
Abstract
Late life deterioration of functional status is associated with adverse health outcomes and increased cost of care. This trial was conducted to determine whether dance-based intervention could reverse functional decline among nursing home (NH) residents. A total of 189 residents of seven NHs in the Czech Republic were randomly assigned to intervention and control groups. More detailed data were collected in a subsample of 52 participants. Intervention consisted of 3-month dance-based exercise. Functional status was assessed by the get-up-and-go test, basic activities of daily living (ADL), instrumental activities of daily living (IADL), and senior fitness tests (SFTs). Participants in the control group experienced a significant decline in get-up-and-go test, IADL, and in four of the six SFTs. The intervention proved to be effective in preventing this deterioration and improved chair stand test and chair sit-and-reach test. The findings indicate that a relatively simple dance-based exercise can slow down deterioration of functional status in NH residents.
Introduction
The deterioration of functional status and decreased level of physical activity that are typical for older adults in the later stages of their life increase their risk of adverse health outcomes such as disability (Lee, Kim, Back, Kim, & Ryu, 2013; Luleci, Hey, & Subasi, 2008) or morbidity (Millan-Calenti et al., 2010), which are associated with a financial burden for the whole society (Martinson, Crain, Pronk, O’Connor, & Maciosek, 2003). Disability itself is the most important predictor of the cost of nursing home (NH) care (Williams, Fries, Foley, Schneider, & Gavazzi, 1994). Because the proportion of older adults is increasing globally, the ability of older adults to function independently as long as possible has emerged as a major clinical and public priority.
Residents of NHs represent one of the most vulnerable, often functionally impaired, populations of older adults who are at high risk of further decline leading to a complete loss of independence and other related deleterious consequences (Ferrucci et al., 2004). In addition, their functional status tends to deteriorate faster than the rest of the older population due to the services provided by facility staff, lack of encouragement to take care of themselves, or simply due to a smaller living space (Cress, Orini, & Kinsler, 2011). Hence, NHs are in great need of effective preventive strategies that may reverse or slow down the functional deterioration of their residents. One possible solution could be the implementation of appropriate physical activity programs.
Regardless of the available evidence of the benefits of physical activity (Chin, van Uffelen, Riphagen, & van Mechelen, 2008; Daniels, van Rossum, de Witte, Kempen, & van den Heuvel, 2008; Rydwik, Frandin, & Akner, 2004), convincing older adults to engage in physical activity is challenging. Implementation of physical activity programs is often prevented by perceived barriers such as physical health problems and frailty, fear of resulting injury or falling, past sedentary lifestyle, insufficient understanding about physical activities, or environmental restrictions to initialize and maintain physical activity (Chen, 2010). Furthermore, those with functional deficits are least likely to participate despite the fact that they would gain the most from such interventions (Ferrucci et al., 2004; Kraschnewski et al., 2014). In addition to various types of motivation, for example, a physician’s advice to exercise (Cohen-Mansfield, Marx, Biddison, & Guralnik, 2004; Schutzer & Graves, 2004), it is vital to develop a suitable physical activity intervention that respects the needs and preferences of today’s elderly. Dance might be one of the options because it offers a social and enjoyable activity that is familiar to many older adults. In addition, because dance combines physical activity, music, and social interaction, it may provide extra benefits than alternative individual activities or activities without the music component. In addition, dance was found to address both physical and cognitive impairment in various groups of older adults by incorporating physical and motor skill activities and engaging cognitive functions, including perception, emotion, or memory (Dhami, Moreno, & DeSouza, 2014). Finally, dance appeared to be most effective in the physically impaired older adults, who showed the lowest performance prior to the intervention (Kattenstroth, Kalisch, Holt, Tegenthoff, & Dinse, 2013), which applies to our sample of NH residents.
Dance-based interventions have been reported to improve most of the components of functional fitness and other related outcomes in healthy older adults (Alpert et al., 2009; Eyigor, Karapolat, Durmaz, Ibisoglu, & Cakir, 2009; Federici, Bellagamba, & Rocchi, 2005; Hopkins, Murrah, Hoeger, & Rhodes, 1990; McKinley et al., 2008; Shigematsu et al., 2002). However, to our best knowledge, the frail or functionally impaired elderly population has been included in only a limited number of studies (Ashley & Crenan, 1993; Borges et al., 2012; da Silva Borges et al., 2014; Holmerova et al., 2010; Sandel, 1994). Of those studies, only three were conducted in institutions (Borges et al., 2012; da Silva Borges et al., 2014; Holmerova et al., 2010).
Previous research with a small number of NH residents found improvement of lower body mobility after dance, while significant deterioration in some lower body mobility measures was observed in the control group (Holmerova et al., 2010). The present study extends these findings by studying an intervention in a significantly larger sample of participants from seven instead of only three NHs. The focus of this study was the overall functional performance, including upper body performance, general mobility, and measures of the ability to perform daily activities. Furthermore, it identified functional deterioration in greater detail. The aim of this randomized control trial was to determine the effect of a dance-based intervention (EXDASE [EXercise DAnce for Seniors]; Veleta & Holmerova, 2007) on functional status in NH residents and whether, in addition to the lower body deterioration observed earlier, there would be a deterioration in other components of functional status (upper body function, complex mobility measures, and autonomy in instrumental activities of daily living [IADL] and basic activities of daily living [ADL] tasks) in the control group.
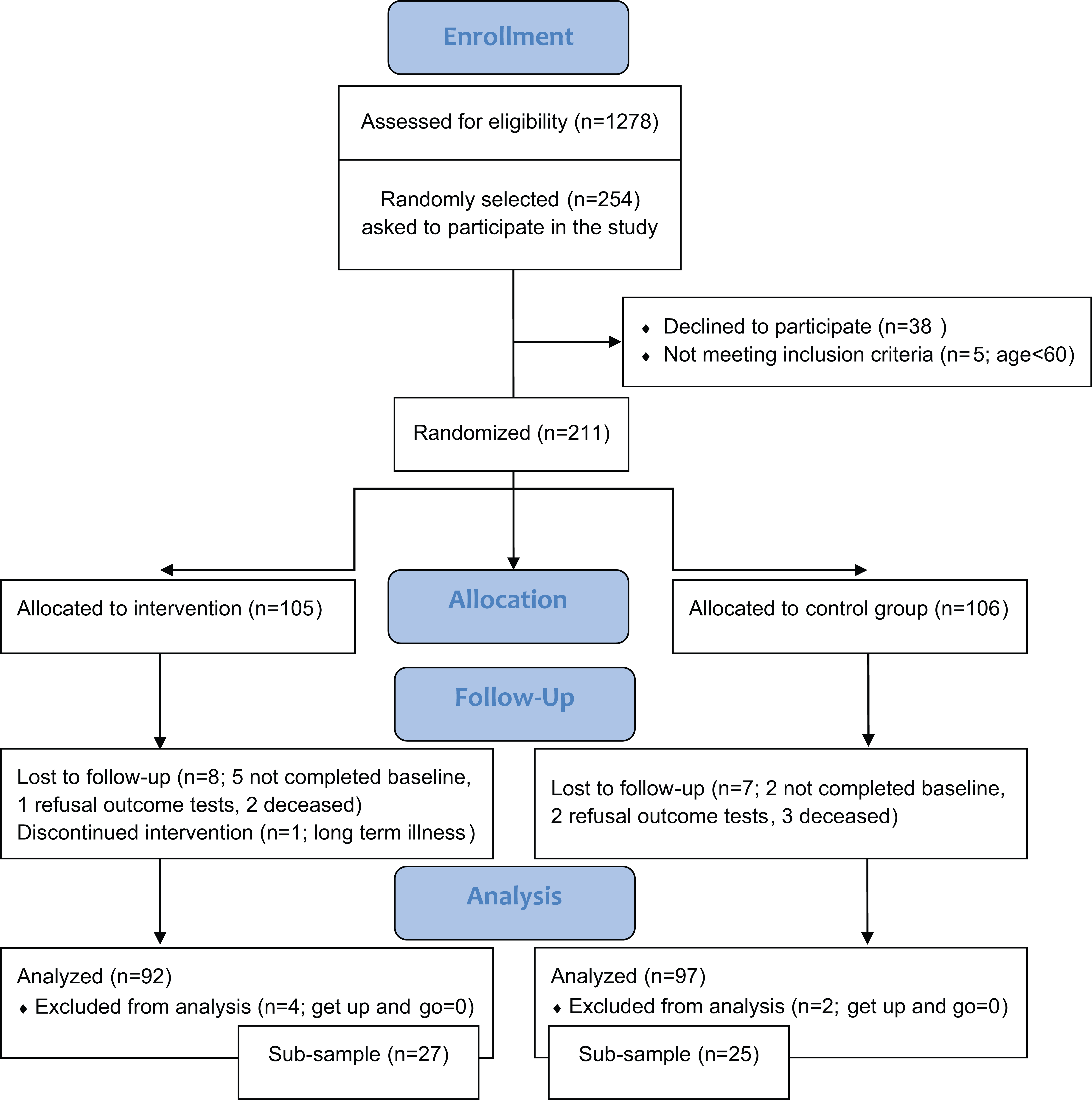
A flow diagram of the study population.
Method
Research Design and Participants
This study, which focused on the possible prevention of functional decline, is based on a multicenter randomized controlled trial of a dance-based intervention in 211 older adults living in seven NHs in the Czech Republic (Vankova, Holmerova, Andel, Veleta, & Janeckova, 2008; Veleta & Holmerova, 2007). Eligibility criteria included (a) being a permanent resident of one of the NHs and (b) being 60 years or older. Additional criteria for the present study included (c) completion of mobility baseline and follow-up tests and (d) having a mobility score (get-up-and-go test) at baseline above 0. More detailed data were collected among study participants living in three of the seven selected NHs in Prague (n = 52; 27 in the intervention and 25 in the control group). These three NHs were selected because of their convenient accessibility and proximity to the research team (convenience sampling). Data specific to this subsample included components of functional fitness measured by the senior fitness test (SFT) battery (Rikli & Jones, 2001).
The baseline data were collected within a week prior to the intervention, and follow-up data were collected within a week after the end of the intervention by blinded test administrators. A waiting list design was used, so all participants in the control group could join the dance sessions after the end of the trial. The Ethical Committee and Institutional Review Board at the Internal Grant Agency of the Ministry of Health of the Czech Republic (NR8487) approved this study. All participants signed the informed consent form.
Intervention
The dance-based program consisted of approximately 1-hr group sessions conducted once per week for 3 months. The intervention is described only briefly because it has been described elsewhere (Holmerova, Vankova, Hradcova, Steffl, & Veleta, in press; Veleta & Holmerova, 2007). The dance sessions were divided into a 10-min warm-up period, a 40-min main dance period, and a 10-min cool-down period, all accompanied by motivating music appropriate for each period. The warm-up period included various slow-paced leg and arm movements mostly in a seated position. The main dance-based exercises involved basic steps and combinations of ballroom dances, including foxtrot, waltz, cha-cha-cha, cancan, and so on. The intensity varied for each participant depending on individual abilities and was individually increased during the trial according to the subjective judgment of the dance instructor to provide maximum benefits. However, the overall goal of the dance instructor was to make each class enjoyable for all participants. The dance instructor always sought to adapt the exercises for participants dancing in wheelchairs. The cool-down period used relaxation techniques such as deep breathing and stretching exercises. The control group participated in the regular activities of the NH.
Measurements
Baseline data
Baseline assessments included sociodemographic characteristics such as age (years), gender, education, and information about mental health and cognitive status. Depressive symptoms were assessed using a short version of the Geriatric Depression Scale (GDS 15; Sheikh & Yesavage, 1986) translated into the Czech language and standardized for use in the Czech Republic (Jirak, 2004). The Mini-Mental State Examination (MMSE; Folstein, Folstein, & McHugh, 1975) was used to assess global cognition.
Outcome measures
Main sample
Mobility
Mobility was assessed by the get-up-and-go test (Mathias, Nayak, & Isaacs, 1986) adapted and standardized for use in the Czech Republic (Holmerova, Juraskova, & Zikmundova, 2003). The test starts in a sitting position in a straight-backed chair. The participant is asked to (a) get up; (b) walk forward 3 m; (c) turn around a cone, walk back to the chair, turn; and (d) sit again. In contrast to the previous study in which the evaluation was performed based on the duration of the test, in this study, we assessed each of the four steps with a score ranging from 0 (cannot perform) to 3 (performs without any problems), resulting in a total score between 0 and 12.
ADL
Ability to perform ADL was assessed by the Barthel Index (range = 0-100, higher scores = better ability; Mahoney & Barthel, 1965).
IADL
The ability to perform the IADL was assessed by questions focused on independence in more advanced daily tasks using the Lawton IADL Scale (Lawton & Brody, 1969) ranging from 0 to 8 (higher scores = better ability).
ADL and IADL were assessed by proxy reports because most of the participants had some level of cognitive impairment.
Subsample
Functional ability
Functional ability was assessed by standardized SFT (Rikli & Jones, 2001) consisting of six performance-based tests designed to measure individual components of functional fitness in older individuals: chair stand test (measure of lower body strength; the number of repetitions in 30 s that a person can come to a full stand from a seated position with arm folded across the chest, higher scores = better ability); arm-curl test (measure of upper body strength; the number of repetitions in 30 s that a person can curl 2.27 kg for women and 3.63 kg for men through the full range of motion by the dominant hand in a seated position with the back straight and feet flat on the floor, higher scores = better ability); 2-min step test (measure of aerobic fitness; number of repetitions in 2 min that a person can step in place raising the knees to a height between the patella and iliac crest, higher scores = better ability); chair sit-and-reach test (measure of lower body flexibility; number of centimeters, either plus or minus, between the tips of the middle finger and the toe while seated at the edge of a standard chair, with one leg extended and the other foot flat on the floor, higher scores = better ability); back scratch test (measure of upper body flexibility; number of centimeters, either plus or minus, between the tip of a middle finger of the preferred hand placed over the same shoulder, palm down and fingers extended and the other hand placed around the back of the waist with palm up, reaching up as far as possible in seated position with the back straight and feet flat on the floor, higher scores = better ability); and 8-foot timed test (measure of agility/dynamic balance; number of seconds needed to get up from the seated position and walk as quickly as possible around a cone that is 8 ft (2.44 m) away and return to the seated position, lower scores = better ability).
Statistical Analysis
Statistical Package for Social Sciences (SPSS for Windows [Version 15.0]) was used to analyze all data. Independent-samples t test or chi-square test was used to detect possible differences between intervention and control groups before the intervention. All results were analyzed using the general linear model (GLM) for repeated measures. This model is similar to the repeated-measures ANOVA and allows direct comparison of pre- to posttest changes across the groups by yielding a Group-by-Test interaction. The 2 (between groups: intervention vs. control at baseline) × 2 (within groups: pretest vs. posttest) factorial design was used because it considers differences between the groups in pretest as well as differences in change between pretest and posttest for the two groups. In addition, paired-sample t tests were used to examine pre- to posttest changes separately for the two groups. Statistical significance was assessed at a two-tailed .05 level.
Results
Baseline characteristics for the main sample and subsample are presented in Table 1. Mean age for the main sample (N = 189) was 83 years, while for the subsample it was 82 years (n = 52). Most of the participants in both samples were women (91% and 88%, respectively). About one third of the participants reported fewer than 9 years of education (34% and 28%). The mean GDS score for the main sample was 5.45 and that for the subsample was 5.16; depressive symptoms (GDS ≥ 6) were present in 46% of the respondents. The MMSE score revealed cognitive deficits in the study participants (23.6 for the main sample and 24.0 for the subsample). The sample included participants with normal MMSE scores (40%, MMSE range = 27-30) and participants with cognitive impairment (49% had MMSE ≤ 24). The remaining 11% had MMSE scores of 25 or 26. The differences were insignificant for all presented characteristics except for two tests—the get-up-and-go test and ADL—in which participants in the subsample performed significantly better. In both samples, independent-sample t test or chi-square test found no statistically significant differences between the control and intervention groups in these baseline measures.
Baseline Characteristics of Study Participants.
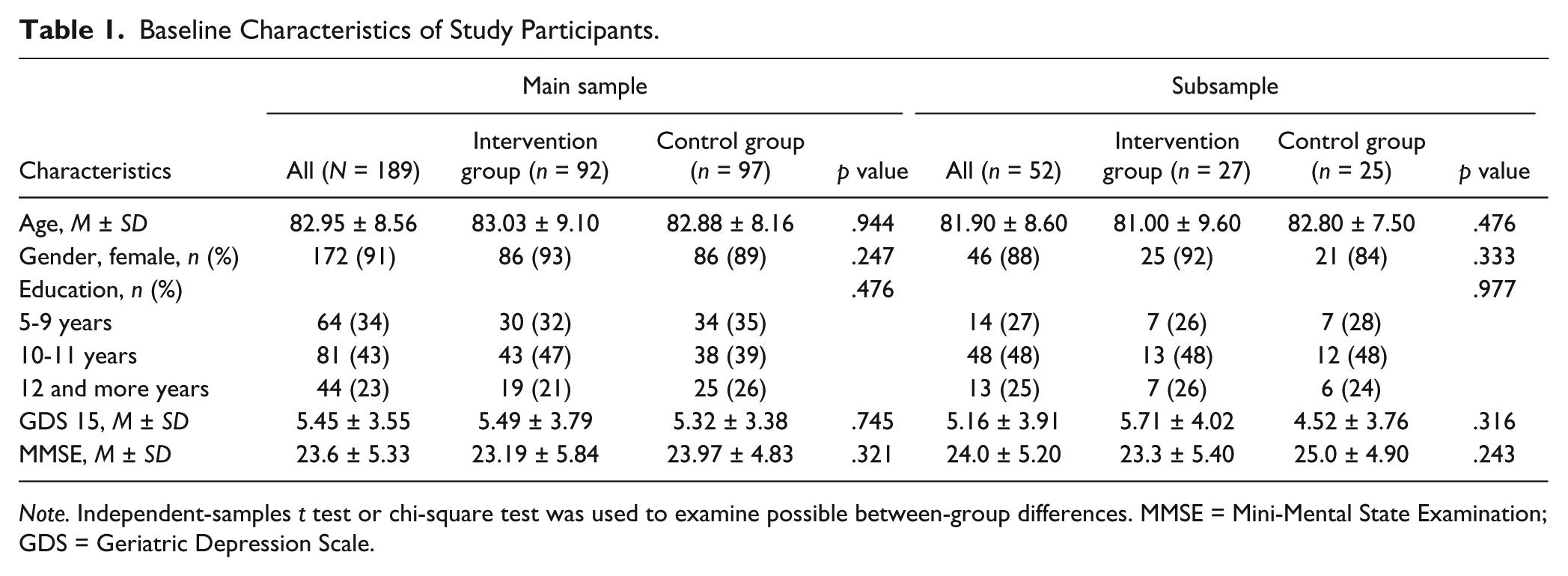
Note. Independent-samples t test or chi-square test was used to examine possible between-group differences. MMSE = Mini-Mental State Examination; GDS = Geriatric Depression Scale.
Table 2 provides the results of outcome variables for the main sample. At baseline, the differences between the intervention and control groups were not statistically significant. However, the control group slightly outperformed the intervention group on the get-up-and-go test and ADL (p > .05). The difference in IADL between the two groups at baseline was statistically insignificant. Paired-sample t tests showed a statistically significant decline in mobility (p = .022) and IADL (p = .013) in the control group. GLM analyses were statistically significant for differences between the intervention and control groups in both these measures. Declines in ADL were observed in both the control and intervention groups but it was not statistically significant. However, the mean ADL score worsened more in the control group than in the intervention group. More detailed analysis of individual ADL items revealed a statistically significant decline in dressing in the control group (t test, p = .033) and a nearly statistically significant decline in walking in the control group (t test, p = .058) with no change in these items in the intervention group.
Functional Performance Measures for Main Sample.
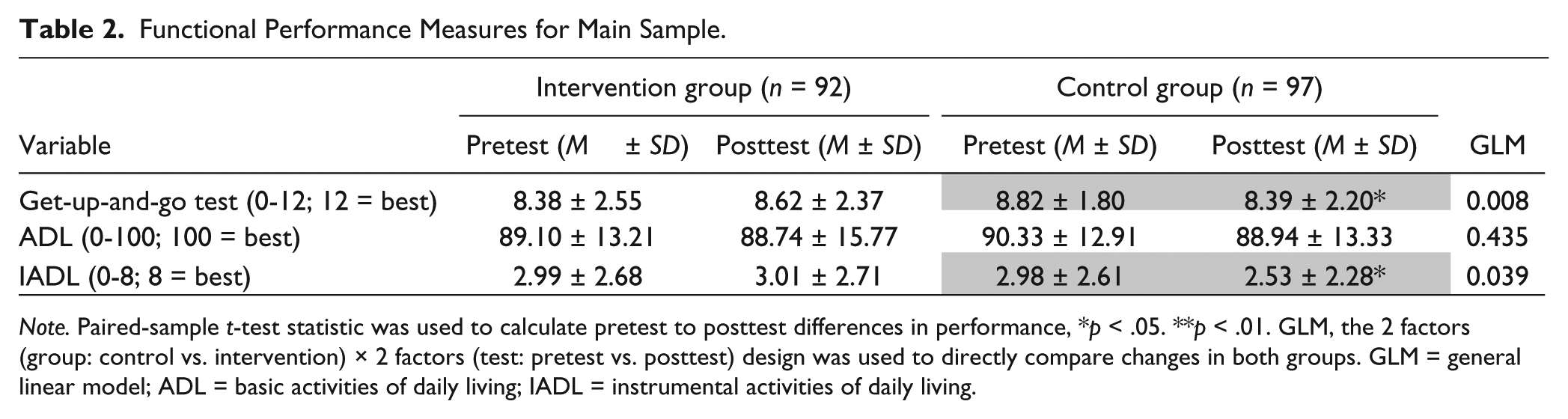
Note. Paired-sample t-test statistic was used to calculate pretest to posttest differences in performance, *p < .05. **p < .01. GLM, the 2 factors (group: control vs. intervention) × 2 factors (test: pretest vs. posttest) design was used to directly compare changes in both groups. GLM = general linear model; ADL = basic activities of daily living; IADL = instrumental activities of daily living.
More detailed data on functional performance collected in 52 of 189 participants are presented in Table 3. At baseline, the intervention group significantly outperformed the control group on the chair sit-and-reach test (p = .033). The remaining differences were not statistically significant. The control group slightly outperformed the intervention group on the chair stand test, whereas the intervention group slightly outperformed the control group on the arm-curl test, 2-min step test, back scratch test, and timed-up-and-go test (p > .05).
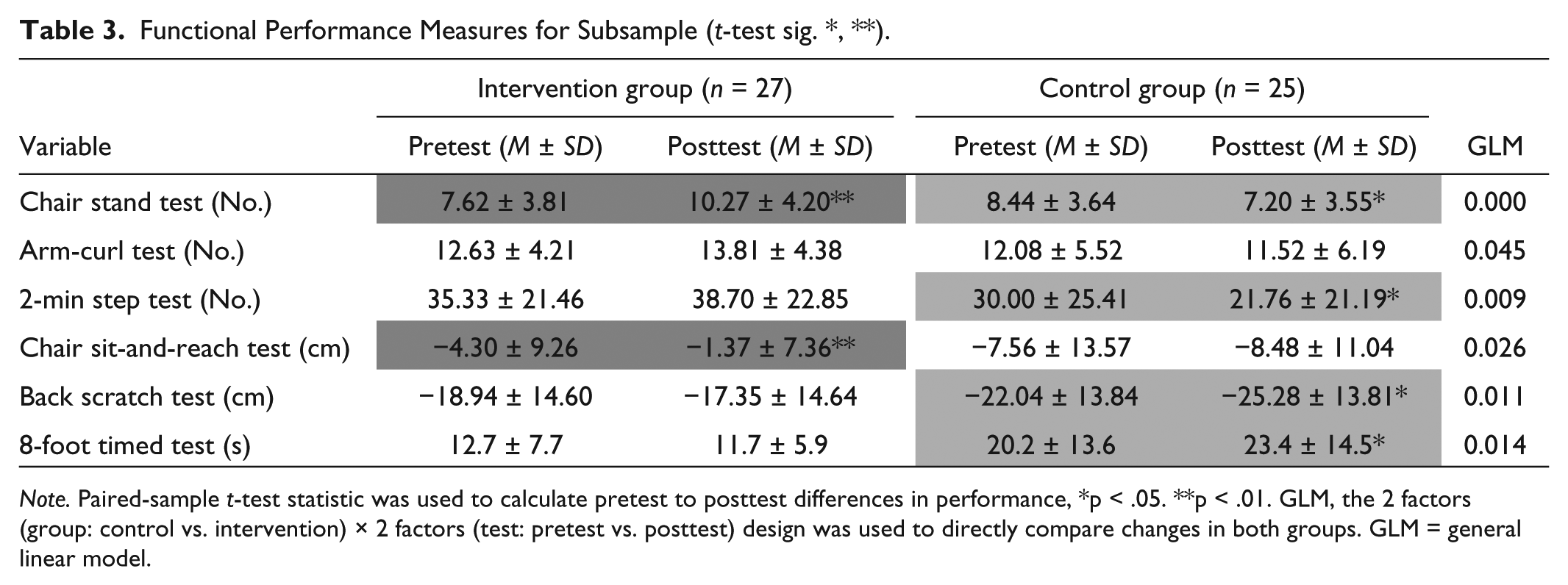
Note. Paired-sample t-test statistic was used to calculate pretest to posttest differences in performance, *p < .05. **p < .01. GLM, the 2 factors (group: control vs. intervention) × 2 factors (test: pretest vs. posttest) design was used to directly compare changes in both groups. GLM = general linear model.
Results of GLM analysis were statistically significant for all six SFT items, indicating significant differences between the control and intervention groups. The paired-sample t test revealed that the control group significantly worsened in four of the six tests, including chair stand test (p = .011), 2-min step test (p = .024), 8-foot timed test (p = .047), and back scratch test (p = .036) and that the intervention group significantly improved in the two tests, including chair stand test (p = .006) and chair sit-and-reach test (p = .008).
Discussion
The present randomized control trial addressed the importance of physical activity among NH residents and investigated whether it could prevent the functional declines typical for this population. A major clinical and public priority is to successfully slow down or even reverse this deterioration in institutionalized functionally impaired older adults, who are at high risk of further decline leading to a complete loss of independence and other related damaging consequences. Our study found that in this population, a significant decline in functional status can be detected after a 3-month interval and that this decline could be prevented by a simple and easy-to-implement intervention.
Functional status was assessed by an adapted version of the get-up-and-go test, ADL and IADL tests. Statistically significant declines in the control group after only a 3-month period were observed in two of these tests (IADL and get-up-and-go test) and in two ADL items. The performance-based mobility test (get-up-and-go test) showed the largest declining trend (p = .008), which has important clinical implications. Because mobility is fundamental for the majority of daily tasks, attention should be paid to even slight declines in this ability before it affects other associated areas of daily functioning, first IADL and then ADL. The skills assessed in IADL are more complex than skills included in ADL, thus it should not be surprising that the decline was first visible in the IADL scores. Statistically insignificant but clearly declining trends in ADL scores suggest that significant declines may be recognizable after more than a 3-month period. Closer examination of individual ADL items showed that worsening of walking—the item most closely associated with mobility—was nearly statistically significant after 3 months.
Analyses of individual SFTs in the subsample support the results of outcome measures in the main sample. All SFTs were significantly different between the control and intervention groups by GLM analyses. In addition, five of them showed statistically significant changes when examined separately for the control and intervention groups by paired-sample t test (either declines in the control group or improvements in the intervention group). Selected results of the SFTs associated with lower body performance were already published in a study focused on the effect of dance on mobility (Holmerova et al., 2010). The only test that was not significantly different by t tests was the arm-curl test assessing upper body strength. This smaller effect of our intervention was most likely due to the type of the intervention. Although dance involves movements of both legs and arms, arm movements only accompany step variations and involve a flexibility type of exercise. This fact was well reflected in the significant change in the upper body flexibility test (back scratch test). Furthermore, improved upper body flexibility was also mirrored in the significant prevention of deterioration of another ADL item: dressing, showing the strong link between functional fitness and everyday functional performance.
Positive effects of physical activity interventions on the general population and healthy older adults have been well established. Growing evidence regarding the benefits of physical activity among frail community-dwelling elderly is promising (Chin et al., 2008; Chou, Hwang, & Wu, 2012; Daniels et al., 2008; Gine-Garriga, Roque-Figuls, Coll-Planas, Sitja-Rabert, & Salva, 2014) but cannot compensate for a lack of research involving frail institutionalized older populations and NH residents with higher levels of impairment (ADL and IADL disability and possible cognitive deficits). The results of the present study support the beneficial effect of physical activity (excluding dance) reported in the few studies conducted in frail institutionalized elderly (Piedras-Jorge, Melendez-Moral, & Tomas-Miguel, 2010; Rydwik et al., 2004). In addition, our study stresses the functional decline occurring in this high-risk population and presents an acceptable and effective physical activity that can prevent it.
According to Weening-Dijksterhuis, de Greef, Scherder, Slaets, and van der Schans (2011), effective physical activity interventions for frail institutionalized populations should include a combination of progressive resistance training, balance training, and functional training. The proposed intensity should be moderate to high, assessed on a 0 to 10 scale, and the training frequency should be 3 times a week with a total duration of at least 10 weeks. Such recommendations are not easily applicable in the Czech NHs due to a lack of financial and personnel resources.
In contrast to the above recommendations, our results suggest that functionally impaired NH residents can benefit from a 1-hr dance-based intervention applied only once a week for 3 months. Similar findings were reported by Keogh, Kilding, Pidgeon, Ashley, and Gillis (2012) who provided evidence that weekly dance exercise can produce significant benefits for older adults. In addition, they found no significant differences between dance sessions applied once or twice per week. Nevertheless, we offer several possible explanations for our findings. One of the reasons might be that our intervention included recommended types of training but was more acceptable for functionally impaired NH residents with potential cognitive deficits. It is also possible that this amount of physical activity is only beneficial for this population because the so-called ceiling effect may prevent improvement in fitter older adults (Buchner, Beresford, Larson, LaCroix, & Wagner, 1992). This hypothesis is supported by Kattenstroth and his colleagues (2013), who compared baseline performance with the improvement following a dance intervention applied only once a week but for 6 months and revealed that those individuals who benefitted most from the intervention were those who showed the lowest performance prior to the intervention. Those results are very encouraging from a clinical point of view because this amount of exercise is the most practical for long-term continuation, given the individual and organizational conditions of NHs.
To ensure satisfactory participation and adherence, it is important to respect the specific preferences and needs of the elderly to motivate them to fully engage in a physical activity program. Familiar movements accompanied by music may support both participation and adherence (Conn, Burks, Minor, & Mehr, 2003), especially by NH residents who often suffer from cognitive deficits because dance is a social and enjoyable activity. This is just one of the reasons why dance is considered a strong candidate for an alternative therapy in neurorehabilitation (Dhami et al., 2014). Palo-Bengtsson and Ekman (1997) found dancing to be very positive for patients with dementia, and this acceptance may ultimately lead to better effectiveness of physical activity programs. The social aspect of dance can play a very significant role.
The prevention of deterioration in functional status documented in this study may also have been mediated by a positive effect of the dance intervention on depressive symptoms described in a previous report (Vankova et al., 2014) due to proven relationship between depressive symptoms and functional status (Eisses et al., 2004; Vankova et al., 2008). Another possible explanation for our findings is that the dance intervention may have increased psychological factors, including self-efficacy, self-evaluation, self-esteem, and self-confidence. The opportunity to share this type of group activity and the overall experience enabled participants to realize that they can still do things they previously considered impossible.
The study results are tempered by a number of limitations. First, the study sample consisted of mostly women. Although a predominance of women is typical for NHs, the ratio between men and women was imbalanced due to men more frequently declining to participate. Second, more detailed data were collected only in a subsample of study participants but the results were similar in both samples. Third, the use of IADL testing in NH residents may be somewhat questionable because some of the tasks are not performed as there is no need, not because of an actual inability. Fourth, the selection of NHs included in the study was not random; however, a large number of NHs were involved. And finally, a longer follow-up period would be more appropriate for this type of study and would have a potential to show even stronger results. However, it is interesting to note that significant deterioration could be detected after only a 3-month period in this population, which itself is alarming. Future research should incorporate longer follow-up periods into the study design.
Conclusion
In conclusion, the findings of this study indicate that a decline in the functional status of NH residents can be observed in as little as a 3-month period and that this decline can be prevented even among high-risk NH residents by a simple dance-based program. This study also verified the feasibility, acceptability, and efficacy of dance therapy in NH residents. Dance represents a unique type of physical activity that provides multisensory stimulation incorporating components such as physical activity, music, and social interaction, and these components most likely affect both physical and cognitive status. In addition to physical and motor skill activities, dance engages cognitive functions, including perception, emotion, and memory (Dhami et al., 2014). The effect on physical and cognitive functions is most likely also mediated by social aspects and the overall enjoyable character of dance lessons. These findings are very promising from a clinical point of view because implementation of such interventions could prolong independence and significantly contribute to the better overall health of NH residents, which may consequently result in a reduction of health care costs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was supported by the grant NT13705 of the Internal Grant Agency of the Ministry of Health of the Czech Republic.