
Abstract
Although existing cross-sectional research suggests that dependent older family members’ resistive behavior (care-recipient [CR] resistance: verbal or nonverbal rejection or resistance toward caregiver [CG] assistance) can be challenging for informal family CGs, we know little about the impact of the occurrence patterns of CR-resistance—average frequency versus daily fluctuation—on CG emotional and physical well-being. To document CGs’ daily experiences with CR-resistance and their emotional and physical well-being, the present study applied short-term repeated measures, collecting data on 8 consecutive days from 63 CGs in Southern Arizona, the United States. Multilevel modeling of the daily data revealed that neither average frequency nor daily fluctuation in CR-resistance alone had a significant impact on CG emotional/physical health. However, the combination of experiencing relatively high frequency and high daily fluctuation in CR-resistance was associated with significant increases in CG physical health symptoms (b = .34, p < .01). Specifically, on days when a CG faced more CR-resistance than his or her usual amount, significant increases in physical health symptoms existed for CGs with relatively high average frequency of CR-resistance, but not for CGs with relatively low average frequency of CR-resistance. Based on our results, it appears that monitoring and maintaining a reasonable level of CR-resistance are effective strategies to maintain CG resilience to the negative impact of CR-resistance daily fluctuation. The findings are interpreted in light of Stress Theory, and recommendations for future research and practical interventions are offered.
Among the various stressors faced by family caregivers (CGs) of dependent elders who require personal care and/or daily activity assistance (e.g., individuals with dementia, pulmonary diseases, other cognitive, and functional limitations), researchers have consistently found that care-recipient (CR) problem-behaviors, including verbal or physical aggression, agitation, and resistance or uncooperative behaviors, have a significant, negative emotional, and/or physical impact on CGs (e.g., Hooker et al., 2002; Pinquart & Sörensen, 2003). Scholars have suggested that the negative impact of CR problem-behaviors on CG emotional and physical well-being may be accounted for partially by the unpredictable nature of those behaviors as compared with other more predictable CG stressors, such as CR cognitive and functional status (e.g., Mahoney, Trudeau, Penyack, & MacLeod, 2006; Ornstein & Gaugler, 2012). Some studies further suggest that the degree of negative emotional and/or physical impact on CGs varies depending on the specific type of CR problem-behavior (e.g., angry and physically aggressive vs. waking CG up at night; Covinsky et al., 2003; Davis & Tremont, 2007), although further investigation is needed in this area (Ornstein & Gaugler, 2012). Interestingly, another set of studies begins to suggest that patterns of occurrence differ across different types of CR problem-behaviors (e.g., Fauth, Zarit, Femia, Hofer, & Stephens, 2006; Malone Beach, Zarit, & Farbman, 1995). Whereas certain kinds of CR problem-behaviors occur inconsistently with fluctuation in their frequency or intensity in any given week, month, or year, other kinds occur fairly evenly and/or consistently without fluctuation. Despite reported differences in types and occurrence patterns of CR problem-behaviors, in the extant CG literature, CR problem-behaviors have most typically been investigated with a variety of global measures (e.g., Cohen-Mansfield & Billing, 1986; Ornstein & Gaugler, 2012; Zarit, Reever, & Bach-Peterson, 1980). With global measures, different types of CR problem-behaviors are typically aggregated or summed in a single, global score; thus, the varying occurrence patterns of different CR problem-behaviors across different time periods and CG contexts are also aggregated or summed. Then, the link between the global score (instead of separate scores for each type of CR problem-behavior) and CG well-being is examined. Notably, a recent systematic review article on CR problem-behavior studies by Ornstein and Gaugler (2012) addresses the need to reconceptualize CR problem-behavior and move away from the use of global measures. Ornstein and Gaugler urge scholars to closely examine specific CR problem-behaviors to understand the specific ways that each may negatively affect CG emotional and physical well-being. Informed by existing research and selected principles from Stress Theory (e.g., Lazarus & Folkman, 1984; Pearlin, Mullan, Semple, & Skaff, 1990), the present study focuses on a specific type of CR problem-behavior—CR-resistance (resistiveness to the CG) during personal/daily care provision. Our aims are to (a) document and capture details of daily occurrence patterns of CR-resistance, and (b) examine the impact of occurrence patterns—the average occurrence and the daily fluctuation of CR-resistance—on CG emotional and physical health with quantitative multilevel analyses.
Background
As noted above, the impact of CR problem-behaviors on CG well-being has typically been examined via a global behavior score that encompasses different types of CR-behaviors (e.g., verbal/physical aggression, wandering, repetitive behavior, resistance to care; Alspaugh, Stephens, Townsend, Zarit, & Greene, 1999; Hooker et al., 2002). When measured as such, most studies have found that CR problem-behaviors as a whole have a significant association with various negative indicators of CG emotional and physical well-being. CGs who report higher global CR problem-behavior scores (mean or total scores of CR problem-behavior frequency and/or severity over a certain CG period) report elevated levels of CG negative health symptoms, such as depressive symptoms (e.g., Clyburn, Stones, Hadjistavropoulos, & Tuokko, 2000), feelings of burden (e.g., Mohamed, Rosenheck, Lyketsos, & Schneider, 2010), physical health symptoms (e.g., Hooker et al., 2002), and perceived overload (e.g., Lawrence, Tennstedt, & Assmann, 1998), compared with those CGs who report lower global CR problem-behavior scores.
However, Stress Theory (e.g., Pearlin et al., 1990), perhaps the most commonly utilized theoretical framework in the CG literature, suggests that the impact of specific CG stressors on CG well-being would vary depending on CG evaluation of their situation including their particular stressors and available resources. In other words, certain types of CR problem-behaviors (e.g., waking CG up at night) might not be as stressful for CGs with certain resources (e.g., good health, available social support, CG efficacy) compared with other types (e.g., angry resistance to taking medications or to going to the doctor). It is surprising that majority of CR problem-behavior empirical studies continue to utilize global CR problem-behavior measures and do not address the possibility of the differential impact of different types of CR problem-behaviors on CG emotional and physical health.
With the frequent use of global measures in the current literature, several major questions remain unaddressed, particularly pertaining to the unpredictable nature (occurrence and trajectory) of CR problem-behaviors. For example, how often and according to what patterns do CGs face these specific types of problem-behaviors (e.g., every day, a few days in the past month)? And, does the predictability of occurrence patterns (e.g., consistent but relatively high occurrence, unpredictable daily fluctuation) differently influence CG emotional and physical well-being? It is possible that the differential impact of CR problem-behaviors on CG well-being may be due not so much to the fact that it is a certain type of problem-behavior and more to a certain pattern of occurrence—unpredictable fluctuation versus predictable stable occurrence.
Occurrence Pattern in CR Problem-Behaviors
In the extant CG literature, research designs with one-time data collection still predominate for convenience reasons (e.g., cost-effectiveness), and research within the CR problem-behavior literature is no exception. However, several longitudinal studies, with multiple data points over a 3-month to 3-year time frame, have documented the changing and/or unpredictable nature of CR problem-behaviors. Interestingly, these studies have consistently found that whereas changes over time in CR problem-behaviors are significant predictors of changes in CG emotional and physical health over time, changes in other CG stressors, such as care assistance demands in CR daily activities, are not (Alspaugh et al., 1999; Hooker et al., 2002). These findings shed light on the importance of investigating changes in CR problem-behaviors and the impact of occurrence patterns on CG emotional and physical well-being. Indeed, the significant impact of changes particularly in CR problem-behaviors (but not in CR care assistance demands) on CG well-being could be partially accounted for by their occurrence pattern—which is perhaps a relatively unpredictable one for many CGs.
The significance of unpredictability is fundamental within Stress Theory (e.g., Lazarus & Folkman, 1984; Pearlin et al., 1990). Stress Theory suggests that unpredictable stressors are likely to trigger greater stress in individuals than more predictable stressors would. As such, unpredictable changes in CR problem-behaviors pose more emotional and/or physical challenges to CGs than the more predictable changes in other CG stressors, such as level of required care, which often coincides with expected CR cognitive and functional decline. Assessing patterns of occurrence (and thus unpredictability) raises the issue of measurement timing. Stress scholars, such as Pearlin and his colleagues (1990), who have attempted to capture care-related changes typically refer to “care-related change” from a rather long-term perspective—over months or years. However, empirical studies suggest that CGs can face changes and transitions over much shorter periods (e.g., Fauth et al., 2006; Koerner & Yenyon, 2007; Malone Beach et al., 1995), such as over weeks or even days. In fact, in a qualitative investigation of CG experience of CR-resistance, unpredictability of CR behavior during day-to-day care provision was identified as a major stressor for CGs (Mahoney et al., 2006). We propose that it may be such day-to-day fluctuation (daily unpredictable pattern) in key CR problem-behaviors that is critical to understanding the emotional and physical challenges of family CGs .
Daily Fluctuation in CR Problem-Behaviors
To date, only a few studies have examined CR problem-behaviors via a daily longitudinal study method; unfortunately, in those studies, day-to-day fluctuation (within-person variance) was determined using global measures of CR problem-behaviors via a summed or averaged daily occurrence of a wide range of CR problem-behaviors. These scores do not capture day-to-day fluctuation of key specific CR problem-behaviors (e.g., physical aggression, resistiveness to care). Nonetheless, these studies have documented significant within-person (CG), across-day variability in the occurrence of CR problem-behaviors as a whole (e.g., Fauth et al., 2006; Koerner & Yenyon, 2007). Koerner and Yenyon (2007) further determined the impact of daily variance in averaged CR problem-behavior on daily variability in CG emotional and physical well-being. Based on 8 consecutive days of daily data from the current study sample, within-person analyses revealed that, on days when CGs experienced more CR problem-behaviors than their average, CGs reported an increased level of depressive symptoms, feelings of burden, and physical symptoms compared with their average. These daily diary studies confirm the impact of occurrence pattern (daily variability) in CR problem-behavior on the daily fluctuation of CG well-being. However, the impact of daily fluctuations of specific CR problem-behaviors has not been investigated. It is certainly possible that the significant daily variability found in CR problem-behaviors as a whole (as a global score) and the impact of that fluctuation on CG emotional and/or physical well-being could be largely a function of certain subtypes of CR problem-behavior such as CR-resistance. The present study focuses on one key, specific CR problem-behavior—CR-resistance—to capture the unique characteristics of this CR problem-behavior with regard to occurrence pattern and the potential impact of the occurrence pattern on CG emotional and physical health.
CR-Resistance
CR-resistance is verbal or nonverbal rejection or resistance by dependent elders toward their CGs. CR-resistance itself has received little research attention, except by a small group of researchers (e.g., Hammar, Emami, Götell, & Engström, 2011; Mahoney et al., 1999; Mahoney et al., 2006; McGilton, Sidani, Boscart, Guruge, & Brown, 2012; Volicer & Hurley, 2003). With an in-depth examination of CR-resistance among dementia patients at long-term care facilities, Mahoney and her colleagues (1999) identified three factors within CR-resistance: physical resistive behaviors (defensive to offensive), vocal or emotional resistance, and protective or reflexive resistance. Mahoney et al. (1999) also pointed out an important contextual difference—that CR-resistance was most frequently reported when nursing home residents were approached by CGs (Mahoney et al., 1999; Rowe, Straneva, Colling, & Grabo, 2000), whereas other CR problem-behaviors were most frequently reported when nursing home residents were alone and unoccupied (Cohen-Mansfield & Billing, 1986). This means that, unlike some other CR problem-behaviors (e.g., being repetitive, wandering), CR-resistance occurs in contexts in which both CG and CR are most likely involved, and thus could directly influence CG emotional and/or physical well-being. Nonetheless, CR-resistance has been most often considered simply as a part of CR problem-behaviors viewed globally (e.g., Disruptive Behavior Scale: Beck, Baldwin, Heithoff, & Cuffel, 1990; Cohen-Mansfield Agitation Inventory: Cohen-Mansfield & Billing, 1986; Revised Memory and Behavior Problems Checklist: Teri et al., 1992) or has not been included in diagnostic measures, such as Neuropsychiatric Inventory (Cummings, 1997) and Behavioral Pathology in Alzheimer’s Disease (Reisberg, Borenstein, Franssen, & Shulman, 1986).
When CR-resistance is measured via existing global behavioral measures, it is captured directly in several items, such as verbally or physically resisting to routines, refusing to follow directions/requests (Disruptive Behavior Scale: Beck, Baldwin, Heithoff, & Cuffel, 1990; Cohen-Mansfield Agitation Inventory: Cohen-Mansfield & Billing, 1986; Revised Memory and Behavior Problems Checklist: Teri et al., 1992) and indirectly within several broader behavioral items, such as presenting verbal or physical agitation/aggression, anxiousness, difficulty concentrating on a task (e.g., Disruptive Behavior Scale, Cohen-Mansfield Agitation Inventory, Revised Memory and Behavior Problems Checklist). The major problem with examining CR-resistance via existing global behavioral measures is that occurrence of CR-resistance could be merged with broader items across different contexts (e.g., evening time, alone time, social time, care provision, meal time); researchers are not able to differentiate the CR-resistance portion to examine its unique impact on CG emotional and physical health.
Research Question and Hypotheses
Based on the current literature and selected principles of Stress Theory, the current study focuses on a specific CR problem-behavior, CR-resistance. We investigate a research question and two hypotheses:
Method
Study Design
Utilizing daily survey data and multilevel analyses, we (a) documented patterns of CR-resistance occurrence (frequencies and within- and between-person variabilities), and (b) investigated the impact of CR-resistance on CG well-being viewed from both a within-person daily variance perspective (daily fluctuation: Level 1) and a between-person 8-day mean-level perspective (average occurrence: Level 2).
Recruitment and Sample
The current study utilized existing quantitative data from the Daily Understanding of Caregiving Study (DUCS; Koerner & Yenyon, 2007). For that project, we recruited participants (N = 63) via flyers at a variety of sites in Southern Arizona (e.g., family practice clinics, geriatric clinics, medical supply and equipment store, CG support group). When potential participants called the number on the flyer, we provided information about the project and asked a set of eligibility questions. To be eligible, the caller had to (a) be the primary CG for a dependent family member (e.g., spouse, parent, in-law) who was at least 60 years of age, and (b) provide at least 10 hr/week of assistance (e.g., dressing, showering, ordering medications, helping with mobility). In addition, (c) the CR had to be community-dwelling—living in his or her own home or in the home of the CG, and could not be receiving extensive in-home professional care (for further details on the recruitment strategy, see Koerner & Yenyon, 2007).
Instruments
In the original DUCS study, each CG completed one initial questionnaire and eight daily questionnaires (DQs). The initial questionnaire tapped stable personal and other characteristics (e.g., age, gender, level of education, CG Relationship to CR). The DQs tapped CG experiences “in the past 24 hr.” For the current analyses, we utilized the DQ measures that assessed CR-resistance and three CG well-being indicators (i.e., depressive symptoms, feelings of burden, and physical symptoms).
CR-resistance
We determined occurrence of CR-resistance during care assistance on each day via 22 items adapted in part from Lawton and Brody (1969). Those 22 items included questions about assistance with Activities of Daily Living (ADL: for example, bathing/showering, mobility), Instrumental Activities of Daily Living (IADL: for example, meal preparation, transportation, arranging for services, ordering medications), and two “other” items. Participants indicated whether they had provided assistance for each of the 22 items in the past 24 hr, and if so, whether they had experienced resistance from their CR. To describe the details of CR-resistance prevalence, we reviewed the frequencies for each ADL and IADL item. To investigate the research hypotheses, we summed the responses regarding CR-resistance across the 22 items to arrive at a CR-resistance daily score for each day; those totals could range from zero through 22, with higher scores representing more occurrences of CR-resistance.
Depressive symptoms
We assessed CGs’ feelings of depression daily via six items based on Gaugler, Davey, Pearlin, and Zarit’s (2000) revised version of the Hopkins Symptom Checklist (Derogatis, Lipman, Rickels, Uhlenhuth, & Covi, 1974). Items appraised loss of energy, lack of motivation, depressed mood, and boredom. We did not include physical symptom items from the checklist because similar items were included in our Physical Symptom Scale. CGs indicated the extent to which they felt these emotions in the past 24 hr on a 4-point scale with choices ranging from 1 (not at all) through 4 (very much). Responses were averaged across the six items to arrive at a depressive symptoms score for each day. The scale had good internal consistency (α = .89).
Feelings of burden
We assessed CGs’ feelings of CG burden daily via the 12-item short version of the Zarit Burden Interview (Bédard et al., 2001). All items began with the stem, “In the past 24 hours, how much did you feel . . . ; example items included ‘that because of the time you spent with [CR] you didn’t have enough time for yourself’ and ‘you should be doing more for [CR].’” CGs responded on a 4-point scale with choices ranging from 1 (not at all) through 4 (very much). We averaged each participant’s responses across the 12 items to arrive at a feeling of CG burden score for each day. The scale had good internal consistency (α = .89).
Physical health symptoms
We asked participants to think back to the past 24 hr and check all of the physical symptoms they experienced from a list of 15 (e.g., headache, dizziness, tightness in chest) plus one “other” category (Larsen & Kasimatis, 1991). Scores reflected the sum of the checked items and therefore could range from 0 through 16 on each day.
Analysis Strategy
Preliminary analyses
Prior to conducting the primary analyses, we ran descriptive analyses via SPSS to screen normality and outliers of the variables of interest, including CR-resistance and the three CG well-being outcome variables (depressive symptoms, feelings of burden, physical heath symptoms). Statistics and histograms indicated a normal to acceptable range of distribution for all variables except CR-resistance, which was positively skewed; to meet the normal distribution requirement for the current analyses, a square-root data transformation was applied to the CR-resistance variable. Descriptive statistics also addressed part of the research question—prevalence of CR-resistance.
To determine whether CG characteristics should be included as control variables in the primary analyses, we evaluated the associations between CG age, gender, ethnicity, and the key variables of interest via either Pearson’s correlation analyses or ANOVA. Because CG age was significantly associated with an outcome variable (depressive symptoms: r = −.274, p < .05), and CG experiences of CR-resistance differed as a function of CG gender, F(2, 60) = 4.67, p = .04, we included CG age and gender as control variables in the primary analyses.
Primary analyses
To address the research question and hypotheses, we conducted a series of multilevel random coefficient analyses. Multilevel modeling (MLM), or hierarchical linear modeling (HLM; Raudenbush, Bryk, & Congdon, 2002), is a statistical approach that considers the nested relationship or nonindependence of repeated within-person measures (Nezlek, Feist, Wilson, & Plesko, 2001)—8 days of data: Level 1 variables, nested within CGs: Level 2 variables, for the current study. We addressed the research question and hypotheses via two different MLM models: unconditional models and Level 2 models.
Unconditional models
Unconditional models, addressing the research question, documented within-person and between-person variability in CR-resistance without any control or predictor variables. We conducted a series of MLM unconditional models to document both within-person across-day (Level 1) and between-person (Level 2) variability in CR-resistance and, additionally, the three CG well-being variables (i.e., daily depressive symptoms, feelings of burden, and physical health symptoms).
Level 2 models
Level 2 models, addressing RH1 and RH2, examined the impact of CR-resistance on CG emotional/physical well-being at two different levels—Level 1: Daily CR-resistance Fluctuation (daily ups and downs from CG’s own average) and Level 2: differences in Person-Mean CR-resistance (average occurrence cross 8 survey days for each CG), including the interaction effect of these two levels. We conducted a series of MLM Level 2 analyses with these Level l (Daily CR-resistance Fluctuation) and Level 2 (Person-Mean CR-resistance) predictors for both intercept and slope for each of the three CG well-being outcome variables, CG depressive symptoms, feelings of burden, and physical health symptoms. We used the following model, illustrated here with depressive symptoms (DepS) as the well-being variable:


At Level 1, DepS refers to CG depressive symptoms for Person
t
on Day
i
: a function of the intercept,
Results
Table 1 presents the demographic information of DUCS participants (N = 63). Table 2 presents basic descriptive (means, standard deviations, range) and correlation results for the three CG well-being variables (i.e., depressive symptoms, feeling of burden, and physical health symptoms) and CR-resistance.
Demographic Characteristics of the Sample.
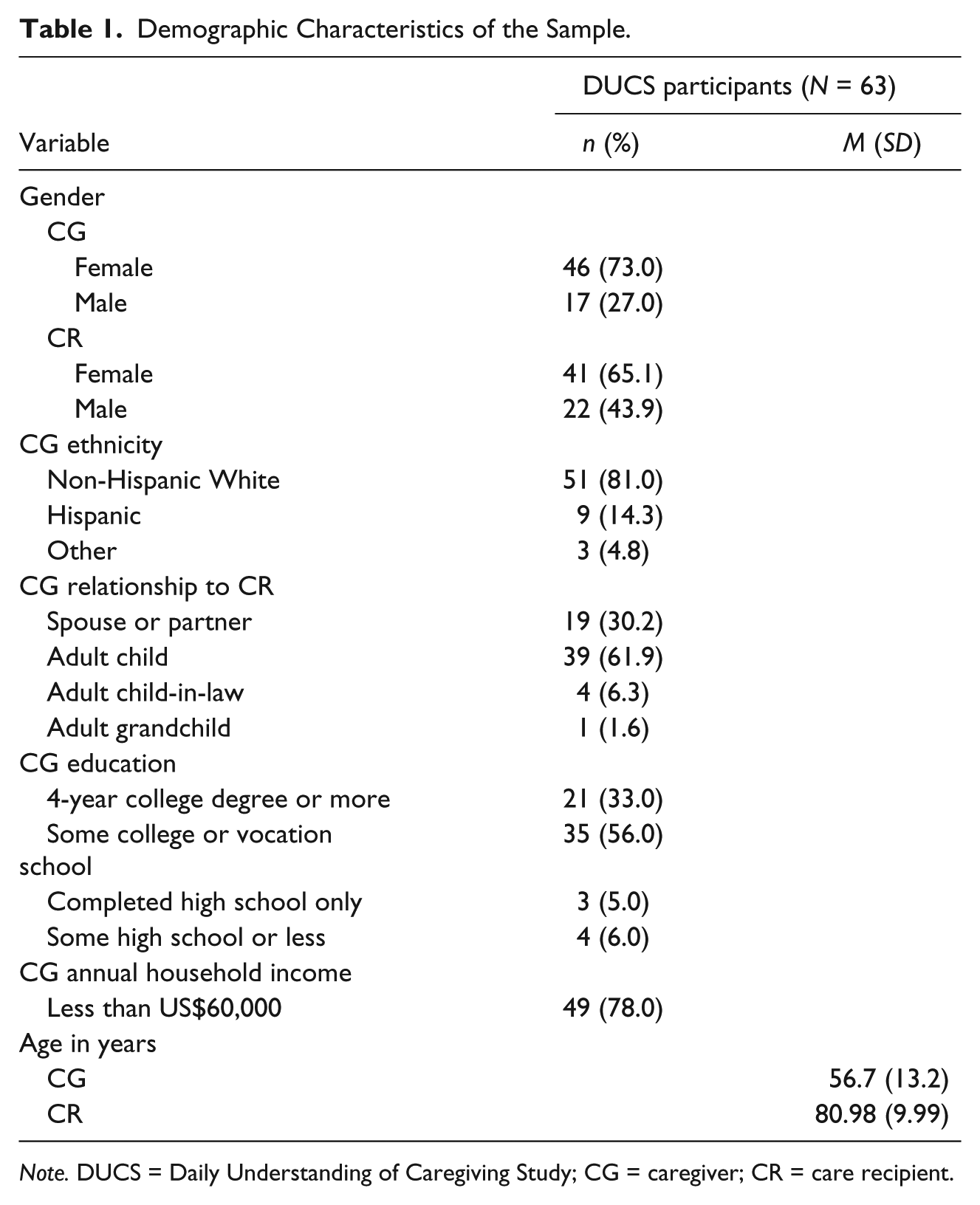
Note. DUCS = Daily Understanding of Caregiving Study; CG = caregiver; CR = care recipient.
Eight-Day Average Score of CR-Resistance, CG Depressive Symptoms, Feelings of Burden and Physical Health Symptoms, and Correlation Results (N = 63).
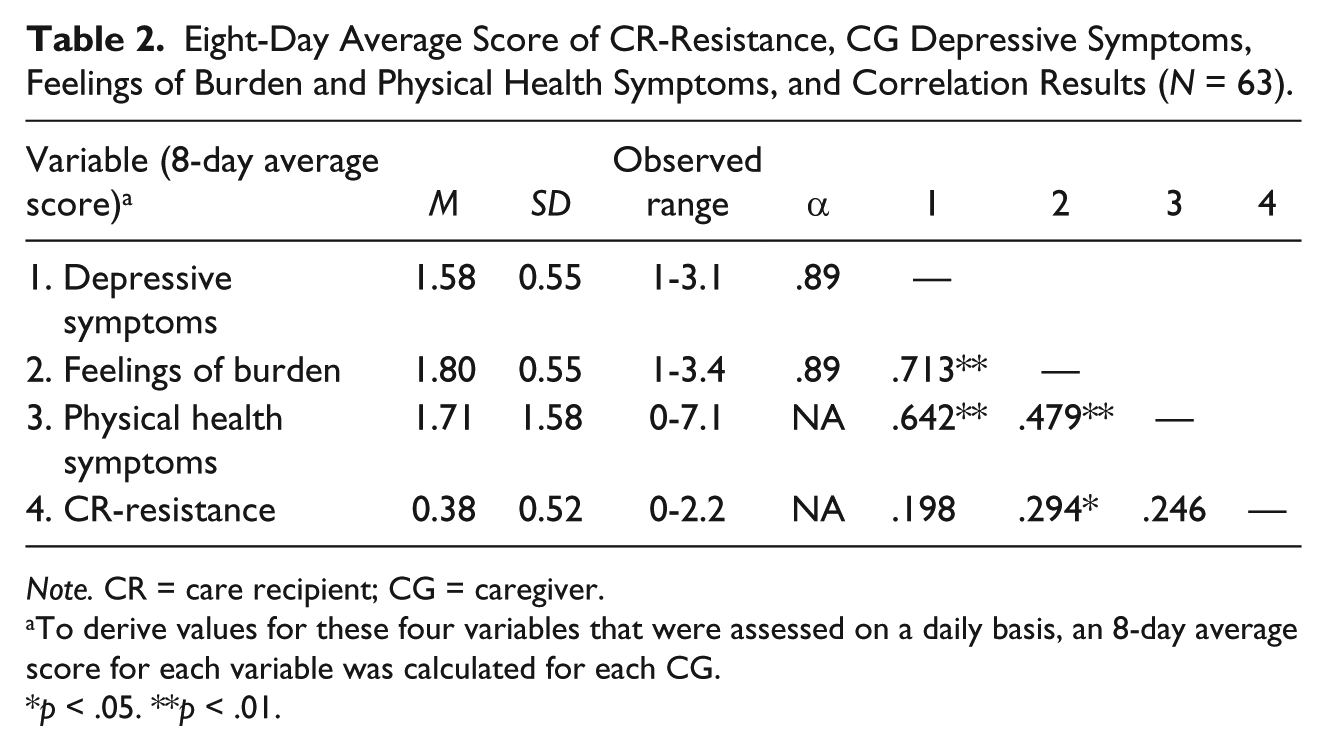
Note. CR = care recipient; CG = caregiver.
To derive values for these four variables that were assessed on a daily basis, an 8-day average score for each variable was calculated for each CG.
p < .05. **p < .01.
Table 3 presents frequencies of CR-resistance. Of the 63 DUCS survey participants, 31 reported that they experienced CR-resistance. Over the 8 survey days, whereas many CGs experienced CR-resistance on only a few days (1-2 days, n = 18), some CGs experienced CR-resistance on several days (3-6 days, n = 11), and the others experienced CR-resistance nearly every day (7-8 days, n = 2). CGs also experienced CR-resistance across different numbers of daily personal care and assistance activities on a given day (i.e., ADL and IADL items); whereas many CRs displayed resistance behavior only in a few activities (1-3 activities, n = 23), others displayed resistance behavior across a wide range of activities (4-10 activities, n = 7). The most frequent resistance was reported during ADL items, including dressing (n = 21), transferring (n = 21), walking/using wheelchair (n = 20), bathing (n = 19), grooming (n = 13), and toileting (n = 12) assistance, whereas relatively low frequency of CR-resistance (n = 2-7) was reported during IADL assistance (e.g., laundry, personal finance, shopping assistance) with exception of medication assistance (n = 18). Table 4 presents the results of the MLM unconditional models, providing statistics regarding variability in within-person (Level 1—σ2: Daily CR-resistance Fluctuation in each CG) and between-person (Level 2—τ: among CG participants) differences in CR-resistance. According to the unconditional model results, CGs were more likely to vary from themselves across the 8 survey days than from each other; 61% of the variance in CR-resistance existed within-person across days.
CR-Resistance Occurrence Over the 8-Survey Days and Across 22 Possible Care/Support Activities.
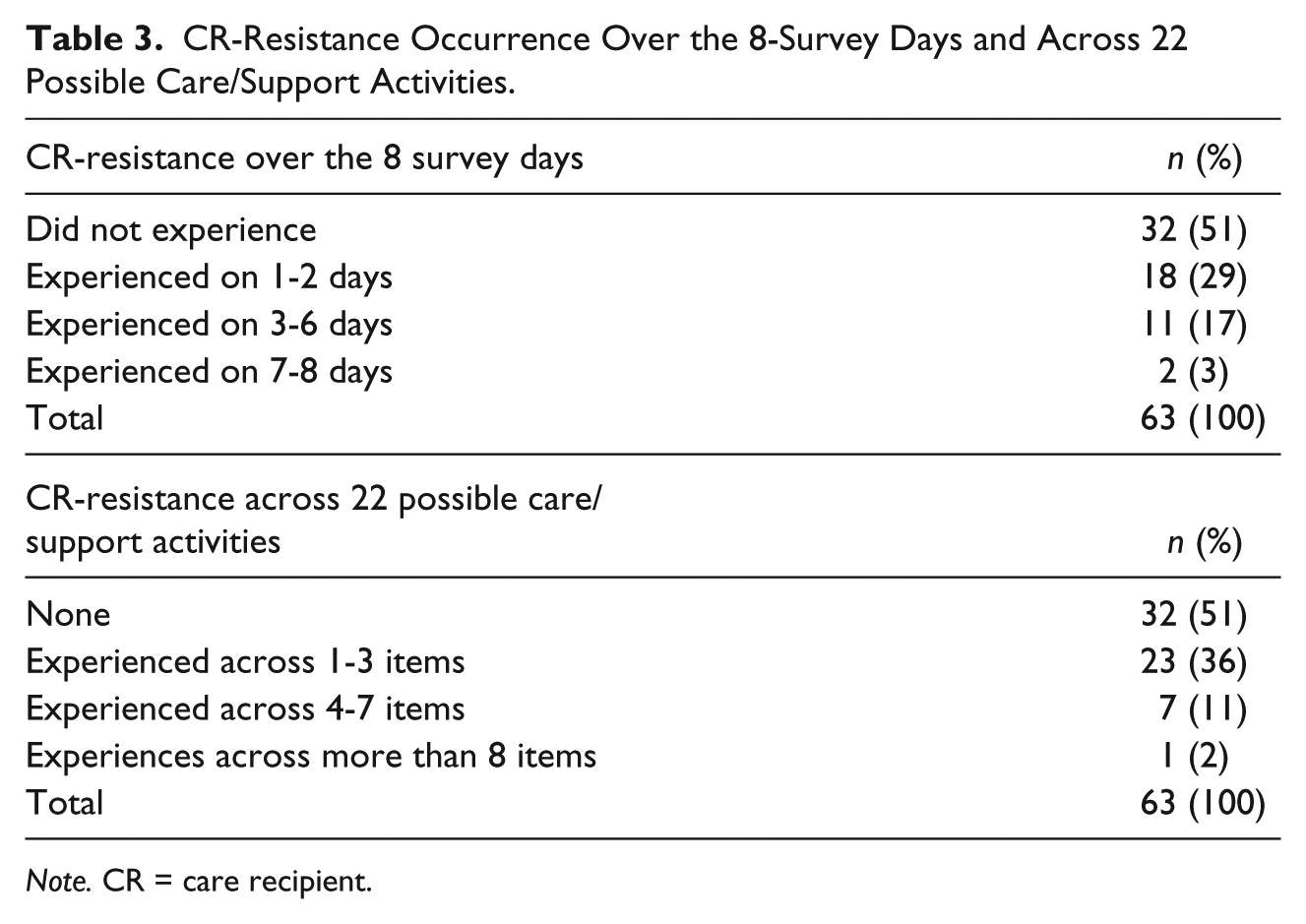
Note. CR = care recipient.
Multilevel Modeling Regressions of Unconditional Models and Level 2 Models: CR-Resistance Predicting Caregiver Well-Being.
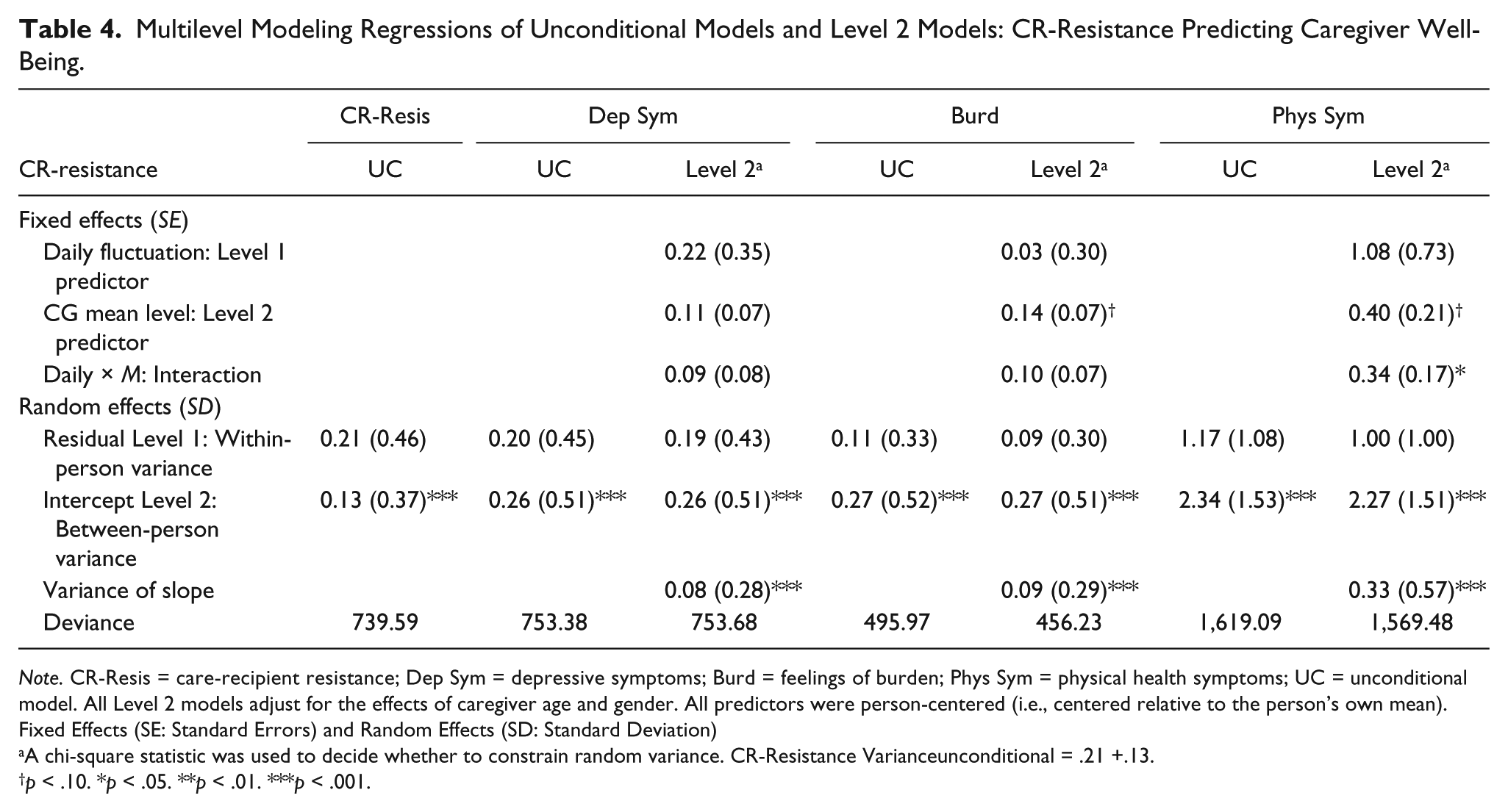
Note. CR-Resis = care-recipient resistance; Dep Sym = depressive symptoms; Burd = feelings of burden; Phys Sym = physical health symptoms; UC = unconditional model. All Level 2 models adjust for the effects of caregiver age and gender. All predictors were person-centered (i.e., centered relative to the person’s own mean). Fixed Effects (SE: Standard Errors) and Random Effects (SD: Standard Deviation)
A chi-square statistic was used to decide whether to constrain random variance. CR-Resistance Varianceunconditional = .21 +.13.
p < .10. *p < .05. **p < .01. ***p < .001.
Table 4 presents results of the MLM Level 2 model. Contrary to our hypotheses, the results indicate that neither Daily CR-resistance Fluctuation (daily ups and downs from CG’s own average, Level 1 predictor) nor differences in Person-Mean CR-resistance (average occurrence across 8 survey days for each CG, Level 2 predictor) by itself were significantly associated with the daily fluctuation in CG well-being. However, the results revealed a significant interaction effect between these two levels: Person-Mean CR-resistance and Daily CR-resistance Fluctuation, on physical health symptoms (b = .34, SE = 0.17, p < .01). Specifically, on days when a CG faced more CR-resistance than his or her usual amount, significant increases in physical health symptoms existed for CGs with relatively high Person-Mean CR-resistance scores, but not for CGs with relatively low Person-Mean CR-resistance scores. Simple slope analyses further revealed that for CGs with higher Person-Mean CR-resistance scores, having a one unit increase in CR-resistance on a given day was associated with a 1.42 unit increase in physical health symptoms (p < .05). For CGs with lower Person-Mean CR-resistance scores, Daily CR-resistance Fluctuation was not significantly associated with changes in physical health symptoms.
Discussion
By utilizing a daily diary assessment technique, the present study brought a unique and focused lens to the scholarship on family CGs’ experience of CR-resistance during daily care activities. The findings confirm the importance of close examination of specific CG stressors—in this case CR-resistance—for which short-term fluctuation has been identified; and a similar approach could be applied to the study of other potential CG stressors (e.g., CR falls, physical aggression, bathroom incidents, urgent or emergency care visits, family arguments) and their link to daily ups and downs in CG well-being.
To date, researchers interested in CG experiences have relied largely on global CR problem-behavior instruments, which aggregate across numerous types of CR problem-behaviors; thus, the varying occurrence patterns of different CR problem-behaviors across time (including days), as well as CG contexts, are blurred. Indeed, using global instruments, CR-resistance during daily care assistance is made indistinct from all other problem-behaviors (e.g., verbal aggression, waking the CG up at night, toileting accidents, withdrawal), and its specific pattern of occurrence for any particular CG (e.g., a few days per week, daily) is disregarded. Ignoring the occurrence patterns of specific CR problem-behaviors is at odds with Stress Theory. According to Stress Theory (e.g., Lazarus & Folkman, 1984; Pearlin et al., 1990) and its emphasis on specific and unpredictable stressors, different CR problem-behaviors (stressors) and their occurrence patterns (as regard to predictability) are likely to have varying impacts on CG emotional and physical health.
With our daily data, we learned that about half of the CG participants reported experiences of CR-resistance during their 8 survey days. This proportion of CGs who experienced CR-resistance is consistent with a previous study (55%; Rowe et al., 2000), confirming that CR-resistance is a common phenomenon faced by family. Notably, we also found that CGs reported more frequent CR-resistance during basic ADLs (e.g., dressing, transferring, walking/using wheelchair, bathing, grooming, and toileting) as compared with during IADL (e.g., personal finance, laundry). ADL activities are typically part of a necessary daily routine for personal care and often require CG initiative, whereas IADL activities usually do not require CG physical assistance and have some flexibility with regard to timing to be accomplished. The difference in CR-resistance likelihood associated with ADL assistance in comparison with IADL assistance is consistent with existing studies, which have shown that CR-resistance most often occurred during personal care activities (e.g., Mahoney et al., 1999; Mahoney et al., 2006; Sloane et al., 2004).
Regarding occurrence patterns in the current study, the HLM unconditional model showed that a larger portion of variance (61%) in CR-resistance was due to day-to-day fluctuation within individual CGs (daily up and downs), whereas a smaller portion of variance (39%) was due to differences in average occurrence among the CG participants (differences in average level among the CGs). In a typical cross-sectional study that examines the impact of CR problem-behaviors with only one data point, researchers are only able to investigate the impact of CR-resistance in regard to the mean difference among the CGs (in this study, the smaller portion of variance: 39%). The large proportion of variance in Daily CR-resistance Fluctuation (61%) justifies the importance of the current study investigating the impact of CR-resistance daily fluctuation on family CG emotional and physical well-being.
In the current study, we examined impact of both within- and between-person variation of CR-resistance on CG emotional and physical well-being. Contrary to our hypotheses, which were based on the extant literature (e.g., Hooker et al., 2002; Ornstein & Gaugler, 2012) and selected principles from Stress Theory (e.g., Pearlin et al., 1990), our multilevel analyses revealed that neither having relatively high average CR-resistance occurrence nor having a relatively great degree of Daily CR-resistance Fluctuation by themselves was associated with CG emotional and physical well-being as assessed via depressive symptoms, feelings of burden, and physical health symptoms. However, for those CGs who have a relatively high average experience of CR-resistance compared with their counterparts, on days when they faced more CR-resistance than their usual amount, significant increases in physical health symptoms resulted. We interpret this result through the lens of the Stress Theory (Lazarus & Folkman, 1984; Pearlin et al., 1990) and, in particular, the precept of daily hassles. According to Stress Theory, the pileup of daily hassles and stressors can pose a greater risk to an individual’s well-being than facing a single significant life event (e.g., Sheidow, Henry, Tolan, & Strachan, 2014; Stefanek, Strohmeier, Fandrem, & Spiel, 2012). CGs in the current study who reported relatively high average occurrence of CR-resistance—a pileup of daily care hassles—might have been worked to the brink of what they could physically and emotionally manage. Thus, they were not able to attend to their additional and unpredictable CR-resistance demands with the best ability and approach, affecting their physical health symptoms.
It is surprising that, in our quantitative analyses, the interaction effect between the mean level and daily fluctuation of CR-resistance was observed only in CG physical health symptoms and not in emotional health indicators, such as CG depressive symptoms and feelings of burden. In our previous study using the same sample (Koerner, Shirai, & Kenyon, 2010), the negative impact of the daily fluctuation in CR problem-behavior as a whole (measured via a global scale) was found in both the emotional and physical health indicators. In the current study, we closely examined the impact of one key CR problem-behavior—CR-resistance; the significant effect of daily fluctuation only on CG physical symptoms may shed light on a unique aspect of this specific CR problem-behavior. The incidents of CR-resistance were reported in the daily necessary care activities that often require personal and physical assistance including dressing, transferring, walking, and bathing. In fact, Hammar et al. (2011) found that pulling away (as opposed to verbal resistance) was the most common CR resistive response during morning care activities. Perhaps, such physical resistance during personal care activities poses additional physical demands on CGs, considering the fact that most family CGs provide such ADL assistance without much training and in isolation (e.g., Mahoney et al., 2006). However, we should cautiously interpret this significant interaction effect between the mean level and daily fluctuation of CR-resistance on CG physical health symptoms as a causal relationship. The participant CGs simultaneously reported their daily experiences of CR-resistance and physical health symptoms. Without examination of time-lagged effects, we cannot know whether these CGs experienced CR-resistance first, and then experienced declines in their physical well-being. A reversed and/or bidirectional causation may exist; it is possible that for CGs with a relatively high average level of CR-resistance, an elevated level of CG physical health symptoms caused an increased number of CR-resistance incidents because these CGs were not able to provide efficient personal care assistance to their CRs due to their worsened physical condition on that particular day. Future investigation of the potential differential impact of CR physical and verbal resistance on CG well-being would clarify the current results.
Regardless of the causal directions of the CG physical health symptoms and CR-resistance, based on our results, it appears that monitoring and maintaining a reasonable level of CR-resistance are effective strategies to maintain CG resilience to the negative impact of CR-resistance daily fluctuation. With limited resources for CG support and the large investment that would be required for delivering individualized interventions, it seems prudent to identify at-risk CGs with a relatively high average level of CR-resistance. Developing a CR-resistance checklist for CGs that quickly assesses overall CR-resistance during their provision of daily care could be an important first step for identifying at-risk CGs most in need of support in dealing with CR-resistance. For at-risk CGs, an intensive intervention should be designed based on real-time and home observations during which interventionists capture the complexity of the CR–CG relationship and other CG demands and stressors (Mahoney et al., 2006); whereas for CGs with moderate CR-resistance demands, less intensive (group or informational) interventions could be provided.
Review articles also show that evidence-based psychological treatments with trained clinicians are effective to reduce destructive CR-behaviors (Logsdon, McCurry, & Teri, 2007) and to provide support to family CGs managing CG-related stressors (Gallagher-Thompson & Coon, 2007). Although centered on formal care as opposed to informal family care settings, a few professional CG studies investigated feasible interventions to reduce CG stressors. For example, Götell, Brown, and Ekman (2002) introduced Music Therapeutic Caregiving (MTC) in which a CG and the CR sing together while they are engaging in personal care activities to promote positive interaction between them. Hammar et al. (2011) investigated the effect of MTC specifically to reduce CR-resistance during morning care activities; they found, using a comparison-group design, that MTC is an effective intervention to reduce resistance behavior. Another promising intervention is an application of Person-Centered Caregiving in which CRs are treated and communicated in person-centered ways instead of provider (institutional)-driven ways (e.g., Burgio et al., 2001; Lann-Wolcott, Medvene, & Williams, 2011). Lann-Wolcott and colleagues (2011) found that Person-Centered CG was significantly and negatively associated with resistiveness to care. These methods of improving the CG–CR relationship for reducing CR-resistance during personal care activities could be easily implemented via family CG brochures, online features, and group information sessions at minimal costs. Perhaps these interventions would provide reasonable solutions for CGs with high average level of CR-resistance who is vulnerable to Daily CR-resistance Fluctuation.
Limitations and Future Directions
Although the current study provides valuable insights for future research projects and development of effective and feasible family CG interventions, the findings must be interpreted in light of the study’s limitations. First, the current sample is relatively small and admittedly nonrepresentative, so generalizability of the findings may be limited. However, the application of short-term repeated daily measures increases statistical power to detect meaningful micro-level (Level 1) and macro-level (Level 2) associations with a fairly small sample size (Singer & Willett, 2003). Although the current study sample size is not ideal for the examination of complex contextual factors related to CG experience of CR-resistance, the study provides a generalizable strategy and information for developing future research and interventions pertaining to daily variation of CG stressors and its relationship to CG well-being. CR-resistance, a key CG stressor, often fluctuates daily, and that daily variation is associated with CG daily fluctuation in CG physical health symptoms for specific CGs (who have relatively high occurrence of CR-resistance). With daily study results, professionals would have numerical data upon which to develop meaningful interventions and tools for the most vulnerable CGs who require extensive assistance. Second, we implemented an 8-consecutive-day daily survey to capture a typical week including week days and one weekend. However, CG experiences of CR-resistance can change over time through years of CG. Although it could bring additional burden on funding, time, and participant CGs, a longer term daily survey or an 8-day daily study repeated over an extended period, for instance, annual 12-day daily surveys over 5 years, would be ideal to capture both daily and long-term changes in CR-resistance and CG experiences. Third, the current daily surveys captured the sheer occurrence of CR-resistance during their daily activities of CG tasks (i.e., ADLs and IADLs) but did not tap potential varied severity of CR-resistance. CR-resistance can vary from gestural and verbal rejection to physically aggressive resistance, such as pulling, biting, and hitting. One physically aggressive rejection by a CR may have a much greater impact on CG well-being than multiple verbal rejections. Varied severity of CR-resistance should be also considered in future studies. Finally, CR-resistance and other CR problem-behaviors occur within a larger CG context. As some research suggests, the potential impact of the CG–CR relationship on CG problem-behaviors and CG emotional well-being (e.g., Lawrence et al., 1998), a reciprocal association wherein CG emotional and physical well-being might also influence the occurrence of CR-resistance, may better describe the phenomenon. This reciprocal or CG–CR dyadic model and other CG-related variables within the Stress Theory framework, such as sense of efficacy, relationship to the CR, type of disability, social support, and other life stressors, should be further explored. Qualitative interviews would also provide in-depth information on CG experiences of CR-resistance necessary to develop meaningful intervention programs, such as CG emotional reactions and the contextual factors (Kenny, Sarma, & Egan, 2012) of their caregiving experiences.
Conclusion
Among the various stressors faced by family CGs of dependent elders, researchers have consistently found that CR problem-behaviors have a significant, negative emotional and/or physical impact on CGs (e.g., Hooker et al., 2002; Pinquart & Sörensen, 2003). Ornstein and Gaugler (2012), in their recent systematic review article of CR problem-behavior studies, called for a methodological shift in how researchers examine the impact of CR problem-behavior on CG emotional health and well-being. They encouraged researchers to look into specific types of CR problem-behaviors instead of using global, summarizing measures, which average across a wide range of CR problem-behavior types. The present study not only directly responded to this recommendation by focusing exclusively on a specific CR problem-behavior—CR-resistance—it also addressed an important additional key component of CR problem-behaviors—occurrence pattern. By documenting occurrence patterns of CR-resistance and exploring the impact of the occurrence patterns on CG emotional and physical well-being, we proposed to help explain untapped potential causes of CG emotional and physical distress.
The quantitative documentation of CR-resistance yielded results that are consistent with the extant literature indicating that (a) about half of CGs experience CR-resistance (Rowe et al., 2000), (b) CR-resistance most often occurs in CG tasks that require CG initiative and CR-cooperation (Mahoney et al., 1999), and (c) the occurrence of CR problem-behaviors, as a group (summed or averaged occurrence of a wide range of CR problem-behaviors on a given day), varies day to day (Fauth et al., 2006; Koerner & Yenyon, 2007; Malone Beach et al., 1995). The current study provides additional information that CGs who experience the specific combination of relatively high average frequency and relatively high daily fluctuation of CR-resistance are most vulnerable for heightened physical health symptoms. We suggest that this interaction effect of CG mean level and daily fluctuation is a key factor to explore in future research efforts examining other key CG stressors for developing effective and efficient CG intervention strategies.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.