
Abstract
Informal older adult caregiving allows older adults to stay in their homes or live with loved ones, but decisions surrounding older adult care are fraught with complexities. Related research and case law suggest that an older adult’s need for and refusal of help are important considerations; the current study is the first to examine these factors experimentally. Two samples (potential caregivers and care recipients) provided responses regarding anticipated emotions, caregiver abilities, and allocation of daily caregiving decision making based on a vignette portraying an older adult who had a high or low level of autonomy and who accepted or refused help. Study findings suggest differing views about caregiving; potential caregivers may not be as well prepared to take on caregiving as the potential care recipients anticipate and potential caregivers may allocate more decisional responsibility to older adults than the care recipients expect. Implications for older adult abuse are discussed.
As the population ages and medical innovations prolong life expectancies (Kung, Hoyert, Xu, & Murphy, 2008), older adults and their family members face an increasing number of legally important, yet emotionally taxing, decisions about older adult abilities and care. Such decisions involve determining where the older adult will live, whether the older adult needs a legal guardian, and how to manage day-to-day responsibilities. Managing these decisions as older adults become more impaired may lead to increased caregiver stress (Starrels, Ingersoll-Dayton, Dowler, & Neal, 1997) and in extreme cases, uninformed or improper decision making could lead to other- or self-neglect of the older adult (People v. Simester, 1997; Peterson v. Florida, 2000; Sieniarecki v. Florida, 2000).
State statutes and case law concerning older adult maltreatment are based on assumptions that caregivers make well-considered, rational decisions about whether and how to provide care for older adults. Oftentimes, these statutes are modeled after laws meant to protect children (Brank, Wylie, & Hamm, 2012), but the statutes do not address the complex array of factors that are involved in older adult caregiving. In fact, an older adult’s personal characteristics are likely to influence the care recipients’ and caregivers’ perspectives on caregiving in specific ways. We examined two such personal characteristics of the older adult: level of autonomy and refusal of help. Furthermore, we examined anticipated emotions because predictions about how one might feel in a caregiving situation will likely influence decision making.
Legal Issues in Older Adult Caregiving
When a parent brings a newborn baby home from the hospital or signs a set of adoption papers, it is clear that the parent is taking on caregiving responsibilities for that child. Under typical conditions, the child will require less care over time as the child becomes more autonomous. State statutes provide guidance as to when, over the child’s life course, the child should acquire adult responsibilities (e.g., voting, enlisting in military). Furthermore, state statutes also define when a child is considered a legally autonomous adult capable of making informed and voluntary decisions (Gardner, 2009).
In contrast, taking on the caregiving role for an older adult often occurs gradually without a specific moment when the older adult clearly “needs” care (Wylie & Brank, 2009). Unlike the distinct age at which a child becomes a legally competent adult, there is no distinct age at which a person becomes a legally incompetent adult—if such status ever occurs. Often medical conditions (e.g., broken hip) lead to a short-term recovery plan that transpires into a long-term caregiving situation (Albert, Moss, & Lawton, 1996; Wylie & Brank, 2009). Caring for an older adult can also be less clear than caring for a child because older adults may at times need more extensive care than at other times (Ford et al., 2000) and may need care for certain tasks, but not others (Hilton, Kopera-Frye, & Krave, 2009). Moreover, caregivers are handling more medical responsibilities and decisions (e.g., deciding whether an older adult needs medical attention) than ever before (O’Mara, 2005).
To compound the uncertainty surrounding how long and how much care might be needed, people age and become less autonomous at varying rates (Ford et al., 2000) making it extremely difficult to construct a universally accepted standard for when an older adult needs care. The sometimes gradual, occasionally sporadic degeneration of physical and mental capabilities complicates caregivers’ and older adults’ ability to know precisely when simple helping turns into “official” caregiving. Thus, a person may not be identified as the caregiver or legally determined as a guardian, which means that caregiving responsibilities may not be clearly defined possibly leading to neglect (Wylie & Brank, 2009).
A number of states have caregiver statutes included within their vulnerable person abuse and neglect laws; however, states differ in their statutory and regulatory definitions. Where some states provide definitions that are detailed and specific, other states’ statutes are brief and vague. Underlying these caregiver statutes are assumptions that laypeople are knowledgeable about physical and mental impairments. Consider the Illinois law stating that a person “reasonably should know of such person’s physical or mental impairment and knows or reasonably should know that such person is unable to adequately provide for his own health and personal care” (Aging Elder Abuse and Neglect Act, 320 ILCS 20/2, 2010). Such statutory language indicates that those interacting with older adults as caregivers must decide whether they have the medical, financial, emotional, and physical abilities to be a caregiver. Subsequent caregiving decisions will range from the mundane (e.g., what clothing the older adult should wear) to more serious (e.g., how much medication to administer). Ideally, these decisions would be based on the potential caregivers’ perceived ability to provide requisite care; however, other factors are likely to interfere in this decision making.
Factors That May Influence Older Adult Caregiving Decisions
Older Adult Characteristics
Taking care of an older adult is certainly a prosocial behavior, but it may not easily fit within traditional conceptualizations of prosocial explanations. Most social-psychological research on prosocial helping behaviors is focused on the behavior of strangers in short-term help-giving situations rather than long-term caregiving behaviors between people in close relationships (Wood & Eagly, 2010). Nonetheless, people in caregiving situations, like in general helping situations, likely try to maximize the ratio of social costs to social rewards. One way to minimize social costs when helping is to help only the “deserving.” Therefore, whether a person chooses to help another person may be partially dependent on the help-recipient’s deservingness of such help. Older adult caregiving case law (People v. Simester, 1997; Peterson v. Florida, 2000; Sieniarecki v. Florida, 2000) demonstrates that such perceptions of deservingness may be related to how much help is needed and whether such help is accepted or refused by the older adult.
Older adult autonomy
Albert and colleagues (1996) investigated family caregivers varying thresholds for deciding when they became “caregivers” and were no longer just “occasional helpers.” By retrospectively asking current caregivers’ when their caregiving duties began, the findings show that self-perceived start of caregiving differed greatly across caregivers, and that level of older adult autonomy was a defining factor for commencement of caregiving across all caregivers. Relatedly, Cicirelli (2000) found that in caregiving dyads, caregivers appeared to “move to the next stage” and viewed themselves as the caregiver in relation to the older adult care recipient’s level of functioning.
Limitations in activities of daily living (e.g., eating, bathing, and dressing) that many older adults experience are known to exacerbate caregiver difficulties (Katz, 1983). Such limitations are related to caregiver burnout (Won & Song, 2012), psychological distress (Lou, Kwan, Leung, & Chi, 2011), and general burden (Savundranayagam & Montgomery, 2010). Therefore, the more help an older adult needs, the more difficult it may be for the caregiver to provide that care because of the stressors, or social costs, it places on the caregiver. Although honoring an older adult’s autonomy is known to improve their quality of life (Ford et al., 2000), upholding such autonomy when an older adult actually needs care could lead to unintentional neglect of the older adult. Notwithstanding the confusing balance between paternalism and autonomy, a majority of people indicate that they would care for an elderly relative because of their respect for the relative (Dellman-Jenkins & Brittain, 2003; Ohuche & Littrell, 1989) or moral obligations they feel toward the relative (Bracci, 2000; Pakula, 2005; Wolfson, Handfield-Jones, Glass, McClaran, & Keyserlingk, 1993).
Acceptance or refusal of help
In Peterson v. Florida (2000), the older adult neglect victim was described as “cranky and hard to deal with” (p. 863). Similarly, in People v. Simester (1997), the defendant described the victim as “generally grumpy” (p. 841). In both cases, the defendant familial caregivers cited the older adult’s refusal of help as evidence that the older adult’s injuries were the result of self-neglect on the part of the older adult. For example, in Peterson, a witness’s testimony stated that the older adult victim “always kept himself in an unkempt condition” (p. 841), and in Sieniarecki v. Florida (2000), the defendant daughter, Theresa, testified that whenever it was suggested to her mother, Patricia, a disabled person, that she should go to a doctor, Patricia would yell in disagreement. In addition to refusing doctor visits, Patricia was said to refuse food and other daily care. A jury found Theresa guilty of neglect of a disabled adult after Patricia died of septicemia that occurred because of malnutrition, among other ailments. On appeal, Theresa argued, among other things, that her mother refused medical treatment and holding Theresa responsible for neglect would violate Patricia’s constitutional privacy rights. The Florida Supreme Court dismissed this claim with the others, noting that constitutional rights are personal and cannot be asserted vicariously.
These case examples illustrate how the personal characteristics of the older adult may lead to confusion in caregiving decisions. Refusal of help could be misconstrued as the care recipient’s decision to forego additional measures to prolong life, which is protected under the common law doctrine of bodily self-determination (Cruzan v. Director of Missouri Department of Health, 1990). In sum, there are several legal factors that should be considered when taking on the day-to-day caregiving role; however, because of uncertainties surrounding caregiving, it is unlikely that potential caregivers will weigh legal implications when assuming this role. Vague caregiving statutes and lack of awareness of such laws may be one explanation for not considering the legal implications. Another reason may be that these decisions often elicit conflicting and strong emotional reactions.
Emotions and Caregiving
Clearly, caregiver decisions, such as deciding whether to live with an older adult or how much autonomy an older adult should have, are fraught with difficulties. Unfortunately, the other layer of complexity is that these decisions are often based not only on multifaceted and powerful current emotions (Donorfio & Kellett, 2006) but also on the anticipation of emotions. Mellers, Schwartz, and Ritov’s (1999) theory of anticipated emotion suggests that people make decisions based on how they anticipate they will feel about outcomes. Anticipated emotions are particularly relevant to older adult caregiving decisions because older adults and caregivers may enter caregiving relationships—or short-term living arrangements that develop into long-term caregiving relationships—based on how they think they will feel in the future.
To further complicate matters, the conflicting emotions of guilt, anger, and compassion are among the emotions caregivers experience (Donorfio & Kellett, 2006). In fact, Lyonette and Yardley (2003) found that current female caregivers are motivated by both extrinsic factors (e.g., guilt, lack of choice, perceived disappointment from others) and intrinsic factors (e.g., desire to care, compassion), with extrinsic factors being more influential. When controlling for other variables, motivation by extrinsic factors, such as guilt, was the strongest predictor of caregiver stress. These results suggest that a person may take on caregiving roles to avoid guilt, yet such a motivation is likely to result in more caregiver stress and potentially a poorer relationship with the older adult. Similar to guilt, the emotion of anger may be related to poor outcomes for caregivers or care recipient maltreatment. For instance, MacNeil and colleagues (2010) found that a caregiver’s anger level was most predictive of caregiver anxiety, depression, and resentment on quality of care provided by the caregiver. Even non-illegal, yet potentially harmful behaviors (e.g., threatening to send the older adult to a nursing home, handling the older adult somewhat roughly) are related to caregiver anger (MacNeil et al., 2010). Of the studies that have explored the role of anticipatory emotions in caregiving decisions, most have focused on caregivers who are actively involved in a current caregiver role and their predicted emotions as that caregiving role continues. For those few studies that have examined anticipatory emotions as they relate to potential caregiving, all have broadly focused on general feelings of anxiety about providing care and how feelings of anxiety may differ according to participant attitudes and personality characteristics (Conway-Turner & Karasik, 1993; Laditka & Pappas-Rogich, 2001; Sorensen, 1998). No study has more specifically examined the important role of anticipatory emotions on caregivers and care recipients as they consider taking on caregiving roles.
The Present Research
Decision making about the caregiving relationship can have serious legal and health consequences, yet we know little about the way in which family members consider informal caregiving before they enter into the relationship. The present study examined both potential caregiver and care recipient perspectives. We included participants who could potentially enter these roles, instead of people currently in these roles to shift the attention away from how caregivers experience the actual caregiving situation once it is in place (and respond retroactively) and instead focus on the decision-making process that leads to older adult informal caregiving situations.
We examined these issues experimentally with a sample of potential caregivers and care recipients focusing on two primary research questions:
We hypothesize the two samples and experimentally manipulated personal characteristics of the described older adult will predict perceived ability and daily caregiving decision making such that the potential care recipients will view the potential caregivers as better able to provide care and make daily caregiving decisions than the caregivers view themselves. Case law has demonstrated that refusal of help by an older adult can result in lower levels of caregiving with daily living needs; therefore, we hypothesize that refusal of help will predict lower levels of daily caregiving decision making, but not directly influence perceived abilities. Given the role emotions play in these decisions, we hypothesize the anticipated emotions of anger, compassion, and guilt to predict perceived ability to provide care and allocation of daily caregiving decision making, with guilt being a particularly powerful predictor for both potential care recipients and potential caregivers.
Method
Participants and procedures
The study included a total of 195 participants with an online sample of potential caregivers (n = 90, M = 41.32 years old, SD = 10.68, 76% female) and a sample of potential care recipients (n = 105, M = 71.96 years old, SD = 7.99, 72% female). All study procedures were approved by the authors’ university Institutional Review Board. The potential caregiver sample was recruited from a national U.S. sample of adults registered with a social science web survey distribution website. Internet-based samples tend to include more middle-aged men (Hewson, Laurent, & Vogel, 1996; O’Neil & Penrod, 2001) and caregivers tend to be more middle-aged women (Brody, 1990); therefore, we oversampled women to increase the representativeness in the sample. Participants in the online sample were randomly assigned to one of four conditions in which they read one vignette that included two manipulated variables (see Appendix). Following the vignette, participants answered manipulation check questions and measures described below. Those who participated in the study were either entered into a drawing to win a US$50.00 gift card for online shopping or paid US$5.00 for participation. 1
The potential care recipient sample was recruited from an older adult community participant pool managed in an urban Midwestern city. Research assistants met the participant in a location that was convenient to the participant such as a senior center or the participant’s home. Those who participated were entered into a drawing to win one of eight grocery store gift cards valued at US$20. All other procedures were the same as described above.
The original sample size included 300 participants (potential caregiver/non-older adults = 175; potential care recipient/older adult = 125). For the potential caregiver sample, participants were removed if they spent either fewer than 8 min or more than 60 min on the online survey (n = 68). The majority of these closed their browser before beginning the study (n = 54); others spent between 4 and 8 min (n = 10); and the few who were removed for spending too long were presumed to have left the study while in progress and were not sensitive to the manipulations (n = 4). In addition, participants were removed because they did not answer the vignette manipulation check questions correctly (potential caregiver = 9; potential care recipient = 18). Within each measure, data were replaced by the participant’s mean for that measure if less than 20% of data were missing (n = 7 participants). Participants were removed if they had more than 20% of responses missing within a measure for two or more measures (potential caregiver = 8; potential care recipient = 2). This relatively large rate of excluded participants resulted because we used a high standard for inclusion to ensure participants were sensitive to the manipulations and had answered most of the questions. After these removals, the final sample included 195 participants (90 potential caregivers; 105 potential care recipients). 2
Design
The study used a between groups vignette methodology to examine issues related to older adult caregiving from the point of view of both the potential caregiver (non-older adults) and the potential care recipient (older adults). Participants were asked to think of themselves as assuming the roles of the people depicted in the vignette. The vignettes varied according to the older adult’s autonomy and help acceptance in a 2 (not autonomous and autonomous) × 2 (acceptance of help and refusal of help) design.
Vignettes—Manipulated independent variables
The vignettes were adapted from the Florida Supreme Court case, Sieniarecki (2000), and based generally on previous older adult caregiving research (Wylie & Brank, 2009). As described above, Sieniarecki involved a vulnerable adult who moved in with her daughter because she could not care for herself, but contentiously refused help when it was offered. The case also involved siblings who did not live in the house, but who visited regularly. Therefore, each of the four vignettes depicted a 78-year-old woman who combined resources with an adult child (live-in adult child) and moved into a new apartment together while another adult child lived 10 min away (10-min-away adult child).
For the not autonomous conditions, the older woman was portrayed as having difficulty preparing her own food, bathing and grooming, and attending medical appointments unaccompanied. In the autonomous condition, the older woman was portrayed as not having any difficulty with these activities. In the refusal of help condition, the older woman was described as unwilling to accept help with eating, bathing, grooming, and attending medical appointments. In the acceptance of help condition, the older woman was described as welcoming help with these activities. Manipulation check questions for both manipulated variables demonstrated that the participants perceived the manipulated variables correctly and that they were independent from each other.
Measures
General notions of caregiving
Two attitudinal measures were included to determine whether the two samples differed on general notions of caregiving. The first attitudinal measure was Cicirelli’s (1990) 30-item Paternalism Scale (potential care recipient α = .92; potential caregiver α = .95) where positive scores indicate stronger paternalistic beliefs about older adults (e.g., “If an elderly parent pays no attention to getting a proper diet, the adult child should decide what the parent will eat,” −2 = strongly disagree, 2 = strongly agree). Second, developed specifically for this study, the Government Involvement scale included four items (potential care recipient α = .84; potential caregiver α = .85) that measured the role government should have in older adult caregiving (e.g., “whether the government should provide an in home assistant for a few hours a week to help with caregiving”; −2 = strongly disagree, 2 = strongly agree) with positive values indicating beliefs that the government should have an active role.
Self-referencing dependent measure—Anticipated emotions
Both samples received similar dependent measures, but the wording differed slightly by sample. In the potential caregiver sample, they were asked to think of themselves as the adult child who combined resources and moved in together with the older adult depicted in the vignette. The potential care recipients were asked to think of themselves as the older adult depicted in the vignette. We asked participants about how they anticipated they would feel if faced with the decision whether or not to move in with either the adult child or the older adult (depending on the sample). We listed the emotions of compassion, anger, and guilt with five additional emotions as fillers thought to be theoretically less related to caregiving decisions (shame, sadness, content, empathy, and joy) and asked the participants to indicate which two emotions they thought they would feel.
Self-referencing dependent measure—Perceived abilities
We asked participants to assume the role of either the adult child (potential caregiver sample) or the older adult (potential care recipient sample) depicted in the vignette and rate how able they thought the adult child would be to provide necessary medical, financial, emotional, and physical care (0 = not able to 4 = completely able). The four items were averaged to create the perceived abilities measure (potential care recipient α = .72; potential caregiver α = .72).
Self-referencing dependent measure—Daily caregiving decision making
Participants answered a series of questions created for this study to gather a more specific view of how participants allocate caregiving responsibility for daily decisions across all three possible caregivers (i.e., older adult, adult child living with older adult, and adult child living 10 min away). 3 This daily caregiving decisions measure adapted from Cicirelli (2003) consisted of 17 decisions (e.g., decisions about household cleaning, driving, or paying bills) and participants indicated with a percentage (totaling 100% across all three possible caregivers) the amount of responsibility each person should have for each decision. For instance, participants provided percentage responsible for, “Who should be responsible for deciding what food should be purchased for the home?” This measure was employed because the division of caregiving is not an “all or nothing” issue (Piercy, 1998) and allowed us to measure more specifically how participants envisioned the caregiving roles—balancing an older adult’s autonomy versus paternalistic decision making made by a caregiver. For the analyses described below, we focused exclusively on the percentage allocated to the older adult because it is likely the older adult’s level of decision responsibility will serve as the reference point for decision making in daily caregiving decisions. Percentages for all 17 items were averaged together to form the daily caregiving decisions score for the older adult (potential care recipient α = .93; potential caregiver α = .94).
Results
General notions of caregiving
The online potential caregiver sample and in-person potential care recipient samples did not significantly differ on the two general notions of caregiving measures, which indicate similar representativeness between the online and in-person samples. Both samples had stronger paternalistic beliefs than autonomous beliefs toward older adults. Although previous research generally demonstrates a difference between younger and older adults on paternalism, those former studies compared mother and daughter dyads (Cicirelli, 1990) and often involved dyads currently in a caregiving relationship (Cicirelli, 2003). Both samples also similarly agreed that there should be some government role in caregiving for older adults (see Table 1).
One-Way ANOVA on Attitudinal Measures Related to Caregiving by Sample (Potential Caregivers and Potential Care Recipients).
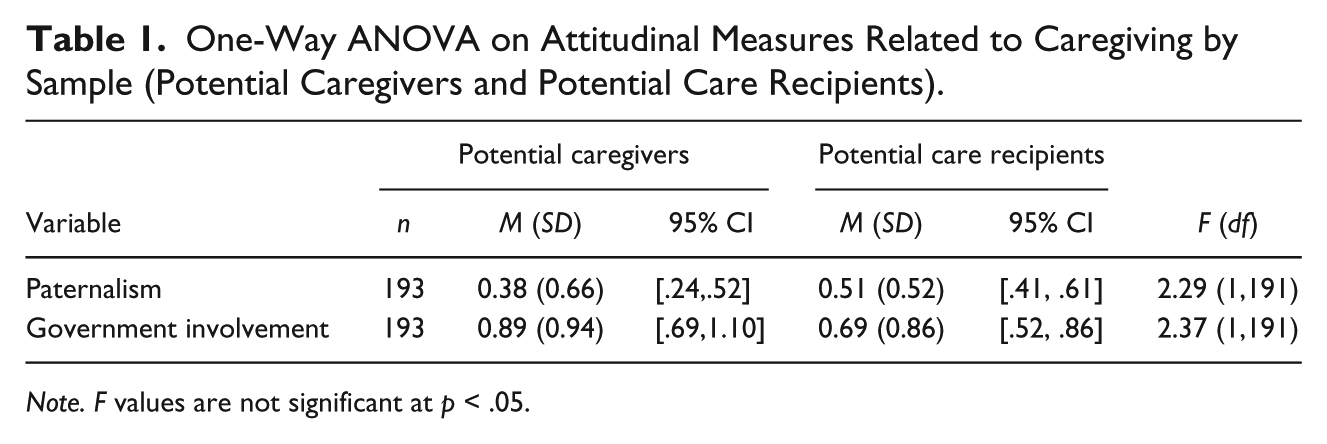
Note. F values are not significant at p < .05.
Anticipated emotions
The emotions participants indicated they would feel if presented with the decision of whether to move in together are presented in Table 2. Overall, the most endorsed anticipated emotion for potential caregivers was compassion, whereas the most endorsed anticipated emotion for potential care recipients was guilt.
Percentage of Emotions Endorsed if Faced With the Decision of Whether to Move in Together.
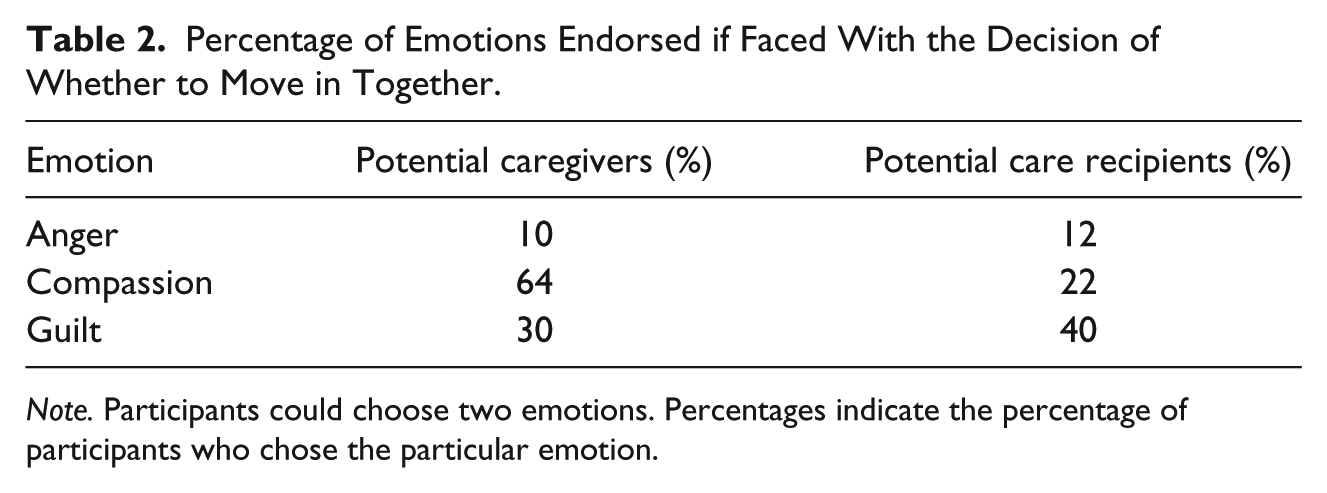
Note. Participants could choose two emotions. Percentages indicate the percentage of participants who chose the particular emotion.
Perceived ability
Potential care recipients perceived the potential caregivers as having significantly greater requisite abilities (M = 2.56, SD = 0.81) than potential caregivers saw for themselves (M = 1.99, SD = 0.95) F(1, 193) = 20.33, p < .01, 95% confidence intervals (CIs) = [2.40, 2.73], [1.82, 2.18], respectively.
Daily caregiving decision making
Potential caregivers perceived the potential care recipients as having significantly greater daily caregiving decision-making responsibility (M = 57.96, SD = 20.07) than potential care recipients saw for themselves (M = 48.64, SD = 21.73) F(1, 193) = 9.55, p < .01, 95% CIs = [53.76, 62.16], [44.44, 52.85], respectively.
Path analyses
Using a series of multiple regressions in two path models, we examined whether the two dependent measures were predicted by sample, the manipulated variables of autonomy and refusal of help, and anticipated emotions. Moreover, we examined the effects that sample, autonomy, and refusal of help had on the indirect dependent measure of anticipated emotions and whether anticipated emotions mediated the relationship between the independent variables and the dependent caregiving decision variables. The three anticipated emotion variables were set to correlate in the model (anger and compassion, r = −.20, p < .001; anger and guilt, r = −.16, p < .001; compassion and guilt, r = −.32, p < .001). Figure 1 illustrates the results of the path analysis for perceived abilities to provide care and Figure 2 illustrates the results of the path analysis for the perceived daily decision responsibility of the older adult. Significant paths are depicted as solid lines and non-significant paths with dashed lines. Standardized regression weights are provided above its respective path. Overall fit statistics were obtained for both models using Mplus (Muthén & Muthén, 1998-2011) and both models had good fit according to chi-square, comparative fit index (CFI), Tucker–Lewis index (TFI), and root mean square error of approximation (RMSEA).
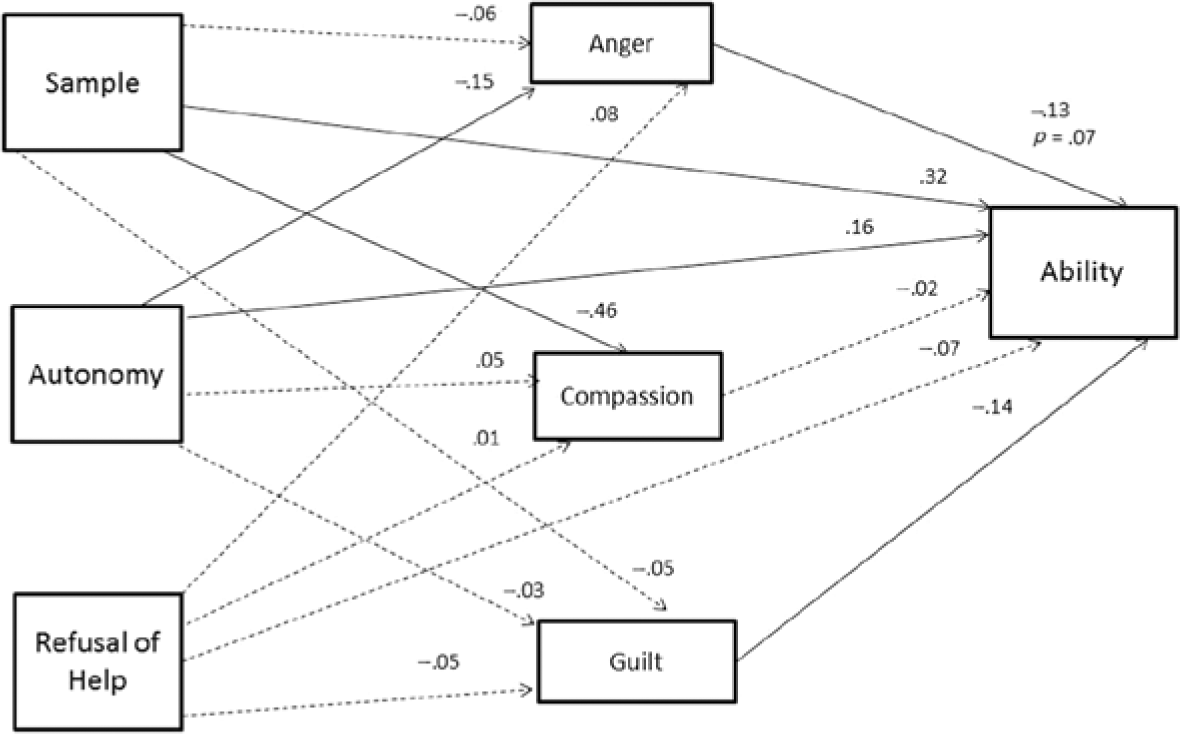
Path model for caregiving ability.
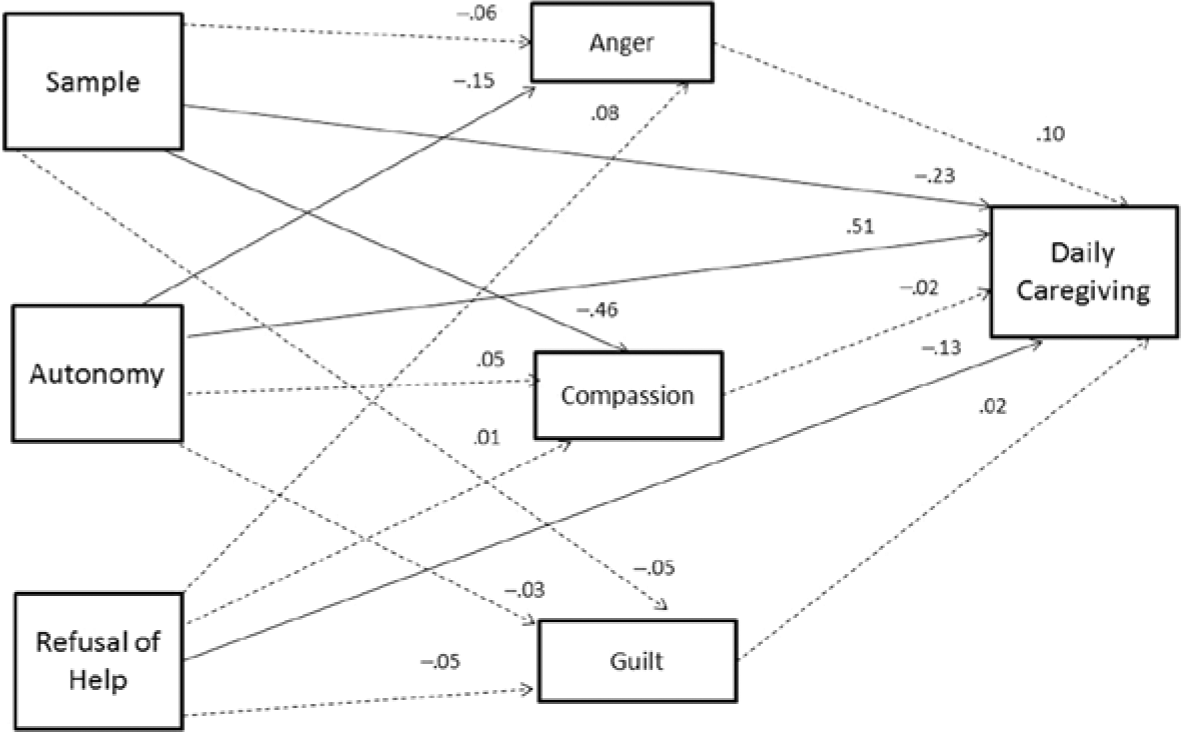
Path model for daily caregiving decisions.
Because the hypothesized models are the same with respect to the relationships between sample, autonomy, and refusal of help, with the emotions predictions (the left side of the models), we will first discuss this side of the model and then separately discuss the effects that the independent variables had on the caregiving decision-dependent variables (the right side of the models). Of the three emotions, compassion had the greatest variance accounted for (R2 = .19, 95% CI = [.10, .30]) and sample was the only variable that had a significant relationship with compassion. Potential caregivers (coded as 0) were more likely to endorse compassion as an emotion that would be a part of their decision to move in with an older parent, than potential care recipients thought would be part of their decision to live with an adult child. The analyses for anger (R2 = .03, 95% CI = [.01, .10]) revealed that the autonomy manipulation was the only variable that had a significant relationship to anger. Those in the not autonomous condition (coded as 0) were more likely to endorse anger as an emotion that would be a part of their decision to move in together, than those in the autonomous condition thought would be part of their decision to move in together. Contrary to expectations, however, none of the independent variables were significantly related to guilt in the models (R2 = .02, 95% CI = [−.01, .05]). There were also no significant indirect effects (mediators) for the anticipated emotions between the independent variables and the dependent caregiving decision variables.
Perceived abilities for caregiver to provide care
The first model explained 16% of the variance (R2 = .16, p < .001, 95% CI = [.07, .26]). As expected, perceived ability was significantly predicted by sample, such that potential care recipients (coded as 1) were more likely to perceive the caregivers as having greater requisite ability than potential caregivers perceived themselves. As expected, participants who read the vignette depicting an autonomous older adult (coded as 1) endorsed higher levels of ability to provide care than participants who read about the not autonomous older adult. Contrary to expectations, the manipulated level of older adult’s refusal of help described in the vignette did not predict perceived ability to provide care.
Anticipated guilt and anger predicted perceived abilities, such that anticipating guilt and anger decreased the perceived ability for the potential caregiver to provide care. However, compassion was not related to perceived ability to provide care.
Daily caregiving decision making
The allocation of daily caregiving decisions model explained 32% of the variance (R2 = .32, p < .001, 95% CI = [.22, .44]). As expected, potential caregivers (coded as 0) were more likely to allocate greater daily responsibility for decision making to the care recipient than potential care recipients would allocate to themselves. In addition, participants who read the vignette depicting an autonomous older adult (coded as 1) were more likely to allocate decision-making responsibility to the older adult than participants who read about the not autonomous older adult. Participants who read the vignette depicting an older adult who refused help (coded as 1) were less likely to allocate decision-making responsibility to the older adult than participants who read about the older adult who accepted help. No anticipated emotions significantly predicted daily caregiving decisions.
Discussion
Despite the potential for physical and mental burdens in older adult caregiving (Butler, Turner, Kaye, Ruffin, & Downey, 2005), most people continue to express strong support toward caring for older relatives (Dellman-Jenkins & Brittain, 2003; Ohuche & Littrell, 1989). With the increase in older adult populations and opportunity for older adult caregiving, social science research on the topic is also increasing. However, much of the social science research and legal analyses concerning older adult caregiving has been limited to caregiver burden and motivation to care for an older adult. The current study was the first to use experimental methodology to examine what effect an older adult’s need for help and refusal of help would have on potential caregivers’ and potential care recipients’ beliefs about perceived ability to provide care and allocation of daily caregiving decision making. The study yielded three main findings. First, potential caregivers and potential care recipients had different notions of perceived ability and daily caregiving decision making. Potential caregivers were less likely than potential care recipients to feel able to provide care and more likely to allocate decision-making responsibility to the older adult. This suggests that potential caregivers may not be as well prepared to take on a caregiving role as the potential care recipient may anticipate. In addition, potential caregivers are likely to allocate more decisional responsibility to older adults than the care recipients would expect.
Second, the described older adult’s autonomy and refusal of help also contributed to these decisions. As would be expected, the older adult’s level of autonomy was an important factor in both decisions such that when the older adult in the vignette was described as less rather than more autonomous, participants were less likely to perceive the potential caregiver as having the ability to provide care. Similarly, when the older adult in the vignette was described as less rather than more autonomous, the participants allocated her less daily decision-making responsibility. The described older adult’s refusal or acceptance of help was a contributing factor for daily decision making, but not for perceived abilities. When the vignette described an older adult who refused compared with accepted help, participants were less likely to allocate decision-making responsibility to the older adult and allocated more responsibility to the adult child living with her. This suggests a paternalistic response such that the refusal of help was interpreted as the older adult needing more help; that is, the adult child should be responsible for more daily decisions than the older adult when the older adult refuses help.
Third, as expected, anticipated emotions played a role in some of the caregiving decision making. Potential caregivers were more likely to anticipate feeling compassion when thinking about entering a caregiving situation than potential care recipients. Only anger and guilt contributed to the perceived abilities to provide care, but none of the emotions contributed to daily caregiving decision making. Both guilt and anger seem to be working in the same way, such that when they were endorsed there was less perceived ability to provide care. The findings are similar to the findings in Lyonette and Yardley (2003) such that guilt (an extrinsic motivator) contributed more than compassion (an intrinsic motivator) to the perceived ability to provide care. Because anticipation of guilt and anger was significantly related to a decrease in perceived ability, perhaps one’s anticipated emotions may assist in recognizing when emotions may interfere with the ability to provide care—especially in light of previous research that suggests anger is related to older adult maltreatment (MacNeil et al., 2010). Such findings could potentially inform older adult abuse prevention strategies by focusing on learning to recognize such negative emotions before deficits in care occur.
Potential caregivers’ and care recipients’ differing views about who should have the responsibility for daily care could lead to misunderstandings about care and potentially lead to unintentional neglect. Although the current study is far from predicting such dire consequences, case law demonstrates that real caregivers are struggling with these issues. For example, the adult daughter in Sieniarecki v. Florida (2000) unsuccessfully argued she was not at fault for her mother’s death from malnutrition because the daughter did not know she was her mother’s caregiver and was responsible for her mother’s daily care needs. The daughter argued it was her mother’s decisions to refuse food and medical care.
One clear weakness of the present study was the use of online vignettes and the lack of situational information about the potential caregivers. As Haynes and Olson (2006) noted, “It is often easier and less costly to help a victim in a laboratory setting than in real-life situations” (p. 666). Indeed, there is no doubt that asking online participants to imagine themselves in a caregiving situation is different from actually providing and receiving care and therefore results must be viewed with caution. For instance, demographic and socioeconomic factors are likely important in making daily and long-term caregiving decisions. Older adults are more likely to expect care from adult children who are unemployed compared with employed (van der Pas, van Tilburg, & Knipscheer, 2005); older adults from rural areas compared with urban areas are more likely to expect care from family members (Lee, Coward, & Netzer, 1994); and financial concerns are likely to play a role in caregiving decisions (National Alliance for Caregiving, 2009). Despite the weaknesses of vignettes, they allowed experimental control of factors that are likely important in caregiving decisions and to do so with a sample of both potential caregivers and care recipients.
The vignettes were a description that involved the caregiver and care recipient moving in together in a new home. We did this both because it was how the caregiving situation occurred in the legal case that was the inspiration for the vignettes (Sieniarecki v. Florida, 2000) and it was meant to equalize the situation for both samples. We suspect that notions of caregivers moving in with care recipients versus care recipients moving in with caregivers are highly related to socioeconomic class and should be examined in greater detail in the future to determine whether it influences notions of caregiver ability and decision making.
We did not address the complicated issues around any specific disease (e.g., Alzheimer’s), yet there is certainly a need to better understand the distinct concerns family members have when taking on caregiving roles for an older adult who has cognitive versus physical disability or some combination of the two. In particular, a caregiver may experience greater stress when their care recipient is degenerating mentally (Starrels et al., 1997) and when the care recipient’s behavioral problems are likely the result of their disease or the medications used to treat the disease. We did not address these issues, but future work should examine how a caregiver makes attributions about the reasons underlying a care recipient’s behavior and characteristics and more precisely measure the different weight a person may give to his or her perceived abilities (e.g., financial vs. medical abilities). We know that help giving in other contexts is related to attributions of blame (Weiner, 2006), but that has not been tested directly in the caregiving context. Relatedly, the study only focused on the parent/child relationship. As the older adult population continues to increase we know that the need for care will be greater than the number of potential caregivers; extended family members will likely be called upon to provide care and as such will come with a different set of burdens and complications. Future research should also examine these decisions with a matched sample of potential caregiver and care recipient dyads to examine responses of those in an actual caregiving relationship. Not only were the samples not matched, but those who self-selected to take part in the study could be significantly different from those who would potentially find themselves in a caregiving relationship.
This study was the first of its kind to experimentally examine the effects that older adult characteristics could have on decisions concerning ability to provide care and allocation of daily caregiving responsibilities. By using an experiment with both potential caregivers and care recipients, we were able to examine some important differences between the way a caregiver and care recipient view a caregiving situation. The results confirm that the complex caregiving decision-making process is fraught with differing viewpoints and emotions that are not adequately captured in statutes that address older adult care. This is especially true when in an informal caregiving relationship. The laws are fairly specific for formal (i.e., paid caregiver) and people who are court-ordered guardians, but the common informal nature seems incompatible with much of the way the laws operate.
Footnotes
Appendix
Acknowledgements
The authors would like to thank James Baker, Sidney Bennett, Christopher King, Claudia Escandon, Andrew Hohenstein, Teresa Kulig, Blake Nielsen, Corey O’Hanlon, and Leroy Scott for their assistance with this research.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: A portion of this research was supported by an American Psychology-Law Society’s Interdisciplinary Grant awarded to the first author and an American Psychology-Law Society Grants-in-Aid awarded to the second author.