
Abstract
The purpose of this research was to explore primary care providers’ willingness and ability to increase HIV prevention efforts among older adults and to gain recommendations for improving HIV prevention in primary care settings. Data were collected through 24 semistructured interviews with primary care providers. The results of the study reveal that the majority of providers find it necessary to increase HIV prevention efforts in primary care settings and are willing to do so; however, they cannot do so without assistance. Providers suggested strategies to increase HIV prevention in primary care, for instance, expanding the use of electronic reminders to include HIV prevention and increasing collaboration among providers of different specialties. As a result of the interviews, additional recommendations for increasing HIV prevention have been identified. These findings will aid in improving the quality of care provided to individuals older than 50 in primary care settings.
Introduction
According to the Centers for Disease Control and Prevention (CDC), there is an increasing number of older adults diagnosed with HIV, living with the disease, and dying from AIDS (CDC, 2015). Currently, approximately 50% of those living with HIV in the United States are older than 50 (Karpiak, Greene, & Havlik, 2015). However, by 2020, that number may rise to 70% (Karpiak et al., 2015). The emergence of highly active antiretroviral therapy (HAART) is a major driver of this increase, but at the same time, the number of new HIV cases among this age group is increasing. According to the Administration for Community Living (2015), some 17% of new cases of HIV are among older people.
Many older adults are sexually active, including those living with HIV. According to Lindau et al. (2007), 73% of individuals 57 to 64, 53% of individuals 65 to 74, and 26% of individuals 75 to 85 are sexually active. Older adults have the same HIV risk factors as younger people, including a lack of knowledge about HIV and how to prevent transmission, as well as possibly having multiple partners (CDC, 2015). Furthermore, risk factors for HIV in the older adult population include normal sexual changes associated with aging (e.g., decreased vaginal lubrication), psychological changes (e.g., loss of spouse), and risky sexual behavior (e.g., infrequent condom use) (Johnson, 2013). The National Survey of Sexual Health and Behavior conducted by the Center for Sexual Health Promotion found that only 5.1% of men and 7.4% of women older than 61 used a condom during their last 10 vaginal intercourse acts (Herbenick et al., 2010).
Approximately 18 million men in the United States suffer from erectile dysfunction (ED) (Selvin, Burnett, & Platz, 2007). Researchers have found that one third of men aged 50 to 64 suffer from ED and that figure increases to about 44% for those 65 to 85 (AARP, 2011). The increased availability of medications used to treat ED may facilitate sex for older men who otherwise would not be able to engage in sexual activity (CDC, 2015)—thus potentially contributing to the increasing number of older adults with HIV. When prescribing medications for ED, primary care providers (PCPs) could provide information on safe sexual practices; unfortunately, it is rare that PCPs provide information about safe sexual practices when prescribing medications for ED. Furthermore, despite the fact that older adults visit their health care providers more frequently, older adults are less likely than younger people to discuss their sexual habits with their health care provider (Lindau et al., 2007).
HIV prevention programs for older adults have been fairly limited and are dated (Davis & Zanjani, 2012). Furthermore, most of the HIV prevention programs for older adults take place in community settings and have not targeted primary care (Davis & Zanjani, 2012). However, the programs that have been implemented and evaluated have been efficacious for those who chose to participate (Coleman, Jemmott, Jemmott, Strumpf, & Ratcliffe, 2009; Falvo & Norman, 2004; Illa et al., 2010; Rose, 1996). PCPs are the main providers of health care for most older adults (CDC, 2009). PCPs are trained to provide preventive care and to obtain complete medical histories. Many studies have investigated increasing preventive health measures in primary care settings. For example, Yarnall, Pollak, Østbye, Krause, and Michener (2003) investigated the amount of time required for primary care physicians to provide all recommended preventive services from the U.S. Preventive Services Task Force (USPSTF). Yarnall et al. (2003) found that there was insufficient time to provide all recommended services. Alternatively, Jemmott, Jemmott, and O’Leary (2007) found that brief single-session, one-on-one, or group skill-building interventions facilitated by nurses in primary care may help to reduce HIV/sexually transmitted disease (STD) risk behaviors in a sample of African American women ranging in age from 19 to 45.
Given the increasing number of older adults living with and being diagnosed with HIV, it is imperative to explore PCPs’—including physicians, physician assistants, and nurse practitioners—willingness and perceived ability to increase HIV prevention practices among older adults, thus the purpose of the current research.
Conceptual Framework
Two theoretical constructs aided in the development of the semistructured interview guide used in this study and the interpretation of the findings by providing a framework for conceptualizing the findings. The ecological perspective (EP; Belsky, 1980; Bronfenbrenner, 1979; Eng, Hatch, & Callan, 1985) “emphasizes the interaction between, and interdependence of, factors within and across all levels of a health problem” (National Cancer Institute [NCI], 2005, p. 10). The theory highlights individuals’ interactions within their physical and sociocultural environments (NCI, 2005). In the EP model, behavior is viewed as being determined by the following factors (McLeroy, Bibeau, Steckler, & Glanz, 1988; NCI, 2005): intrapersonal levels (i.e., individual characteristics that influence behavior), interpersonal level (i.e., interpersonal processes and primary groups including peers), institutional level (i.e., rules, regulations, policies, and informal structures), community factors (i.e., social networks and norms, or standards), and public policy (i.e., local, state, and federal policies and law that regulate or support health actions and practices).
The theory of planned behavior (TPB) is an extension of the theory of reasoned action that adds a construct concerned with perceived control over performance of behavior (Ajzen & Driver, 1991). Perceived behavioral control was added in an effort to account for factors that are outside of the individual’s control that may affect their behavioral intention. The presence or absence of things that can make it easier or harder to perform the behavior affect perceived behavioral control (NCI, 2005). From the TPB, behavioral intention is the perceived likelihood of performing a behavior.
Taken together, these theories may help to explain PCP’s HIV prevention practices for older adults by taking into consideration the multiple levels that can affect HIV prevention practices in primary care settings (i.e., the EP) and other factors that are often outside of the control of PCPs that may influence their practices (i.e., theory of planned behavior).
Materials and Method
A total of 24 PCPs were interviewed, using a semistructured interview guide, regarding their willingness to increase HIV prevention efforts among older adults and the resources needed to do so. Saturation was reached with a total of 24 interviews. Interviews ranged from 12 min (n = 1) to an hour, with the average time being approximately 27 min. The interviews took place by telephone (n = 14) and face-to-face meetings (n = 10). Face-to-face interviews took place at a location most convenient for the providers, most commonly the provider’s office.
The sample was selected based on the availability of contact information for potential participants, for instance, business address or email address. Also, university health care and health care websites were used to obtain contact information for potential participants. Once contact information was obtained, potential participants were recruited through email messages, facsimile, and/or personal telephone calls. A total of 162 potential participants were identified and contacted via email, phone call, or fax and asked about their willingness to participate in a study about PCP’s HIV prevention practices among older adults. Of the 162, 58 indicated that they were no longer in primary care, one did not have time due to a high volume of patients, and the remainder failed to respond to email or telephone message (n = 79). All 24 interviews were transcribed verbatim, using Microsoft Word. Data analysis was conducted simultaneously with data collection by reviewing transcripts, making interpretations and notes, and revising questions, as appropriate. Once data collection was completed, the transcripts were reviewed repeatedly to ensure familiarity with the data and to make sure that there were no errors. Data from the semistructured interviews were organized and analyzed using thematic analysis (Burnard, 1991). The resulting themes were compiled into a codebook using Microsoft Excel. The Excel spreadsheet organized relevant key phrases and ideas by frequency to identify and explain repeating ideas or themes (Auerbach & Silverstein, 2003) in relation to each of the research questions.
Three strategies were used to enhance the accuracy of findings and reduce bias. Digital recording of interviews, notes, and entries into a reflective journal was reviewed to ensure familiarity with the data (Creswell, 2009). Data were collected from a range of participants who varied by years of experience, training, and medical specialty (Creswell, 2009). To increase reliability, the researchers checked transcripts to make sure that they did not contain mistakes during transcription. In addition, a subset of the interviews (n = 9) was co-coded to ensure consistent interpretation of themes (i.e., cross checks or intercoder agreement). A health care provider was involved in all aspects of this research.
All protocols and consent procedures were approved by the University of Kentucky Institutional Review Board (Approval No. 12-0686-P4S).
Results
A semistructured interview guide was developed as a guide for the interviews. Each participant was asked each question and additional questions to follow up on points made during the interview. All of the questions in the interview guide can be found in Table 1.
Interview Guide Questions.
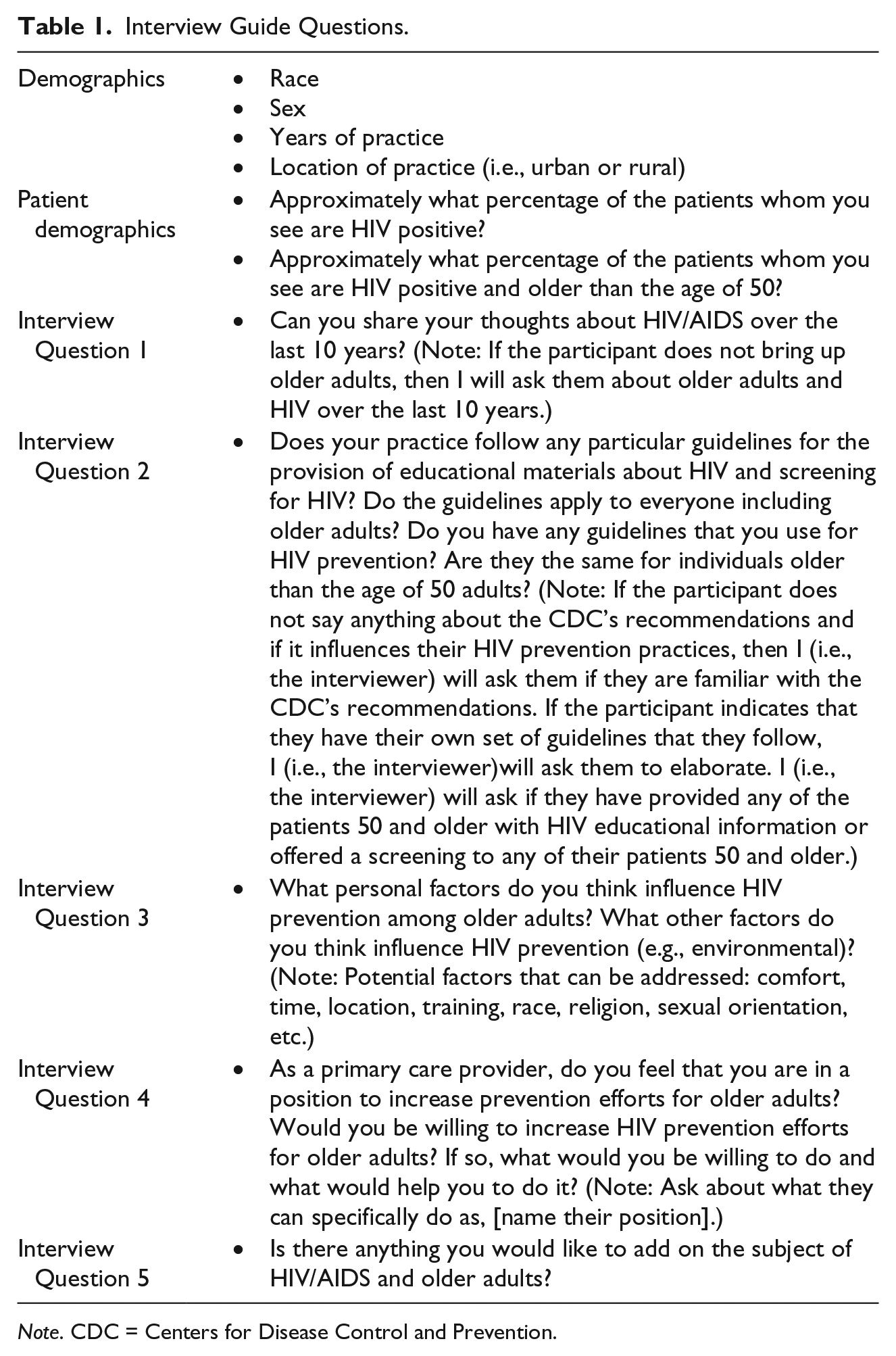
Note. CDC = Centers for Disease Control and Prevention.
A total of 24 PCPs were interviewed for this study, six nurse practitioners, two physician assistants, and 16 physicians. Participants represented a variety of medical specialties: internal medicine (n = 11), community clinics (n = 5), family medicine (n = 4), women’s health (n = 1), and infectious disease (n = 2). The providers were mostly female (n = 15) and White (n = 19). The remainder of the participants were Lebanese (n = 1), Hispanic (n = 1), Indian (n = 1), and African American (n = 2). A number of themes emerged when the qualitative interviews (n = 24) were analyzed in this study. The themes were shared by all the participants interviewed and included the following seven themes: (a) overall willingness to increase HIV prevention, (b) collaboration, (c) normalization, (d) increasing prompts to screen, (e) opportunities for HIV prevention, (f) improving the provider education, and (g) educating patients.
Overall Willingness to Increase HIV Prevention
To increase HIV prevention efforts in primary care settings, providers have to be willing to increase their prevention efforts for older adults. The majority of those interviewed indicated that they are willing to increase HIV prevention efforts. Only two of the 24 providers interviewed indicated that they would not be willing to increase their HIV prevention practices for older adults. One of the unwilling providers responded by saying: Given my empiric observation, the only patients that I see with HIV have had it for a long time. I don’t think that the elderly is a target population for HIV, now if you spun it around for syphilis or for gonorrhea or chlamydia those are definitely going to be things that are probably underappreciated especially in these, you know, senior living centers.
This may indicate a lack of awareness of the increasing number of older adults diagnosed and living with HIV and that a risk factor for HIV is the presence of other STDs. If an older adult is being screened for syphilis, gonorrhea, or herpes, then they should also be screened and educated about HIV. In the United States, people who get syphilis, gonorrhea, and herpes often are coinfected with HIV or are more likely to get HIV in the future (CDC, 2015).
Collaboration
Among those who were willing to increase HIV prevention for older adults, several suggested that collaborating with other providers would help to increase their efforts. One physician described an experience she had during her residency: We were supposed to offer it [HIV testing] like every time people came in unless they had one in three months. The nurses just did it themselves and have the results ready for you and um, that’s the kind of facilitation you need.
Collaboration may be an essential portion of the successful implementation of HIV prevention programs for older adults in primary care settings. As mentioned in the “Introduction” section, physicians alone cannot provide all preventive recommendations to their patients. However, if there is a collaborative effort among all providers in primary care, increasing HIV prevention practices may be less onerous. For example, another physician stressed that the team health care models have been effective in managing other types of chronic diseases and may prove effective in HIV prevention: I think that there is no doubt how we arrange sort of care team models and care management models and helping nurses to help be the gatherers of data and help us kind of do some of this front end work. Yes, I absolutely think that that’s [collaboration] always been proven in diabetes chronic care management and in other disease care management. Chronic disease management projects state that when the CMA or the nurses are engaged in processes it helps the physician and the numbers get better in diabetes, A1C numbers get better, their lipids get better, because someone is on top of it all the time . . . If in that process of the annual visit, the nurse can go through a checklist to say you know have you ever had HIV testing done and if so, when was it so that when you go in there, it’s like boom boom boom, man we need to do this.
Normalization, Increasing Prompts, and Opportunities for HIV Prevention
The theme of normalization emerged again and again. Participants reported that normalizing HIV testing would be beneficial to improving HIV prevention practices. One physician opined that HIV testing needs to be standardized: You know, when we, and I teach this to the first year medical students in interviewing that you say when you get to a sexual history we ask all patients about this and then you ask a preset list of questions.
A physician assistant shared a similar sentiment: It is just not the responsibility of the clinic, but that everyone who has a stake, has a responsibility to intervene and talk about it, so um, even when you have a different specialist you may have a cardiologist and endocrinologist and a primary care doctor and some you see in the emergency room to realize that everyone has a stake in prevention . . .
In an effort to increase the normalization of HIV prevention for older adults, there is a need to increase prompts to screen for HIV. If HIV prevention is to be viewed as a normal part of health care, then there should be prompts to screen for HIV, just like there are prompts for other annual screenings. Most providers suggested that electronic reminders would help increase their HIV prevention practices. According to one physician, So, having them be, then again it’s the norm, how do you get it on a template as more places go to EMRs [Electronic Medical Records] where it just says “hey like it pops up, person due, offer rapid HIV test.”
One physician emphasized that having reminders for HIV prevention on the intake form in addition to EMRs would be helpful: Like having it on the intake form that would signal our effort. Um, it would be nice to have something electronically too, to have an electronic reminder pop up and say this person has not been tested.
Opportunities for HIV prevention in primary care were discussed many times during participant interviews. The majority of providers indicated that wellness visits are an ideal time for HIV prevention. However, several mentioned other opportunities. One nurse practitioner suggested including HIV screening into the Welcome to Medicare visit: Medicare will pay for this expensive history/physical and updating it, here you can get your flu shot, you can get all this, I have not had the occasion to do one, but if it were included on that, there is like a checklist, then that might help.
Similarly, one physician discussed including HIV into the medical home concept: In some of those [medical home] are screening, appropriate screening, so I don’t know if this documentation of offering HIV screening is going to be a part of that yet or not. I don’t think it’s a measure I think they started with the easiest to digest. You know are you checking your diabetes A1C every six months are you getting your people referred to mammogram every two years?
Normalizing HIV prevention and increasing prompts for HIV prevention for adults may help to reduce the stigma associated with HIV and to increase overall rates of screening. Increasing HIV screening among older adults is essential in reducing delayed diagnosis and delays in treatment, as older adults often receive a late diagnosis of HIV and have a rapid transition from HIV to AIDS. If screening and education are offered yearly during a physical examination, that will help to normalize HIV prevention—so that it is just a routine part of health screenings.
Improving Provider Education and Educating Patients
Education for both providers and patients was a recurring theme. Providers suggested improving the HIV continuing medical education (CME) requirements to include information about older adults. One physician stated that the CME is not very useful as it is currently designed: There’s a HIV CME that is actually required in the state of Kentucky . . . um, it has nothing to do with HIV . . . it’s all about universal precautions basically.
Many providers reported that in medical school, there is no information on HIV/AIDS and aging. A PA specifically discussed integrating lesbian, gay, bisexual, and transgender (LGBT) health concerns into medical education: LGBT health concerns and issues should be mandatory in all medical curriculums period. It should not be something that you have a day of it is over. When we are talking about minority care we should include LGBT communities, both Lesbians and Gays have different risk factors for cancers and things like that. I think it starts in the training programs, when you don’t get it in school you don’t think that it is important to know . . . if there are not questions about it on your board exams um, there are not questions about it that you have to answer to get your degree then you don’t think that it is important.
One physician reported that she needs more practice having sexual health discussions with her patients: I probably need to have more practice having sex behavior discussions. Um, even if you are going to be in a monogamous relationship, they’ve never been tested, that kind of stuff needs to be done, because you know you need to test everybody and then say ok, well your spouse needs to be tested, too, you know?
In addition to education for providers, several providers suggested that educating patients about HIV/AIDS and aging would help to improve HIV prevention practices. For example, one NP suggested educating older adults about their risk factors: “I would think public health efforts to educate the population about their risk and things, so that they make better choices and practice safe sex.” Similarly, a physician felt that public education would help to raise awareness of HIV/AIDS among older adults. Other providers reported that having brochures with information specifically for older adults about HIV available for older adults would improve HIV prevention in their practice.
One physician acknowledged that older adults are more likely to have less information about HIV/AIDS as compared with other segments of the population. She indicated that providing information that included the number of older adults with HIV/AIDS would be helpful: And then they [older adults] suddenly find themselves widowers or widowed; they then have a second adulthood, and meet somebody and think that this person is okay and not knowing that the disease is out there. They are just ignorant because a lot of them have not had to deal with infidelity or having sex because they have been in a monogamous relationship for many years.
Educating both providers and patients will help everyone involved to recognize the importance of HIV prevention for older adults. Hopefully with education, providers will be more diligent about offering education and screening to older patients and older patients will be empowered to take control of their sexual health and ask for the information and screenings that they need.
Discussion
The results indicate that the majority of the providers are willing to increase HIV prevention efforts for older adults. However, many indicated that they would need assistance to increase prevention practices, for instance, increasing collaboration among providers and normalizing HIV prevention. Most providers suggested that increased collaboration among health care professionals would help to increase HIV prevention efforts. Previous literature indicates that NPs are in an ideal position to address unhealthy lifestyle practices and to promote health behavior change through ongoing patient encounters, such as cardiovascular disease (van Nes & Sawatzky, 2009). Also, several providers suggested that there should be greater collaboration among providers from different specialists in an effort to normalize HIV prevention. If HIV prevention efforts for all age groups become the standard of practice, then perhaps it will become less of a taboo topic—thus normalizing it. Increasing collaboration among providers is one way to normalize HIV prevention. Providers suggested that PCPs should collaborate with dentist and other medical specialists. A high percentage of individuals see the dentist annually (Siegel et al., 2012), and many signs and symptoms of HIV can be found in the mouth. Therefore, dentists are poised to be involved in HIV prevention efforts. Siegel et al. (2012) suggested that a larger cultural change may be required to engage dentists more actively in primary prevention and population-based screening.
Many providers suggested that using electronic reminders to prompt HIV prevention would be beneficial. Several recent studies have found that electronic reminders can increase HIV prevention practices in primary care facilities in the Department of Veterans Affairs. Bessesen, Stamper, Shaw, et al. (2012) found that the implementation of an electronic reminder system increases HIV testing rates from 2.7% to 16.7% (Bessesen, Stamper, Ojha, et al., 2012). Similarly, Loo et al. (2011) found that electronic reminders for other health screening and information improved the rates of vaccinations, bone density screening, and designation of health care surrogates among patients 65 and older (Loo et al., 2011). Providers recommended that electronic reminders could facilitate discussions regarding safe sexual practices when prescribing medications for sexual dysfunction. The Affordable Care Act and the American Recovery and Reinvestment Act should make the implementation of electronic medical health records easier, as they provide US$25 billion in incentives for physicians to use electronic medical records with the capacity for drug reconciliation, guidelines, alerts, and other decision supports (Kocher, Emanuel, & DeParle, 2010). The increase in electronic medical records has clear potential to increase HIV prevention among older adults.
It is well documented that older adults have little general knowledge about HIV/AIDS and their risk factors for contracting it (Altschuler, Katz, & Tynan, 2004; Falvo & Norman, 2004; Orel, Wright, & Wagner, 2004). Another component of collaboration is HIV/AIDS education for older adults. Many participants recommended that a clear need exists to increase opportunities for HIV/AIDS education among older adults, thereby enabling them to be collaborators in their own health.
Little is known about provider’s HIV prevention practices for older adults. Many providers suggested educating providers about HIV/AIDS during their medical education and continuing throughout their career. For instance, it was suggested that provider’s initial medical education be updated to include information about HIV/AIDS and aging. In addition, it was suggested that continuing education training be updated to include information specifically about HIV/AIDS and aging. Research on the effectiveness of CME varies; however, CME strategies that are interactive, use multiple methods, and are designed for small groups of providers may be most effective (Mansouri & Lockyer, 2007). Participants suggested giving providers an opportunity to practice having discussions about HIV prevention and sexual health with patients, thus developing CMEs that are interactive and designed for small groups of providers may prove effective.
The majority of providers indicated that wellness visits are an ideal time for HIV prevention practice, although several providers mentioned looking for other opportunities for HIV prevention, such as the Welcome to Medicare visit. The Welcome to Medicare visit is an appointment with a patient’s PCP that is devoted to organizing a preventive care plan. It presents an opportunity for providers to emphasize the importance of recommended screening tests and immunizations (Woolf, 2005), which should include HIV prevention. In addition, the medical home concept could be another opportunity to increase HIV prevention efforts for older adults. The medical home concept is described as a model or philosophy of primary care that is patient-centered, comprehensive, accessible, coordinated, and committed, to the quality and safety (Patient-Centered Primary Care Collaborative [PCPCC], 2013). The comprehensive component of the model includes preventive health (PCPCC, 2013), to which HIV prevention could be added. Both the Welcome to Medicare visit and the medical home concept offer opportunities to engage patients in HIV prevention efforts, in addition to annual wellness visits.
When interpreting the results of this study, there are some limitations to consider. For instance, we had a small sample size. In addition, the sample lacks geographic diversity. Future studies need to incorporate a larger, more diverse, and randomly selected sample to enhance HIV primary prevention efforts for older adults. This exploratory study serves as a first step in assessing PCP’s willingness to increase HIV prevention efforts among older adults and challenges that impede prevention efforts. This study adds to the literature on HIV and aging by providing recommendations from PCPs for improving HIV prevention in primary care settings. Primary care settings have been largely overlooked as a place for HIV prevention, despite the fact that older adults frequent primary care. The majority of interventions that have been tested have focused on those infected with HIV or gay or bisexual men in locations other than primary care. These recommendations will aid in the development of interventions designed to prevent HIV among older adults and to reduce the number of HIV-infected older adults who receive a delayed diagnosis of HIV among. Due to the immediate need for increased HIV prevention efforts for older adults, it is recommended that interventions be tested promptly.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.