
Abstract
The purpose of this study was to determine the effectiveness of an 8-week Tai Chi Chih exercise program on physical functional performance (PFP) among women aged 45 to 65 years. A quasi-experimental design with a nonequivalent comparison group was used. Forty-one healthy inactive women were assigned to either an intervention group (n = 19) or a comparison group (n = 19). A 60-min Tai Chi Chih exercise class was conducted twice a week for 8 weeks. PFP was measured at baseline and postintervention using the Continuous Scale Physical Functional Performance–10 (CS-PFP 10). Between-group differences were analyzed using one-way analysis of covariance (ANCOVA). After participating in the 8-week program, intervention group participants showed greater improvement in the CS-PFP measures (p < .05, η2 > .06). However, the comparison group had little changes. The findings from this study suggest that participation in an 8-week Tai Chi Chih exercise program can improve PFP in healthy, community-dwelling middle-aged women.
Introduction
Older adults are the fastest growing segment of the United States, especially adults aged 65 years and above (Zedlewski, Barnes, Burt, McBride, & Meyer, 1970). Currently, there are 39 million older adults living in the United States accounting for 13% of the population, and this number is expected to almost double by 2030 (Federal Interagency Forum on Aging-Related Statistics, 2010). The aging process is associated with many health-related problems that could lead to the decline in physical and psychological well-being including decline in musculoskeletal function, limited mobility, and loss of bone density and muscle mass that increases the risk of falls and loss of daily performance (Manini & Pahor, 2009; Qin et al., 2005). Falls are a major threat to the health and independence of older adults. Falls are not an imminent effect of aging, however, and typically occur as the result of poor balance and functional status, fear of falling related to pain and suffering, or low self-efficacy (Li et al., 2001; Sattin, Easley, Wolf, Chen, & Kutner, 2005). All of these factors are also more prominent among the female population after the onset of menopause (Manini & Pahor, 2009). Despite women having longer life spans, they are often more inactive and disabled than men (Conn, Burks, Pomeroy, Ulbrich, & Cochran, 2003). Unfortunately, older adults also are less likely to adopt a physically active lifestyle than younger adults. Therefore, targeting insufficiently active women in middle age, as in this study, can prevent or slow the onset of the detrimental effects of physical inactivity as women age.
Tai Chi Chuan (Tai Chi), Pilates, and Yoga are a few exercises that are better for older adults because they are low-impact exercises that are associated with improved balance, strength, flexibility, psychological well-being, and quality of life (Lan, Lai, & Chen, 2002). Tai Chi is a “mind–body” exercise that is based on the Chinese philosophy Taoism, and involves balancing chi or an individual’s personal bioelectric energy. Tai Chi is also a low-cost, low-speed, and low-impact weight-bearing exercise (Lan et al., 2002). The slow movements of Tai Chi are performed by coordinating diaphragmatic breathing with graceful motions that are practiced in a semisquat posture (Kit, 2002). These movements are designed to produce mind tranquility through breathing and meditation, and participants are encouraged to respect their limitations and not over exert themselves. Many studies have shown the positive effect of Tai Chi on physical functioning in older adults (Chen, Hsu, Chen, & Tseng, 2007; Fyre, Scheinthal, Kemarskaya, & Pruchno, 2007; Li et al., 2001). However, little attention has been devoted in determining the effect of Tai Chi in middle-aged adults. Currently, only a few studies have documented the improvement in physical function in adults younger than 60 years of age (Shih, 1997; Jacobson, Cheng, Cashel, & Guerrero, 1997). To address this gap, the present study documents the changes in physical function in community-dwelling middle-aged women. If women enter the period of “old age” with high physical functional performance after practicing Tai Chi, this should result in extended independent living, improved functional status, and a better quality of life (Gu & Conn, 2008).
Tai Chi is differentiated into five major styles: Chen, Yang, Wu, Sun, and Wu (Hao; Kit, 2002). Another type, Tai Chi Chih, is a simpler form of Tai Chi exercise that is composed of only one pose called “cosmic consciousness pose” and 19 movements (Schaller, 1996). It has visual similarities to other forms of Tai Chi except the martial arts aspect. It is completely nonviolent and widely practiced among the elderly because it does not require a high level of fitness and usually takes about a short period of 8 weeks to learn (Fontana, Colella, Baas, & Ghazi, 2000). Tai Chi Chih is a set of movements focused on generation of an intrinsic energy called Chi. It is effective in reducing stress; improving balance, physical functioning, mental health; and general well-being (Detert, Derosia, Caravella, & Duquette, 2007; Fontana et al., 2000; Irwin, Pike, Cole, & Oxman, 2003; Schaller, 1996). In these studies, the duration of exercise was either 1 hr or 45 min once a week for 10 to 15 weeks. However, the exercise intensity was not specified in these studies. This form of Tai Chi was used in the current study due to its unique benefits. In addition, one of the goals of this study was to determine whether middle-aged sedentary women can benefit from an activity that is less vigorous than those normally identified by the lay person as “exercise.” If so, Tai Chi Chih may be an effective means of facilitating regular physical activity and improve physical function among women who are inactive. As there are only a few studies that have focused on Tai Chi Chih, more research is needed to determine the effectiveness of Tai Chi Chih in middle-aged and older adults.
Physical function is measured by the ability to perform both activities of daily living (ADL) and instrumental activities of daily living (IADL), which incorporate balance and coordination, flexibility, muscular strength, and endurance (Gu & Conn, 2008). ADLs are defined as routine tasks done on a daily basis necessary to maintain independent living (eating, walking, using toilet, getting in and out of bed or chair, dressing, taking shower, etc.) and IADLs are defined as the secondary-level activities important to daily living that involves the use of a tool (cooking, shopping, driving, taking medication, making phone calls, laundering, housekeeping, etc.). To live independently, older adults have to be able to carry out a majority of their daily activities on their own. Studies have indicated that higher aerobic capacity provided a greater aerobic reserve, which in turn was associated with higher physical functional performance (Arnett, Laity, Agarwal, & Cress, 2008; Posner et al., 1995). As noted, few studies have been conducted to evaluate the impact of Tai Chi exercise on physical function using self-reported and performance-based measures of physical function (Chen et al., 2007; Fyre et al., 2007; Li et al., 2001) and documented significant improvement in functional performance after participation in Tai Chi. Verhagen, Immink, Meulem, and Bierma-Zeinstra (2004) performed a systematic review on the effect of Tai Chi on fall prevention and self-reported physical function in older adults. They reviewed a total of seven studies. The inclusion criteria were randomized or concurrent controlled trial, the age of the study population was 50 and above, and one of the interventions was a form of Tai Chi, and falls, balance, and cardiorespiratory functions were used as outcome measures. Intervention periods ranged from 10 weeks to 1 year. From this review, it was concluded that physical function improved and falls were reduced in people aged 50 and above after practicing Tai Chi (Yang style) for 1 hr weekly. Fyre et al. (2007) investigated the effectiveness of Yang-style Tai Chi and low-intensity exercise on physical function and psychological well-being in sedentary, older adults. Physical function was assessed using performance-based measures that included the 2-min step test, 8-foot up-and-go test, and grip strength test. Both exercise groups improved significantly with respect to body strength, balance, physical function, and well-being after the intervention; specifically, the Tai Chi group had a 7.1% increase in upper body strength, 11.9% increase in lower body strength, a 25.7% increase in endurance, and a 15% increase in balance. These studies support the conclusion that physical functional performance can be improved in participants who are 50 years and older by participation in Tai Chi.
This study aimed to provide more evidence on the effectiveness of Tai Chi Chih in improving the physical functional performance in healthy, community-dwelling women aged 45 to 65 years. It was hypothesized that there would be greater improvement in physical functional performance in the intervention group than in the comparison group.
Methods
Sample and Study Design
This study targeted healthy, sedentary middle-aged women living in the Norman, Oklahoma, area. Recruitment occurred in the area using program flyers in community displays and by convenient sampling technique. The study was conducted in the early spring of 2010 (from the beginning of March until the end of April), which is usually still rather cool in the area where the study was conducted. Participants had to be 45- to 65-year-old community-dwelling women who were insufficiently active (<30 min a day of moderate activity, 5 days a week or <150 min of moderate activity a week) or sedentary and physically able to participate in an exercise program. They could not have participated in a Tai Chi program within the previous 12 months. Participants with any chronic disease or any condition that would limit them from any type or amount of physical activity were required to get a medical clearance from their physician before volunteering for the study. An a priori sample size calculation using the parameters of α = 0.05, power value of 0.80, and Cohen’s d = 0.80 (Lan, Lai, Chen, & Wong, 1998) was used, and it was found that 20 participants were needed for both groups (Borenstein, Cohen, & Rothstein, 1997).
A quasi-experimental research design (pre-/posttest) with a nonequivalent comparison group was used. After reviewing the medical histories of 41 volunteers who met the inclusion criteria, women were assigned to either the intervention or comparison group. Assignment was based on their ability to meet on the days and times that were established for the Tai Chi Chih class. Those who could commit to the class schedule were assigned to the intervention group and those who could not attend classes on a regular basis were assigned to the comparison group. A total of 3 women dropped out of this study, 2 from the intervention group and 1 from the comparison group, resulting in 19 participants for each group. One participant dropped out due to a leg injury that was unrelated to participation and the other 2 dropped out for personal reasons.
Measurement Procedures
At preintervention and after completion of the 8-week intervention, both groups were tested using the Continuous Scale Physical Functional Performance–10 (CS-PFP 10) testing protocol. Testing was conducted in the Functional Performance Laboratory at the University of Oklahoma. The CS-PFP 10 test battery involves completion of 10 standardized tasks. The testing battery has been documented to be a valid, reliable, and sensitive measure of physical function (Cress, Petrella, Moore, & Schenkman, 2005). The CS-PFP 10 is a group of performance-based measurement protocols that mimic “real life” activities designed to provide a comprehensive measure of physical function that reflects functional abilities in several separate physical domains. It consists of 10 household tasks that are categorized based on the physical exertion that is required to complete the task. Low-effort tests include activities such as (a) carrying a weighted pan from one counter surface to another; (b) picking up a jacket, putting it on, closing the front, removing the jacket, and putting it back; and (c) reaching as high as possible and placing a sponge on an adjustable shelf without losing balance. Medium effort tests include activities such as (a) sweeping the floor and collecting the litter in a dustpan, (b) picking up scarves from the floor, and (c) transferring clothes and 9 lbs of sandbags from a washer to dryer and transferring clothes from dryer to a clothes basket. High-effort tests include tasks such as (a) sitting on the floor from standing and then standing back up, (b) walking up one flight (9) of stairs without pulling the body up the stairs, (c) carrying bags of groceries a specified distance including up- and downstairs, and (d) walking as far as possible in 6 min. Task performance was quantified by time required to perform the task, weight carried during the task, and distance traversed during task performance (Cress et al., 2005). Because the time required to complete tasks, weight carried during tasks, and in some cases, distance covered during a task are determined by the participant, it is highly unlikely that participants can “outperform” the measurement capabilities of the test. This results in a low probability of a ceiling effect when using the CS-PFP test battery. A composite score was calculated for total physical functional performance (CS-TFP) and summary scores were computed for five domains: upper body strength (CS-UBS), upper body flexibility (CS-UBF), lower body strength (CS-LBS), balance and coordination (CS-BAC), and endurance (CS-END; Cress et al., 2005; Hearty, Schenkman, Kohrt, & Cress, 2007). Scores were calculated using a standardized algorithm that integrates time, weight, and distance measures from multiple tasks that are associated with each performance domain. For instance, computation of lower body strength utilizes data from 6 of the 10 tasks (scarf pick-up, two laundry tasks, floor sweep, grocery carry, floor up and down, and stair climb). Raw data were recorded and input into an analysis package developed specifically for this testing protocol and to produce the summary scores for the total and five domains mentioned above. Scores were scaled from 0 to 100, using a formula based on lower and upper extremes of performance from previously tested older adults (Cress et al., 1999; Hearty et al., 2007). An overview of variables is presented in Table 1.
Overview of Variables—CS-PFP 10.
Note: CS-PFP 10 = Continuous Scale Physical Functional Performance–10.
Intervention
Tai Chi Chih is a form of Tai Chi that is regularly taught to adults at a local senior center in the community in which this study was conducted. Because of this, there was a qualified instructor available to conduct classes, which was important because of the specialized nature of the movements. The Tai Chi Chih intervention was provided in two 1 hr-sessions per week for 8 weeks. This time frame was chosen based on the previous finding that at least 8-week intervention duration was needed to produce changes in physical functioning using Tai Chi exercise (Schaller, 1996; Tsang & Hui-Chan, 2004; Yan, 1998). The certified Tai Chi Chih instructor taught all 19 movements of Tai Chi Chih to the class throughout the 8-week period. Each class consisted of 10 min of warm-up exercises, 40 min of Tai Chi Chih movements, and 10 min of cooling down exercise. There was no cost for participation in the Tai Chi Chih class or testing. The warming up exercise comprised walking around with moving hands. The Tai Chi Chih exercise involved lateral arm extension and trunk rotation, bending of knees in wide steps, moving forward and backward, sideway stepping, and weight shifting (Choi, Moon, & Song, 2005; Li, Devault, & Oteghen, 2007). The cycle of 19 movements was repeated for 40 min while listening to traditional instrumental music to maintain slow and continuous movements. The cooling down exercise comprised stretching of arm and leg muscles and breathing exercises (Li et al., 2007). There was a make-up session during weekends for those who missed a session during the week. Comparison group members did not attend the classes during the study period because it may serve as a standard for comparison against the intervention group where the intervention is applied. In addition, they did not receive an incentive; however, they were given an opportunity to attend Tai Chi Chih class at a very low cost after the intervention. Members of the comparison group were instructed to maintain their normal daily activities and avoid participation in any form of organized exercise during the 10-week testing and intervention period. However, no measures were taken to verify that this group did not participate in outside exercise during the study period.
Data Analysis
Data were analyzed using SPSS V17.0. To first determine if groups were equivalent at baseline, pretest measures were compared using an independent t test for all dependent variables. Because there were preintervention differences in the CS-PFP outcome variables between the comparison and intervention groups, one-way analysis of covariance (ANCOVA) using preintervention CF-PFP variable scores as covariates was used to control for these differences to identify between-group differences after the intervention.
Results
Baseline Measures
The average age of participants was 56.5 years. Almost all the participants were White/non-Hispanic (95%), married (74%), and worked either full or part-time (76%). This was also a well-educated sample with 63% having some college and 37% having a 4-year college degree. A majority of participants reported their health status as good or excellent, which was evaluated using a self-reported questionnaire (see Table 2). All participants reported themselves as independent and healthy prior to participation in the study. None reported health concerns or physical limitations that could be aggravated by participating in the Tai Chi Chih class. Looking at potential differences in demographic characteristics between the groups, the average age of the intervention group was higher, but not statistically different from the comparison group. The comparison group had a higher percentage of people who rated their health excellent. There were no statistical differences in demographic characteristics between the groups. During post-testing, six participants from the intervention group reported having minor leg or foot pain. Most of them believed that it may have been related to becoming more active after being sedentary for a long time. Demographic data are presented in Table 2.
Participant Characteristics.

Note: Categorical variable—% (n).
The baseline values for the CS-PFP scores for both groups are presented in Table 3. Analyses indicated that all baseline CS-PFP scores (CS-UBS, CS-UBF, CS-BAC, CS-LBS, CS-END, CS-TFP) were significantly different between groups with the comparison group having better scores than intervention group. A possible reason for this is that participants were not randomly assigned into groups, but were assigned based on their ability to meet at the designated time for eight straight weeks of intervention. These results are consistent with the fact that comparison group members also reported better health status than the intervention group. Therefore, to control for these differences, preintervention CS-PFP scores were used as covariates when testing for between-group differences post-intervention.
Independent t-Test Results for CS-PFP Baseline Scores.

Note: CS-PFP = Continuous Scale Physical Functional Performance; CS-UBS = upper body strength; CS-UBF = upper body flexibility; CS-LBS = Lower body strength; CS-BAC = balance and coordination; CS-END = endurance; CS-TFP = total functional performance; IN = intervention group; COM = comparison group.
Significant difference between two groups (α = 0.01).
Outcome Measures
The percent change in CS-PFP scores from pre-to post-intervention are presented in Table 4. For the intervention group, a 32.5% change in lower body strength (CS-LBS) was the largest improvement with the smallest percent change in this group being 19.1% in endurance (CS-END). To determine the impact of Tai Chi Chih participation on physical function, ANCOVA was used to test for between-group differences post-intervention. As noted above, a comparison of baseline scores were significantly different between groups. Therefore, pretest scores were used as covariates in subsequent analyses. Results showed a significant main effect for CS-LBS, F(1, 35) = 6.1, p = .02; CS-BAC, F(1, 35) = 6.8, p = .01; CS-END, F(1, 35), = 6.1, p = .02; and CS-TFP, F (1, 35) = 6.0, p = .02. The effect sizes for CS-LBS (η2 = 0.148), CS-BAC (η2 = 0.162), CS-END (η2 = 0.149), and CS-TFP (η2 = 0.146) were large in size, supporting the conclusion that participation in Tai Chi Chih resulted in meaningful improvement in physical function among study participants. The ANCOVA results are presented in Table 5.
Percent Change in Pre- to Postintervention CS-PFP Scores.

Note: CS-PFP = Continuous Scale Physical Functional Performance; CS-UBS = upper body strength; CS-UBF = upper body flexibility; CS-LBS = lower body strength; CS-BAC = balance and coordination; CS-END = Endurance; CS-TFP = total functional performance; IN = intervention group; COM = comparison group.
ANCOVA Results and Effect Sizes for Changes in CS-PFP Scores.
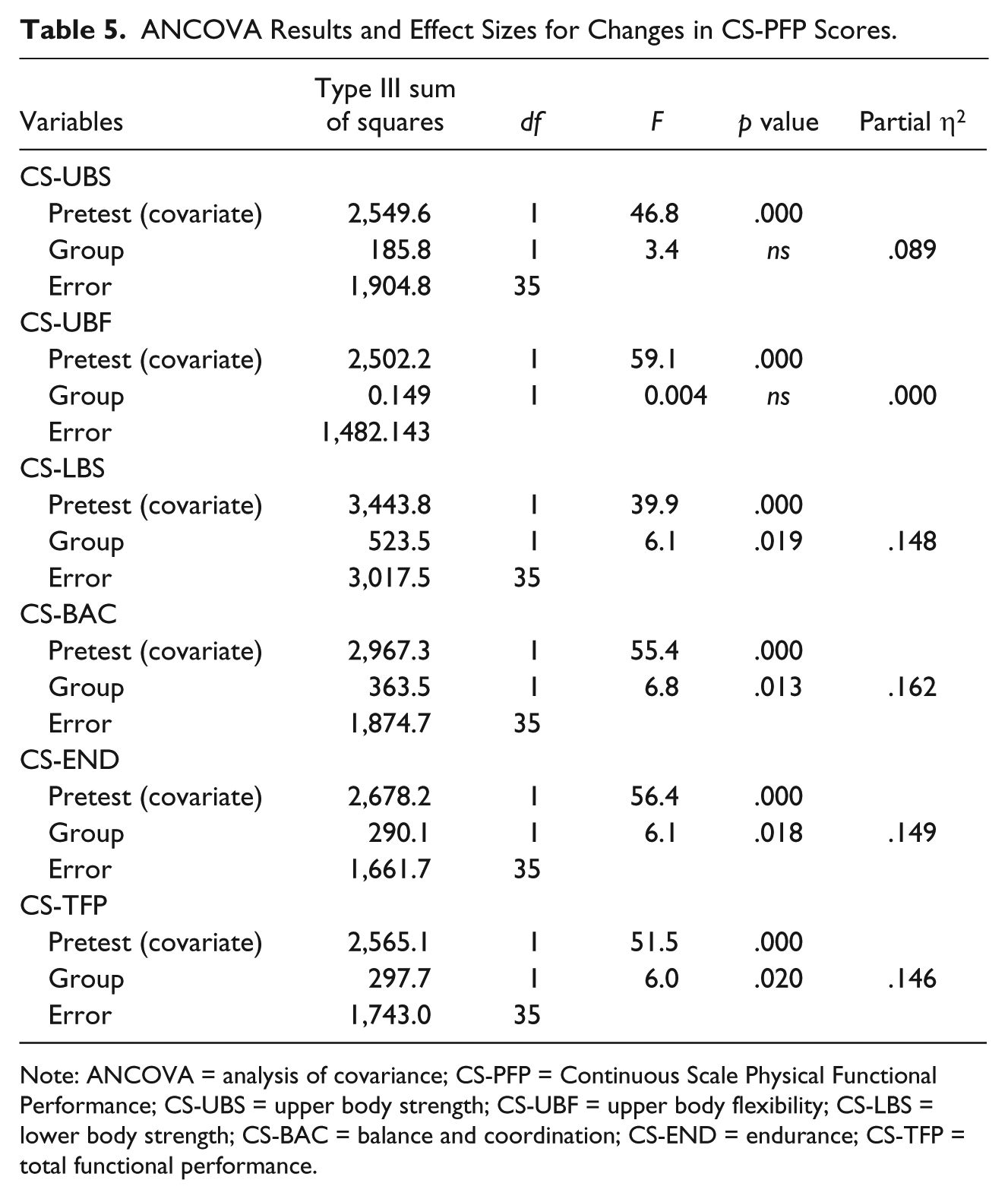
Note: ANCOVA = analysis of covariance; CS-PFP = Continuous Scale Physical Functional Performance; CS-UBS = upper body strength; CS-UBF = upper body flexibility; CS-LBS = lower body strength; CS-BAC = balance and coordination; CS-END = endurance; CS-TFP = total functional performance.
Discussion and Conclusions
The purpose of this study was to determine the effectiveness of an 8-week Tai Chi Chih exercise program in improving physical functional performance among middle-aged women. Results indicate that participation in this program had a beneficial effect on the majority of CS-PFP scores. Because Tai Chi Chih involves low-intensity yet challenging activities, it may be the type of activity that encourages participation among previously inactive/insufficiently active women as suggested by average attendance rates of greater than 90% per session.
Tai Chi Chih consists of 19 movements that are executed from a single pose called the cosmic consciousness pose. This may also have contributed to the success of this intervention. The cosmic consciousness pose requires constant use of the leg and thigh muscles, which could explain the improvement in lower body strength and balance. The slow, gentle, and continuous hand and body gestures associated with Tai Chi Chih also suggest the possibility of enhanced range of motion and upper body muscle power, which could improve flexibility and upper body strength. Practicing Tai Chi Chih twice a week for 1 hr (18 total hours of training) evidently was enough activity to increase stamina/endurance and improve overall physical functional performance. The degree of improvement also may be related to the fact that participants were a fairly robust group of middle-aged women. The mean age of the study participants was 56.5 years. Other trials of Tai Chi Chih with positive effects on physical functional performance also had participants with mean ages of 50 years and older (Chen et al., 2007; Fyre et al., 2007). Moreover, most participants of this study rated their health as good to excellent and reported no physical limitations. Most of the studies mentioned a beneficial effect of Tai Chi on physical function, and in most studies, this conclusion was based on a pre- to post-intervention analysis. Some of the studies also demonstrated that there was lack of evidence on the benefits of Tai Chi on physical function (Logghe et al., 2009). Varied results from different studies may result from the use of different physical function measurements, different research designs, type of Tai Chi practiced, and duration of intervention. One of the major limitations of the study was the use of convenient sampling without random assignment of participants into groups, which caused unequal baseline level in the CS-PFP outcome variables between the comparison and intervention groups. However, one-way ANCOVA using preintervention CF-PFP variable scores as covariates was used to control for these differences to identify between-group differences after the intervention. Moreover, the intervention group was initially less active than the comparison group, so, “being active” may have contributed to a better chance of improvement by the intervention, which may not be a part of the effect of Tai Chi Chih itself. Earlier studies carried out with older participants also resulted in improvements in physical function after practicing Tai Chi. However, the length of the intervention was typically longer than the intervention used in this study. For instance, Fyre et al. (2007) utilized a 12-week intervention while several other studies utilized 6-month Tai Chi programs (Chen et al., 2007; Li et al., 2001). Because of this, these results should only be generalized to healthy middle-aged women. Moreover, since the study population was primarily Caucasian, the results should not be generalized to a more diverse population. Follow-up evaluations to assess the long-term impact of Tai Chi interventions among participants with diverse ethnic and socioeconomic statuses are warranted, and should be done in future studies.
It is important to note that different methods have been developed to assess physical functional performance, such as self-reported questionnaires and performance-based testing. In the previously mentioned studies, Li et al. (2001) and Chen et al. (2007) used self-reported questionnaires to measure physical function, and only one study used performance-based measures (Fyre et al., 2007). Self-reported questionnaires are efficient and inexpensive but they may not provide adequate information about functional limitations, and in healthy, high-functioning respondents, there is a likely ceiling effect, which can limit their effectiveness in identifying change over time. Therefore, performance-based testing may be better, as it gives valid and reliable objective measures of physical function rather than participant perceptions about their level of function (Cress et al., 1995). A strength of this study is that physical function was measured using a performance-based test battery (CS-PFP 10). A particular advantage of this test battery is that it integrates activities that reflect the types of personal, household, and mobility tasks that are necessary to maintain functional independence, thereby reflecting the activities that are routinely classified as ADLs and IADLs.
The threshold CS-PFP TFP score, referred to as physical reserve, has been identified as >57 (Moore-Harrison, Speer, Johnson, & Cress, 2008). Physical reserve is an individual’s physiologic capacity in excess of that required to perform daily tasks (Petrella & Cress, 2004). This acts as a safety margin that helps older adults to maintain their physical function even after they experience changes related to age or disease. The “margin of safety” conceptualized by physical reserve serves as a buffer against unexpected demands or temporary decline in functional performance (Cress & Meyer, 2003). Individuals with CS-PFP score >57 can lose physiological capacity without reducing their functional probability to live independently. For the present study, all the participants had adequate physical reserve in the baseline sample using the >57 benchmark on the TFP score. The comparison group pre-intervention score was 69.1 and the intervention group pre-intervention score was 57.5, which was only slightly above the physical threshold. These scores indicate that members of the comparison group had a higher physical reserve than the Tai Chi group before the intervention. However, after the intervention, the results indicated a significant improvement in the physical reserve in the intervention group. The post-test score of the intervention group was 70.3 with an improvement of 22.3%. These findings indicate that participation in Tai Chi Chih had a positive effect on the physical functional performance and physical reserve of the intervention group. As noted previously, the use of a middle-aged sample makes this study novel, since previous studies mostly focus on women older than 65 years old. This finding supports the value of targeting middle-aged women in an effort to improve functional performance and physical reserve at an age when they still respond relatively quickly to an exercise stimulus that could help them to enter the period of “old age” with more fitness, better balance, and greater physical functional ability.
In conclusion, the findings from this study indicated that participation in Tai Chi Chih class can improve physical functional performance significantly in relatively healthy, community-dwelling middle-aged women. Tai Chi incorporates the advantages of a low-cost and versatile training activity, which could be suggested for older women for the prevention of falls and for middle-aged women as a means of increasing physical activity, enhancing physical function, and improving physical reserve.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.