
Abstract
The number of older adults residing in assisted living facilities (ALF) and utilizing adult day care services is expanding with the increasing population of older adults. Currently, there are no standardized requirements for continuing education for assisted living and adult day care service staff at a national level. Given that 62% of states within the United States require continuing education for ALF staff and/or administrators, a more formalized system is needed that provides evidence-based gerontological training to enhance the quality of care and services provided to older adults. This article describes the challenges and lessons learned from conducting a program evaluation of a Statewide Training and Continuing Education Program for Assisted Living Facility and Adult Day Care Service staff in Virginia. Survey evaluation data from a 6-year period was examined and a formative program evaluation was conducted. The findings from the survey evaluation and formative evaluation are discussed as are the lessons learned.
Keywords
The number of older adults residing in assisted living facilities (ALF) and utilizing adult day care center (ADCC) services is increasing as older adults and their family members seek alternatives to traditional nursing home care (White & Cadiz, 2013). Given that ALF and ADCC facilities are regulated by individual states, training requirements are inconsistent and vary considerably. Yet, it is well established that a trained and educated workforce is essential for providing quality care for older adults (Tolson et al., 2011). Sengupta, Ejaz, and Harris-Kijetin (2012) found that when compared with professional caregivers employed by home health providers, certified nursing assistants (CNAs) working in long-term care were less likely to feel that their job training had prepared them “well” for their current position. Kemper et al. (2008) found that job satisfaction for direct care workers in ALF could improve if there was an increase in the frequency of opportunities for staff to engage in job-related training and continuing education. In addition to increasing the frequency of training sessions offered, it is essential to recognize that quality training and continuing education opportunities for the direct care workforce must be offered to meet the gaps and make connections from previously gained knowledge to be effective (as described by Needs Theory, Maslow, 1943; McClelland, 1978).
In the State of Virginia, it is a requirement for staff in Virginia’s 569 licensed ALFs and 72 ADCCs to complete at least 8 to 16 hr of annual training based upon license type (i.e., residential only vs. residential and assisted living). As well, regulation changes for ALF administrators in 2008 resulted in continuing education requirements of at least 20 hr of training related to management or operation of a residential facility for adults within 12 months from the date of employment and annually thereafter to renew an assisted living administrator license. ALF and ADCC administrators manage and coordinate all services for older adults within their facilities. Administrators have the responsibility of ensuring that all staff provides quality care and services and that resident/client needs are continually met. Although requirements vary, most states require licensure for assisted living administrators. Most typically, administrators must hold a minimum of a 4-year degree, pass a licensing exam (the National Association of Long-Term Care Administration Boards), and complete a state-approved training program.
Currently, there are only five states within the United States (Colorado, District of Columbia, Hawaii, Mississippi, and Utah) that do not specify any continuing education requirements for administrators and/or staff members. The required training hours vary widely for the states that do specify requirements for continuing education for assisted living administrators and staff. For example, continuing education requirements for administrators can range from 6 to 30 hr per year, whereas continuing education requirements for staff can range from 2 to 24 hr per year (National Center for Assisted Living, 2013). Sixty-two percent of the states with specific requirements for continuing education do not specify an agency that approves the continuing education programs (National Center for Assisted Living, 2013).
In Virginia, the Virginia Department of Social Services (VDSS) is responsible for monitoring compliance with annual training requirements for ALF and ADCC staff. Annual inspections by VDSS licensing inspectors follow an approved protocol to ensure compliance for all standards and regulations established by the VDSS. Licensing inspectors attend initial training regarding division practices and shadow veteran inspectors in the field. However, at this time, there is no requirement for the licensing inspectors’ themselves to attend training and continuing education on an ongoing basis.
To address the need for required ongoing continuing education for ALF and ADCC staff, the Department of Gerontology at Virginia Commonwealth University partnered with the VDSS to develop and implement a system of coordinated statewide training and continuing education for ALF and ADCC staff in Virginia, called the Virginia Statewide Training and Continuing Education Program (VSTCEP).
Description of the Training
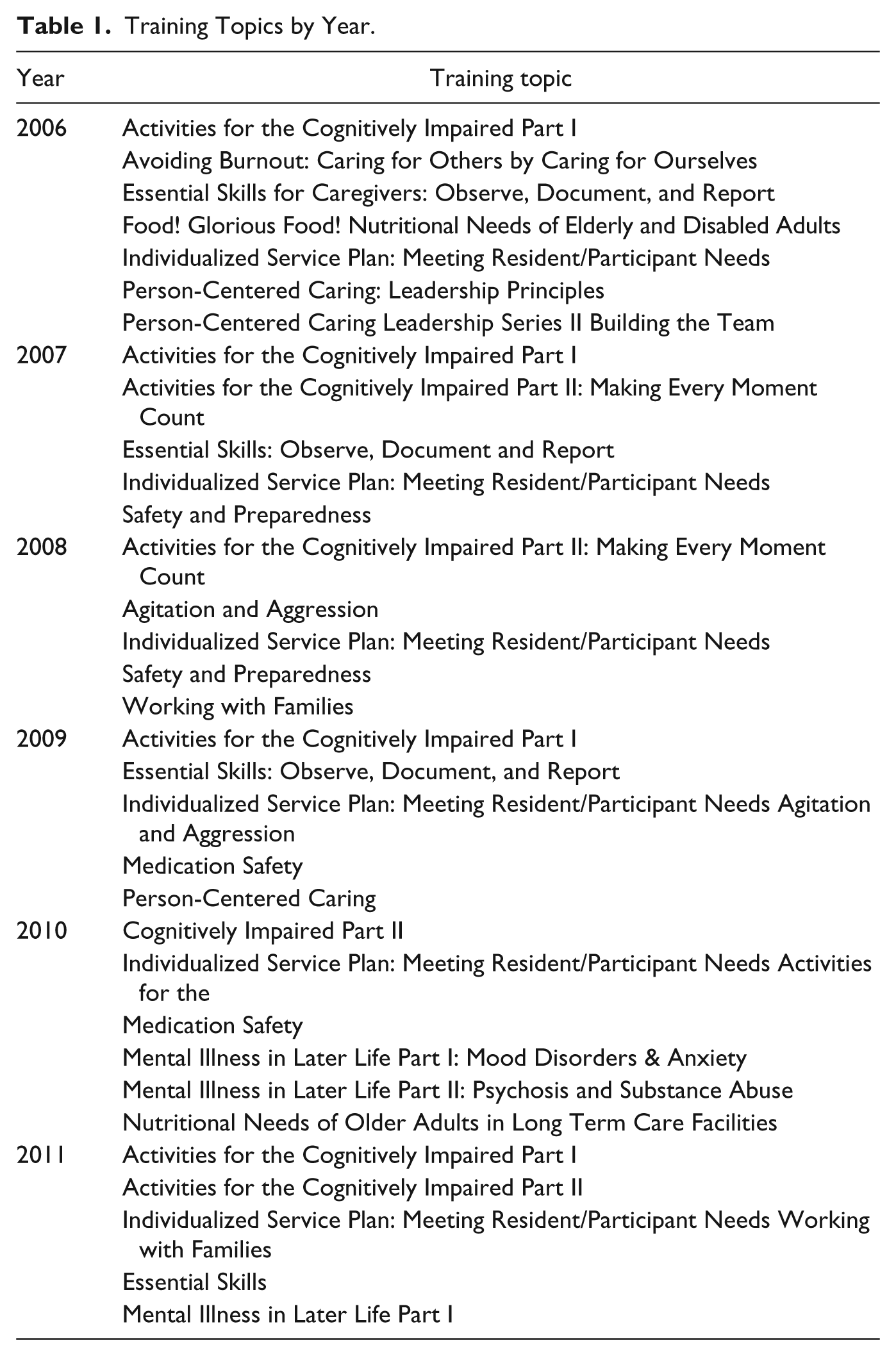
The Virginia Statewide Training and Continuing Education Program sessions include didactic instruction as well as group activities that require active participation by the attendees. Training session topics, course descriptions, and learning objectives are described in Tables 1 and 2. There is a nominal registration fee (US$15) to attend the 6-hr training session, and Continuing Education Units (CEUs) are provided for an additional fee upon request.
Training Topics by Year.
Sample Course Descriptions and Learning Objectives.
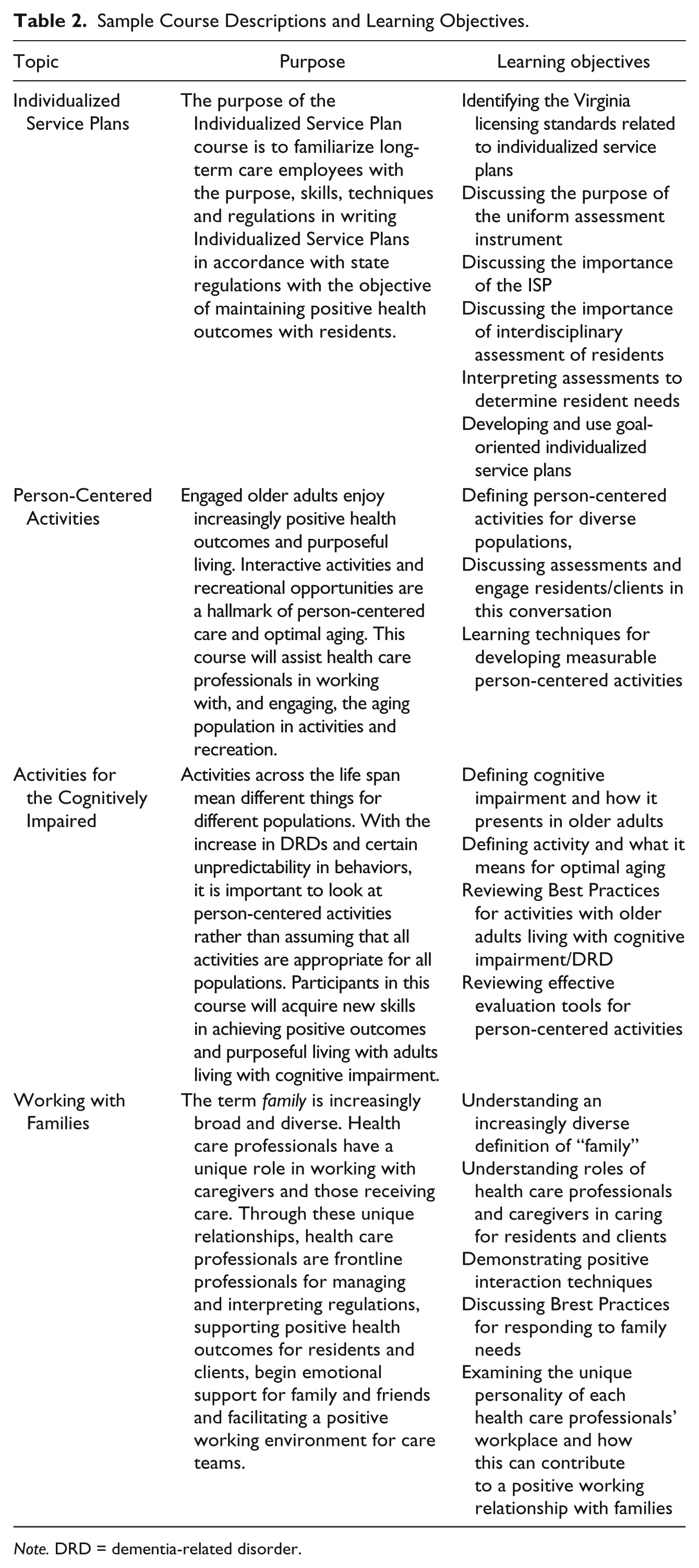
Note. DRD = dementia-related disorder.
Curricula for the VSTCEP program were designed by focusing on the training needs of ALF and ADCC staff based on a needs assessment conducted by the VDSS. Since the program’s inception, the curricula was broadened to accommodate an increasing number of administrators attending the training (driven by the new regulations requiring licensing with subsequent renewal and the requirement that continuing education should meet the specifications as mandated by the Virginia Board of Long-Term Care Administrators). As well, a substantial curriculum revision was used to promote a person-centered and positive aging framework that takes an 80/20 approach to aging (i.e., 80% of the aging population ages independently within community, and 20% requires assistive services). This 80/20 approach represented a purposeful shift in perspective to promote expansion of personal and professional views of optimal aging to educate participants on successful aging practices and combat the rampant ageism and gerontophobia that exist among those that work with older adults. This is important as research has demonstrated that fear of older adults and fear of our own aging affect job satisfaction and career commitment for people working with older adults (Gendron, Myers, Pelco, & Welleford, 2014).
In an effort to examine the efficacy of the Virginia Statewide Training and Continuing Education Program (VSTCEP), an evaluation was used that examined program survey data from 2006 to 2011. Following survey data analysis, a formative program evaluation was conducted to address program efficacy and consistency in program delivery. This article describes the challenges and lessons learned from conducting and analyzing the program evaluation of the Virginia Statewide Training and Continuing Education Program. Institutional review board (IRB) approval was obtained for this study (HM14342).
Program Evaluation Design
The program evaluation was conducted as a two-step process that included analyzing the survey data from 2006 to 2011, followed by a formative process evaluation as a standardized and systematic approach to assess program delivery. Between 2006 and 2011, the VSTCEP offered a total of 370 programs on 12 different topics. Upon completion of each training session, participants were asked to complete an evaluation form which included participant demographics, knowledge gained, program satisfaction, and recommendations for improvement.
The post-training survey questionnaire includes six items that capture knowledge gained as a result of attending the training session. These items include the following: (a) Did this program broaden your knowledge in this topic? (b) Did this improve your ability to identify and solve problems in your job? (c) Do you foresee that this program will have an effect on practices in your facility/practice area? (d) Did this program affect your view of your residents’/clients’ quality of life? (e) Did this program relate to your particular job responsibilities? and (f) Usefulness of the knowledge/skills acquired. Items were measured on a 5-point Likert-type scale (5 = exceptional, 4 = exceeds requirements, 3 = meets requirements, 2 = marginal, 1 = Unsatisfactory). In addition, a question was asked regarding the overall rating of the training session using the same 5-point Likert-type scale above.
After survey analysis, a process evaluation was conducted to determine whether the training was consistently being implemented appropriately, specifically assessing the degree of fidelity and variability in the programs across sites. The process evaluation was an important component of the evaluation process given that multiple program sites can increase the variability in content delivery (Oakley, Strange, Bonell, Allen, & Stephenson, 2006). The process evaluation was also used to assess the degree to which different instructors and training sites increased variability in delivery of program content. The process evaluation protocol utilized a rubric for observer ratings on topics including the degree to which each training topic was covered, the level of participant engagement, the instructional methods used, and participant and trainer interaction. Evaluators used systematic descriptive observation utilizing field notes on program surveillance. Systematic observation is used to conduct careful recoding of ongoing and co-occurring behaviors during the training sessions (Blatchford, Bassett, & Brown, 2005). Evaluators also provided their recommendations and conclusions at the end of each session.
Challenges to the Evaluation Process
There were several notable challenges to the program evaluation process regarding analysis of the post-training survey data. First, it is likely that some participants attended more than one training session during the study time frame, but the evaluation forms did not have identifiers; therefore, it was not possible to track participant attendance over time. Due to staffing changes and changes in program oversight, the evaluation forms changed during the 6-year study period; therefore, information regarding education and type of job had to be evaluated in a way that would satisfy the different versions of the forms. The education variable provided selections on the older forms that included level of nursing rather than level of highest educational degree received. Therefore, for clarity and consistency, we categorized highest level of education into medical credentials (i.e., CNA, licensed practical nurse [LPN], registered nurse [RN], and doctorate of medicine [MD]) and other credentials (i.e., high school diploma, associate’s degree, bachelor’s degree, master’s degree, and doctoral degree). It was noted that job type and highest level of education were duplicate responses for those with medical credentials. For example, CNAs reported that their highest level of education was completing a CNA course as opposed to having a high school diploma. Therefore, we found it necessary to examine job type to look deeper into potential differences for those with other non-medical credentials, such as administrators.
Another limitation of the survey form was that work-related variables such as length of time working in the field, length of time working in current position, and training received in other states or other jobs were not collected. Additional work-related information should be addressed in follow-up studies.
The Participants
Participants included ALF and ADCC staff (n = 7,230) working in VDSS-licensed facilities in Virginia. However, since identifiers were not collected, it is likely that the same participants attended two or more training sessions over the 6-year period. Therefore, the total N does not represent unique data points. Participants were 18 to 79 years old (M = 44.87, SD = 12.37), and 92.2% were female. The sample was diverse by race/ethnicity, highest level of education completed, and occupation (Table 3). The demographics collected from each participant included the city or county of employment, age, gender, race/ethnicity, and highest level of education completed. Thirty-four percent (n = 2,278) worked in Central Virginia, 24% (n = 1,598) worked in Eastern Virginia, 31% (n = 2,063) in Northern Virginia, and 11% (n = 730) in Western Virginia. Viewed another way, 58% of participants worked in urban areas, 21% worked in rural areas, and 21% worked in mixed areas with both rural and urban localities.
Demographic Characteristics of Participants (N = 7,230).

Note. CNA = certified nursing assistant; LPN = licensed practical nurse; RN = registered nurse; MD = doctorate of medicine.
Results
Survey Data
Preliminary analyses included descriptive statistics and Pearson’s product–moment correlation coefficients. Correlation coefficients indicated that the six outcome items regarding knowledge gained were moderately to highly correlated (α = .65-.82). Descriptive data for post-training survey items are presented in Tables 4 and 5. ANOVA indicated significant differences based on those with medical credentials for all items measuring skills and knowledge gained including broadening knowledge on the topic, F(3, 2457) = 14.10, p < .001; improving ability to problem solve, F(3, 2463) = 15.73, p < .001; perceiving an effect on job practice, F(3, 2460) = 9.35, p < .001; having an effect on residents’ quality of life, F(3, 2457) = 17.87, p < .001; relating to job responsibilities, F(3, 2452) = 8.22, p < .001; and usefulness of the knowledge/skills acquired, F(3, 2343) = 6.55, p < .001. Tukey’s honest significant difference (HSD) demonstrated a consistent trend, with all but one item highest for CNAs. ANOVA also indicated a significant difference for the overall evaluation of the training session, F(3, 2337) = 9.59, p < .001, with MDs and CNAs reporting the most satisfaction with the training.
Mean Scores for Knowledge Gained Items and Overall Evaluation of the Training for Medical and Non-Medical Credentials.

Note. Higher scores indicate greater knowledge gained using a 5-point Likert scale CNA = certified nursing assistant; LPN = licensed practical nurse; RN = registered nurse; MD = doctorate of medicine.
Mean Scores for Knowledge Gained Items and Overall Evaluation of the Training for Job Type Among Those With Other (Non-Medical) Credentials.

Note. Higher scores indicate greater knowledge gained using a 5-point Likert scale.
ANOVA indicated significant differences for those with other (non-medical) credentials for all knowledge gained items including broadening knowledge on the topic, F(4, 4208) = 30.56, p < .001; improving ability to problem solve, F(4, 4208) = 36.57, p < .001; perceiving an effect on job practice, F(4, 4204) = 20.39, p < .001; having an effect on residents’ quality of life, F(4, 4196) = 35.80, p < .001; relating to job responsibilities, F(4, 4194) = 15.15, p < .001; and usefulness of the knowledge/skills acquired, F(4, 4127) = 11.52, p < .001. Tukey’s HSD demonstrated a consistent trend, with all items significantly lower for bachelor’s and master’s level than all others. ANOVA also indicated a significant difference for the overall evaluation of the training session, F(4, 4122) = 11.18, p < .001, with bachelor’s level reporting the least satisfaction with the training.
ANOVA was also performed for the subset of participants with non-medical degrees that reported type of job. ANOVA analysis demonstrated significant differences based on type of job for those with other non-medical credentials for all knowledge gained items including broadening knowledge on the topic, F(5, 950) = 5.54, p < .001; improving ability to problem solve, F(5, 949) = 7.83, p < .001; perceiving an effect on job practice, F(5, 946) = 7.86, p < .001; having an effect on residents’ quality of life, F(5, 943) = 6.14, p < .001; relating to job responsibilities, F(5, 945) = 3.78, p < .001; and usefulness of the knowledge/skills acquired, F(5, 935) = 8.34, p < .001. Tukey’s HSD demonstrated a consistent trend, with all items significantly highest for administrators. ANOVA also indicated a significant difference for the overall evaluation of the training session, F(5, 930) = 6.52, p < .001, with administrators reporting the most satisfaction with the training.
Process Evaluation
Results of the process evaluation indicated that topic items were completely covered 80% of the time and partially covered 20% of the time. All of the evaluators reported a mixed method of instruction including teaching aides (e.g., pictures, films, slides) and participatory discussion and activity. Observer evaluation of participant engagement reported that participants were highly engaged 75% of the time and somewhat engaged 25% of the time. Observer evaluations indicated that two thirds (66%) of training participants were actively participating without prompts and that all participants engaged in program activities.
Instructional methods and quality of training was also evaluated during the formative evaluation process. All of the training instructors met the criteria for arriving on time and being prepared for the day’s events, providing introductory background on their expertise, gaining attention of the group, outlining the objectives, emphasizing the key points, encouraging participation and small group activity among participants, and checking for understanding among the participants. Non-participant observations reports indicated that the instructors did not deliver the content clearly at 33% of the training sessions. In addition, non-participant observation reports indicated that during 7% of the training sessions instructors were unable to clearly and knowledgably answer questions, did not appear knowledgeable about the subject matter, and failed to present information at a moderate pace.
Lessons Learned
Evaluation results suggest that knowledge gained from participating in an individual training session was different within type of credential and type of job reported for those with other (non-medical) credentials. Participants with high school, associates degrees, and doctoral degrees in addition to those with a CNA medical credential or a medical doctorate reported greater knowledge gained from participating in training sessions than those with other degrees and credentials. In terms of job type, administrators had consistently higher scores than other reported job types among those with other (non-medical) credentials. This is important information given that the training content and learning material was initially designed for ALF and ADCC direct care staff (which typically consist of people with less formal education) who have more daily, face-to-face contact with older adults than administrators. Therefore, the curriculum was appropriately designed to meet the need of the primary audience. However, it was unclear whether administrators would gain value from a curriculum that was designed for a direct care workforce. Upon review, it is encouraging that administrators also rated knowledge gained highly and felt attending the training positively impacted what they do. In light of these findings, one potential implication for co-training administrators and other staff is that it provides a mechanism for administrators to better understand their employees in terms of job requirements, skill, and knowledge level.
The formative program evaluation through non-participant observation indicated inconsistencies among the training sessions. During the study period of 2006 to 2011, most trainers were hired based on their previous experience and an interview involving a short assessment of their training skills. In addition, there was no formal mechanism in place for trainers to receive an evaluation, feedback, or guidance regarding their performance. Based on the findings of the program evaluation, immediate steps at program improvement were taken including the following: (a) The program has now been restructured to allow for continuous feedback through the use of mandatory semi-annual orientation-style webinars; (b) ongoing observation and in-person evaluation of trainings and trainers; (c) establishing a policy and procedure manual for all trainers; (d) an end of year evaluation report with special recognition awards; (e) learning materials provided on the principles of adult learning theory (Woodard, 2007) prior to facilitating any programs and encouragement to utilize such principles as encouraging group participation and activities, reflection, meaningful questions and examples, and respecting group expertise; and (f) an online learning site for trainers to share techniques and ideas.
As well, changes were made to the hiring process including the following: (a) An employment application specific to the training program was developed to assess specific areas of expertise, (b) trainers are now required to shadow a veteran trainer to provide the opportunity for questions and clarification about logistics prior to beginning the job, and finally (c) creating a mentorship pipeline where veteran trainers are assigned to mentor current and future trainers.
Analysis of the program evaluation also highlighted the lack of participation by state licensing inspectors in the training program. On several occasions, non-participant observers noted in their field notes that participants expressed a desire to have inspectors present at the trainings. It was noted that participants made comments regarding the variability among licensing inspectors regarding interpretation and application of regulations during inspection visits. Because the state does not require the licensing inspectors to receive training and continuing education on an ongoing basis, the VDSS encourages its licensing inspectors to attend training and continuing education programs. Therefore, while some inspectors do regularly attend trainings, they do so of their own accord. Therefore, evaluation results uncovered a training gap within the local VDSS licensing offices. A policy addressing a standard and consistent format which drives the hiring and training processes of licensing inspectors across the state is needed. New policy should consider a requirement for licensing inspectors to complete standardized ongoing training and continuing education. This policy shift would promote a more consistent licensing inspection workforce with the benefit of improved partnerships with the ALF and ADCC staff serving Virginia’s older adults and ultimately improved eldercare.
Summary
An evaluation of 6 years of survey data in addition to a formal process evaluation highlighted both successes and areas for improvement. Most notably, results indicated that the targeted curriculum was successful in reaching its intended audience. In addition, it was very encouraging that administrators also consistently provided high ratings for the training. Needs theory, established by Maslow (1943) and supported by McClelland (1978), contend that to maximize learning, content should relate to fulfilling specific needs; despite the fact that administrators might not directly utilize the skills taught in the training program, their high ratings imply that they found value in attending the training. Given Maslow (1943) and McClelland’s (1978) perspective, specific training needs of administrators should continue to be explored that expand upon management or operation procedures and include opportunities to better understand the daily work being performed by their staff. As well, research is needed to determine whether the staff members benefit from a co-training environment that provides exposure to the daily workload of administrators.
Although previous research has demonstrated that continuing education programs show overall benefits for participants, much of it suggests an impact of training based on the difference in level of formal education (Robben et al., 2012; Slater, Lawton, Armitage, Bibby, & Wright, 2012). This evaluation demonstrated that type of job, in addition to level of education, was important in how the program was perceived by the participants. Pursuant of the goal to improve the quality of care provided to older adults, this finding has significant implications for the continuation, expansion, and improvement of continuing education efforts, particularly as it relates to targeting trainings to diverse staff needs and roles.
Evaluation findings highlighted the need for program improvement and expansion opportunities at the program level (e.g., updated train-the-trainer materials, orientation for trainers, and new protocol for hiring trainers), which were immediately addressed and incorporated into program implementation processes on an annual or even training by training basis. Other recommended program improvements are far beyond the scope of the program and must be addressed at a higher statewide policy level. The scope of these findings further indicates the necessity for statewide partnerships across agencies to promote standardization and broad-based collaboration. The evaluation uncovered a disconnect between the continuing education of licensed inspectors across the state and ALF and ADCC facility staff. Standardized training and continuing education requirements for licensed inspectors should be considered to improve the inspection process and improve the working relationships between inspectors and ALF and ADCC facilities and staff. Further research is needed to determine the short- and long-term benefits of training licensing inspectors and whether their training affects the quality of life of their older adult clients. In addition, further examination is needed to determine whether administrators would benefit from targeted training and continuing education that directly provides relevance to their job responsibilities and whether staff members benefit from co-training with administrators. Future research can also address whether targeted training for ALF and ADCC staff improves long-term training impact, job satisfaction, and career commitment.
This study has provided additional evidence to help explain the need for training and continuing education among the direct care and administrative workforce in ALF and ADCC. One of the challenges that many of these providers may face is financing these opportunities for staff. Virginia’s example of a successful statewide continuing education program is built upon a relationship between the VDSS, the licensing body for ALF and ADCC in Virginia, and the Department of Gerontology at Virginia Commonwealth University. The monies that support this program come from provider fees and penalties assessed by the VDSS and are awarded to the Department of Gerontology as grant money to fund training and continuing education opportunities for the ALF and ADCC providers. This allows for a significant decrease in cost for staff to attend these statewide training sessions. This is one example of a model that helps to ease the financial burden of providing high-quality training to staff members outside of the ALF and ADCC setting. A similar statewide information resource program highlighted best practices for funding models to include revenue coming from memberships or fees for services, grants, and state funds (Aspinall, Chew, Watson, & Parker, 2009). Additional funding and models to promote culture change should be explored that place a stronger emphasis on the necessity of quality training and education for ALF and ADCC staff.
Footnotes
Acknowledgements
The authors would like to thank Annette Kelley at the Virginia Department of Social Services, Division of Licensing Programs, for her assistance in the planning and delivery of this continuing education program.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This continued program and research are supported by a grant from the Virginia Department of Social Services, Division of Licensing Programs.