
Abstract
Introduction
The patient-centered medical home (PCMH) is a multi-dimensional model for delivering primary care services that has received widespread adoption in the United States. The model consists of several guiding principles: (a) physician-centric care delivery, (b) holistic care orientation toward patients, (c) enhanced patient access to services, (c) improved quality and safety of care, and (d) better coordinated care across the various parts of the health care system (American Academy of Family Physicians, 2016). The National Committee for Quality Assurance (NCQA) has created a checklist of approximately 30 operational elements that individual primary care practices must consider implementing to be accredited as a PCMH (NCQA; 2015). Among other things, these elements include providing after-hours access to patients, practicing team-based care, providing self-care support and access to community resources, and tracking patient referrals, tests, and care transitions. Generally, the PCMH model is meant to provide a more patient-centric care experience.
Thus far, the PCMH model has met with mixed success (Friedberg, Schneider, Rosenthal, Volpp, & Werner, 2014; Hoff, Weller, & DePuccio, 2012; Jackson et al., 2013). It has been shown to improve various aspects of health care quality, particularly related to chronic disease management, while also lowering both hospital and emergency department utilization (Hoff et al., 2012; Jackson et al., 2013; Reid et al., 2009). But some of its quality enhancement potential has not yet been shown and, in some cases, the implementation of PCMH models of care can lead to increased health care costs, for example, around primary care service delivery (Jackson, 2013; Reid et al., 2009).
Physicians also remain mixed in their support for the medical home concept, with meaningful percentages of both primary care and specialist doctors believing less that the model will be transformative in its effects on health care quality and costs (Merritt Hawkins, 2012). Finally, we are still not fully sure how patient experience is affected by being cared for in a medical home environment (Hoff et al., 2012; Reddy, Canamucio, & Werner, 2015). Despite continued debate, primary care practices nationally have moved quickly to becoming full-fledged medical homes, as defined by the NCQA (2015) standards. In addition, the Affordable Care Act has provided incentives for the field of primary care to pursue PCMH-type change.
An important gap remaining in this literature is the need to better understand whether the model can be fully realized for different types of patient populations, particularly older adults, who are the biggest users of primary care services. There is little available information in the PCMH research literature around PCMH implementation for this specific subpopulation. Addressing this gap may help inform our understanding of why the PCMH model could underperform in certain situations, which it has been shown to do. Specifically, how directly applicable the standard PCMH model, as articulated through the NCQA PCMH standards, is for seniors looms an important question (Hoff, 2012; Reuben, 2009). One prior study showed that seniors’ experiences with their care improved in medical home care settings, but quality of care improvements were no better than in non-medical home environments (Fishman et al., 2012).
Seniors have a particular interest in seeing primary care practices adopt medical home care effectively. For example, seniors have unique needs, disease profiles, expectations, and preferences when it comes to receiving primary care services (Hoff, 2012; Reuben, 2009). They are a generally sicker population, possessing more complex care needs because of higher rates of chronic disease and the presence of comorbidities at a higher intensity than the general population (Freedman, Martin, & Schoeni, 2002; National Center for Health Statistics, 2014). Seniors visit their doctor more often, have more complex care coordination needs, and see specialists with greater frequency (Centers for Disease Control and Prevention, 2015). They also have greater visual, physical, and cognitive impairments that can make accessing care challenging and require them to rely upon a diverse array of services and supports to receive timely, ongoing attention to their medical care needs (Freedman et al., 2002). Finally, they may have other non-clinical needs and requirements in areas such as transportation and social support that require addressing. In theory, PCMH care can respond to many of these particular realities.
Seniors also have some unique expectations and preferences that affect primary care service delivery and medical home approaches, in particular. For example, there may be greater resistance to or ambivalence about using technology for some older adults and a greater preference for face-to-face care delivery, particular among cohorts above the age of 70 (Choi, 2011; Safran, 2003; Sarkar et al. 2011). In addition, the reimbursement structure surrounding primary care service delivery to seniors, given heavy reliance on Medicare and its still-largely episodic payment philosophy, may present challenges to medical practices interested in providing ongoing, multi-faceted care to their seniors. Despite a new monthly care coordination payment made available to primary care physicians to proactively manage care for their sickest senior patients, most care to seniors is still reimbursed through patients coming into the office to receive care (Pear, 2014).
Given these realities, it might be expected that not everything in the PCMH model can be implemented equally well for this particular patient population. But which elements of the PCMH model are more difficult to implement for seniors, and why? And how do primary care physicians and their staff try to learn from, overcome, work around, or avoid altogether those aspects of PCMH care they find difficult to implement for their senior patients? These are questions that remain unexplored within the literature. They are important because they speak to (a) the overall applicability and potential of PCMH care elements for seniors, (b) how PCMH care may need to be modified to account for unique care situations and services such as those some seniors require, and (c) what other reimbursement, services, and supports may need to complement PCMH care to fully account for improving the quality of health care delivery for seniors.
The present study addresses these questions and discusses the implications of the results for these issues. It uses ideas from sensemaking theory in the field of psychology (Brown, Colville, & Pye, 2015; Weick, 1995). These ideas seek to explain how physicians and their staff make sense of and respond behaviorally to aspects of PCMH implementation that their prior experiences tell them are challenging to perform for their older patients, for reasons that they may feel that they can or cannot control. Sensemaking generally involves individuals cognitively processing the lived experience, and then using that learning as a subsequent means of deciding future behavior. In this way, sensemaking is about contextual rationality, that is, how individuals deal with discrepant cues or signals that interrupt their ongoing activities and require them to come up with interpretations that are both plausible and justify, at least to themselves, how they choose to respond (Weick, 1995).
Data and Method
The specific research setting for the study are six primary care medical organizations located in Upstate New York. At the time of data collection, the medical practices had or were about to achieve “Level 3” NCQA PCMH certification, the highest medical home standard possible. The practices were located across a mix of geographic areas, and included one general internal medicine practice and five family practices. They are typical of other primary care practices in the sense that they are of average size (e.g., 2-10 providers), located in appropriate areas where primary care is delivered, maintain the same PCMH accreditation as others, and serve a variety of low, middle, and higher income seniors. These practices were selected purposively on the basis of gaining a variety of locations, sizes, and organizations that were far enough along on the medical home transformation journey.
Two of the six practices were located in poorer, inner-city geographic locations, and treated a higher percentage of patients above the age of 65 and possessing multiple chronic diseases. Thus, these two practices differed in a key sense from the other four in the extent to which they needed to implement PCMH care particularly for older adults. All six practices had functional electronic medical record systems which were used for tasks involving direct patient care, care coordination, scheduling, and care management. These tasks included recording and tracking lab tests and referrals, medication management, preparing clinical visit summaries, and documenting various performance metrics for the management of chronic diseases such as diabetes. All six practices were in some phase of implementing electronic portals for patient use, although none of the six reported that their portals were being used yet in any meaningful way by patients. None of the six practices used any type of telehealth innovations in performing patient care. Each of the six practices also belonged to a larger administrative organization, which helped them to manage financial risk, negotiate insurance contracts, and manage quality reporting. Four practices belonged to one such organization, and two others belonged to a different one. All six practices still functioned largely independent of influence from the umbrella organization, which served more to connect practices into a loose affiliation with one another. The study was approved by the first author’s institutional review board (IRB# 12-11-27).
Qualitative data were collected through in-depth, semi-structured interviews with 51 staff working in six different, NCQA-accredited PCMH primary care practices (Table 1). Interviews were used given the desire to explore physician and staff views and perceptions and gain description on their experiences implementing certain aspects of medical home care for seniors. The percentage of total providers interviewed within each of the six practices ranged from 46% to 100%, yielding good coverage of most of the clinical expertise within each practice. Non-physician staff were also interviewed, as effective medical home implementation requires a collaborative team approach among primary care workers. Each interview lasted on average between 45 and 60 min. Interviews were conducted in person, with a few done by phone.
Interview Sample (n = 51) and Dimensions Associated With the 6 PCMH Organizations.
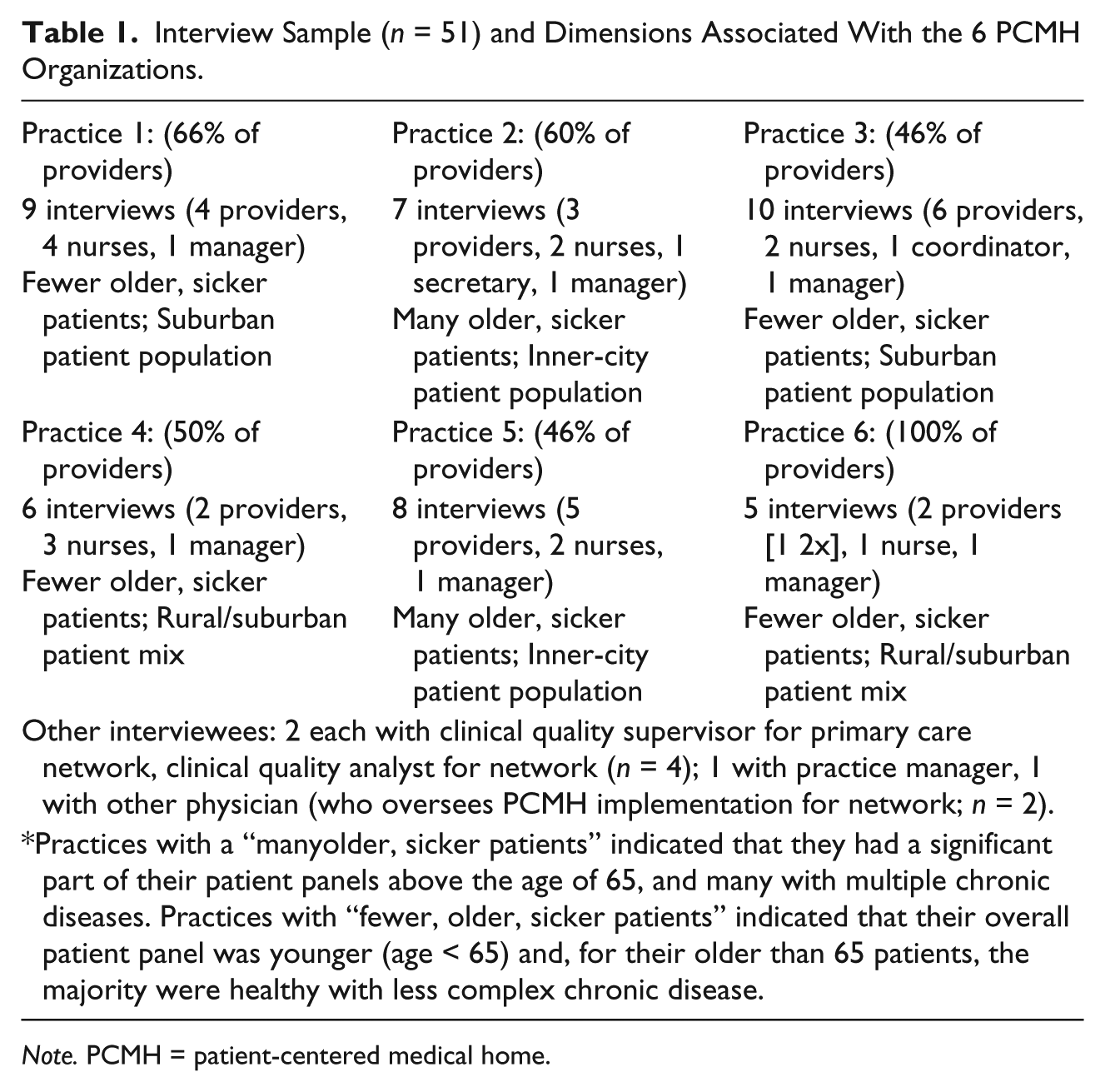
Note. PCMH = patient-centered medical home.
The interviews were guided by a semi-structured protocol that asked physicians and their staff about various aspects of medical home care (e.g., care coordination and management, medication management, providing enhanced patient access to the practice) and how these aspects in particular were being implemented for seniors, focusing on the everyday activities in which staff engaged. Data acquisition involved gaining rich description from interviewees about the opportunities and challenges related to particular PCMH aspects for seniors, using stories and experiences from individuals, and then trying to identify the implicit logics and responses the individuals and organizations used to make sense of a given implementation challenge they encountered. This approach is particularly effective when less is known about a phenomenon, and when there is a need to have those immersed in the everyday organizational setting provide insight that otherwise would be difficult to obtain (Strauss, 1987). Data were digitally recorded, transcribed verbatim into Word documents, and then analyzed by the two co-authors using Atlas.ti version 7 qualitative analysis software.
Generally accepted methods of qualitative analysis were adhered to in the study, including theoretical sampling, validation of codes by multiple researchers, and multi-level coding approaches (Miles & Huberman, 2014). Theoretical sampling was employed in an iterative manner, as the 51 interviews underwent preliminary analysis in batches of 10 at a time. This process involved exploring each batch of 10 interviews, identifying major themes and patterns that informed the research questions through open coding, and then modifying the interview protocol slightly to explore in greater depth, using subsequent interviews, those patterns that were emerging as dominant across the data set. This process defined the particular theoretical sampling approach taken in the study. In this way, key PCMH implementation gaps for seniors were identified at an earlier stage and then physicians and staff were asked more about them, both to validate their presence across the six medical organizations and also to examine how individuals made sense of and responded to the gaps.
A two-stage coding process was performed on the data throughout the 51 interviews. Both co-authors participated in each stage of coding, with the first co-author assuming responsibility for conducting coding on the entire data set, and the second co-author involved with the first 20 interviews (e.g., first two batches as described above). After the first 10 interviews had been coded jointly around the identification of both the PCMH implementation gaps and staff sensemaking around those gaps, the co-authors met to discuss any discrepancies or areas of uncertainty, refined their coding, and then jointly coded the next batch of 10 interviews. At that point, there was consensus regarding the gaps that had emerged and the sensemaking in relation to the gaps. These first 20 interviews involved staff working in the six different practices. The first co-author then analyzed the remaining interviews to ensure the gaps and sensemaking identified during the first 20 interviews remained consistent. Several additional insights related to these gaps and sensemaking emerged during analysis of the latter interviews, and these insights were discussed among the co-authors and, where necessary, factored back into the interpretive schemes being developed.
First-order coding revealed several key implementation gaps that staff believed existed from everyday experiences with PCMH care and their seniors. Second-order coding involved identifying deeper patterns in the data related to the individual understandings and behavioral responses occurring in response to the implementation gaps found in the first-order coding exercise. These deeper patterns touched upon the ways in which physicians and their staff were interpreting various challenges for seniors; whether or not a given challenge was the result of something the practice was doing wrong; or whether it was caused more by an external stakeholder. They also spoke to how these interpretations shaped their own actions with respect to the implementation gap (i.e., the “sensemaking” occurring and its impact on behavior).
Results
Overall, physicians and staff across the six primary care practices believed that seniors on average were more unique than younger patients in terms of needs, required more investigation and time, and were more challenging generally with respect to caring for them within a medical home model that stressed holistic patient care, timely access, and prevention. Regardless of the staff interviewed, these were consistent themes that came out as individuals were asked to comment initially on how the medical home model could be applied to seniors. Reasons given for this singling out of seniors as a challenging group for PCMH care varied, and included rationales rooted in the more isolated nature of seniors still living in their homes to a more complex disease burden than other patients, as well as the greater tendency for many seniors to “spread out” across the health care system, seeing more specialists especially, making medical home goals of enhanced care coordination and care management more difficult.
We do have a lot of elderly patients that live independently that shouldn’t, so you know who they are. You take more time with them and you take more time and get them squared away. (Secretary, Practice 2) A lot of older folks, they’re in isolation, a good handful of them have significant chronic diseases like diabetes, hypertension, they are overweight or obese, some are on their way to renal failure, cardiovascular disease, maybe they have angina, anything like that, or stroke. They’ve got all of these chronic things, and they’re seeing lots of different people in the system. (Physician, Practice 1) Take the visit aspect of it. You know, you can’t see a 65-year-old hypertension follow up in 15 minutes and then see another 74-year-old patient with COPD and then another, you know, 84-year-old patient with a six-month follow up for diabetes—all in 15 minute increments without falling behind because they have comorbidities and it’s unrealistic for older patients to have them come in for one thing. (Physician, Practice 2)
Implementation Gaps Around Medical Home Care Delivery for Seniors
While the general principles of medical home care were acknowledged as challenging to apply fully to seniors, the first-order analysis performed identified three major PCMH implementation gaps specific to seniors that were common to all six primary care practices. These gaps were identified and discussed by all staff more than any others in the interview sample. Representative quotes illuminating these gaps are included in Table 2. They included (a) performing in-depth clinical assessments on seniors, (b) identifying seniors’ life needs and linking older patients with community resources, and (c) care management and coordination, in particular self-management support for seniors. Clinical condition assessment was perceived as an important medical home element that, for many seniors, helped medical practices to identify emerging conditions or health issues including dementia, sudden changes in existing disease status, or other functional impairments.
Representative Quotes Illuminating PCMH Implementation Gaps.

Note. PCMH = patient-centered medical home.
However, primary care physicians and their staff felt that in-depth, formal assessments were difficult to perform on more than an ad hoc basis for their seniors. The need for them could be unpredictable and went according to sudden changes in patient status and did not often align neatly with the periodic exams allowed by payers such as Medicare. In fact, most physicians believed that the need for in-depth assessment existed for many older patients any time they were presenting in the office, and also during random moments in between the 3- and 6-month check-ups that were the norm (Table 2).
Identifying seniors’ life needs and linking them to community resources was defined as the medical practice’s ability to learn about, record, and take action related to non-clinical issues such as transportation difficulties, access to good food, home safety, and social/family support. To primary care personnel, the “taking action” part involved knowing and connecting their older adult patients with other appropriate community-based organizations (e.g., Visiting Nurse Association, Meals on Wheels) in their “medical neighborhood” (Fisher, 2008). Staff believed that seniors possessed a diverse array of non-clinical needs including transportation and family support, and that meeting these needs was critical in assuring high-quality care provision.
For instance, respondents mentioned situations where seniors had difficulty understanding or following directions, needed extra help to meet the directives of a clinical order, or had insufficient social supports to help them navigate the health system or access needed care. They believed that their own role in identifying and meeting these needs was limited, and that seniors’ families also sometimes proved problematic in this regard. They also believed that the community supports available varied across geographic locations and were often difficult to work with in getting assistance. Many staff expressed feeling disconnected from the larger support system in the local community.
The third PCMH implementation gap was broadly defined as care management and coordination, with a special emphasis placed on patient self-management. Physicians and staff in all six practices expressed challenges in attempting to manage many seniors’ care as the latter moved through different health care settings such as hospitals and specialist offices. Some of this was focused on the difficulty in overseeing major care transitions for seniors from hospitals to nursing homes or rehabilitation facilities. In particular, interviewees felt that it was their ability to help their older adult patients self-manage their care that was negatively affected by several factors external to their practice. This self-management included simpler things, such as an older patient being able to manage their medications, and collect and transmit basic biometric information to the practice (e.g., blood pressure), to the more complex, such as identifying and correcting safety issues in their homes, and self-assessing at a basic level for impairments such as memory loss.
Making Sense of and Responding to the PCMH Implementation Gaps
Each of the six medical practices, as well as staff within the practices, expressed similar behavioral responses to the implementation gaps identified. These responses were shaped by how primary care physicians and their staff made sense of the implementation gaps (see Table 3). It was clear that the individual-level understandings involved in articulating two of the three gaps, that is, clinical condition assessment and understanding/addressing seniors’ life needs focused outwardly on structural problems such as misaligned Medicare reimbursement policies, the relative isolation of primary care practices from other community organizations, and coordination problems with specialists that were less of their own doing. As mentioned, there was also a strong perception that seniors were more unique than other types of patients in terms of needs and required a wider array of personalized approaches, which interviewees felt was neither necessarily always within their purview of responsibility nor something they had the time or compensation to do (see Table 3).
PCMH Implementation Gaps Identified and Staff Sensemaking Around and Responses to Gaps.

Note. PCMH = patient-centered medical home.
These reasons deflected the problems outward, away from each organization’s control, making them easier to ignore. For example, individuals were convinced that being less able to perform (and get paid for) in-depth assessments in real-time for seniors, and often, when they were actually needed, was beyond their ability to fix, the specific result of (a) Medicare payment approaches still built largely around episodic, reactive care delivery that discouraged direct contact with seniors except at sporadic intervals; (b) a portion of seniors having fast-changing conditions that made it impossible to plan rationally for their care; and (c) an inability to get timely information from specialists. This set of beliefs on their part seemed to foster a collective feeling within each medical practice that performing this aspect of medical home care would need to fall upon someone else within the system, that is, that it was not truly within their particular purview.
Thus, at the same time, they blamed payers and specialists for undermining their own organization’s inability to remain current on the senior patient’s condition and they also implied it was up to others to address this problem. Some of this lack of empowerment also appeared to stem from a perception that, in the case of identifying and addressing a broader range of seniors’ life needs, anything involving “non-clinical” work was less in their domain of responsibility. Through this conveyed logic, it could be easier for each organization to splice off larger chunks of the kinds of “holistic care” PCMH approaches promoted, making their roles as medical homes less comprehensive for seniors.
For only one of the three major PCMH implementation gaps was there a significant sense of empowerment among physicians and their staff that the gap could be proactively addressed by their own actions. This was in the area of care management, particularly involving care transitions for seniors (e.g., moving from a hospital stay to nursing home), where individuals believed that there were specific system incentives made available through the PCMH funding model which could be used strategically to do things like fund additional staff that could work on patient outreach and develop tailored information systems to track patient information (Table 3). The greater action orientation in the six medical practices toward this brand of care management, compared with the other two gaps, appeared largely the result of individual understandings about this medical home component that saw external stakeholders, such as private insurance plans and Medicare, as willing to support their activities in this area, and whose interests were in key ways aligned with their own because of quality metrics that emphasized cost control and lower utilization of hospital and specialty services.
As a result, staff talked more proactively about their efforts to try and ameliorate this gap, although they acknowledged the gap was one they alone could not overcome completely. These efforts involved creating new practice workflows and protocols to take advantage of the financial incentives and resources (e.g., care coordinators, better electronic record systems) offered by insurers and the larger practice network to which they belonged and which sought to achieve goals pertinent to multiple stakeholder interests, such as reducing unnecessary hospital and emergency department utilization and improving quality in high-cost areas such as diabetes care. When discussing how they tried to respond to the care transition gap, for instance, individuals felt that it was a fairer environment for them in which to take action, as this action was supported by outside interests. In this way, their action responses to making PCMH care management work for seniors did not stem from any moral inclination to do whatever it took, but rather from a pragmatic appreciation for how to garner the extra financial and human capital resources that others would make available to them in return for doing certain things.
Discussion
The findings presented add to the existing PCMH implementation literature. That existing literature has two major foci at present: (a) the structural factors (e.g., information technology infrastructure, team-based care) that predict PCMH implementation success (Aldina, Schneider, Singer, & Rosenthal, 2014; Gale et al., 2015) and (b) linking various degrees of effective PCMH implementation within medical practices to outcomes such as quality of care and cost containment (Alexander et al., 2015; Nelson et al., 2014). To our knowledge, the present study is one of the first to explore how primary care physicians and their staff experience PCMH implementation for an important patient population, that is, seniors, and how that experience feeds into sensemaking that shapes their subsequent psychological and behavioral responses to future implementation practice. In this way, our study examines the important roles practice culture and individual cognition play in PCMH implementation success.
This focus is revealing in its insights. First, the results demonstrate that not all aspects of PCMH care may be equally implementable across different patient care populations, at least from the perspective of staff expected to perform the care. This may seem like an obvious point, but it is one largely missing from PCMH implementation research at the present time and strikes at the core of advocating for one, standardized PCMH definition. Certainly, for the senior population which has unique needs, a single definition may not fit well. There remains an implicit assumption, both in the NCQA (2015) standards for PCMH care and in how the medical home model is generally talked about in the health policy community, that primary care practices can learn how to perform (and will embrace) most, if not all, of the various PCMH activities once they (a) simply pay greater attention to the need to do them regularly and (b) are surrounded by the appropriate structural environment within which to do PCMH care.
The six practices here add an important nuance to this understanding, however, which is that in addition to both awareness and structural support (e.g., a working EMR system or team-based care), there are feelings of learned helplessness and, in other cases, empowerment among physicians and staff that must also be understood and managed to assure PCMH implementation success. These feelings are part of a sensemaking process that transfers the personal lessons learned from attempting difficult aspects of PCMH care delivery into a shared meaning system about those care aspects that becomes a future framework for action or inaction on the part of staff.
This framework for action is strategically derived, that is, there is an element of conscious choice by primary care workers as to which PCMH behaviors are worth doing and which are not. In this way, learning occurs from doing PCMH care, but it may be that some learning undermines, rather than promotes, future staff motivation to perform certain elements of PCMH care for senior patients in a vigorous way. A key implication of this observation for both policy making and research is that we need to consider more seriously the experiences and subsequent choices primary care workers make based on those experiences, when evaluating the feasibility of doing some variants of PCMH care for seniors. Research in this area would extend recent research examining PCMH implementation as a culturally driven process (Hoff, 2013; Stout & Weeg, 2014).
Relatedly, an implication for management and policy is that there must be deeper appreciation that simply providing “one size fits all” solutions such as more reimbursement dollars or infrastructure within a medical practice for PCMH care may not make the full difference if staff believe, from their own experiences, that other external factors beyond their control will undermine implementation efforts in select care areas or for patient populations such as seniors. This reality favors introducing more supportive facilitation into practices (see K. Coleman et al., 2014) to help physicians and staff examine their own learned assumptions around PCMH care carefully, process their ongoing implementation experiences in more mindful ways, and create action orientations toward future PCMH care delivery that embody greater proactiveness and risk-taking.
This study continues support for researching PCMH implementation as a contextually bound phenomenon, but places additional emphasis on how physicians and staff create their own meaning systems in relation to that context which then shape behavior. This makes the surrounding PCMH context more subjective than objective, that is, mediated through the lens of how workers make sense of various contextual features such as the level of direct contact with patients, the types of activities for which they get paid, their own roles within the overall system of care, and the characteristics of the patient populations for which they care. For complex patient populations such as seniors, the subjective context may be even more important to study as a predictor of PCMH implementation success than the mere presence of objective structural features such as information technology or additional reimbursement.
Finally, on a practical level, if there is an assumption that primary care practices NCQA-accredited as “patient-centered medical homes” are meeting the full range of seniors’ needs and expectations, but in reality they are not, important gaps in care for the senior population will remain unaddressed. Care fragmentation, lack of access to timely care, and lack of social and community support remain front-and-center issues for many seniors (Coleman, 2003). If becoming a medical home does not ameliorate these issues on a grander scale, as it has been advertised to do, then other policies, innovations, and approaches are warranted. Yet it is fair to ask how much this fact is realized or acted upon, given wide acceptance of the PCMH model.
It might be posited, based on these points, that for special populations like seniors, there needs to be a wider array of care innovations tried, and the results compared, to pick the most effective approach. For instance, if important activities such as the real-time assessment of seniors’ conditions, linking seniors with community-based resources and support, and identifying seniors’ unique life needs go under-addressed in the existing PCMH model, we should be seriously debating whether or not primary care practices should be expected to perform them and, if so, what can be introduced specifically into the primary care setting to convince physicians and their staff that they are worth doing on a regular basis.
The chief limitation of this study is that it is a small sample of practices and individuals, making it more difficult to generalize the results. That said, we believe the practices selected included an appropriate mix of types of seniors, were located in typical (for primary care) geographic areas, and, on average, were typically sized. Another meaningful limitation is the sole emphasis on individual perceptions and experiences to identify PCMH implementation gaps for seniors. Finally, linking the implementation gaps identified to outcomes such as seniors’ satisfaction with care or morbidity of some kind might lend even further import to the findings.
Future research could seek to validate these types of findings with other patient populations besides seniors, assuming there also may be other patient populations besides seniors upon which one or more of the standard array of PCMH care elements does not align very well with the everyday realities of service delivery (Schwenk, 2014). Expanding our investigations into the larger “medical neighborhood” and communities that surround primary care delivery for seniors would also enable us to better understand how different providers and organizations may complement one another in providing the full spectrum of medical home care (Bodenheimer & Pham, 2010; Fisher, 2008). As mentioned, the PCMH model at present makes few adjustments to account for the unique care realities of seniors, and in this regard, questions can be raised as to how the model falls short, and in what ways it can be improved, for that segment of the U.S. population that requires and benefits from primary care the most. It is also interesting to explore in the near future how the advancement of health information technology might help to alleviate one or more of these implementation gaps. As more primary care practices become comfortable using such technology, and as EMR systems get embedded in a larger number of everyday patient care activities, there may be ways to get providers and staff to become more proactive in several PCMH implementation areas in which they feel less empowered. This is an empirical question worthy of additional investigation.
In conclusion, this study demonstrates that seniors are a patient population which may not be fully benefiting from the PCMH care model at the present time, in part because of how primary care workers are choosing to implement certain aspects of that model. Primary care physicians and their staff believe from their everyday experiences that there are important implementation gaps in applying the PCMH model to seniors and, if the findings here are to be believed, they are acting strategically in embracing some PCMH activities while turning away from others. This reality may not fully show up on the standardized PCMH accreditation checklist used to validate an organization’s arrival as a medical home. But that does not preclude its existence. Instead, it may only be creating the false impression that for senior patients, being accredited as a “patient-centered medical home” is good enough.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Agency for Healthcare Research and Quality, Grant 5R03HS02093102.