
Abstract
Concerns about sleep problems and falls in older adults are significant. This article reviews the association between sleep problems and falls in community-dwelling adults aged 65 years or older. Multiple databases were searched from inception until 2015 using sleep, sleep disorders, and falls as keywords, limiting to studies published in English in peer-reviewed journals. After screening and assessing for eligibility, 18 articles were selected based on the inclusion and exclusion criteria. Findings of an association between sleep problems and risk of falls are conflicting, but some specific sleep problems such as extremely short sleep duration, daytime sleepiness and naps appear to be significantly related to falls in older adults. Methodological limitations including variability in covariates included in the analyses and measurement of the exposure and outcome variables were identified. The results of this review identified the need to have comparable definitions, validated tools, and rigorous design of future studies.
Introduction
Falls are among the most common and serious problems faced by older adults. About 30% of community-dwelling adults aged 65 years or above experience a fall per year and about 15% of them fall two or more times per year (Stel et al., 2003; Tromp, Smit, Deeg, Bouter, & Lips, 1998). In addition, 50% of adults aged 80 years and older fall at least once a year (Clyburn & Heydemann, 2011; Inouye, Brown, & Tinetti, 2009). Falls cause both fatal and nonfatal injuries. Falls are associated with reduced functioning, loss of independence, and premature nursing home admissions (Panel on Prevention of Falls in Older Persons, American Geriatrics Society and British Geriatrics Society, 2011). Specifically, falls are the primary reason for 85% of all injury-related hospital admissions (Weir & Culmer, 2004) and for more than 40% of nursing home admissions (Donaldson et al., 2005).
Various definitions of falls have been proposed. The World Health Organization (WHO, 2007) defines a fall as “an event which results in a person coming to rest inadvertently on the ground floor or other lower level.” Other similar definitions are provided by the Prevention of Falls Network Europe (ProFANE) group (Lamb, Jorstad-Stein, Hauer, Becker, & Prevention of Falls Network Europe and Outcomes Consensus Group, 2005) and the Kellogg International Working Group (Ory et al., 1993). Variations in the definition of falls may cause comparability issues among studies. The risk of falls is multifactorial (Panel on Prevention of Falls in Older Persons, American Geriatrics Society and British Geriatrics Society, 2011) and risk is associated with modifiable factors such as impaired vision, impaired balance and mobility, orthostatic hypotension, fear of falling, mood disorder, osteoporosis, incontinence and polypharmacy, and nonmodifiable factors such as age, gender, and race (Fabre, Ellis, Kosma, & Wood, 2010; van Nieuwenhuizen et al., 2010).
One important risk factor for falls that is still controversial is poor sleep in older adults. Sleep complaints are common in older adults. Approximately 50% of independently living adults aged 65 years or older in the United States report chronic sleep complaints (Crowley, 2011; D. Foley, Ancoli-Israel, Britz, & Walsh, 2004; D. J. Foley et al., 1995). Studies have used the terms sleep problems, sleep disturbance, poor sleep, and difficulty sleeping interchangeably. Sleep problems primarily include nighttime sleep problems such as trouble falling asleep and trouble with waking during the night (Brassington, King, & Bliwise, 2000). Daytime sleepiness and poor quality of sleep are also considered as sleep problems (Brassington et al., 2000). It is reasonable to expect that sleep problems might be a risk for falls for several reasons: Lack of sleep may cause daytime sleepiness, cognitive deficits, and reduced psychomotor performance, which might lead to increased risk of falls (Avidan et al., 2005), and insomnia could result in falls in older adults due to increased activity during the night in darkness (Brassington et al., 2000).
The consumption of medications to aid sleep such as sedative hypnotics is prevalent in older adults (Glass, Lanctot, Herrmann, Sproule, & Busto, 2005), and studies have shown that use of these medications is significantly associated with falls in older adults (Glass et al., 2005; Woolcott et al., 2009). However, most of these studies do not consider sleep problems as a potential confounder when assessing the relationship (Glass et al., 2005; Woolcott et al., 2009), and it is still unclear whether sedative hypnotics that are used for sleep problems contribute more than sleep problems alone to the risk of falling in this population; thus, it is imperative to first identify the association between sleep problems and falls in older adults. In addition, evidence of the association between sleep problems and falls among community-dwelling older adults is inconsistent in the literature. To date, there has been no systematic review integrating studies evaluating the association between sleep problems and risk of falls in older adults. Therefore, we conducted a systematic review of the literature to investigate the association between sleep problems and falls in community-dwelling adults aged 65 years or older. This study will help to elucidate whether sleep problems are a significant risk factor for falls in independently living older adults.
Method
The review was conducted based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher, Liberati, Tetzlaff, Altman, & PRISMA Group, 2010).
Eligibility Criteria
Studies were included if they met the following criteria:
Studies that evaluated poor sleep or other types of sleep problems as an independent predictor variable and the occurrence or number of falls or the risk of falls as an outcome variable.
Studies that included community-dwelling adults aged 65 years old or older. Community-dwelling older adults are noninstitutionalized older adults who live independently.
Studies that were published in English.
Studies that were published in a peer-reviewed journals.
Studies were excluded if they met the following criteria:
Studies that included specific subpopulations of older adults with specific health conditions such as Parkinson’s disease or dementia.
Studies that were reviews, commentaries, case-reports, case-studies, or newsletters.
Information Sources
A systematic search of studies from major databases was conducted from inception until December 31, 2015. The search was applied to Pubmed/MEDLINE (1946-2015), CINAHL (1937-2015), and PsycINFO (1887-2015) to identify relevant studies. Restrictions were applied to limit the search to studies in English. The last search was conducted in September 1, 2016. In addition, the gray literature was searched to find nonconventional publications through The New York Academy of Medicine (NYAM; 1992-2015).
Systematic Search Strategy
MeSH terms and text words of sleep problems and falls were used: (“Sleep”[Mesh] OR “Sleep Disorders, intrinsic ”[Mesh] OR “Sleep”[tw] OR “sleep disorders”[tw]) AND (“Accidental Falls”[Mesh] OR “Falls”[tw]). Similar search terms were used for CINAHL and PsycINFO. Quick search of the database for the gray literature through NYAM with a combination of “healthy aging fall” and “prevention fall” was conducted. See appendix for search algorithm.
Study Selection
Eligibility assessment was performed in a standardized manner by all the authors. In the first phase of the review, the authors independently reviewed the titles and the keywords of the articles. Studies that included the terms sleep or falls or older adults/elderly within a title or keyword were retained for further review of their abstracts. In the second phase of the review, abstracts were reviewed to determine whether the full texts should be reviewed. In addition, abstracts were reviewed if a title of keyword was not sufficient to determine whether to include it in the review.
Data Collection
Data extraction was conducted by all authors and reviewed multiple times to reduce error. The data included study design, year of publication, location, study population, study duration, sample size, measurement of sleep problems (a predictor variable), measurement of falls (an outcome variable), adjusted covariates, and association statistics such as odds ratio with 95% confidence interval and p value.
Methodological Quality Assessment
The Newcastle–Ottawa Scale (NOS) was used to assess the methodological quality of the studies. NOS is recommended by the Cochrane Collaboration as one of the most useful tools to evaluate nonrandomized studies, and it is simple to apply (Higgins & Green, 2011). The scale is used to judge the selection of the groups, the comparability of the groups, and the ascertainment of the exposure and the outcome of interest (Higgins & Green, 2011). Because 11 out of 18 of the reviewed studies were cross-sectional studies, an adapted form of NOS for cross-sectional studies developed by Herzog et al. (2013) was applied. The scores are predicted to be low and similar across the studies because most studies have assessed the predictor and outcome variables by self-report. Results are shown in Tables 1 and 2.
Methodological Quality of Included Prospective Cohort Studies by Newcastle–Ottawa Scale.

Note. A study can be awarded a maximum of one star for each numbered item within the Selection and Outcome categories. A maximum of two stars can be given for Comparability.
Methodological Quality of Included Cross-Sectional Studies by Newcastle–Ottawa Scale.
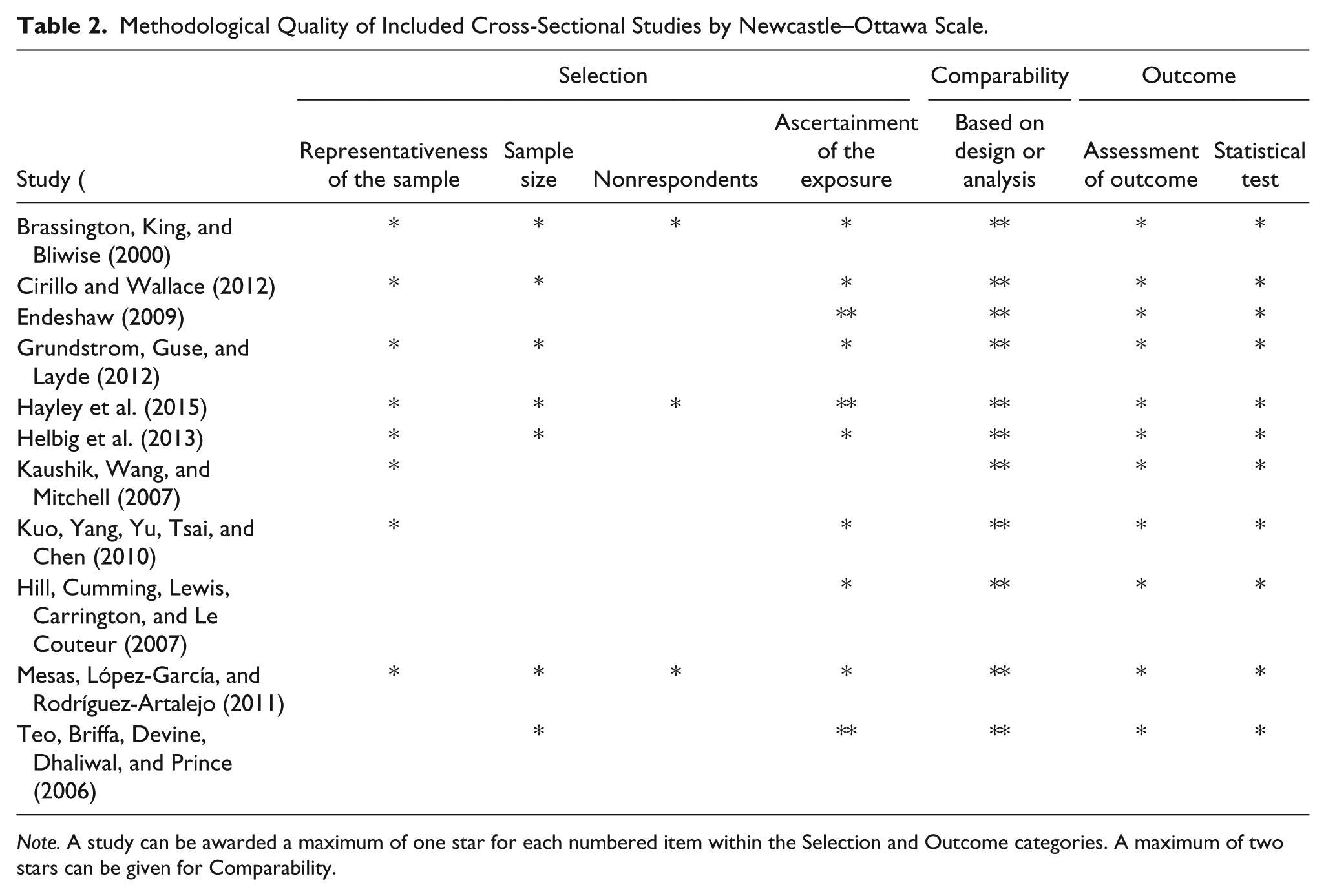
Note. A study can be awarded a maximum of one star for each numbered item within the Selection and Outcome categories. A maximum of two stars can be given for Comparability.
Summary Measures
To evaluate the association between sleep problems and falls, association statistics were reported as well as 95% confidence intervals. Adjusted association was the main statistic reported, but various confounding variables were adjusted across the studies.
Results
Study Selection
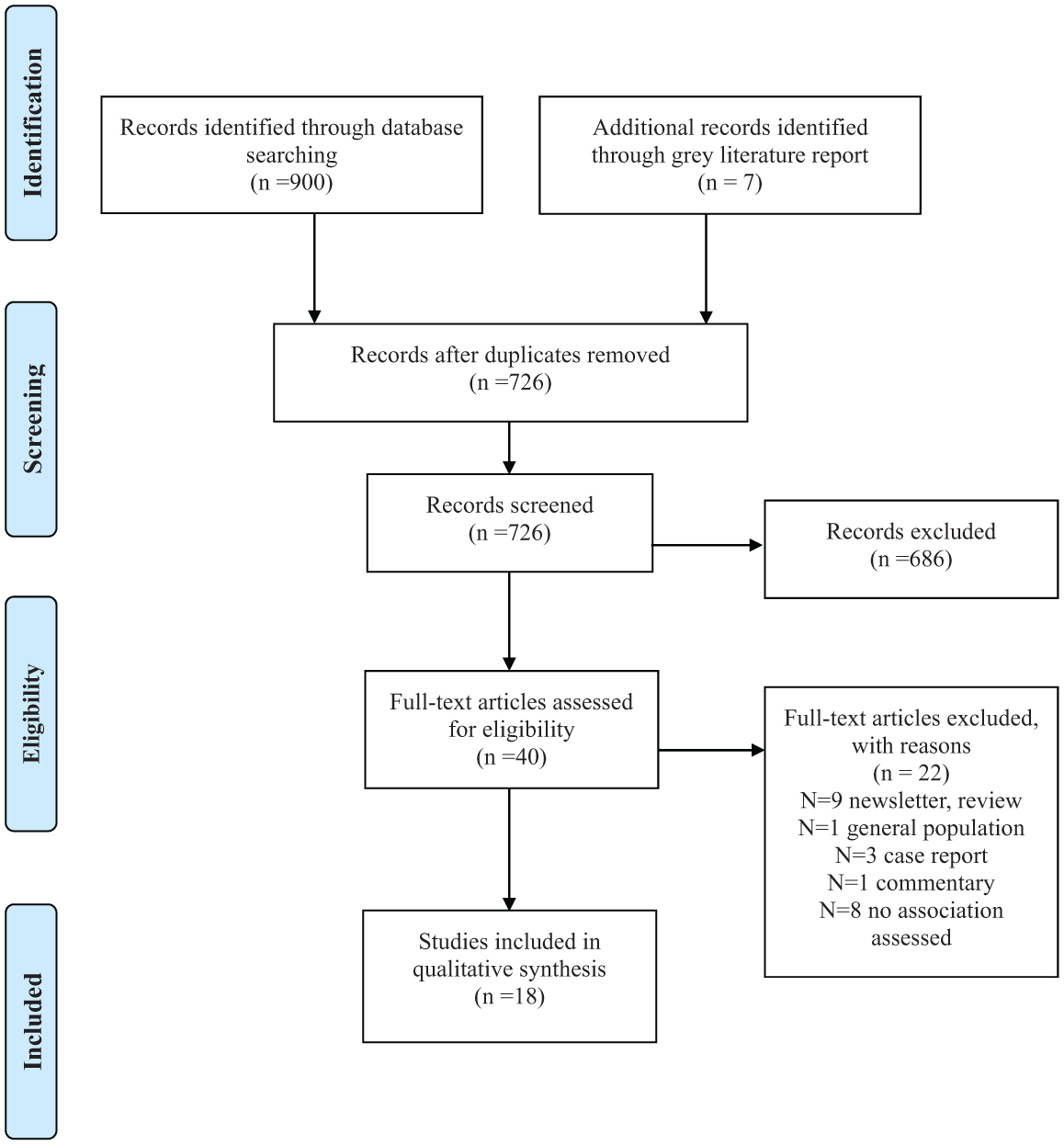
Figure 1 shows the flow diagram of studies included in the systematic review. A total of 584 studies were retrieved from PubMed, 291 studies from CINAHL, and 25 from PsycInFO. After a selection process, a total of 18 original research studies were included in this review.
Flow diagram for search strategy.
Study Characteristics
Out of 18 studies, 11 were cross-sectional studies and seven were prospective cohort studies. Sixteen studies included only community-dwelling older adults, while two studies included both institutionalized and community-dwelling older adults. Most of the studies were conducted in the United States and Australia. The predictor variable “sleep problems” was primarily collected by self-report or validated questionnaires. The most common questionnaire used was the Epworth Sleepiness Scale (ESS) which is a measure of daytime sleepiness. The outcome variable “falls” was collected by self-report either as a fall in the past 6 or 12 months. Table 3 provides a description of each study. The findings are organized by type of sleep problem evaluated in the study.
Summary of Included Studies.

Note. PSQI= Pittsburgh Sleep Quality Index ; BMI = body mass index; ESS = Epworth Sleepiness Scale; SF-36 = Short Form 36; IADL= Instrumental Activities of Daily Living.
Nighttime Sleep Problems and Falls
Four studies investigated whether nighttime sleep problems have an association with falls in older adults (Brassington et al., 2000; Byles, Mishra, Harris, & Nair, 2003; Helbig et al., 2013; Teo, Briffa, Devine, Dhaliwal, & Prince, 2006). Two studies reported a finding of a significant association between nighttime sleep problems and occurrence of falls (Brassington et al., 2000; Helbig et al., 2013). However, validated questionnaires were not used to assess the sleep problems in both studies. In addition, Helbig et al. (2013) found a significant association only in adults above 75 years of age. This might be due to differences in the level of frailty between younger old, that is, between 65 and 75 years old, and older and oldest old, that is, more than 75 years of age.
In contrast to these findings, two studies found no significant increase in risk of falls associated with nighttime sleep problems (Byles et al., 2003; Teo et al., 2006). Both of these studies (Byles et al., 2003; Teo et al., 2006) included only community-dwelling older women; thus, it is difficult to generalize to the entire population. It is possible that both studies included relatively healthy older women and therefore sleep problems did not results in falls in this population.
There are many differences among the studies that may contribute to the inconsistent findings. However, Brassington et al. (2000) and Helbig et al. (2013) included community-dwelling older adults of both sexes and with a broader range of age. Furthermore, these studies adjusted for more variables, including medical status or medications, that could be related to falls to account for the effect of the confounders in an attempt to find the relationship between sleep problems and falls (Brassington et al., 2000; Byles et al., 2003; Helbig et al., 2013; Teo et al., 2006); thus, nighttime sleep problems appear to be associated with falls in older adults.
Sleep Quality and Falls
Four studies specifically evaluated the relationship between sleep quality and falls (Endeshaw, 2009; Hill, Cumming, Lewis, Carrington, & Le Couteur, 2007; St George, Delbaere, Williams, & Lord, 2009; Stone et al., 2014). Only one study found that those who had no sleep problems (14%) were less likely to fall (OR = 0.3, 95% CI = [0.1, 0.9]; Hill et al., 2007). Endeshaw (2009), St George et al. (2009) and Stone et al. (2014) reported contrary findings. However, St. George et al. did not report the results separately for self-care units and assisted-care hostel participants, so there could have been different results in independent-living older adults alone.
Two studies did not define poor sleep quality and did not use a validated questionnaire to assess sleep quality (Hill et al., 2007; St George et al., 2009). Three studies (Endeshaw, 2009; Hill et al., 2007; St George et al., 2009) included both males and females, and all of the studies adjusted for the use of some kind of medication. Based on the studies that evaluated sleep quality and falls, poor sleep quality was not shown to be associated with the risk of falls, but this may be due to a lack of a consistent definition of sleep quality or the failure to use of validated tools to measure it.
Daytime Sleepiness and Falls
Six studies assessed the association between daytime sleepiness and falls in older adults (Brassington et al., 2000; Hayley et al., 2015; Helbig et al., 2013; Hill et al., 2007; Stone et al., 2014; Teo et al., 2006). Teo et al. (2006) showed that daytime sleepiness increased by twofold the risk of falls after adjusting for covariates of fall-related risk factors (OR = 2.05, 95% CI = [1.21, 3.49]). Similarly, Hayley et al. (2015) reported excessive daytime sleepiness to be associated with at least one fall (OR = 2.54, 95% CI = [1.24, 5.21]) in women after adjusting for use of a walking aid, nocturia, and antidepressant use. In addition, Stone et al. (2014) found daytime sleepiness to be significantly associated with risk of recurrent falls (OR = 1.52, 95% CI = [1.14, 2.03]). These three studies above used the ESS to measure the daytime sleepiness, and the ESS score greater than 10 indicates abnormal daytime sleepiness. Studies by Teo et al. and Hayley et al. found the risk in older women and the study by Stone et al. found the risk in older men. Brassington et al. (2000) found that daytime sleepiness is significantly associated with the number of falls but not with the occurrence of falls. In contrast, Hill et al. (2007), who used the ESS, found that daytime sleepiness was not significantly associated with falls in older adults. Despite using the same measure, varying results were documented. In addition, Helbig et al. (2013) did not find a significant association. Thus, it is difficult to conclude whether daytime sleepiness is significantly related to falls. To further investigate the relationship, more prospective studies that use objective measures of daytime sleepiness are needed.
Sleep Duration and Falls
Other sleep problems in older adults include short or fragmented sleep duration. Overall, the studies suggest that older adults experiencing short duration of sleep (less than 5 hours of sleep) are at risk for experiencing more falls than those who sleep normal hours (between 7 and 8 hours). Long duration of sleep (more than 9 hours) as a risk factor remains controversial.
Short duration of sleep
Nine studies assessed the association between short duration of sleep and falls in older adults. Five studies showed a significant relationship between short sleep duration and falls adjusted for use of either sedatives or psychotropic medications (Kuo, Yang, Yu, Tsai, & Chen, 2010; Mesas, López-García, & Rodríguez-Artalejo, 2011; St George et al., 2009; Stone et al., 2008; Stone et al., 2014). Of five studies, two prospective studies by Stone et al. (2008) and Stone et al. (2014) objectively measured sleep characteristics by using sleep actigraphy and found that sleeping 5 hours or less was significantly associated with recurrent falls compared with sleeping 7 to 8 hours per night.
In contrast, the same study that found a significant association with short sleep duration and falls did not find the association when sleep duration was self-reported (Stone et al., 2014). Cross-sectional studies by Brassington et al. (2000) and Hill et al. (2007) did not find a significant association between sleeping less than 8 hours a day and with the occurrence and number of falls. A cross-sectional study by Helbig et al. (2013) did not find any association with short duration of sleep (≥5 or 6 hours) and at least one fall in multivariable model including adjustment of psychotropic medication use. Finally, another cross-sectional study by Grundstrom, Guse, and Layde (2012) evaluated adults aged 85 years and older to assess whether days of perceived insufficient sleep, which represents the days when participants did not feel they got enough sleep or rest in the past 30 days, are associated with risk of falls. Insufficient sleep over the last 30 days was not associated with a higher risk of falls in the past 3 months (OR = 1.01, 95% CI = [1.00, 1.02]; Grundstrom et al., 2012). Among the studies that show no significance in the association, only the study by Helbig et al. adjusted for the use of sedative medications.
Long duration of sleep
Five studies evaluated long duration of sleep (8 hours or more per night) and falls (Helbig et al., 2013; Mesas et al., 2011; Stone et al., 2008; Stone et al., 2006; Stone et al., 2014). Two studies found that long duration of sleep was significantly associated with falls only in older adults (Helbig et al., 2013; Mesas et al., 2011). However, all three prospective studies by Stone et al. (2006), Stone et al. (2008), and Stone et al. (2014) found no relationship between long sleep (8 or more hours) and risk of falls in multivariable adjusted models.
Napping and Falls
Five studies investigated the association between napping and falls (Brassington et al., 2000; St George et al., 2009; Stone et al., 2008; Stone et al., 2006; Stone et al., 2014). There is a correlation between the two sleep factors of sleep duration and napping in that people who sleep less at night also have longer naps during the day. Three studies reported a significant association between napping and fall in old adults (Brassington et al., 2000; St George et al., 2009; Stone et al., 2006). Daytime napping was self-reported in all of these studies. Stone et al. (2006) found that women who took daily naps were more likely to have two or more falls during the following year (OR = 1.32, 95% CI = [1.03, 1.69]). The authors also found that women who nap 3 hours or more per week have a significant increased risk of recurrent falls compared with those taking naps less than 3 hours per week (OR = 1.33, 95% CI = [1.10, 1.60]; Stone et al., 2006). Studies that did not find any association with falls used actigraphy to measure naps (Stone et al., 2008; Stone et al., 2014). Actigraphy measures intentional and unintentional naps which could have measured more napping hours compared with measuring by self-report. Considering the consistency of the results that used self-report as a measure of napping, older adults reporting daytime napping have a significantly increased risk of falls.
Sleep Disorders
Five studies have investigated the relationship between specific sleep disorders and falls (Cauley et al., 2014; Cirillo & Wallace, 2012; Gassmann, Rupprecht, Freiberger, & IZG Study Group, 2009; Kaushik, Wang, & Mitchell, 2007; Stone et al., 2014). A prospective study by Gassmann et al. (2009) found that a diagnosis of a sleep disorder is a significant predictor among occasional fallers with only one fall (OR = 2.69, 95% CI = [1.58, 4.6]) and recurrent fallers who had two or more falls (OR = 2.96, 95% CI = [1.44, 6.06]) during the past 6 months compared with nonfallers in community-dwelling older adults (Gassmann et al., 2009). However, there was no further description or definition of sleep disorder provided; thus, the effect of the specific type or severity of the sleep disorder could not be assessed.
In a cross-sectional study by Kaushik et al. (2007), self-reported diagnosis of sleep apnea was found to be significantly associated with two or more falls during the previous 12 months (OR = 2.23, 95% CI = [1.11, 4.47]) after adjusting for covariates in older adults (Kaushik et al., 2007). No other sleep-related variables including snoring or witnessed apnea were found to be related to falls; however, quantitative results were not reported for these other variables.
A cross-sectional study by Cirillo and Wallace (2012) evaluated whether restless legs syndrome is associated with functional limitations among American elders. Based on the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5; American Psychiatric Association, 2013) criteria, restless legs syndrome is classified as a sleep-wake disorder. It is a tingling feeling in your legs and is often worse at night or when inactive. Two or more falls in the last 2 years were significantly associated with higher prevalence of restless legs syndrome (OR = 2.63, 95% CI = [1.49, 4.66]) but there was no association detected with falling only once (Cirillo & Wallace, 2012).
Finally, a prospective cohort study by Cauley et al. (2014) tested if nocturnal hypoxia during sleep is related to risk of falls because sleep disordered breathing is a common disorder in older adults. The study found that men with 10% or more of sleep time with oxygen saturation less than 90% had a greater risk of one or more falls (RR = 1.25, 95% CI = [1.04, 1.51]) and two or more falls (RR = 1.43, 95% CI = [1.06, 1.92]; Cauley et al., 2014). Similarly, the recent study by Stone et al. (2014) found nocturnal hypoxemia to be significantly associated with falls (OR = 1.62, 95% CI = [1.17, 2.24]). Both studies defined nocturnal hypoxia as 10% or more of total sleep time at a resting arterial oxygen saturation (SaO2) level less than 90%.
Specific sleep disorders, such as sleep apnea and restless legs syndrome were found to be significantly related to falls. Sleep apnea was defined by self-reported diagnosis and doubled the risk of experiencing a fall. In addition, people who fell two or more times had a higher prevalence ratio of restless legs syndrome. Sleep symptoms such as problems with early awakening were adjusted in the analysis to focus specifically on the impact of restless legs syndrome on the risk of falls.
Discussion
To our knowledge, this is the first systematic review to focus on the association between sleep problems and falls in community-dwelling older adults. Most of the studies that were included in the review explored this relationship as their primary objective. Based on this review, although the results are not consistent among all studies, short sleep duration, daytime sleepiness, and napping appear to be associated with an increased risk of falls. Because most of the studies were cross-sectional, it is difficult to draw conclusions about causality; however, the current results suggest that intervention strategies targeted to specific sleep problems could be developed that could reduce sleep problem-related risk of falls. Medication interventions such as benzodiazepine receptor agonists are commonly used to treat sleep problems by reducing sleep latency and improving total sleep duration (Taylor & Weiss, 2009), but they are recommended to be avoided in older adults due to other adverse events and if they must be used, it is recommended to use with other strategies that would help reduce fall risk (The American Geriatrics Society 2015 Beers Criteria Update Expert Panel, 2015). Moreover, the combined effect of poor sleep quality while using sleep medications increased the risk of falls (Min, Kirkwood, Mays, & Slattum, 2016), so focusing on the implementation of nonpharmacologic interventions to decrease daytime sleepiness and improve sleep duration may make more of a difference in fall risk than adding medications that may increase the risk of falls if sleep is not effectively treated.
Sixteen out of 18 studies accounted for medication use in assessing sleep problems and falls in older adults. Most studies mentioned specific classes or type of medications that were accounted for while only two (Brassington et al., 2000; Cirillo & Wallace, 2012) adjusted for any prescription medication use or the number of chronic medications used. Six studies clearly mentioned that they adjusted for sedative medications (Byles et al., 2003; Endeshaw, 2009; Helbig et al., 2013; Kaushik et al., 2007; Kuo et al., 2010; Mesas et al., 2011). Two studies adjusted for psychotropic medications (Helbig et al., 2013; St George et al., 2009) which one of them clearly considered sedative hypnotics (Helbig et al., 2013) and one study adjusted for medications acting on the central nervous system (CNS; Teo et al., 2006). Four studies adjusted for benzodiazepines (Cauley et al., 2014; Stone et al., 2008; Stone et al., 2006; Stone et al., 2014). However, the magnitude of the fall risk associated with sleep problems with or without adjusting for these medications was not possible to compare in most of the studies.
The association between sleep disturbances and falls can be explained by various mechanisms. Sleep disturbances may cause daytime sleepiness, impaired cognitive performance, balance and gait problems, and slower response time (Ancoli-Israel & Cooke, 2005; Avidan et al., 2005; Schlesinger, Redfern, Dahl, & Jennings, 1998). In addition, it is frequently mentioned that poor sleep may cause cognitive dysfunction with memory and concentration problems (Alapin et al., 2000; Cohen-Zion et al., 2001; Crenshaw & Edinger, 1999; Hill et al., 2007). All of these impairments are reported to be caused by poor sleep which may increase the likelihood of falls. In addition, combined impact of sleep problems and use of sleep medication can increase the risk of falls (Min, Kirkwood, et al., 2016; Min, Nadpara, & Slattum, 2016).
The NOS was used to assess the methodological quality in the included studies. The scores for the cross-sectional studies that were included in this review ranged from 5 to 9, while cohort studies ranged from 3 to 7. Lower scores indicate that there are deficiencies in the methodology of the studies (Herzog et al., 2013). Most studies included samples which are representative of the population of interest; however, they did not provide justification of the sample size. In addition, most studies controlled for demographic variables in addition to comorbidities and number of medications used. However, the type and number of covariates that were adjusted for varied across the studies which might result in comparability issues among the studies.
All studies except for three used subjective measures to assess sleep problems which can result in information bias (Cauley et al., 2014; Stone et al., 2008; Stone et al., 2014) Most studies did not use validated measures to assess sleep problems. In addition, the outcome of falls was primarily collected for the previous 12 months and evaluated by self-report. As the report of the outcome depended solely on the participants’ recall, recall bias is highly possible due to inaccurate memory of the past (Garcia, Dias, Silva, & Dias, 2015). It is imperative to accurately define the outcome of interest but there were variations in the definitions of falls across studies that were included. This systematic review has potential limitations. First, most studies included were cross-sectional in design. Out of the 18 studies that were included in the review, only seven studies were prospective cohort studies. Causal relationship cannot be established in cross-sectional studies. Second, two studies in the review included both institutionalized and noninstitutionalized elderly populations and reported the combined or less descriptive results. If the studies had evaluated both populations separately, it would have added to our understanding of the relationship between sleep problems and falls specifically for community-dwelling older adults. Third, there is a measurement bias in evaluating sleep problems and falls. Most studies designed their own questionnaires to collect sleep problems resulting in heterogeneity in assessments. Finally, some studies did not provide a definition of sleep problems and falls that they were examining. Consensus in defining the exposure and outcome will facilitate interpretation of the results of future studies.
In the future, there is a need to have more well-designed prospective cohort studies in this population to investigate the relationship between various kinds of sleep problems and falls. In addition, including a comparison group without any sleep problems would lead to a stronger conclusion about the association. It has been reported that self-report of certain aspects of sleep are not significantly different from polysomnographic estimates (Bliwise, 1992). However, more studies are needed that measure sleep objectively or at least use validated measurement tools which may better assess the exposure and facilitate comparisons among the studies. The same is true for the reporting of falls. There is a need to assess falls by more than one method to confirm each outcome.
Conclusion
In conclusion, this review provides insights that sleep problems are an important consideration in older adults with respect to the outcome of falls. Short sleep duration, daytime sleepiness and napping have the most evidence for increasing the risk of falls. Future research is needed to establish which specific aspects of sleep problems can cause falls, so that health care professionals can include appropriate assessments and interventions when managing fall risk in patients with sleep problems.
Footnotes
Appendix
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.