
Abstract
Specialized dementia care units (DCUs) house individuals whose behaviors cannot be managed in other settings. To ensure environmental fit, admission/discharge criteria are recommended for DCUs; however, there is no consensus about what criteria should be used. This study aimed to describe, in a random sample of DCUs, the current admission criteria, current/recommended discharge criteria, and services to support discharge. Usable surveys were returned by 23 of 30 facilities. Residents were most frequently admitted because they had a diagnosis of dementia and exhibited cognitive/behavioral problems. The four most common discharge criteria in place/recommended were resident ability to manage in a non-specialized long-term care environment, lack of socially inappropriate behaviors, dependency in activities of daily living, and inability to participate in dementia care activities. These findings suggest that discharge from DCUs is relatively ad hoc. The study lays the groundwork for future research to evaluate the use/appropriateness of these criteria.
Over half of long-term care (LTC) residents have some form of dementia (Canadian Institute for Health Information [CIHI], 2012). To address the specialized needs of this rapidly increasing population, dementia care units (DCUs) have been established. DCUs are controlled access environments for people with dementia who exhibit behaviors (e.g., elopement, aggression, hoarding) that cannot be accommodated in other settings. These locked units commonly provide an increased staff to resident ratio and decreased stimulation. In 2006, approximately 29% of LTC facilities in the United States reported having a DCU (Castle, 2008)).
In keeping with Lawton’s (1982) model of environmental press, matching the residents’ environments to their current functional levels is intended to facilitate adaptive behaviors and improve quality of life (Warren et al., 2001). However, if a resident does not require the environmental modifications that a DCU provides, this may produce maladaptive behavior and decreased quality of life. Therefore, appropriate admission/discharge criteria are critical to ensure that appropriate residents are admitted to and remain on these units (Maas, Swanson, Specht, & Buckwalter, 1994).
Research on DCU admission/discharge criteria is limited. One retrospective study found that an increased need for personal care was the most common reason for relocation from a DCU (Horttana, Ahlström, & Fahlström, 2007). A similar study identified eight reasons why residents were relocated from DCUs, which included inappropriate placement, behavioral difficulties, lack of benefit from programming, decreased ambulation and oral feeding, change in financial status, acute illness, and family request (Specht et al., 1999). Based on the discharge criteria in place at one facility, which included severe cognitive impairment, limited capacity to take part in activities, resident disruptions, psychiatric symptomology, and functional deterioration (decreased ambulation), Kovach (1998) concluded that 60% of discharged residents had not been appropriately placed initially. Furthermore, there are few studies that describe how discharge from a DCU can be supported.
In light of concerns about the potential for inappropriate placement, and potential problems associated with relocation and challenges with discharge, a study was conducted that sought to answer the following questions about DCUs:
What admission criteria are in place?
What discharge criteria are in place or recommended?
What methods to support discharge are currently in place or recommended?
Method
The study was approved by the appropriate university and regional ethics boards. The data were acquired through a self-administered survey that was developed and administered using Dillman’s (2007) tailored design method. The survey consisted of nine questions. The first three questions collected information on survey respondent demographics. The fourth question collected information about each facility’s admission criteria. The last five open-ended questions collected information about (a) current admission criteria, (b) current and (c) recommended DCU discharge criteria, and (d) current and (e) recommended practices to support discharge. Respondents were also asked to provide copies of any formal admission or discharge criteria they had in place.
To ensure the clarity of questions, the survey was reviewed and piloted with four other DCU health professionals who were not included in the survey. Only minimal wording changes to ensure clarity were suggested.
Sample and Sampling Procedures
The sampling frame included all 45 DCUs within the province of Alberta, Canada. To obtain a representative sample, surveys were sent to a random selection of 30 DCUs. Surveys were addressed to the resident care managers. They were asked to complete the survey or have it completed by a delegate who could answer the questions. Managers were targeted because it was anticipated they would have the most global perspectives of how the DCUs functioned.
Recruitment Process
Initial email invitations were sent out to managers at each facility and a link and consent form were emailed three days later. A $2 coffee card, survey link, and consent form were also sent via regular mail to the 30 selected DCU centers. Reminder emails were sent 1 and 3 weeks after the initial invitation to encourage survey completion.
Data Analysis
Descriptive statistics were calculated for closed-ended questions. To analyze open-ended questions, content analysis was used (Taylor-Powell & Renner, 2003). Each question was analyzed independently. After reviewing all of the responses, a list of mutually exclusive concept codes was created, which was applied to each question.
Results
Twenty-six survey responses were received. One of these responses was deleted, as it was a blank form. Two additional surveys were deleted as IP addresses indicated that the same individual submitted the survey twice (partially initially and fully on a second occasion). Thus, an overall response rate of 77% was obtained with 23 successfully completed surveys returned.
Participant Characteristics
Most respondents were facility managers or administrators (n = 15). Other respondents included registered nurses (n = 7) and one physiotherapist. The mean number of beds in these facilities was 38. The largest number of respondents worked in facilities with 11 to 20 beds (n = 9).
Survey Findings
Admission criteria currently in place are described in Figure 1. Results indicated that admission is commonly based on the case manager assessment and recommendation, presence of socially inappropriate behaviors, diagnosis of dementia, and cognitive status. Almost all respondents indicated that they used the Resident Assessment Instrument (RAI) assessment outcome (n = 22) to inform admission decision into their DCUs. One respondent used the Changes in Health and End-stage disease Signs and Symptoms (CHESS) score. Respondents did not indicate how these scores were used.
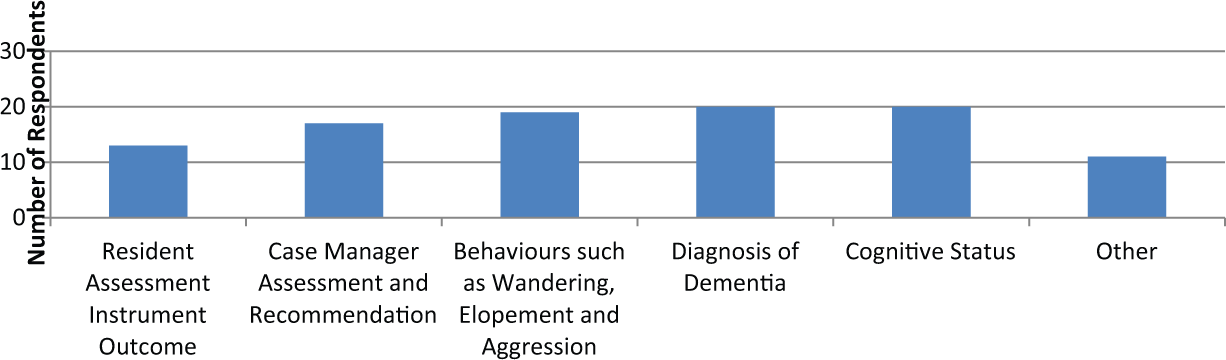
Criteria used for admission to dementia care units (n = 23).
Existing discharge criteria are described in Figure 2. The most frequently identified discharge criteria were the resident’s ability to function in a regular LTC environment, need for two person assistance with activities of daily living, and lack of socially inappropriate behaviors. Four facility representatives stated that they had no formal discharge criteria in place; however, three of these respondents went on to list informal discharge criteria. Although requested, none of the respondents supplied any formal discharge policies.
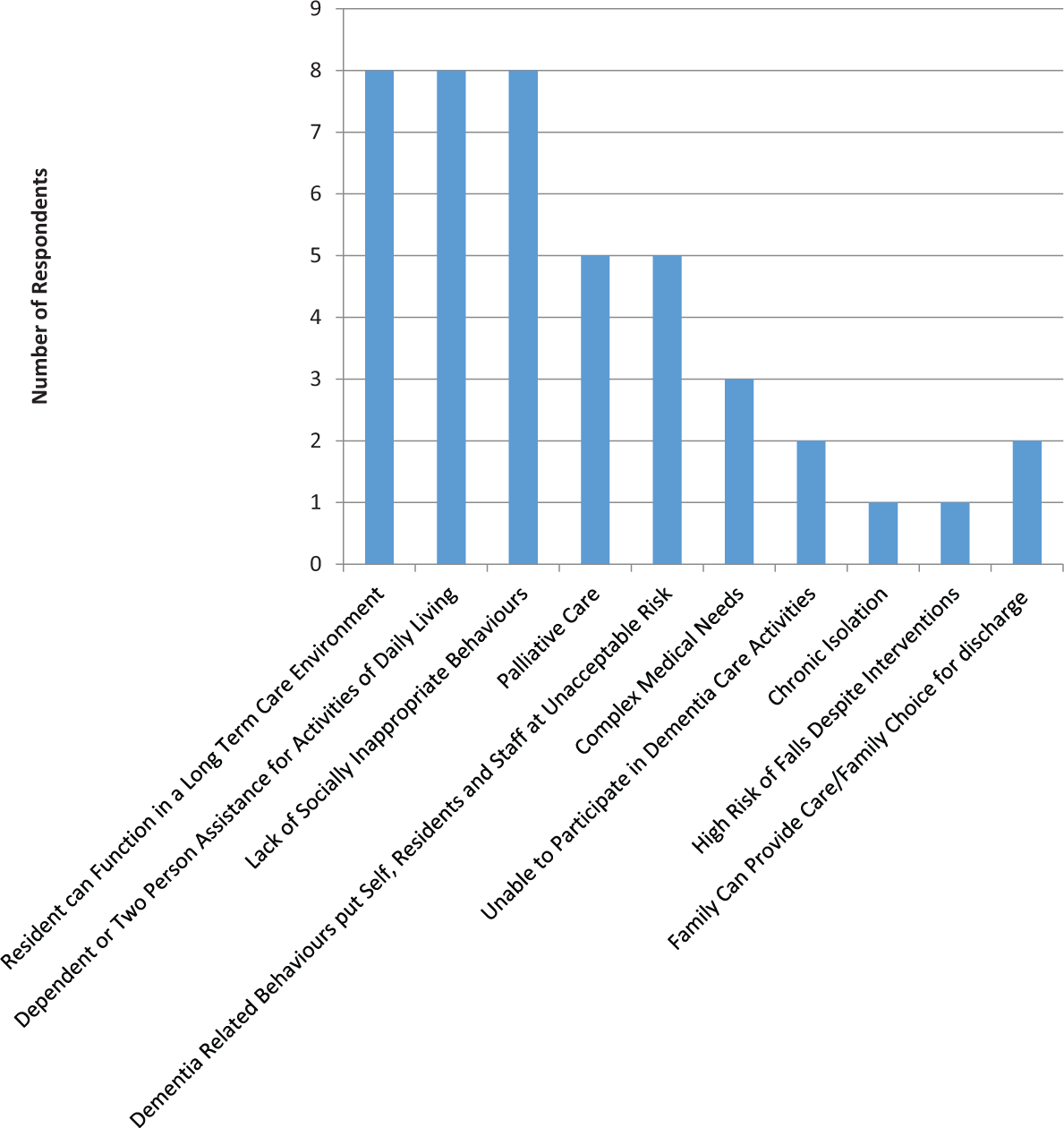
Discharge criteria currently in place in dementia care units (n = 23).
Recommended discharge criteria for DCUs were very similar to the discharge criteria already in place. All of the discharge criteria currently in place were also recommended. Two additional criteria that were suggested were disease progress/decreased cognition (n = 1) and not meeting admission criteria (n = 1). Two respondents stated that they supported aging-in-place and did not recommend discharge from DCUs.
Existing methods of supported discharge are exhibited in Figure 3. The most prevalent method listed was collaboration with other professionals (n = 16). Three of the DCUs did not currently have any services available to facilitate a resident’s discharge.
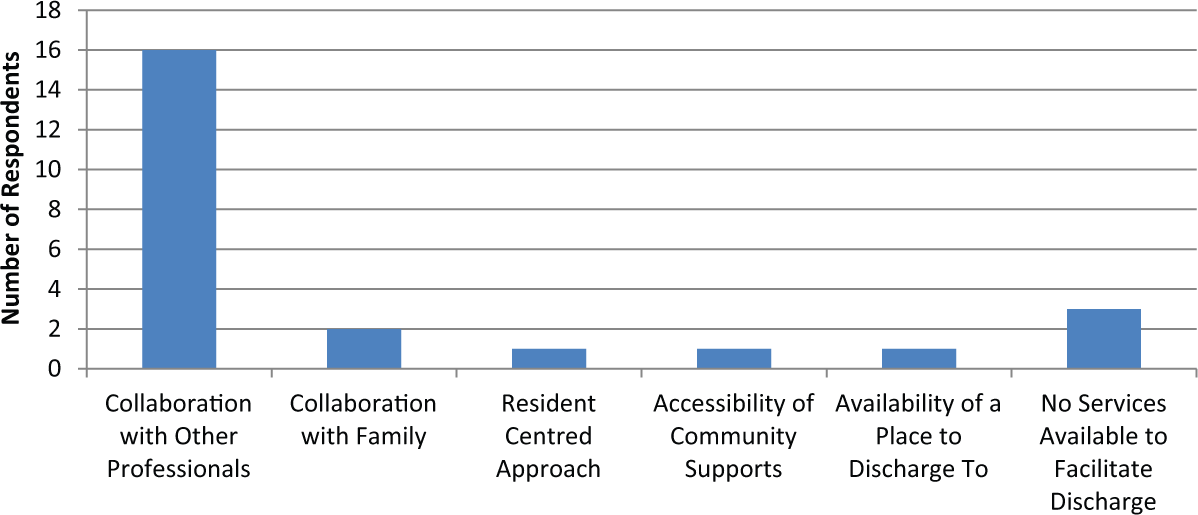
Supportive discharge practices in place in dementia care units (n = 20).
Similarly, the most frequently recommended method of supporting discharge was collaboration with other professionals (n = 11). One respondent stated that he or she recommended the resident not be discharged from this environment (i.e., aging-in-place recommended). Other recommended methods of supporting discharge included family support (n = 2), increased staff to resident ratios (n = 2), improved communication between staff (n = 3), and other (seven individual recommendations).
Discussion
To our knowledge, this is the first study to explore the admission/discharge criteria that are in place and/or recommended in DCUs. The study found that the admission to and discharge process from DCUs was relatively ad hoc. Although participants identified a variety of admission/discharge criteria, many did not indicate how these criteria were operationalized. As none of the respondents provided any formal discharge policies, as was requested, it seems many of these criteria may be informal. Although informal criteria may give facilities flexibility, they make it difficult to evaluate the suitability of these criteria and may contribute to inappropriate placement if residents are not re-evaluated regularly. The discharge criteria recommended by participants, such as resident’s ability to function in a regular LTC environment and a lack of socially inappropriate behaviors, are in line with the discharge criterion of “inappropriate placement” described by Specht et al. (1999). Other discharge criteria, such as the residents’ care requirements, have also previously been identified (Horttana et al., 2007; Specht et al., 1999).
Given the importance of environmental press in promoting function and quality life (Lawton, 1982) and the potential influence of the environment on self-directedness (Lawton, 1990), ongoing assessment for suitability would seem warranted; however, there appears to be controversy surrounding whether it is better to allow a resident to reside in a familiar environment or relocate to an environment where current needs can be better met through specialized care/environments (Horttana et al., 2007; Kovach, 1998; Wilden & Froese, 1991). Some studies have found that relocation is associated with an increase in mortality/morbidity, increased depression, decreased cognition, and a general decline in wellness, especially if the move is done without preparation (Holdera & Jolley, 2012; Laughlin, Parsons, Kosloski, & Bergman-Evans, 2007). Aging-in-place was a surprising theme identified in the survey. In this regard, some respondents stated that their units did not have discharge criteria, nor did they recommend any, because their facility supported allowing residents to age-in-place. The concept of aging-in-place in the context of residential care is contentious, however, as these residents have already been displaced from their own homes in the community.
Although it seems intuitive that “ability to manage in a regular LTC environment” would be a discharge criterion, there is a question about how this would be operationalized. If residents are relocated to an environmental setting that does not suit their functional needs, it may potentially increase their agitation (Satariano, 2006). Given issues associated with relocation, there is also a question about how long a probationary transfer is considered necessary and also concerns about whether a bed would be available if the relocation is unsuccessful.
Although DCUs were established to meet the specialized needs of this population, this study raises concerns about their ability to handle challenging behaviors. If DCUs are the highest level of care for people with dementia, and are unable to meet their needs safely, this represents a potential gap in service. This finding suggests that DCUs may need additional supports in place to deal with these behaviors or may need to re-evaluate how these clients are managed to prevent unnecessary relocations.
A discrepancy was noted between the supportive discharge practice recommended and those in place. Given that three respondents indicated that their facilities currently do not have any services to facilitate discharge, this suggests there is an unmet need. Furthermore, there were more supportive discharge practices recommended than were currently in place, which may indicate a gap in service. In this regard, it appears respondents believed that the discharge process could be improved with better communication among interdisciplinary care staff and between staff and families as well as increased staffing levels to allow for greater attention to resident needs during relocation.
Strengths and Limitations
The study had several strengths and limitations. The response rate of 77% can be categorized as “very good” as it is over 75% (Babbie, 2007). Random sampling is also a strength of this study. This, combined with our high response, should allow us to generalize the findings to all facilities in the sampling frame (Rockerville, Sorra, & Nieva, 2004). However, in light of the sampling frame, the results may not generalize to DCUs outside of Alberta. Furthermore, given the survey questions, respondents did not identify how the criteria they identified informed decision making.
Implications for Practice
This study suggests that there is a lack of uniform admission, discharge, and supportive discharge practices for DCUs. In addition, research is needed to gather more detailed information about how admission/discharge criteria are operationalized in a larger sample of DCUs (i.e., understanding how the RAI is used to inform decision making). It would be helpful to explore what happens to residents who are deemed inappropriate for their current settings and for the DCUs to which they have been referred to identify those who fall through the system. Criteria illustrated in our study could be used as the basis for a Delphi study to develop more consistent criteria and policies. Longitudinal studies that follow residents throughout this process would be beneficial to help evaluate the merit of these criteria and success of their implementation. This research could help identify the best way to determine whether a DCU resident is able to function in a regular LTC environment.
Conclusion
Staff from DCUs were surveyed to find out what admission/discharge criteria and discharge supports were currently in place or were recommended. The results suggest that admission to and discharge from DCU is relatively ad hoc. Participants suggested discharge could become more supportive with better communication among staff and family members, and increased staffing resources to support residents who are being relocated. The study lays the groundwork for future research to further explore these criteria, evaluate how these criteria are used in practice, and determine their appropriateness. These steps are necessary to ensure suitable environmental fit and optimal quality of life for these residents.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.