarily on the same day. Very few (2%) stated that they had used complementary strategies and avoided medical strategies to treat their headaches. Eight percent used only passive measures on days that they experienced a headache, and 1% reported none of those responses.
Distribution of Combination of Strategies by Symptom.

Percentages may not add up to 100 due to rounding errors.
Among older adults who reported that they experienced fatigue on one or more diary days, 25% reported that they had used only complementary therapy on one or more days. Twenty-six percent reported that they had used both complementary therapy and medical treatment in response to fatigue; 9% reported that they had used a medical strategy but not a complementary strategy. Forty percent reported only passive responses, and 1% reported no response.
Older adults used different combinations of treatment categories in response to three upper respiratory symptoms. Among those who experienced a runny or stuffy nose on one or more diary days, almost half (49%) indicated that they had used a medical strategy, but not a complementary strategy, on any of the diary days. Among older adults who had runny or stuffy noses, 3% had used only complementary therapies to treat their symptom. Twenty-one percent used both complementary treatment and medical strategies on one or more days during which they experienced the symptom, although not necessarily on the same day. Twenty-six percent reported only passive responses, and 1% did not indicate any response to the symptom.
The most common strategy used by older adults who experienced a sore throat was to combine complementary and medical strategies (38%), although not necessarily on the same day. Twenty-two percent used only medical strategies to treat their sore throat, and 10% restricted treatment to complementary therapies. One quarter used only passive responses, and 5% did not indicate that they used any of the above strategies in response to a sore throat.
Half of the older adults who experienced a cough reported that they used medical strategies for at least 1 day on which they experienced the symptom while forgoing use of complementary therapies on any of those days. Five percent reported that they had used complementary therapy on at least 1 day they experienced a cough but did not use any medical strategies. Twenty-six percent used both complementary and medical strategies. Nineteen percent reported only a passive response to the cough; 1% did not report any of the strategies analyzed.
Lack of Consistency of Typology Across Symptoms
Participants may use one or multiple strategies in response to sets of particular symptoms. One older adult used complementary therapy but not medically based treatment, for both his headache and fatigue (Table 4). Four percent of older adults relied exclusively on medical strategies on one or more days that they experienced headaches or fatigue. Ten percent reported using both complementary therapy and medical approaches to treat both their headache and fatigue, although not necessarily the same day. Seventy-nine percent of older adults who reported a headache and fatigue on at least 1 diary day, although not necessarily on the same day, used complementary and conventional medical strategies inconsistently across general symptoms. Five percent reported only passive responses to general symptoms.
Consistency of Typology Across Symptoms.
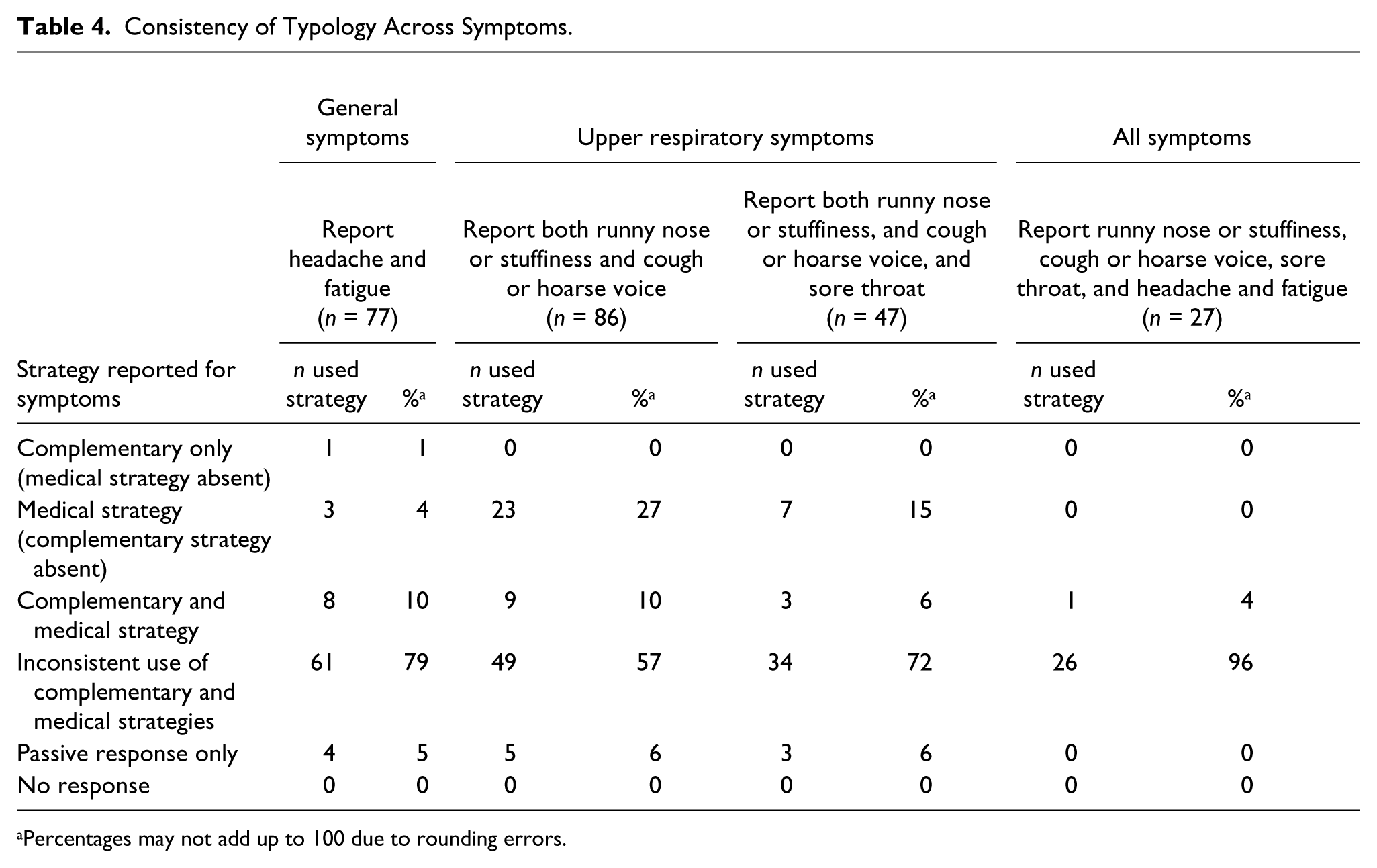
Percentages may not add up to 100 due to rounding errors.
Eighty-six older adults indicated that they had experienced both a runny nose and cough on 1 or more diary days, although not necessarily on the same day. None reported that they had used complementary therapy, but no medical treatment, on 1 or more diary days. Twenty-seven percent, however, indicated that they had used medically based treatments on at least 1 day they experienced each symptom yet had not used complementary therapies on any days they had experienced a runny nose or cough. The majority (57%) of older adults who experienced both symptoms on 1 or more days were inconsistent in their use of complementary and alternative approaches to responding to the two different symptoms. Six percent of the older adults responded to both symptoms solely by resting or reducing their activities.
No older adults used complementary therapy to treat each of the three respiratory symptoms while refraining from using a medical approach to treat any of those three symptoms. Only 15% of older adults drew upon a medical approach for each of the three symptoms while forgoing complementary therapy to treat any of those symptoms. Only 6% used complementary therapy and medically based treatment for each of the three upper respiratory symptoms. Seventy-two percent were inconsistent in their use of complementary and conventional medical strategies to treat three upper respiratory symptoms. Six percent engaged solely in passive responses.
The lack of consistency in treatment type became more apparent when all symptoms were included in the analysis. Of the 27 older adults who reported that they had experienced all three upper respiratory symptoms, headache, and fatigue on 1 or more diary days (not necessarily the same day), 96% drew upon inconsistent use of complementary and conventional medical strategies across symptoms. The remaining older adults used both complementary therapy and one or more medical approaches to treat each of the five symptoms.
Discussion
General and upper respiratory symptoms are experienced over an individual’s life course, providing older adults with substantial opportunities to identify and use multiple strategies to treat those ailments. Each of seven distinct therapies addressed in this analysis was used by at least 20% of the older adults in response to one or more general or upper respiratory symptoms they experienced on a daily diary day. The most commonly used treatment strategy used by older adults varied by symptom. With the exception of fatigue, OTCs were used by at least 50% of older adults reporting each symptom. No other distinct therapy was used by more than 50% of participants for six of the seven categories. The highest percentage of use of complementary strategies, but not medical strategies, was reported among those who had experienced fatigue. Older adults who had reported a headache were most likely to report that they had used a medical strategy, but not a complementary strategy, to treat the symptom. The greatest percentage of use of both complementary and medical strategies was reported among those who had sore throats. Older adults who had experienced fatigue were more likely than those who had reported other symptoms to respond passively. These findings suggest that the treatment strategy used should be examined in the context of specific symptoms and not simply whether individuals use particular treatment strategies.
Older adults who reported multiple general or upper respiratory symptoms used treatment strategies inconsistently across symptoms. Use of only complementary strategies, only medical strategies, or a combination of complementary and medical strategies to treat any one particular symptom did not appear to correspond to use of the same strategy to address other symptoms. Older adults who combined complementary and medical treatments to address one general or upper respiratory symptom were likely to draw upon treatments from a different category when responding to another symptom.
Older adults draw upon multiple treatments to address a diverse range of common symptoms. This is consistent with other research on this population (Calnan et al., 2005; Foster, Phillips, Hamel, & Eisenberg, 2000; Musil et al., 1998; Sleath, Cahoon, Sloane, & Callahan, 2008). Older adults do not necessarily assume that conventional medical and complementary strategies are in opposition to each other; they may complement each other (Arcury, Bernard, Jordan, & Cook, 1996). The range of strategies for any one symptom may also reflect variation in knowledge about different treatment strategies that may minimize the symptom and variation in the effectiveness of the different strategies, as perceived by older adults who had used that strategies previously (Arcury et al., 2011; Prior, Evans, & Prout, 2011).
Strategies that older adults implemented to treat one symptom were often not implemented to treat other symptoms. Variation in use of treatment strategies to address specific symptoms may relate to interpretations placed on the older adult’s perception of the cause of symptoms, such as colds, allergies, or asthma, in the case of upper respiratory symptoms (Kleinman, Eisenberg, & Good, 1978; Musil et al., 1998; Verbrugge & Ascione, 1987). The analysis did not examine whether different symptoms were present on the same day or the order in which symptoms appeared. The presence or absence of other general and upper respiratory symptoms and, among symptoms experienced on the same diary day, the order in which the symptoms first appeared may influence the older adults’ lay diagnoses and their evaluation of appropriate treatments. Furthermore, individuals may interpret symptoms as evidence of a particular illness or as a condition not associated with any illness (Musil et al., 1998). Finally, older adults may perceive that one treatment strategy may not adequately address all their symptoms when they intuit that one condition or illness causes multiple symptoms.
Older adults have had decades of experiences with and responses to symptoms and illnesses. They have multiple resources they may draw upon to identify symptoms and illnesses, associate symptoms with specific illnesses, and determine appropriate treatment strategies. These resources include information provided from family members and friends over their life span, recollections of personal experience, knowledge developed through interactions with conventional health care professionals, and information gleaned from articles and accounts about symptoms and diseases, including conventional and alternative perspectives, in popular media (Cavender & Beck, 1995; Mathews, 1987). Furthermore, intensive advertising campaigns for OTCs marketed to relieve upper respiratory symptoms and widespread availability of those OTCs may contribute to the widespread use of OTCs for their symptoms.
The findings are consistent with Leventhal’s self-regulatory model of illness and self-care literature (Cameron & Leventhal, 2003; Haug, Wykle, & Namazi, 1989; Stoller et al., 1993). The model recognizes that individuals’ responses to symptoms are complex and rely on subjective interpretations that may or may not correspond to diagnoses made by physicians. Treatment strategies may be influenced by individuals’ perceptions of illness. Furthermore, individuals bring problem-solving skills that they have developed over a lifetime, including knowledge that they have gained from interacting with other people, textual sources, as well as through their own experience using treatments, alone or in combination with others, to address symptoms and illnesses (Cameron & Leventhal, 2003; Leventhal et al., 2008; Stoller et al., 1993). Although the results are consistent with Leventhal’s model, other models may also be used to effectively to explain older adults’ use of treatment strategies (Andersen, 1995; Kleinman et al., 1978).
The study results may have implications for older adults’ management of chronic disease. Older adults often report that they use inconsistent strategies to address symptoms that are commonly related to each other, such as a runny nose and cough. These findings suggest that older adults with chronic disease may use different types of strategies to address different disease-related symptoms. Health care providers should not assume, based on the patients’ account of how they manage one symptom, that they will use comparable strategies to treat other symptoms associated with chronic disease.
The distinction between medical and complementary therapy is sometimes less clear than implied in this analysis. Physicians may, for example, recommend that patients gargle with salt water when they experience mild sore throats (The Flu: Caring for Someone Sick at Home, 2010) or use a neti pot (Sur & Scandale, 2010) to reduce exposure to allergens in nasal passages. These treatment strategies would be identified as home remedies in this study, although their use may be recommended and encouraged by physicians. Furthermore, older adults may take OTCs in doses or for reasons that are not encouraged by health care professionals (Qato et al., 2008). “Medical” strategies used by some older adults are considered inappropriate by conventional health care providers while some “complementary” strategies are endorsed by conventional medical providers.
Our analysis emphasizes reported symptoms. The data collected do not enable us to determine whether the participants attributed runny noses to colds or allergies or both or whether the attributions changed over time or by presence or absence of other symptoms. Nor do the data enable us to determine whether the older adults ascribed their symptoms to diseases that would be recognizable to conventional practitioners. Finally, our analysis does not examine the effect of perceived symptom severity on treatment used. The results do, however, focus our attention to the variation in use of treatments strategies by individuals across symptoms. Future studies would benefit from analyzing how self-perceptions of illness and symptom severity and physicians’ diagnoses affect the use of treatment strategies by older adults.
There are limitations to this study. Older adults were recruited from rural areas in three counties in North Carolina; therefore, generalizations to populations in urban settings or other regions of the United States should be made with caution. Although a random sampling frame was not used, by recruiting participants at 34 locations and limiting the number of participants selected from any one site, and recruiting similar numbers of men and women, African American and white older adults, the sample population includes substantial variation. This approach improved the variation across our sample; however, the sample size does not allow us to analyze the pattern of treatment strategies across symptoms by ethnicity and gender.
The results from this analysis redirects the focus from whether individuals use a particular type of treatment to respond to symptoms to combinations of strategies that individuals employ both for specific symptoms and across symptoms. The findings suggest that research that focuses on whether patients with particular characteristics are more or less likely than others to use complementary or conventional care strategies may not adequately capture how older adults respond to common symptoms. Older adults draw upon diverse categories of strategies to treat symptoms; these strategies are frequently inconsistent across symptom category. Future research would benefit by analyzing how older adults use health care strategies across symptom categories.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors declared the receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from the National Center for Complementary and Alternative Medicine, R01 AT003635.