
Abstract
This study examined the relationship between food insecurity and health care utilization (physician, inpatient, emergency room, and home health visits) among older adults. Survey data collected from Georgia Advanced Performance Outcomes Measures Project 6 linked to the Centers for Medicare and Medicaid Services (GA Advanced POMP6-CMS) data 2008 (N = 957) were analyzed. Nearly one half of the sample (48.3%) was food insecure. Food insecure individuals were significantly less likely than food secure individuals to have any physician (69.7% vs. 80.2%) and home health visits (24.9% vs. 32.3%) during 2008. However, there were no significant differences in levels of health care utilization by food secure and food insecure older adults. Food secure and food insecure older adults utilized comparable levels of health care services. Public assistance programs such as Medicare and meal services targeted toward older adults may enable economically constrained, food insecure older adults to access needed health care services.
Introduction
Health care utilization patterns among older adults have received increasing attention due to escalating health care costs and disproportionate share of health care resources consumed by the rapidly growing older population in the United States. Although Medicare, the federal health insurance program for older adults aged 65 or older, reduces financial risk associated with health care expenses (French & Jones, 2004), rising health care costs due to longer life expectancy and higher prevalence of chronic diseases increase the health care burden of older adults (Kelley et al., 2013). Medicare has significant cost-sharing responsibility and gaps in benefit coverage for services that are particularly crucial for those with multiple chronic conditions. As baby boomers enter retirement years with stable or declining incomes, the financial toll of declining health and rising health care expenditures can be a significant challenge (Crystal, Johnson, Harman, Sambamoorthi, & Kumar, 2000; Kelley et al., 2013) and can force many resource-constrained older adults to make trade-offs between basic needs such as food and health care (Bengle et al., 2010; Biros, Hoffman, & Resch, 2005; Kushel, Gupta, Gee, & Haas, 2006; Ma, Gee, & Kushel, 2008; Sattler & Lee, 2013; Sullivan, Clark, Pallin, & Camargo, 2010).
Alongside rapid health care expenditure growth, food insecurity has emerged as a growing public health problem among the older adults in the United States (Lee, Gundersen, Cook, Laraia, & Johnson, 2012; Ziliak & Gundersen, 2015). Food insecurity is defined as “limited or uncertain availability of nutritionally adequate and safe foods or limited or uncertain ability to acquire acceptable foods in socially acceptable ways” (Anderson, 1990, p. 1560). Approximately 3.0 million (8.9%) households with elderly experienced food insecurity in 2014 (Coleman-Jensen, Rabbitt, Gregory, & Singh, 2015). Since the beginning of economic recession in 2007 until 2013, the number of elderly experiencing marginal food insecurity increased by 56% (Ziliak & Gundersen, 2015).
Food insecurity is associated with adverse health consequences, such as poor self-reported health status (Lee & Frongillo, 2001; Stuff et al., 2004; Ziliak & Gundersen, 2014), obesity (Brewer et al., 2010; Martin & Ferris, 2007), physical and mental health problems (Kim & Frongillo, 2007; Klesges et al., 2001; Lee & Frongillo, 2001; Nelson, Brown, & Lurie, 1998; Stuff et al., 2004; Ziliak & Gundersen, 2014), higher cardiovascular risk (Seligman, Laraia, & Kushel, 2010), poor diabetes self-management (Billimek & Sorkin, 2012; Nelson et al., 1998; Seligman, Davis, Schillinger, & Wolf, 2010), hypertension (Seligman, Laraia, & Kushel,2010), and medication nonadherence (Afulani, Herman, Coleman-Jensen, & Harrison, 2015; Bengle et al., 2010; Berkowitz, Seligman, & Choudhry, 2014; Kushel et al., 2006; Sattler & Lee, 2013). Therefore, food insecurity is a clinically relevant problem and has significant implications for health care utilization and costs of older individuals and the nation.
Researchers have examined the relationship between food insecurity and health care utilization mostly among the adult population. In general, previous research shows that food insecure individuals were more likely to delay care when needed and more likely to utilize acute care and be hospitalized than food secure individuals were. Food insecurity was associated with delaying needed medical care and medications and increased utilization of emergency rooms and hospitalizations among low-income adults aged 18 to 64 (Kushel et al., 2006), higher physician utilization among low-income adults with diabetes (Nelson, Cunningham, Andersen, Harrison, & Gelberg, 2001), higher utilization of hospitalization and emergency rooms among homeless adult users of Health Care for the Homeless (HCH) clinic sites (Baggett et al., 2011), and more visits to emergency rooms due to poor self-management of diabetes (Seligman, Davis, et al., 2010). Studies based on samples of adult patients in emergency rooms found that food insecure adults make explicit choices between food and medicine (Biros et al., 2005; Kersey, Beran, McGovern, Biros, & Lurie, 1999; Sullivan et al., 2010). In a sample of adults aged 18 to 64 from Ontario, Canada, Tarasuk et al. (2015) found a higher likelihood of health care use among severely and moderately food insecure than food secure households.
Despite the clinical and health care implications of food insecurity, only a few studies have examined the extent to which food insecurity is associated with health care utilization among the older adults (Bhargava, Lee, Jain, Johnson, & Brown, 2012; Wolff, Starfield, & Anderson, 2002). This gap in research may in part be due to the lack of appropriate data to examine these issues in the existing data sets (Lee, 2013). Existing data such as Medical Expenditure Panel Survey (MEPS) with data on health care utilization among older adults lack information on the food security status of the older adults, whereas data sets such as National Health and Nutrition Examination Survey (NHANES) include information on the food security status of the older adults but lack data on health care utilization. To address this gap, this study examined the relationship between food insecurity and health care utilization among the older adults using state-level data established by linking Georgia aging services client data and Medicare claims data from the Centers for Medicare and Medicaid Services (CMS) in 2008 (Georgia Advanced Performance Outcomes Measures Project 6 [GA Advanced POMP6]-CMS). Specifically, we examined the relationship between food insecurity and the utilization of four types of health care services—inpatient, physician, emergency room, and home health services. Tarasuk et al. (2015) used similar approach of using population-based Canadian Community Health Survey merged with administrative data on health care utilization to examine association between household food insecurity and health care utilization in a younger population.
The relationship between food insecurity and health care utilization may be explained through at least two mechanisms. First, due to the adverse health consequences of food insecurity, food insecure individuals may need more health care services. The health consequences of food insecurity are potentially more severe for the older adults due to age-related decline in health and higher prevalence of diet-related chronic conditions such as diabetes and hypertension than among younger adults. Andersen’s framework of health care access and utilization has been widely used to understand individuals’ utilization of health services. This framework considers the use of health care services to be a function of three types of factors: predisposing factors such as demographic and other individual characteristics, enabling factors such as income and health insurance coverage, and need factors such as health status (Andersen & Newman, 1973). Within Andersen’s model, food insecurity can be seen as a predisposing factor that affects health care utilization. Based on Andersen’s model, there will be a positive association between food insecurity and utilization of health care services. Second, according to neoclassical household production framework (Becker, 1965), consumption is constrained by household resources. Resource constraints may require food insecure individuals to trade health care for food as a coping strategy, implying a negative association between food insecurity and health care utilization. Existing research on the link between food insecurity and health care utilization, however, is largely atheoretical and provides little guidance regarding the magnitude and direction of the relationship among older adults.
This exploratory study is the first of its kind to investigate associations between food insecurity and the utilization of health care services among older adults using unique data with measures of food insecurity and health care utilization in a substantially large sample of older adults. Given the limited ability to carefully consider any potential endogeneity bias from the available data sets, this study was not intended to examine the causal relationship between food insecurity and health care utilization; therefore, the results should be interpreted with caution. As policymakers contemplate ways to contain the rising health care costs of the nation and as services aimed at enhancing the food security of older adults face severe cutbacks, it is critical to have a better understanding of the relationship between resource constraint phenomena such as food insecurity and inadequate health care utilization to guide efforts directed at ensuring that the diverse needs of the growing older population are met.
Method
Data and Sample
The merged GA Advanced POMP6 and CMS data provide the key study variables for this study in a substantially large sample of low-income, minority, noninstitutionalized older adults in the state of Georgia. The GA Advanced POMP6, a collaborative project between the Georgia Division of Aging Services (GA DAS) and the Department of Foods and Nutrition at the University of Georgia (UGA), was designed to assess the impact of Older Americans Act Nutrition Program (OAANP) participation on food security and nutritional health in older Georgians. In the GA Advanced POMP6 project, community-dwelling, active, and new OAANP participants and waitlisted people completed self-administered mail surveys. The project included both a cross-sectional and a longitudinal component. A detailed description of the study design, study population, and measurement validation has been published elsewhere (Lee, Johnson, & Brown, 2011; Lee, Johnson, Brown, & Nord, 2011; Lee, Sinnett, Bengle, Johnson, & Brown, 2011). As described in previous publications (Bhargava et al., 2012; Lee, 2013), the GA Advanced POMP6 provides self-reported or subjective data on sociodemographic and economic characteristics, food insecurity, medication adherence (Bengle et al., 2010; Briesacher, Gurwitz, & Soumerai, 2007; Sattler & Lee, 2013), and general health status collected through surveys and Georgia aging client database systems.
The CMS data provide objective measures of Medicare and out-of-pocket service utilization and expenditures, and health status based on administrative health claims data.
The merged data include 4,653 participants (85% of the total GA Advanced POMP6 sample). The Institutional Review Boards on human subjects of the Georgia Department of Community Health (Project No. 091203) and the UGA (Project No. 2008-10404-2) approved this study. The merged GA Advanced POMP6 and CMS data provide an exceptional opportunity to examine the relationship between food insecurity and health care utilization in a sample of low-income, noninstitutionalized older adults in need for food assistance.
For the purposes of this study, 2008 CMS and baseline data from the longitudinal study sample of the GA Advanced POMP6 were used. The study sample includes all persons who began OAANP participation as well as those added to program waitlists between July and early November 2008 and who completed the baseline survey (N = 1,594). Out of 1,594 participants in the GA Advanced POMP6 sample, 1,377 (86%) were merged with the CMS data. The analytic sample included only those participants aged 65 years and older and who had complete information on key study variables in the merged 2008 GA Advanced POMP6 and CMS data (N = 957, 70% of the 1,377 total merged sample, M age 76.9 ± 87.8 years, 31% male, 71% White).
Measurement of Variables
Dependent variables
Measures of health care utilization
The CMS data provide event-level information on the utilization of four different types of health care services (i.e., physician visits, inpatient visits, emergency room visits, and home health visits) for the period from January 1 to December 31, 2008. These data were measured on a continuous scale as the number of health care services utilized for the period from January 1 to December 31, 2008 (Table 1).
Description of Variables.
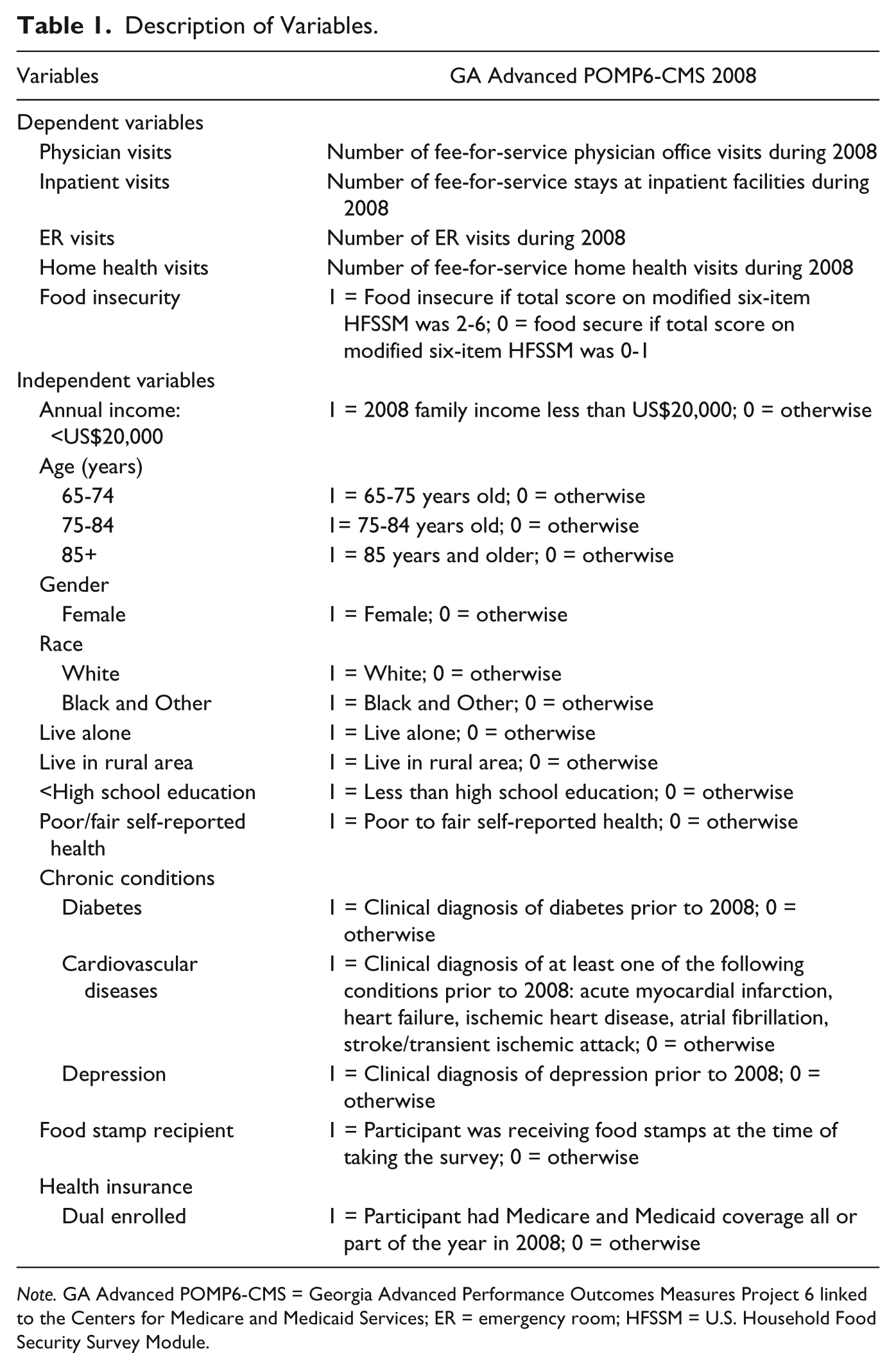
Note. GA Advanced POMP6-CMS = Georgia Advanced Performance Outcomes Measures Project 6 linked to the Centers for Medicare and Medicaid Services; ER = emergency room; HFSSM = U.S. Household Food Security Survey Module.
Primary independent variable
Food insecurity status
Food insecurity status in the last 30 days was assessed using a validated modified version of the six-item U.S. Household Food Security Survey Module (HFSSM; Table 1; Lee, Johnson, Brown, & Nord, 2011). The six-item HFSSM is shown to reliably assess food insecurity in older adults in need of meal services (Lee, Johnson, Brown, & Nord, 2011). Based on the sum of affirmative responses to the six-item HFSSM, a food insecurity summary score (score of 0-6) was calculated and used to classify the individual as either food secure (score of 0-1) or food insecure (score of 2-6).
Control variables
Demographic and socioeconomic characteristics
Demographic and socioeconomic information in GA Advanced POMP6 data obtained from the Georgia aging client database systems included age, gender, race, education, and county of residence. Age was measured as a continuous variable and then divided into three categories: (a) 65 to 74 years, (b) 75 to 84 years, and (c) 85 years and older. Race was categorized into White, and Black and Other. Level of education was dichotomized, that is, less than high school or high school graduate or more. The county of residence was classified according to a scheme developed by Bachtel (2007) as urban (urban, urbanzing, and suburban) and rural (rural growth and rural decline). Living arrangement was a binary variable indicating whether the respondent lived alone or not. Total combined income for all persons in the household was assessed by the survey. A dichotomous variable measured whether the household income was below US$20,000.
Program participation status
Two program participation variables were included in the models. The GA Advanced POMP6 survey asked whether the respondent was receiving food stamps at the time of the survey. The Medicare claims data provided information on Medicaid coverage status of Medicare beneficiaries. A binary variable, labeled dual enrolled, measured whether the participant had both Medicare and Medicaid coverage.
Health status
Health status was assessed using subjective measures from GA Advanced POMP6 data and objective measures from CMS data. Self-reported health, reported on a 5-point scale ranging from “poor” to “excellent,” was categorized as either “fair to poor” or “good to excellent.” Information on chronic conditions was drawn from CMS Chronic Condition Warehouse (CCW) data (Buccaneer, n.d.). As described in our previous publication, the CCW was created by the CMS using Medicare and Medicaid claims and available assessment data across the continuum of care and provided 21 predefined chronic conditions. From these data, three common chronic disease variables were created, including cardiovascular diseases (acute myocardial infarction, heart failure, ischemic heart disease, atrial fibrillation, stroke/transient ischemic attack), diabetes, and depression.
Statistical Methods
Descriptive and multivariate analyses were used to examine the relationship between food insecurity and health care utilization. Hypothesis of association between food insecurity and health care utilization was tested using statistical models that control for demographic, socioeconomic, program participation, and health characteristics of respondents. Chi-square tests were used to examine any differences in proportion of those who used health care services by food insecurity status. Measures of health care utilization derived from CMS data are count variables that take on discrete integer values only. Health care utilization data from Medicare claims also have disproportionately high number of observations at zero reflecting nonuse of health care services during the study period. For example, only about 36% of the sample had at least one inpatient visit during the study period. Therefore, among those who had at least one visit to the health care provider during the study period, nonparametric Mann–Whitney tests were used to assess statistical significance of any differences in health care utilization of food secure and food insecure older individuals. Negative binomial regression method, appropriate for analyzing count data and dealing with skewness of health care utilization (Cameron & Trivedi, 1998), was used to examine the relationship between food insecurity and health care utilization, controlling for other variables. The significance level was set at p < .05. In all models, we included an interaction term of food insecurity with food stamp participation to assess any conditional effects of food stamp participation on health care utilization. These interaction effects were not statistically significant in any of the models and did not modify the relationship between food insecurity and health care utilization.
Results
Descriptive and Bivariate Analysis
The demographic, socioeconomic, and health characteristics of food secure and food insecure older adults from GA Advanced POMP6-CMS 2008 are presented in Table 2. About half of the study sample was food insecure. Nearly 41% of the sample was aged 65 to 74 years, 31% were male, and 71% were White. The majority of the sample reported fair or poor health (75%), about two thirds had at least one cardiovascular disease, and half of the sample had diabetes. Nearly three fourths of the sample had income below US$20,000, and about one fifth of the sample was receiving food stamp benefits. Compared with food secure participants, food insecure participants were more likely to report income below US$20,000 and to be younger, from racial minorities, less educated, and recipients of food stamp benefits. Food insecure participants were also more likely to report poorer health status and to have diabetes.
Characteristics of the Study Sample by Food Insecurity Status (N = 957).

Differences between groups were tested using the Pearson’s chi-square test.
Nearly 36% and 75% of the sample had at least one inpatient and one physician visit recorded during 2008, respectively (Table 3). Approximately one fourth of the sample had at least one emergency room visit and 29% had at least one home health visit during 2008. Based on chi-square analysis, food insecure individuals were significantly less likely than food secure individuals to have any physician (69.70% vs. 80.20%, p < .05) and home health visits (24.89% vs. 32.32%, p < .05) during 2008. Among those who used any health care services, there were no differences in health care utilization between food secure and food insecure older adults.
Bivariate Association Between Health Care Utilization and Food Insecurity Status (N = 957).

Note. SD = standard deviation; Q1 = first quartile; Q3 = third quartile; ER = emergency room.
p values are based on Wilcoxon–Mann–Whitney test comparing number of visits between food insecure and food secure participants.
Food insecure elderly were significantly less likely than food secure older adults to have any physician visit (69.70% vs. 80.20%) and home health visit (24.89% vs. 32.32%) during 2008; Pearson’s chi-square test, p < .05.
Multivariate Analysis
Results of multivariate negative binomial regression models revealed no significant differences in health care utilization by food insecurity status (Table 4). Several health and demographic factors were associated with health care utilization. Those who had diabetes, cardiovascular disease, and depression had significantly higher levels of utilization of all types of health care services than those who did not have these chronic conditions. Compared with those reporting very good to excellent health, those reporting poor or fair health status had significantly fewer inpatient, emergency room, and home health visits. Those aged 65 to 74 and 75 to 84 had significantly fewer home health visits than those aged 85 or older. Females had significantly more physician visits than males. Minorities had significantly fewer physician and home health visits than Whites. As shown in Table 4, McFadden’s pseudo-R2 for all models was low with values ranging from 3% for physician visits to 8% for the emergency room visits model.
Results of Multivariate Negative Binomial Regression Models for Association Between Food Insecurity and Health Care Utilization (N = 957).

Note. ER = emergency room; SE = standard error.
p < .05, based on negative binomial regression models.
Discussion and Conclusion
This study examined the relationship between food insecurity and health care utilization among older adults using state-level data from the GA Advanced POMP6-CMS 2008. The prevalence of food insecurity in the GA Advanced POMP6-CMS 2008 study sample of low-income older adults was very high compared with that in the national sample of older adults from other nationally representative surveys (Coleman-Jensen et al., 2015; Ziliak & Gundersen, 2015). When various demographic, socioeconomic, health insurance, and health status factors associated with health care utilization were held constant, food secure and food insecure older adults had comparable utilization of all types of health care services. This finding contradicts previous research, which suggests that food insecure adults are more likely to utilize acute care, be hospitalized and use more physician services than food secure adults. However, these findings are largely based on studies examining the relationship between food insecurity and health care utilization in adult subpopulation. Georgia is one of the poorest states in the nation, with high prevalence of food insecurity, chronic conditions, and disability in older adults (Lee, Fischer, & Johnson, 2010). Understanding health care utilization patterns of food insecure older Georgians provides guidance for state and federal programs and policy decisions aimed at improving effectiveness of nutrition and health care services for low-income older Americans. Comparable levels of health care utilization among food secure and food insecure older adults may be indicative of effectiveness of public assistance programs such as Medicare and meal services in helping economically constrained older adults with meeting their basic needs. Further research is needed to investigate effectiveness and cross-benefits of these programs in alleviating economic insecurity of most vulnerable subpopulations.
Several limitations of the study must be noted. First, due to a lack of data on the utilization of health care services covered by Medicaid and other supplemental insurance policies, utilization in GA Advanced POMP6-CMS data may be underestimated. This underestimation may be more pronounced for low-income older adults. Nearly 46% of the low-income Medicare enrollees in our study sample were also receiving Medicaid, which may pay for services not covered by Medicare. For dual eligible Medicare beneficiaries, besides assisting with payment of Medicare premiums, deductibles, coinsurance, and copayments, Medicaid may provide extended benefits including coverage for dental services, eyeglasses, hearing aids and exams for fitting them, nursing home care, and home- and community-based services that may not or be partially covered by Medicare (Cubanski et al., 2015). Second, food insecurity is often a cyclic phenomenon and cross-sectional data may not elucidate the dynamic relationship between health care utilization and food insecurity. Longitudinal measurements of food insecurity, health status, and health care utilization are needed to fully understand any potential association between food insecurity and health care utilization.
Despite these limitations, this study contributes to the scant research on the health effects of food insecurity, especially among subpopulations that are socioeconomically challenged. Lack of existing data on food insecurity, health, and health care utilization severely limits the opportunity to examine this relationship among the older adults. Our study overcomes this limitation by utilizing state-level data established by merging survey, administrative, and Medicare claims data. The data used in this study are uniquely suited for this purpose, as low-income older adults with the most critical needs are usually underrepresented in the national-level surveys. These data could also be used to better understand the distribution of older individuals with limited access to healthy affordable food and healthcare services, which is critical to identify those at high risk of food insecurity and health care burden and to strategize optimal delivery and coordination of needed services and programs to them (Lee, Shannon, & Brown, 2015).This study sheds light on the type of data needed for more in-depth investigation of trade-off decisions that resource-constrained older adults may face in fulfilling their food and health care needs. Future research should use more comprehensive data to account for other competing needs, such as housing and utility expenses, in addition to food and health care, as well as available resources such as financial (e.g., total assets) or nonfinancial (e.g., having a usual source of care and availability of health care services) factors affecting health care utilization for a more thorough examination of the link between food insecurity and health care utilization.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by University of Georgia Poverty and Economy Grant.