
Abstract
This convergent mixed methods study examined 35 healthy, independent living individuals’ (above 85 years) perceptions of their relationship with their primary health provider (PHP) and health practices. The relationship between PHP relationship perceptions and locus of control (LOC), resilience, and self-efficacy was explored through surveys and interviews. The majority indicated they visited their PHP just for preventative care; the number of PHP visits per year was significantly lower than reported for individuals above 85 by the CDC, possible reasons for this finding are provided. A positive relationship between LOC, resiliency, and self-efficacy for the oldest old was found. Few participants indicated their PHP had discussed normal changes with aging. This study has deepened understanding of the complexity inherent to the healthy oldest olds’ relationship with their PHP. The findings suggest this relationship relates to the PHP’s personal characteristics, the older adult patients’ personality, and the influence of the accompanying patient escort.
The 2000 U.S. Census (2001) reported 4.2 million people were above the age of 85 (1.5% of the population); this group has been designated the “the oldest old” by demographers and is the most rapidly growing age group. Currently the cost of health service utilization for the oldest old averages US$22,000 per year compared to US$9,000 for individuals 65 to 74 years old (Krause, 2010). It would be logical to assume individuals on the less healthy side of the spectrum, who require nursing care or are in facilities (21.9% of this age group; Gist & Hetzel, 2004), bias this US$22,000 mean. However, little is known about the oldest old who are on the healthy end of the continuum. How do these individuals interact with their Primary Health Provider (PHP) and how do their personalities affect the interaction? Participants in the current study, while primarily seeing physicians, also mentioned physician assistants and nurse practitioners; thus, the more generic term, Primary Health Provider is used.
The patient-by-treatment-context interactive model of Christensen and Johnson (2002) provides the framework for the study. The model proposes that the relationship between patient characteristics (e.g., personality and beliefs) and patient adherence (e.g., preventative care) is moderated by the treatment context (e.g., PHP characteristics and behavior). The model has been successfully applied to specific illnesses; for example, renal insufficiency and hemodialysis (Christensen, Moran, & Ehlers, 1999) and cardiac rehabilitation (Christensen et al., 1999). It does not appear to have been previously applied in the present context of ongoing preventative care in older adults. The patient (LOC, resilience, self-efficacy, beliefs, and behavior) and treatment (PHP characteristics, health behaviors) variables in the current study were derived from the literature and are consistent with this model.
The current mixed methods study attempts to clarify PHP interactions and patient personality characteristics through surveys and interviews examining how independent living oldest old perceive their relationships with their PHP and how this affects their health care.
Oldest Old and Physicians
The relationship between the physician and patient is unique; in a medical encounter, often involving the meeting of two strangers, the patient reveals very personal topics and an examination of the patient’s body occurs (Adelman, Greene, & Ory, 2000). How PHPs handle such encounters can mean the difference between a patient following suggested medical advice or disregarding it (Adelman et al., 2000).
When considering the oldest old, one relevant issue is the frequency of physician or PHP visit. M. Parks (The Centers for Disease Control, [CDC], Division of Heath Care Statistics, personal communication, June 11, 2012), supplied the information shown in Table 1.
Office Visits by Patient Age: United States, 2009.
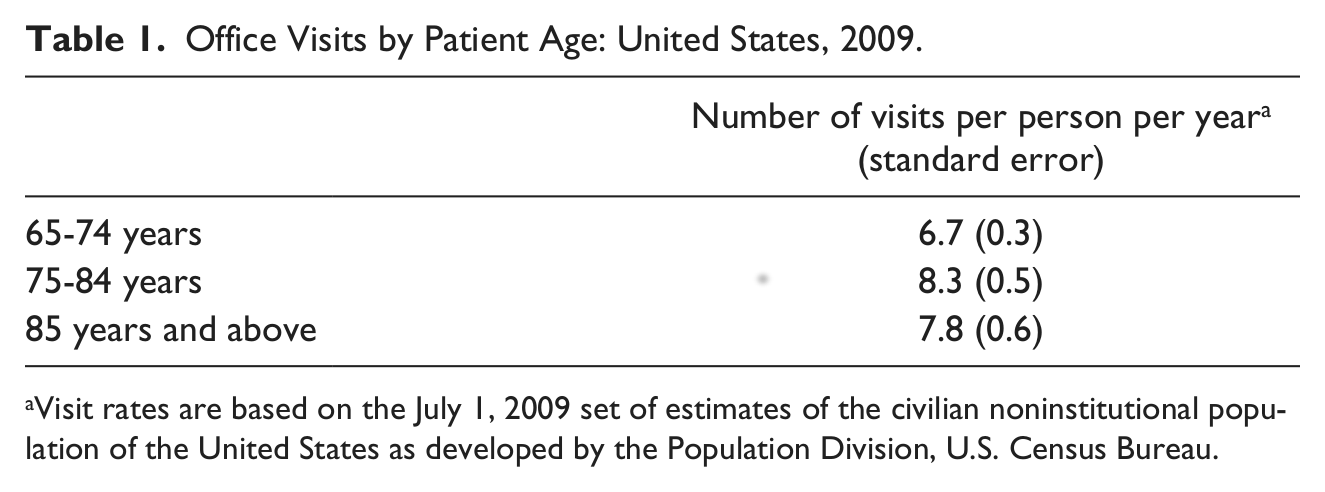
Visit rates are based on the July 1, 2009 set of estimates of the civilian noninstitutional population of the United States as developed by the Population Division, U.S. Census Bureau.
It is apparent that the oldest old have fewer PHP visits than individuals who are younger. These trends are similar to Wolinsky, Mosely, and Coe’s (1986; Wolinsky, Arnold, & Nallapati, 1988) who reported the oldest old in their sample had fewer physician visits than did younger individuals. Wolinsky et al. (1988) speculated the decline in physician visits might be due to a general decline in mobility, making accessing health care more difficult. This is a reasonable assumption for the least healthy individuals, but it is not clear if this assumption holds for the more healthy members of this age group.
Patient Satisfaction and the Older Adults
There is a large literature on general patient satisfaction (Hertz, 2012; Lee & Kasper, 1998; Sherbourne, Hays, Ordway, DiMatteo, & Kravitz, 1992). Patient satisfaction is an indicator of quality of care, however, such studies tend to be surveys with little opportunity for the participant to go beyond the questions and answers listed.
Kong, Camacho, Felman, Anderson, and Balrishnan (2007) reported those above 65 had higher physician satisfaction scores and were less concerned with waiting times than were the younger adults. Lee and Kasper (1998) found relative to 65 to 69 year olds, people 80 to 84 were 20% to 30% less likely to be highly satisfied with their quality of care and physician quality. The older patients objected to the physician’s lack of technical skills and interpersonal manner. However, Lee and Kasper (1998) relied on archival data and were not able to ask follow-up questions of their participants. The sample was limited to people below the age of 85, not the oldest old. In addition, medical schools have made a recent effort to train physicians in geriatric care (Croasdale, 2008; Siegler & Capello, 2005), which may affect the current older adults’ opinions of their PHP.
The present study examined a sample of independently living oldest old from across the United States using a mixed research method. This method allowed participants to express their opinions of and satisfaction with their PHP and permitted follow-up questions, which may clarify the reasons the oldest old may be satisfied or dissatisfied with their physicians. There is a lack of research examining certain oldest olds’ individual characteristics that are known to be associated with health care and health providers. Thus the current study also examined the relationship between Locus of Control (LOC), resilience, and self-efficacy to participants’ opinions of their PHP.
LOC
LOC is derived from Rotter’s (1966) social learning theory. Rotter hypothesized people who view reinforcements as contingent on their own behavior (internals) are better adjusted than those who see reinforcements as determined by fate, chance, or powerful others (externals). The three subscales within the LOC measure are internal control, powerful others, and chance (Levenson, 1973; Rotter, 1966).
Rennemark, Holst, Fagerstrom, and Halling (2009) found a negative correlation between physician visits and functional ability, education level, and internal LOC. High scores on the powerful others and chance subscales are predictors of patients’ trust in their physician (Brincks, Feaster, Burns, & Mitrani, 2010). High internal LOC scores also tend to be correlated with being proactive in seeking information, making health modifications, and treatment adherence (Macaden & Clarke, 2010).
Resilience
Resilience moderates the negative effects of stress and promotes adaptation (Wagnild, 2009; Wagnild & Young, 1993), and is described as an enduring personality characteristic (Foster, 1997). Nygren et al. (2005) suggested that the development of resilience constitutes a form of compensation for losses of functional capacity and physical health. Leppert, Gunzelmann, Schumacher, Strauss, and Brahler (2005) reported that higher scores on the resilience scale correlated with lower rates of subjective complaints and has been associated with health-promoting behaviors (Wagnild, 2009). Higher resilience has been found to be correlated with higher self-efficacy (Caltabiano & Caltabiano, 2006); it has also been found to be correlated with LOC in women with traumatic experiences (Friedman, 2009), but this relationship has not been previously examined using the Wagnild and Young scale in the oldest old.
Self-Efficacy
Self-efficacy is defined as people’s beliefs in their own abilities to manage upcoming situations and unexpected events (Bandura, 1986; Bandura, Barbaranelli, Caprara, & Pastorelli, 1996). Bandura (1986, 1993) suggests self-efficacy beliefs regulate an individual’s ability to deal with stress and anxiety when faced with unexpected and stressful events. Previous research has reported self-efficacy (Schwarzer & Jerusalem, 1995) correlates with LOC (Rotter, 1966). A recent study by Halisch and Geppert (2012) reported a similar finding in an older adult population; however, the percentage of oldest old in their sample was limited. The present study will confirm whether the finding is evident in the current oldest old sample.
Clayman et al. (2010) noted self-efficacy influences the older patient’s ability to act on information disseminated during a physician visit as well as confidence in asking questions of the doctor. Individuals with higher self-efficacy are more likely to benefit from health education interventions (Kostka & Jachimowicz, 2010), as they are able to perceive and apply the important information. The present mixed method study will examine the interrelationships between LOC, resilience, self-efficacy, and opinions of the oldest old about their PHP.
Design and Method
Design of the Study
The study used a convergent mixed method design (Creswell & Plano-Clark, 2011) in which the same participants were asked quantitative questions and interviewed. Parallel data collection was used in which the same concepts were used in the demographic questionnaire (detailed below) and in the interview. This design allowed the two data sets to be directly compared. The demographic questions were asked first, followed by the interview.
There were four primary research questions for the study. (a) How do the oldest describe their relationship with their PHP relative to their reported health practices? (b) How do scores on the personality measures self-efficacy, resiliency, and LOC interact with PHP relationship descriptions and reported health practices? (c) Schwarzer and Jerusalem (1995) and Halisch and Geppert (2012) reported that self-efficacy correlates with LOC in younger older adults. Does this relationship continue into the oldest old age group? (d) The CDC reported that for people above the age of 85 there is an average of 7.8 (SE = 0.6) yearly physician visits, which is less than for individuals between 75 and 84 years. In the current study with a healthy sample of oldest old, there are at least three possible outcomes. First, the healthy sample could show more visits than the CDC’s statistics, the argument could then be made that it is because of the higher rate of visits and presumably more preventative care leading them to be healthier than their peers. Alternatively, there could be no difference between the present sample and the CDC’s statistics, which would suggest that these individuals are within the normal expected range of PHP visits. Finally, a lower number of visits suggests that these individuals may be healthier, in general, and perhaps are only visiting the PHP for preventative care.
From the perspective of the patient-by-treatment-context interactive model of Christensen and Johnson (2002), adherence (preventative care) is expected to be best when the patient’s characteristics (personality and beliefs) are consistent with the treatment context (PHP characteristics and behavior; Christensen, 2004). Thus, in the current study, there should be consistent preventative care (adherence) when the patient has higher internal LOC (being proactive in health), higher resilience (inner strength and optimism, health-promoting behaviors), and higher self-efficacy (more likely to seek information and self-confidence) and to indicate that they like or feel comfortable with their PHP (treatment). In addition, it would be expected that there would be less preventative care (lack of adherence) when the patient has lower internal LOC (i.e., external; not proactive in health), higher powerful others, and chance scores (increased trust in PHP). Other expectations include lower resilience (higher level of subjective complaints, fewer health-promoting activities), lower self-efficacy (less likely to apply health interventions [preventative care] and less self-confidence), and to indicate that they do not like or feel comfortable with their PHP (treatment).
A modified collaborative research method (Knight, Roosa, & Umaña-Taylor, 2009) was used as the recruitment strategy. This method is commonly used to recruit hard to reach populations (Knight et al., 2009). In the collaborative method, members of a targeted group are considered research collaborators and recruit members from their community. The modified method’s targeted collaborators (research assistants [RAs]; eight Whites, one biracial, and one African American) asked individuals from their social network to refer independently living oldest old. An additional validity check was put in place, which moved the recruitment beyond the RAs’ immediate social group by requiring that the RAs not personally know the recruited individuals.
Method
Ten doctoral student researchers served as RAs for the study under the direction of three faculty members (Primary Investigators [PIs]). RAs were recruited through student list servs of a large online university. Ten psychology students were chosen as RAs based on an interest in gerontology, their ethnicity, and their geographical location to ensure a nationally representative sample for the study. None of the RAs had previously worked with the PIs in any related research. All RAs were volunteers and received course credit for their participation in an online lab course and their work in the study. The RAs were trained on the design and study protocol. Walden University’s Institutional Review Board approved this project: Approval No. 03-09-11-0784474.
Participants
RAs maintained an ecomap (Sokolovsky, & Cohen, 1981) of their social network. Thirty-eight Whites were referred to participate; five were not above 85 or did not pass the Mini Mental State Exam (MMSE), leaving 33 participants. Minorities were much more difficult to recruit. Seven RAs reported asking 58 minority individuals in their social network for referrals, four provided referrals, 2 of these individuals agreed to participate. A variety of reasons for nonreferrals were given, some examples: not wanting to participate in research with White researchers, did not know anyone that fits the criteria, and the older adults did not want to participate.
The final sample consisted of 35 independent living participants ranging in age from 84 to 96 (M = 88.4 years, SD = 3.12). Our definition of independently living included individuals in assisted living facilities but did not include nursing home residents. Six males (17.1%) and 29 females (82.9%) participated in the study; two individuals self-reported as African American (5.7%), all others were White. Twenty-four were widowed (68.6%), seven were married (20.0%), one was divorced (2.9%), and three were single (8.6%). Four (11.4%) did not finish high school, 12 (34.3%) had just a high school diploma, 15 (42.9%) had some college or trade school, 3 (8.6%) received a bachelor’s degree, and one (2.9%) had a master’s degree. Sixteen states were represented: Arkansas, California, Florida, Georgia, Idaho, Kansas, Maryland, New Mexico, New York, North Carolina, Oregon, Pennsylvania, Texas, Virginia, Washington, and West Virginia.
Procedures
The surveys and interviews were conducted individually in an environment comfortable to the participant. They were offered choices for the interview: in their home, a neutral location (such as a library or coffee shop), phone interview, or Skype.
All RA interactions with the participant were digitally recorded, starting when the participant signed the consent form until the completion of debriefing. PIs monitored all recordings for adherence to protocols. A modified MMSE to check cognitive status was conducted (asking questions such as “What is your current address?”). Participants were required to be able to answer all questions without hesitation and accurately to be included in the study. Other inclusion criteria included being able to speak and write English and able to hear adequately for an interview. All participants completed a consent form; on passing the MMSE they completed the surveys and were interviewed over approximately 1 hr. All participants who qualified for the study completed the surveys and interviews.
Quantitative Portion
Participants completed a detailed demographic survey and the following measures in addition to the interviews in this mixed method study:
Locus of control
The Levenson Multidimensional Locus of Control scale (Levenson, 1973) is a 24-item assessment measure, which includes three separate subscales: internal LOC, powerful-others LOC, and chance LOC. Respondents were required to indicate the extent to their agreement with statements on a 6-point scale ranging from strongly agree to strongly disagree. The internal scale statements include items such as, “When I make plans, I am almost certain to make them work.” The powerful-others scale statements include items such as, “I feel like what happens in my life is mostly determined by powerful people.” The chance scale statements include items such as, “When I get what I want, it is usually because I’m lucky.” Previously reported internal consistency (Cronbach’s alpha) for the subscales is .58 for internal, .71 for powerful others, and .67 for chance (Levenson, 1973). In the current study, the Cronbach’s alpha was .75 for the internal subscale, .79 for powerful others, and .82 for chance.
Resilience
Wagnild and Young’s (1990) resilience scale is comprised of 25 items reflecting five characteristics of resilience: inner strength, competence, optimism, flexibility, and the ability to cope effectively when faced with adversity. Respondents indicated the extent to which statements apply to them on a 7-point scale ranging from disagree to agree. An example statement is “When I make plans I follow through with them.” Previously reported internal consistency (Cronbach’s alpha) for the scale is .91. In the current study, the Cronbach’s alpha was .79.
Self-efficacy
The Generalized Self-Efficacy scale (Schwarzer & Jerusalem, 1995) is a 10-item scale that assesses the strength of an individual’s belief in his or her own abilities to respond to unexpected and stressful situation. Respondents are required to indicate the extent to which statements apply to them on a 4-point scale from not at all true to exactly true. The statements include items such as, “I can always manage to solve difficult problems if I try hard enough.” A total score is derived by summing the scores for all items, yielding a maximum score of 40. The higher the score, the greater is the level of general self-efficacy. The scale demonstrated internal consistency in the original sample with a Cronbach’s alpha of 0.86 (Schwarzer & Jerusalem, 1995). In the current study, the Cronbach’s alpha was .87.
Demographic survey
The PIs designed a demographic survey that asked about the individual’s relationship with the PHP and health practices. It also asked questions about the interaction of family members and staff from facilities in participants’ health care. The survey was piloted on three older adults with changes made to clarify language.
Qualitative Portion
The PIs developed and piloted the 18 interview questions (available from the authors), which followed up on questions in the demographic survey. The interviewers periodically checked to see if the participants needed breaks. At the end of the interview session, the participant was debriefed.
Two PIs reviewed all interview recordings to insure the quality of the data and consistency in protocol compliance. A single transcriptionist transcribed the digitally recorded interviews. A coding scheme was developed for the qualitative data and all responses were coded and categorized into themes by the PIs. The qualitative data was transformed into quantitative data by reducing themes and codes to numeric information, using a scoring rubric to systematically quantify the interview data as recommended by Creswell and Plano Clark (2011). The subsequent results were analyzed through correlations and/ or chi square as appropriate. Clarification of the results is provided in the subsequent section through participant quotes.
Results
The results section is organized through the four research questions. The first research question asked, “How do the oldest old describe their relationship with their PHP relative to their reported health practices?” Thirty-three (94.3%) individuals indicated they were satisfied with their PHP, 2 (5.7%) were dissatisfied. An example of a satisfied comment: Satisfied. She explained what the results of everything were, what could be done about it and what couldn’t be done about it. (Jane, age 86)
A dissatisfied comment: Dissatisfied. Well, that again had to do with this shoulder thing. And she was going to send me to a specialist. And I asked her what the point was in sending me to the specialist. And she said, they probably could do more than she could. And so, on my way home I got to thinking about it. And as soon as I got to the bottom of the hill I called and told them I wasn’t going to go because there was no point. And she wouldn’t talk to me. I talked to the nurse and I talked to the receptionist, but she wouldn’t talk to me. So, I decided that was it. (Mona, age 90)
On the demographic survey, 32 (91.4%) indicated they liked the provider. Individuals without a chronic condition were less likely to indicate their relationship with the PHP was good or very good, r(34) = −.358, p < .05.
Participants indicated their PHP talked to them from 2 to 30 min, with a mean of 15.8 min. During the interview, participants described their PHP. Some examples of positive comments made by participants about their PHP: [He gives me] all the time that I need when I go, and as I said, he doesn’t rush me. He gives me time to think them out. (Lora, age 85) He really explains everything good, to me. What’s wrong and what I got to do. I feel real free talking to him. (Evelyn, age 87)
Some negative comments: Her mind just seems to be somewhere else. And I think she’s got problems. (Mona, age 90) I don’t think he listens to me the way he should. (Terry, age 90, female)
A majority of participants indicated someone went with them to the PHP (n = 21, 60%), primarily family members escorted them (spouse 14.7%, daughter/daughter-in-law 26.5%, son/son-in-law 5.9%), 14.7% went with a friend. An escort to the PHP increased the likeability of the PHP, r(35) = −.347, p < .05, and the PHP was more likely to be described as “kind,” r(35) = −.516, p < .01.
Only one person reported audiotaping the PHP visit. Twenty-five people (71.4%) reported either family or staff where they live asked them about what happened during the visit.
Participants were asked on the demographic survey about various health-related practices. Twenty-nine percent indicated occasionally or frequently drinking alcohol; males were more likely to be in these categories (p < .05). The majority (91%) indicated they do not use tobacco. Seventy-seven percent reported they occasionally or frequently exercised. Eighty-six percent indicated they read for pleasure, the majority of whom were women (p < .05). Twenty-six percent of the participants indicated they never or seldom gambled, while 97.1% ate meat on a regular basis. The combination of tobacco use, drinking alcohol, and gambling tended to be correlated (p < .05).
Participants responded to questions about their comfort with discussing various health related topics with their PHP. Sex-related information led to the highest reports of discomfort, with 22.9% reporting to be uncomfortable or very uncomfortable with this topic. People with higher scores on the self-efficacy survey were more comfortable with the topic of sex than those with low scores (p < .05).
Participants were asked during the interview whether their PHP had discussed normal changes that occur with aging. Five (31.4%) responded “yes”; 10 (28.6%) responded “a little”; 20 (57.1%) said “no”; and 11 (31.4%) said they received the information from someone other than PHP. An example of a “yes, a little” response: Yes, we have [discussed changes with aging]. It was in a picking way. I told her, I said, “You sure do get mighty feeble when you get a little age.” And she’ll go on about something like that. (Maybelle, age 87)
An example of an explanation of aging changes: She explained [aging] like an engine in a car. After so many years the engine wears. That some of the parts of the body do the exact same thing. She said that we try to repair them as much as possible. When they’re not the same, we just try to repair. (Jane, age 86)
An example of receiving information from someone other than PHP: Well, you know, this place where I live is for older people. They have nurses who run different seminars on different things about aging. And I always check in on that kind of stuff. (Mona, age 90)
Participants were asked on what aging topics they would like more info from their PHP. The results were assisted living (n = 2); body changes with aging (n = 5); depression and anxiety (n = 4); exercise (n = 6); incontinence (n = 4); medication management (n = 2); nutrition (n = 3); sex and aging (n = 4); herbs and vitamins (n = 5).
The second research question examined, “How do scores on the personality measures self-efficacy, resiliency, and LOC interact with PHP relationship descriptions and reported health practices?”
The LOC scale had three subscales: internal (M = 35.9, SD = 9.1, range = 12-48), powerful others (M = 16.8, SD = 10.6, range = 0-39), and chance (M = 21.3, SD = 11.4, range = 0-45). Higher chance score was related to a higher powerful others score, r(35) = .722, p < .001. A high internal LOC score was correlated with a high resiliency score, r(34) = .364, p < .05. Having an escort to the PHP was related to a higher powerful others score, r(32) = .397, p < .05. A difference was present for internal LOC and gender: no males were in the low range, r(34) = −.364, p < .05. Individuals with a high internal LOC were more likely to ask for a referral from their PHP than those with a low score, r(34) = .431, p < .01. Individuals with a low belief in powerful others were more likely to state they exercise regularly, r(34) = −.315, p < .05, as were individuals with a low belief in chance, r(34) = −.513, p < .01.
The mean for the resilience scale was 140.03 (SD = 13.13), with a range of 110 to 166. A higher resilience score was related to a high self-efficacy score, r(35) = .573, p < .01, and a high internal LOC score, r(34) = .364, p < .05. Individuals with a high resilience score were more likely to have recently had a full physical, r(32) = −.356, p < .05, and to report visiting the PHP for preventative care, r(34) = −.402, p < .05.
The mean for the self-efficacy scale was 31.3 (SD = 4.6), with a range of 22 to 39. Higher self-efficacy was related to higher education, r(35) = .334, p < .05. Females were likely to have a lower self-efficacy than males, t(32) = 4.84, p < .01. Higher self-efficacy resulted in being more comfortable in discussing sexual issues with the PHP, r(35) = .394, p < .05.
Individuals with high internal LOC, r(33) = −.432, p < .05, and high resilience, r(34) = −.402, p < .05, scores were more likely to see the PHP for preventative care only.
The third research question examined, “Schwarzer and Jerusalem (1995) and Halisch and Geppert (2012) reported self-efficacy correlates with LOC in younger older adults. Does this relationship continue into the oldest old age group?” In the current study, a high internal LOC score was correlated with high self-efficacy, r(34) = .394, p < .05.
The fourth research question explored, “The CDC reported that for people above the age of 85 there is an average of 7.8 (SE = 0.6) yearly physician visits. Is the sample of healthy oldest old individuals in the current study equivalent to the CDC’s statistics or do they show a different pattern?”
Three primary questions examined how often the individuals visits their PHP. The first demographic question examined frequency of PHP visit. The frequency of visits ranged from 1 to 12 times, with a mean of 4.16. A one-sample t test was conducted using the CDC’s mean of 7.8 as the test value, t(31) = −3.64, p < .0001, thus the current sample had significantly fewer visits .
The second demographic question examined time (in months) since their last full physical (range = 0-82 months, M = 12.7 months). The third question was an interview question: “Why do you tend to go to your PHP?” and resulted in three themes. Twenty-one (60%) participants indicated they go just for preventative care. Such responses included
I just go to get my heart checked. (William, age 95) It is a regular checkup I go on, every five months. I go regularly. (Evelyn, age 87)
Five (14.3%) individuals went to the PHP only when they are ill, these responses included
I don’t want to go unless I’m sick. (Ann, age 94) I don’t go to him unless I have something special that I need to see him about. I don’t like to go to doctors. (Virginia, age 87)
The remaining 9 (25.7%) participants reported that they visit the PHP for preventative care and when ill. Such comments included
I usually go about every four months, and then if I have a cold or anything in-between, if I need to go, I go then. Mostly it’s every four months. (Garnet, age 90) Well, it’s a combination of both, but I have a regular six month checkup like thing. (Lora, age 85)
Interestingly, six (17.1%) volunteered they “never get sick”; these individuals also only went to their PHP for preventative care: I don’t know what that word [sick] is. I haven’t been sick in years. (William, age 95) I can’t tell you the last time I was sick. (Marion, age 88)
In response to a demographic question, four individuals (11.4%) reported the cost of care affected how often they visited their PHP, r(35) = −.408, p < .05. All of these individuals reported only having Medicare coverage and no private insurance. On the demographic survey, one (2.9%) participant indicated transportation was a problem in getting to the PHP and one indicated that sometimes it was a problem.
Discussion
The first research question asked, “How do the oldest old describe their relationship with their PHP relative to their reported health practices?” Lee and Kasper (1998) reported relative to 65- to 69-year-olds, people 80 to 84 were 20% to 30% less likely to be highly satisfied with their quality of care and physician quality. The older individuals particularly had issues with the physicians’ technical skills and interpersonal manner.
Contrary to Lee and Kasper (1998), the majority of the participants in the current study indicated they were satisfied with and liked their PHP. Two participants indicated they were dissatisfied; these individuals indicated they felt the PHP did not pay sufficient attention to their concerns, which is in accordance with Lee and Kasper’s (1998) findings. Both of the dissatisfied individuals were above the age of 90; while the number is insufficient to draw any conclusions, it suggests that additional research should examine the topic further, particularly with the oldest individuals.
Males were most likely to report drinking alcohol regularly. The majority (91%) of participants indicated they do not use any form of tobacco (consistent with Cherry et al., 2013), and they read for pleasure (85.7%). Reading has been associated with a reduction in the development of dementia (Tesky, Thiel, Banzer, & Pantel, 2011). Virtually all participants (97.1%) indicated they eat meat regularly; although meat has been a traditional dietary staple for this age group, its use is related to an increase in cardiovascular risk (American Heart Association, 2012; Polychronopoulos et al., 2010). The combination of tobacco use, drinking alcohol, and gambling was correlated; thus, PHPs should be aware these practices occur concurrently, particularly with males.
The results suggest it would be advantageous for PHPs to recommend that someone accompany the oldest old on visits. Individuals who had escorts tended to indicate they liked their PHP and considered them more kind than people who went alone. There are a number of possible explanations for this finding; it may be that escorts encourage patients to change PHPs if they do not approve of them. On the other hand, having someone else approve of the PHP may cause a halo effect (Greenwald & Banaji, 1995), improving the oldest olds’ perception of the PHP. An alternative is that those who like their PHP may be more motivated to get treatment, and thus more likely to secure an escort. Additional research is needed in this area.
Only 5 (31.4%) participants indicated their PHP had discussed normal changes with aging with them. The participants expressed interest in a number of topics related to aging. It appears it would be advantageous for PHPs to have brochures or booklets available on aging topics for their patients.
The second research question examines, “How do scores on the personality measures self-efficacy, resiliency, and LOC interact with PHP relationship descriptions and reported health practices?”
Previous research has reported that LOC is associated with patient–provider relationships. Brincks et al. (2010) and Rennemark et al. (2009) found a negative correlation between physician visits and functional ability, education level, and internal LOC. Individuals with a high internal LOC score also tend to be proactive in seeking information, making health modifications, and treatment adherence (Macaden & Clarke, 2010).
The current study was consistent with these findings (although the correlation with education was not significant). A high internal LOC was correlated with a willingness to ask for a referral from the PHP, evidence of assertiveness. A high internal LOC was also correlated with visiting the PHP for preventative care, consistent with Macaden and Clarke (2010). Participants with a high belief in powerful others were more likely to have an escort to the PHP. Perhaps these individuals believe the escort would mitigate the power of the PHP, or would be an advocate if needed.
Individuals with a low belief in powerful others were more likely to state they exercise regularly, consistent with previous research (Grant-Savela, 2009). This finding suggests internal beliefs may be the influencing factor rather than an external source such as the media or PHP recommendation. Individuals with high scores on the chance subscale were also less likely to indicate they would confront a PHP when they were unhappy with their care. These individuals appear to believe confrontation would not be effective, but rather they must cope with the status quo.
Males had higher self-efficacy as did individuals with higher education. Individuals with a higher self-efficacy indicated they would be more comfortable in discussing sexual issues with the PHP than those with lower self-efficacy. This finding is consistent with the research of Clayman et al. (2010) who reported that high self-efficacy results in an increased confidence in asking the PHP questions. It is also further evidence of individuals’ confidence in managing their own needs even to the point of overcoming the embarrassment of the topic of sexuality.
Kostka and Jachimowicz (2010) reported individuals with higher self-efficacy were more likely to benefit from health education interventions. This was confirmed in the present study whereby high self-efficacy was correlated with PHP visits for preventative care.
The only previous study examining Wagnild and Young’s (1990) resilience scale and LOC was with middle-aged women with a history of traumatic experiences (Friedman, 2009). This relationship was confirmed in the present study in the oldest old: high resilience scores are correlated with an internal LOC.
The third research question examined, “Schwarzer and Jerusalem (1995) and Halisch and Geppert (2012) reported self-efficacy correlates with LOC in younger older adults. Does this relationship continue to into the oldest old age group?” In the current study, a significant positive relationship was found between self-efficacy and internal LOC, leading to the conclusion that the relationship between the variables appears to continue through the life span.
The fourth research question explored, “The CDC reported that for people above the age of 85 there is an average of 7.8 (SE = 0.6) yearly physician visits, which is lower than for those 75 to 84 years of age. Is our sample of healthy oldest old individuals equivalent to the CDC statistics?”
The present study’s reported number of PHP visits per year was significantly lower than the CDC’s statistic for the age group. If the patient initiated the visit for preventative care, it would seem that a personality factor such as internal LOC or self-efficacy should be related to the number of visits, which they were not. Socioeconomic indicators such as cost and family income were not related to the number of visits, suggesting that it is not a cost issue, which, considering everyone in this age group is eligible for Medicare/Medicaid, seems appropriate. Participants indicated fewer visits were not a transportation issue contrary to Wolinsky et al.’s (1988) speculation that the decline in physician visits in this age group may be due to a general decline in mobility. The PHPs’ personal characteristics (PHP gender, descriptions by patients) had a negligible effect on frequency of visits. An additional possibility is that their memory for number of visits was skewed due to self-report; however, since the majority of participants reported regular, scheduled preventative care, this does not seem likely. One explanation may be a family history of long, healthy lives in combination with their regular preventative care scheduled by the PHP. The present findings warrant additional study with a larger sample.
A minority (14.3%) stated they visit their PHP only when ill. This finding suggests the rationale for less frequent PHP visits in this age group may be more complex than has previously been evident through surveys (e.g., Wolinsky et al., 1988). It suggests that some may not appreciate the need for preventative care, which puts them at risk for future health problems.
The patient-by-treatment-context interactive model of Christensen and Johnson (2002) was found to be consistent with the current study. It led to the prediction that there would be consistent preventative care (adherence) when the patient has higher internal LOC, which was found. Higher resilience scores were expected due to their inner strength, optimism, and health-promoting behaviors, which were seen in higher preventative care. Higher self-efficacy was expected and, in the current study, these individuals were more comfortable with their PHP.
Furthermore, it was also predicted that there would be less preventative care (lack of adherence) when the patient had lower internal LOC (more external), which was found. It was expected that higher powerful others and chance scores would be indicative of less trust in the PHP, these scores were correlated with less exercise, and that they would not confront the PHP. Lower resilience scores were expected due to fewer health-promoting behaviors, in the present study, these individuals were less likely to report going for preventative care. Lower self-efficacy was related to feeling less comfortable discussing sexually related topics with the PHP.
Additional research is indicated that specifically targets oldest old individuals in minority groups to examine the relationship of the model to their care. In the current study, the participants were on the healthier end of the spectrum for their age group. It would be interesting to examine the model’s reliability with less healthy members of the age group.
It is important to consider the generalizability of the current study. This study examined relatively healthy, independently living, oldest old adults recruited through online students’ social networks; thus, the results are specific to this group and may not be generalizable to the general population of oldest old. This sample is only generalizable to the extent other individuals share the sample’s key demographics. A modified collaborative sampling technique was used, which is commonly used to recruit hard to reach populations (Knight et al., 2009); therefore, it is not known the extent to which the current sample reflects the population. This sampling method was chosen specifically because the researchers wanted to reach minority participants, yet it still resulted in only a small number of minorities in the sample. This experience highlights the need for more attention to the process of recruiting minority oldest old for research projects.
This mixed method study’s results suggest the relationship between the oldest old and their PHP is more complex than has been previously reported. The PHP relationship with the oldest old appears to relate to not only the PHP’s personal qualities but also personality characteristics and beliefs of the older adult patients and even the influence of the accompanying escort of the patient.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article: This research was supported by the Presidential Fellowship for Research in Online Education from Walden University.