
Abstract
To better understand the process and outcomes of family involvement for long-term care residents with varying stages of dementia, we analyzed family and staff data for 467 residents of 24 residential care/assisted living and nursing-home settings. Adjusted analyses found that although the amount of family visitation did not significantly vary by resident cognitive status (15 versus 20 visits/month to persons with and without dementia, respectively), the nature of the visit did. Families of cognitively intact residents spent more time in activities related to social and community engagement, such as taking residents on trips and calling and writing letters (p < .001), while families of more impaired residents spent more time on care-related activities, including tasks related to nutrition (p < .027), mobility (p = .001), and discussing care with staff (p = .007), the latter of which was associated with greater burden (p < .001). Staff identified similar patterns but perceived less family involvement.
Introduction
There is little doubt about the importance of families in long-term care settings. Family involvement benefits long-term care residents by reducing risk of infection and hospitalization (Zimmerman, Gruber-Baldini, Hebel, Sloane, & Magaziner, 2002), promoting participation in activities (Dobbs et al., 2005), and preserving quality of life and wellbeing (Greene & Monahan, 1982; Mitchell & Kemp, 2000). Families also benefit by having less emotional and physical fatigue and greater family intimacy (Gaugler, Anderson, Zarit, & Pearlin, 2004). Interventions to enhance family involvement in the long-term care setting have achieved similar positive results and have additionally recognized benefits for long-term care staff (e.g., Partners in Caregiving, Pillemer et al., 2003; Family Involvement in Care, Maas et al., 2004).
Estimates of family visitation—perhaps the most common and fundamental measure of family involvement—vary widely, and suggest that between 23% and 76% of residents receive family visitors at least weekly (Bitzan & Kruzich, 1990; Hopp, 1999; Tornatore & Grant, 2002). The amount of family involvement does not significantly vary by either long-term care type (e.g., residential care/assisted living [RC/AL] or nursing home [NH]; Port et al., 2005) or resident-dementia status (Dempsey and Pruchno, 1993; Zimmerman et al., 2005; cf. Port et al. 2001).
Although the amount of family involvement may not vary by dementia status, one would expect the nature of this involvement to vary by necessity. For example, it may be expected that families of residents with dementia might spend less time doing recreational activities than families of residents without dementia. Beyond expectations, however, a review of the literature yielded little information about how resident-dementia status relates to the nature of family involvement. One study of residents with dementia found that the most common forms of family involvement were visiting or taking the resident on trips outside the long-term care setting (11 times per month); monitoring wellbeing and care (6-7 times per month); and calling on the telephone and writing letters (6 times per month; Port et al., 2005). This type of involvement is consistent with what families have identified as “their” responsibilities; other family-owned responsibilities include managing resident finances, shopping, and decorating the resident’s space (Dempsey & Pruchno, 1993). Families overwhelmingly identify more care-oriented tasks, such as helping the resident to eat, bathe, dress, and toilet, as the responsibility of the staff (Dempsey & Pruchno, 1993; Natan, 2009). This distribution of responsibility is similar to that reported by Bowers (1988), who additionally determined that although families hold staff accountable for the actual performance of most care-oriented tasks, they hold themselves responsible for monitoring and evaluating the thoroughness and quality of the care provided. This family responsibility translates into families teaching staff how to provide care in accordance with personal preferences and standards, filling in when staff fail to meet these standards, and providing care themselves (Bowers, 1988).
Although such an oversight role may seem straightforward, family caregivers commonly experience stress and care-giving burden when they act in this capacity in the long-term care setting (Friedemann, Montgomery, Maiberger, & Smith, 1997; Ryan & Scullion, 2000). Indeed, family caregiver stress and burden do not end with long-term care placement. For families who stay involved post-placement, in addition to the stress of oversight, other sources of stress include perceived responsibility for resident care, especially as related to instrumental activities of daily living (Gaugler & Kane, 2007); financial burden (Williams et al., 2008); difficulty communicating with staff caregivers (Friedemann et al., 1997); and role ambiguity (Whitlatch, Schur, Noelker, Ejaz, & Looman, 2001).
So as to better understand these and other types of family involvement for residents with varying stages of dementia in long-term care settings, this manuscript analyzes baseline data derived from a group-randomized trial of Families Matter, an intervention to improve resident, family, and staff outcomes by supporting families in identifying and creating roles for themselves within the long-term care setting. These data address family involvement from the family and staff perspective and examine the specific activities in which families engage. We expected that the nature of family engagement would differ in relation to resident-cognitive status, and perhaps by respondents (i.e., family versus staff), because staff are not likely aware of all the times and ways that families are involved. This manuscript also offers insights into the relationship between family involvement and burden. Better understanding the process and outcomes of real and perceived family involvement in long-term care, and how these relate to resident-dementia status, may help inform and craft future programs and interventions in these settings.
Method
All study materials and procedures were reviewed and approved by the Institutional Review Boards of the University of North Carolina at Chapel Hill and Duke University.
Setting
Participating NH (n = 6) and RC/AL settings (n = 18) were members of the Collaborative Studies of Long-term Care located within an approximately 1-hr drive of the project office (Zimmerman et al., 2001). Eligible settings had a minimum of 50 beds (so as to ensure that the desired sample size was available), and administration agreed to be randomized into either condition of the trial.
Subjects
A random sample of approximately 20 eligible family caregivers was enrolled per setting. Eligible family caregivers were English speakers, at least 18 years of age, who visited a resident at least monthly, and were identified by the administration as the individual who best knew the resident. For each enrolled family caregiver, the direct care worker who best knew the paired resident was identified; this direct care worker was at least 18 years of age, worked a minimum of 20 hr/week during the morning or afternoon shift, and had worked in the setting at least 1 month prior. Families were mailed an invitation letter and were then contacted by telephone to explain the study, invite participation, and obtain informed consent. Staff members were approached and consent obtained in person. Of the eligible families and staff members invited to participate, 78% of families and 99% of staff provided informed consent and enrolled in the study.
Data Collection
Family caregivers were interviewed by telephone, and staff members were interviewed in person. Family caregivers provided descriptive data about themselves and the resident and additionally provided information about their involvement in the setting and their feelings of care-giving burden. Staff members provided descriptive data about themselves and cognitive and functional data about residents and also reported family involvement with individual residents. Thus, for each resident, families and staff independently provided data about family involvement. Family (n = 467) provided data about only one resident; at times, one staff member reported on more than one resident (i.e., one staff member reported on four residents; three staff members reported on three residents; 77 staff members reported on two residents; and 300 staff members reported on one resident). A total of 381 staff members provided data about residents.
Measures
Descriptive information was obtained about the resident (e.g., age, years in setting, functional and cognitive status), family (e.g., age, relationship to resident, employment status), and staff (e.g., age, race, years of experience). Other measures included the following:
Cognitive status
For each resident with whom they were paired, staff members completed the Minimum Data Set Cognition Scale (MDS-COGS), a nine-item measure that asks about short- and long-term memory; awareness of surroundings; decision making; understanding; and ability to dress oneself over the past 7 days (i.e., a functional task). The theoretical score range is from 0 to 10. Accepted score cut points are 0 to 1 no cognitive impairment; 2 to 4 mild cognitive impairment; and 5 to 10 severe cognitive impairment. The MDS-COGS has acceptable sensitivity (.49-.95) and specificity (.84-1.0) across samples, informants, and against varying gold standards (Hartmaier, Sloane, Guess, & Koch, 1994; Zimmerman et al., 2007).
Functional status
Staff members also reported resident independence in activities of daily living per the MDS–Activities of Daily Living Scale (MDS-ADL; Morris, Fries, & Morris, 1999). The MDS-ADL assesses resident’s level of independence in performing daily tasks related to continence, transfer, and personal care. Resident independence in performing instrumental tasks of daily living (e.g., managing medications and finances, shopping, cleaning) was measured using a modified version of the Instrumental Activities of Daily Living scale (IADL; Lawton & Brody, 1969).
Family involvement
Involvement in 12 areas was reported by family and staff for each resident, using a modified version of Murphy et al.’s (2000) Involvement scale, which assesses involvement in various care activities, such as calling and writing letters, doing resident laundry, helping the resident walk or move around, playing games and conversing, and monitoring finances. Family and staff reported the numerical (i.e., continuous) and categorical (e.g., seldom, often) frequency of each activity during the past month. For example, family were asked both, “In the last month, have many times did you visit your mother?” and “In the last month, would you say that you visited your mother seldom, sometimes, fairly often, or often?” Staff were similarly asked, “In the last month, how many times did Mrs. Jones’ family visit her?” and “In the last month, would you say that Mrs. Jones’ family visited her seldom, sometimes, fairly often, or often?”
Family burden
Family caregivers reported care-giving burden using the 22-item version of the Zarit Burden Interview (ZBI; Zarit, Reever, & Bach-Peterson, 1980). Scores on the ZBI range from 0 to 88, with higher scores indicative of greater care-giving burden. The scale displays good internal consistency, alpha = .89 (Zarit, Antony, & Boutselis, 1987).
Analyses
Tests for differences in characteristics among residents with different levels of cognitive impairment and among their respective family members were performed using linear and nonlinear mixed models, with a random effect for site. Although the reported frequencies of involvement are summarized in tables with means and standard deviations, analyses comparing frequencies across levels of dementia (Table 2 left-hand columns) are based on grouping the reported frequencies for each type of involvement into ordered categories. This was done because the frequencies were not normally distributed, being positively skewed and clustered around a small number of values (e.g., 1 to denote once per month; 4 to denote once per week; 30 to denote once per day). Frequencies were grouped into categories such that each category contained approximately equal numbers of respondents and was bound by natural breaks in the frequency counts for that activity. For example, the four categories for “visiting” translated roughly to once per week; 2 to 3 times per week; every other day; and daily. These data were analyzed using a SAS macro that implements a generalized estimating equation (GEE) analysis of categorical ordinal data and produces robust variance estimates to minimize Type II error (Lipsitz, Kim, & Zhao, 1994); for these, the created ordinal variables were response variables and the resident’s dementia status was the predictor variable. A similar approach was used to analyze the relationship of the categorically reported frequencies of involvement with dementia level (Table 3). The Wilcoxon matched-pair signed-ranks test was used to examine whether family and staff differed in their reports of the frequency of family-member involvement (Table 2, right-hand columns). Linear mixed models were used to analyze the relationship of frequency of involvement with burden (Table 4); for these, the Zarit Burden Inventory score was the response variable and the ordered categories of frequency for each type of involvement were used as predictor variables, controlling for resident dementia level.
Results
All settings were for-profit; they averaged 88 beds, and had 51% and 47% of residents with dementia and receiving Medicaid, respectively (see Table 1). At baseline, 467 family caregivers and 381 staff members provided data about themselves and their paired resident (n = 467). Approximately 28% (n = 132) of the residents had severe dementia, 25% (n = 115) mild/moderate dementia, and 47% (n = 220) no dementia (see Table 1). Residents averaged 81 years of age (SD = 12 years), were primarily female (75%), and had spent an average 2.4 years (SD = 2.5 years) in the setting. These characteristics did not significantly vary by dementia status. Residents with severe dementia were significantly more impaired in MDS-ADL and IADL scores than their less cognitively impaired counterparts and were also more likely to reside in NHs (p < .001). Family caregivers averaged 58 years of age (SD = 11 years), were primarily female (73%), White (75%), and generally were not employed fulltime (55%). The family characteristics that significantly differed as a function of resident-dementia status were age (p = .01) and fulltime employment (p = .05).
Characteristics of Settings and Staff Caregivers (Overall), and of Residents and Family Caregivers, as a Function of Resident Dementia Status a .
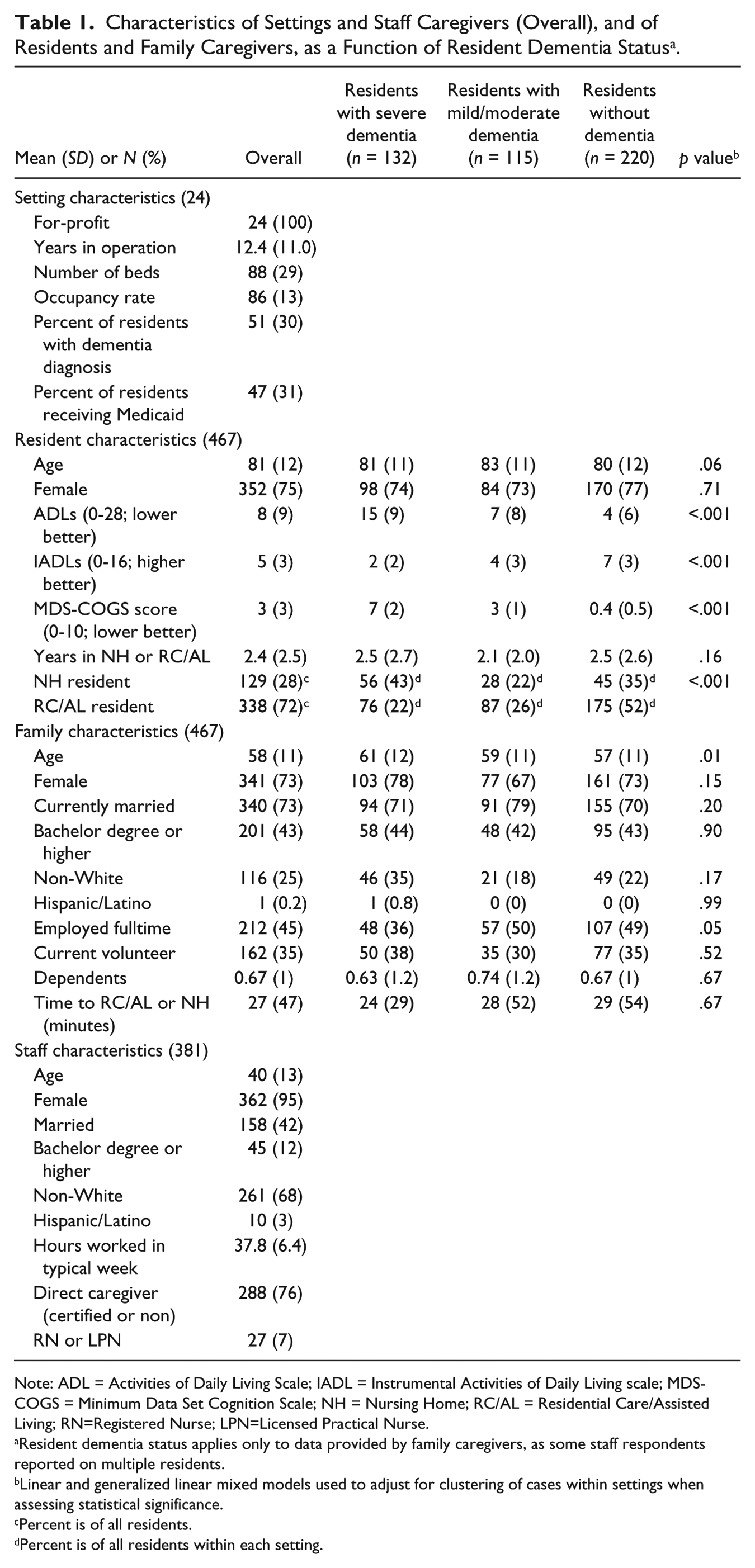
Note: ADL = Activities of Daily Living Scale; IADL = Instrumental Activities of Daily Living scale; MDS-COGS = Minimum Data Set Cognition Scale; NH = Nursing Home; RC/AL = Residential Care/Assisted Living; RN=Registered Nurse; LPN=Licensed Practical Nurse.
Resident dementia status applies only to data provided by family caregivers, as some staff respondents reported on multiple residents.
Linear and generalized linear mixed models used to adjust for clustering of cases within settings when assessing statistical significance.
Percent is of all residents.
Percent is of all residents within each setting.
Staff respondents averaged 40 years of age (SD = 13 years), were primarily female (95%), non-White (68%), and were best classified as a direct caregiver (78%; includes certified nursing assistants, nursing assistants, and nurse aides).
As shown in Table 2, neither families nor staff reported a difference in the number of family visits as a function of resident dementia. Families reported visiting residents between 15 (no dementia) and 20 (severe dementia) times per month, whereas staff reported between 10 (no dementia) and 13 (severe dementia) visits per month. Across all levels of resident dementia, families reported greater family visitation than did staff (i.e., families reported between 5 and 7 more visits per month than staff; p < .001).
Family and Staff Perceptions of Family Involvement in the Previous Month, for Residents With Severe Dementia (Sev), Mild/Moderate Dementia (M/M), and Without Dementia (None).
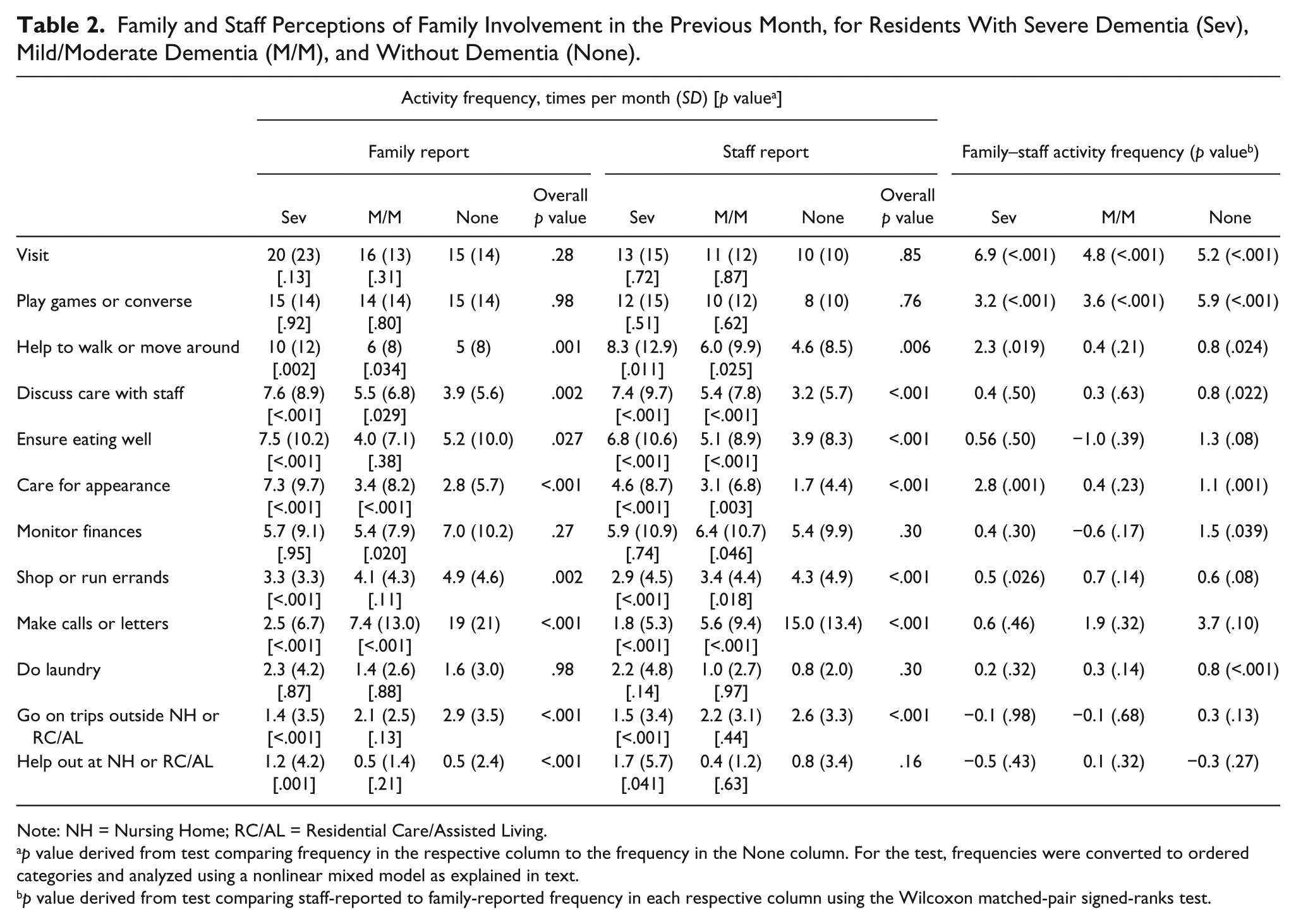
Note: NH = Nursing Home; RC/AL = Residential Care/Assisted Living.
p value derived from test comparing frequency in the respective column to the frequency in the None column. For the test, frequencies were converted to ordered categories and analyzed using a nonlinear mixed model as explained in text.
p value derived from test comparing staff-reported to family-reported frequency in each respective column using the Wilcoxon matched-pair signed-ranks test.
Consistent with staff report, families of residents with dementia reported spending significantly less time than families of residents without dementia on activities including shopping and running errands (per family report, only for severe dementia; p < .001); making phone calls or writing letters (p < .001); and going on trips outside the NH or RC/AL setting (severe dementia only; p < .001). Also consistent with staff report, families of residents with dementia reported spending significantly more time helping the resident walk or move around (p < .05); discussing resident care with staff (p < .05); ensuring the resident was eating well (not significant for families of residents with mild/moderate dementia; p < .001 for other family and staff comparisons); caring for resident’s appearance (p < .01); and, for residents with severe dementia only, helping out around the RC/AL or NH (p < .05). There were no differences by dementia status or respondent in relation to doing laundry or playing games or conversing, but families of residents with mild/moderate dementia reported less often monitoring finances than those of residents without dementia (p = .02).
Staff reported that families of residents without dementia spent less time than families reported on several activities, including playing games or conversing (p < .001); helping the resident walk or move around (p = .02); discussing care with staff (p = .02); caring for resident’s appearance (p = .001); monitoring resident finances (p = .04); and doing resident laundry (p < .001). Staff reported that families of residents with dementia spent significantly less time than families reported playing games or conversing (p < .001); helping the resident move or walk around (severe dementia only; p = .02); caring for the resident’s appearance (severe dementia only; p = .001); and shopping or running errands (severe dementia only; p = .03).
Table 3 displays the median number of times that families reported participating in different activities as a function of whether they considered their involvement to be seldom/sometimes, fairly often, or often. The categorization of an activity significantly varied by activity type (p < .001). For example, a median frequency of 30 times per month was associated with “Often” for making calls or writing letters, whereas a median frequency of 4 times a month was categorized as “Often” for going on trips outside the NH or RC/AL setting. For all activities, an increased frequency related to an increased perception of involvement (e.g., frequency of visits increased from 3 to 8 to 15 as perception of involvement increased).
Family Caregiver Reported Frequency of Monthly Participation in Activities as a Function of Reported Categorical Involvement (n = 467).
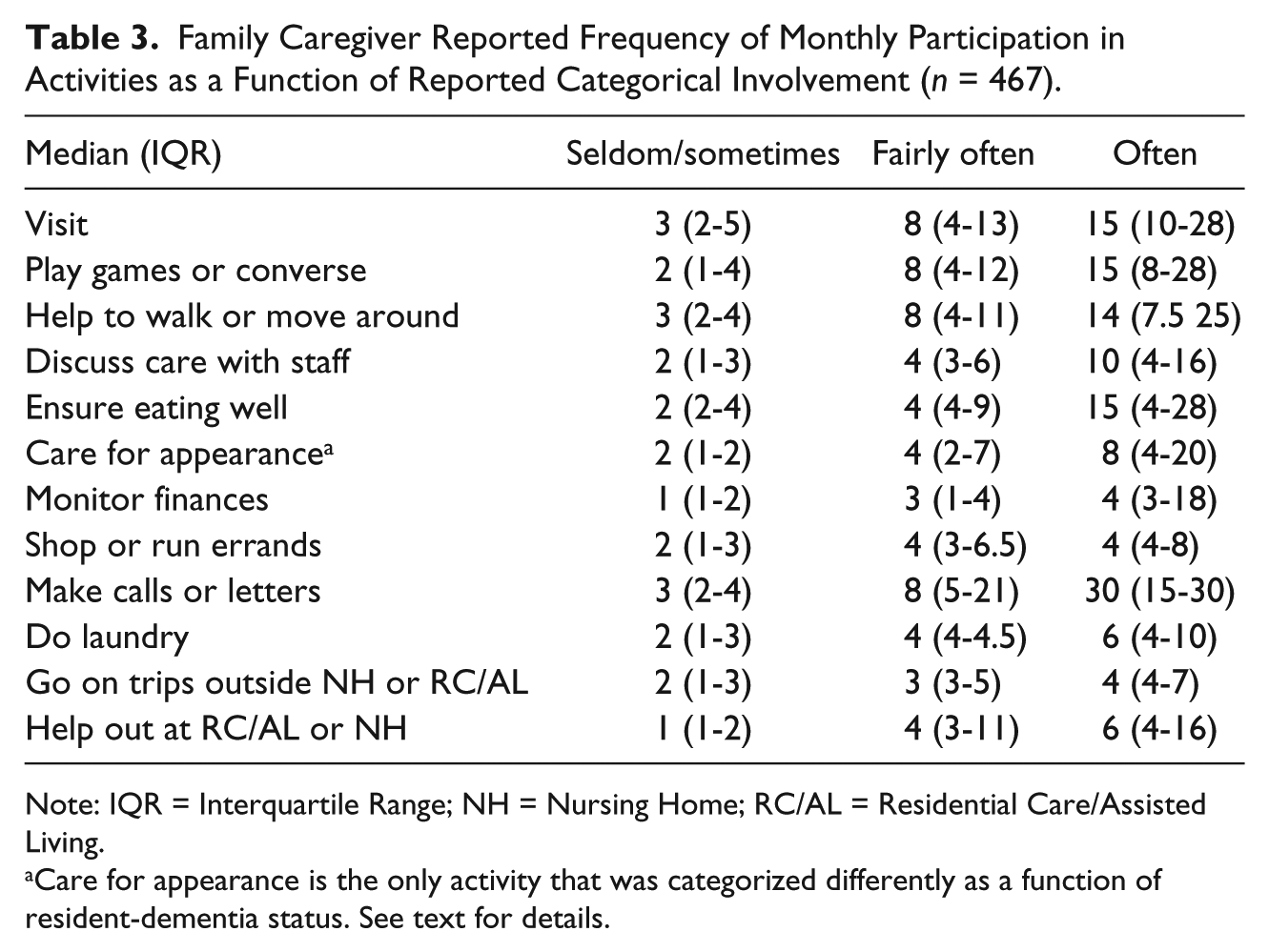
Note: IQR = Interquartile Range; NH = Nursing Home; RC/AL = Residential Care/Assisted Living.
Care for appearance is the only activity that was categorized differently as a function of resident-dementia status. See text for details.
Categorizations did not significantly vary by resident-dementia status, except for caring for the resident’s appearance. In this case, a perception of “Often” translated to a median frequency of 4 for residents without dementia, 5 for those with mild/moderate dementia, and 15 for those with severe dementia (test-wise p = .02; no versus mild/moderate dementia, p = .004; mild/moderate versus severe dementia, p < .001).
As shown in Table 4, higher family-reported frequency of discussing care with staff (p =.007), monitoring resident finances (p < .001), shopping or running errands (p < .001), and making calls and writing letters (p = .019) was significantly associated with increased family burden.
Relationship Between Frequency of Monthly Participation in Activities and Burden a .
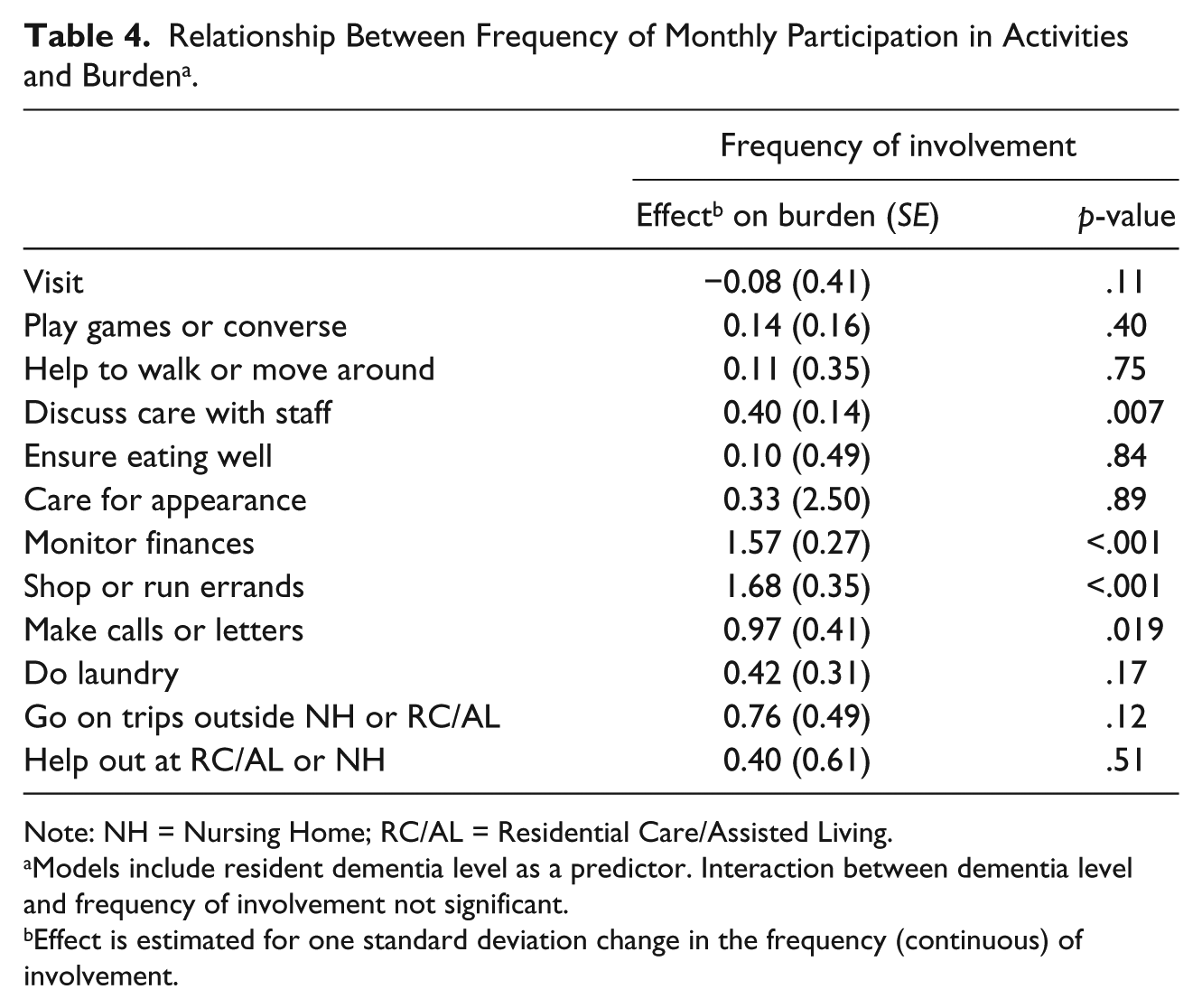
Note: NH = Nursing Home; RC/AL = Residential Care/Assisted Living.
Models include resident dementia level as a predictor. Interaction between dementia level and frequency of involvement not significant.
Effect is estimated for one standard deviation change in the frequency (continuous) of involvement.
Discussion
Our results show that families make between 15 (to residents with no dementia) and 20 (to residents with severe dementia) visits each month, and that the number of visits does not significantly differ by resident-cognitive status. What seems to be affected by cognitive status, however, and advances our understanding of family involvement in these settings is what family members are doing during these visits. While families of cognitively intact residents spend more time in activities related to social and community engagement, such as by taking the resident on trips, calling and writing letters, and shopping or running errands, families of residents with dementia instead spend more time on activities to support resident care. These families are more likely to spend time engaging in activities to promote resident nutrition, mobility, and appearance and to discuss care with staff.
Although families of residents with dementia may well adopt new care-giving roles as the disease progresses, it is worth noting that these care-giving tasks are those that families historically have identified as the responsibility of staff (Dempsey & Pruchno, 1993). It may be that in recent years, families have come to recognize that they are care partners with long-term staff. What is not known, however, is whether families choose (either from desire, obligation, perceived resident need, or insufficient care) to participate in these activities. While recent years may well have brought a change in family attitudes coincident with “culture change” in long-term care (Koren, 2010), it is worth noting that in earlier work, families who provided care responsive to perceived ADL and IADL needs were less satisfied, suggesting that families respond to inadequate care (Levy-Storms & Miller-Martinez, 2005). Previous data indicate that increased resident impairment is a source of dissatisfaction, just as substandard care—and the subsequent perceived responsibility for providing hands-on care—is a source of stress for family caregivers (Dobbs & Montgomery, 2005; Givens, Lopez, Mazor, & Mitchell, 2011).
Indeed, families reporting more involvement in some activities experienced greater burden. Specifically, with an increase in family involvement in discussing resident care with staff, monitoring resident finances, shopping or running errands, and making calls and writing letters, families reported significantly greater burden. Two of these more burdensome activities (shopping or running errands and making calls and writing letters) were more often done by families of residents without dementia, suggesting that burden is shared by family caregivers of less impaired residents, as well. These caregivers in our sample were significantly younger and more likely to be employed fulltime than those of residents with more severe dementia; thus, the juggling of multiple responsibilities may have made these caregivers especially vulnerable to burden.
Two of the activities related to burden are primarily those of monitoring and providing oversight (discussing resident care with staff and monitoring resident finances), supporting previous suggestions that these tasks—which may not fit well within a “visitor” model of long-term care—are especially stressful to families (Friedemann et al., 1997; Ryan & Scullion, 2000). Williams and colleagues found a similar relationship for staff discussions and theorized that more discussions about resident care with staff may be stressful to family caregivers due to the negative circumstances (e.g., illness or pending death) around which increased discussions about resident care often occur (Williams et al., 2008). In terms of monitoring resident finances, significantly increased involvement was reported only by families of residents with mild/moderate dementia. Presumably, residents with no dementia are more able to manage their own finances or at least participate in financial oversight, and, given that those with severe dementia were more likely to reside in NH settings, they simply had fewer finances to manage. By knowing the activities and circumstances that create burden, families and those who support them can better plan for their involvement, and when involvement itself cannot be attenuated, then additional support should be provided.
Not surprisingly, staff members consistently reported that families visit and take part in all activities to a lesser extent than what the families themselves reported. This finding is expected, given that staff members cannot conceivably accurately report the activities of a cadre of family caregivers, especially when not all staff members’ working hours correspond to all family members’ visiting hours. Regardless the reason, incongruous beliefs between family and staff caregivers about what one or the other is doing may produce unfavorable conditions for building trusting and respectful relationships. The existent interventions designed to improve family involvement and family and staff relations (e.g., Partners in Caregiving, Pillemer et al., 2003; Family Involvement in Care, Maas et al., 2004; Majerovitz, Mollett, & Rudder, 2009) address better communication between staff and families but do not explicitly focus on how these more subtle perceptions of roles, accountability, and task burden may influence relationships. More transparency of the others’ roles and involvement might foster more a sense of caregiver partnership. Such transparency might also increase each group’s accountability (such as if a family member knows that the staff are aware if they are present) and enhance perceptions of being respected and appreciated by the other (such as if a staff member is proud of work he/she did that day, knowing that the family will be there to see it and implicitly—if not explicitly—acknowledge the staff member’s efforts).
It is important to keep in mind that negative perceptions about poor care are not only held by families about staff members; they are also maintained by staff members about families and can contribute to conflict and staff burnout (Abrahamson, Suitor, & Pillemer, 2009; Berdes & Eckert, 2007). The aforementioned, current, and future programs to promote family involvement and staff and family interaction should consider these perceptions as part of design and implementation. These programs might, for example, incorporate weekly communication (verbal or written) so as to better convey involvement, improve perceptions, and elicit (and correct, if needed) each group’s perceptions of the other’s involvement on an ongoing and routine basis.
Our conclusions are subject to some limitations, namely those of generalizability and interpretation. The 24 settings were all within the state of North Carolina, and all had 50 or more resident beds. Although there is no a priori reason to expect that amount of family involvement differs by state, it might well vary by setting type and size; in addition, one might expect that the ways in which families are involved differ as a function of these characteristics. As one consideration, RC/AL staffing levels and responsibilities vary by state and setting size, so the extent to which families participate in activities to fill a perceived void, their involvement and related burden may vary as well. In addition, families who did not visit the setting at least once a month were ineligible for participation, and thus we cannot speak to the level, type, or burden of involvement for those who visit infrequently. In terms of interpretation, residents with dementia experience cognitive and functional deficits, and so it is not clear whether family involvement was responsive to one or the other of these deficits, or to another resident or family characteristic.
Regardless, our findings show that in a large sample of long-term care families and residents, family involvement in RC/AL and NH settings does not differ as a function of resident-dementia status, but the nature of the involvement does. Families of cognitively intact residents spend more time in activities related to social and community engagement, while those of residents with dementia instead spend more time on activities to support resident care. Because families are more sensitive to—and in some cases burdened by—involvement in some types of activities, any interventions to increase family involvement in the long-term care setting should consider these findings as part of implementation efforts.
Footnotes
Acknowledgements
The authors express appreciation for the involvement of the staff, residents, and families participating in the Collaborative Studies of Long-term Care and their efforts to improve care and outcomes in long-term care.
Author’s Note
The grantor had no role in the study design or conduct, or in the collection, analysis, interpretation, or reporting of these data.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the National Institutes of Health (R01AG025443).
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.