
Abstract
Alzheimer’s disease and other dementias are often associated with a gradual loss of the ability to participate in rewarding activities. Caregivers may struggle with spending quality time with the person with dementia (PWD) when the demands of caregiving dominate. However, the importance of activity participation among PWDs is internationally recognized. The Pleasant Events Schedule–Alzheimer’s Disease (PES-AD) Short Form measures frequency of engagement in pleasant events. It has been used to assess overall frequency of engagement in 20 activities. The current study involves a psychometric evaluation of the PES-AD Short Form and reveals two separate activity domains: active and social events, each with preliminary evidence of reliability and construct validity. Furthermore, the frequency with which the PWD enjoys social and active events are not uniformly related to PWD and caregiver characteristics and well-being, which has measure- and practice-focused implications that should be considered when engaging PWDs.
With the notable increase of persons more than 65 years being diagnosed with Alzheimer’s Disease and other related dementias, family caregiving has become a critical national health and social concern for our country. Quality time spent with the person with dementia (PWD) becomes a challenging goal for the caregiver when the many demands of caring dominate the home environment. Over time, caregiving becomes especially arduous for the family member, whether spouse, adult child, or sibling. Moments of satisfaction and pleasure for the dyad are few, as the daily tasks of attending to the increased number of personal care activities takes precedence (Burton, Zdaniuk, Schulz, Jackson, & Hirsch, 2003).
One notable consequence of the disease process is the PWD’s gradual loss of ability to participate in rewarding activities (Teri & Logsdon, 1991). One study by Teri and Logsdon (1991) noted that caregivers aware of appropriate and enjoyable activities for the PWD often experience an improved sense of efficacy as well as reduced feelings of burden and hopelessness. More recently, in a randomized controlled pilot study using a home-based intervention (Gitlin et al., 2008), activity prescriptions were implemented with caregiver dyads. Although there was no difference in quality of life between intervention and control groups, the program was readily accepted by the PWD and rated positively by caregivers. As noted by Letts and colleagues (2011) in a systematic review of leisure interventions, studying outcomes such as caregiver burden, activity, and participation have value and should be pursued. The challenge, then, for practitioners and researchers alike, is identifying activity programs that significantly enhance positive behaviors of the PWD and decrease caregiver stress.
The importance of activity participation has now been internationally recognized by the World Health Organization (WHO) in its revised document, International Classification of Functioning, Disability and Health (WHO, 2001). It contains language used to describe the everyday life of persons with some kind of limiting impairment of body function and/or structure. It looks specifically at their activities (i.e., performance of a task or activity), the contextual factors of a person (intrinsic to the individual) and environment (physical, social, and attitudinal), and the participation of the person in life situations. No matter whether the impairment is mental, physical, or social, everyday activities play a key role in one’s health and quality of life (American Occupational Therapy Association, 2014).
One tool to identify meaningful activities in which the PWD may engage is the Pleasant Events Schedule–Alzheimer’s Disease (PES-AD; Teri & Logsdon, 1991), developed as a clinical measure to assess pleasant activities with persons diagnosed with Alzheimer’s. Consisting of 53 events appropriate for an Alzheimer’s population, it was derived by selecting and modifying events from the original PES (MacPhillamy & Lewinsohn, 1982) and the PES-Elderly (Teri & Lewinsohn, 1982). An emphasis was placed on items appropriate for persons with mild dementia, including an equal number of items that were active–passive and social–nonsocial. For example, exercising” would be active, and “listening to music” would be passive. In addition, “having meals with friends or family” would be social, and “watching TV” would be nonsocial. The PES-AD Short Form (Logsdon & Teri, 1997) was then derived from the PES-AD to better suit the capabilities of PWDs and their caregivers. Thirty-three items were eliminated on the basis of redundancy, being rated as only minimally enjoyable, or not relating to the total score, resulting in 20 activities on the PES-AD Short Form. The 20 items are balanced between the two bipolar domains: social–nonsocial and active–passive. Respondents rate the frequency with which they have engaged in each activity in the past month (where 0 = “not at all,” 1 = “1-6 times,” and 2 = “7+ times”) and whether they enjoy each activity (where 0 = “no” and 1 = “yes”). Although the original PES-AD and the PES-AD Short Form can be scored in several ways, the most meaningful and commonly used method involves calculation of an overall “enjoyment” score, which represents the frequency with which the PWD engages in enjoyable activities. This score is calculated by taking the product of the frequency (rated 0, 1, or 2) and current enjoyment scores (rated 0 or 1) for each of the 20 activities on the PES-AD and then taking a sum of the products. This scoring is consistent with the “obtained pleasure” scoring method of the original PES (MacPhillamy & Lewinsohn, 1974, 1982). Overall, PES frequency of enjoyment scores range from 0 to 106 for the PES-AD and from 0 to 40 for the PES-AD Short Form.
Given widespread use of the PES-AD and the PES-AD Short Form (Cernin & Lichtenberg, 2009; LeBlanc, Cherup, Feliciano, & Sidener, 2006; LeBlanc, Raetz, Baker, Strobel, & Feeney, 2008; Mausbach, Coon, Patterson, & Grant, 2008; Mausbach, Harmell, Moore, & Chattillion, 2011; Mausbach et al., 2010; Moore et al., 2011; Searson, Hendry, Ramachandran, Burns, & Purandare, 2008), it is surprising that only one study has evaluated their psychometric properties (Logsdon & Teri, 1997). It evaluated the measures using a sample of 42 Alzheimer’s outpatients with mild cognitive impairment and revealed a strong association between enjoyment scores on the PES-AD and the PES-AD Short Form (r = .95, p < .0001). Furthermore, the enjoyment scores for both versions displayed adequate internal consistency reliability (α = .90 for the PES-AD and α = .96 for the PES-AD Short Form) and split-half reliability (α = .90 for the PES-AD and α = .96 for the PES-AD Short Form; Logsdon & Teri, 1997). There is also some evidence of convergent validity, such that those with better cognitive functioning, those with fewer depressive symptoms, and those without a depression diagnosis have greater enjoyment scores on both the PES-AD and the PES-AD Short Form, relative to those with worse cognitive functioning, or those with depression or greater depressive symptoms. Demographic characteristics (patient gender, age, relationship to caregiver) were not related to activity enjoyment for either version of the PES-AD (Logsdon & Teri, 1997).
A more extensive psychometric evaluation of the PES-AD Short Form is warranted because it may be more feasible to use with cognitively impaired patients and their caregivers (relative to the PES-AD, more than twice as long). The scoring and factor structure of the PES-AD Short Form is one area in which more investigation would be of value; the frequency by enjoyment product for all 20 activities is summed together to create one overall frequency of enjoyment score, despite the PES-AD Short Form having been developed with distinct, theoretically based social–nonsocial and active–passive domains in mind. Scoring the PES as one overall score based on all 20 items is especially surprising, given the multiple factors identified in psychometric work conducted on the original PES (MacPhillamy & Lewinsohn, 1982), from which both the PES-AD and the PES-AD Short Form were derived. In this work, one general and six specific subscales of the 320-item PES have been noted, based on theoretical and varied statistical rationale (principal component analyses, correlations, cluster analysis): social versus nonsocial, masculine–feminine, introverted–extraverted, outdoorsmanship–inside; sexual activity; and items related to positive mood (MacPhillamy & Lewinsohn, 1982). With the exception of the positive mood scale, the PES scales demonstrated adequate test–retest reliability at 2 months as well as concurrent, predictive, and construct validity (MacPhillamy & Lewinsohn, 1982).
Although earlier work has demonstrated high internal consistency and some evidence of convergent validity for the PES-AD Short Form, a substantially larger sample is necessary to adequately assess the PES-AD Short Form’s dimensionality. Therefore, the primary aim of this study was to examine the factor structure of the PES-AD Short Form among 220 Veterans with mild-to-moderate dementia and to then gather some preliminary evidence of construct validity on the resulting factor structure. Using data from a large Veterans Affairs (VA) treatment outcome study, we investigated whether the 20 activities on the PES-AD Short Form best function as one or more scales.
Method
Participants
Participants were 220 Veterans with pain and mild-to-moderate dementia enrolled in a randomized controlled trial of a pain treatment intervention (intervention described in Kunik et al., 2016). Participants were identified whether they had (a) a dementia diagnosis represented by the International Classification of Diseases, Ninth Revision, Clinician Modification codes 290, 294, or 313, resulting from a search of the VA Outpatient Data Files; (b) an active prescription of a VA class CN900 medication for dementia (donepezil, galantamine, memantine, or rivastigmine) as indicated in the VA’s Decision Support System pharmacy files; or (c) a provider referral to the study. Participants met the following inclusion criteria: (a) documented diagnosis of dementia, (b) receipt of primary care from the Veterans Health Administration, (c) residence outside a long-term care facility, (d) residence within 50 miles of the Michael E. DeBakey VA Medical Center in Houston, Texas,USA, (e) mild-to-moderate dementia (as determined by Functional Assessment Staging Test [FAST] scores between 2 and 6), (f) no history of aggression in the past year, (g) presence of a caregiver directly involved with the PWD at least 8 hr per week, and (h) clinically significant pain, as noted by either the caregiver or the PWD, indicating that the PWD had at least “a little pain” overall on the Philadelphia Geriatric Pain Intensity Scale. Veterans who met inclusion criteria completed a written consent form and a phone-based baseline assessment. The current study exclusively used screening and baseline data.
Measures
Demographic data, including age, education, ethnicity, race, income, and relationship type, were collected from both the PWD and his or her caregiver during the baseline assessment. Other measures included the following:
PES-AD Short Form
As discussed above, although various versions of the PES exist for different populations, the 20-item PES-AD Short Form was derived from the 53-item PES-AD and designed to be a brief measure of enjoyment of pleasant events for respondents with cognitive impairment (Logsdon & Teri, 1997). For each activity, caregivers rated the frequency with which the PWD had participated in the activity over the last month (0 = “not at all,” 1 = “1-6 times,” 2 = “7+ times”) and whether the PWD enjoyed the activity (0 = “no” and 1 = “yes”). For each activity, frequency scores (0-2) were multiplied with enjoyment scores (0-1) and then responses were summed across the 20 activities. Total frequency of enjoyment scores ranged from 0 to 40 with higher scores indicating greater engagement in enjoyable events than lower scores.
FAST
The FAST is a clinician-rated measure of functional decline in dementia that consists of seven stages (from one to seven), with higher stages indicating greater cognitive impairment and more severe dementia (Reisberg, Sclan, Franssen, Kluger, & Ferris, 1994). The FAST combines clinical observation with informant data and has demonstrated adequate reliability and validity (Reisberg et al., 1994).
PWD worst pain
Worst pain was assessed via the Philadelphia Geriatric Pain Intensity Scale, which asks “thinking about the past several weeks, please rate how bad your pain was when it was at its worst” (where 0 = no pain, 1 = little pain, 2 = moderate pain, 3 = quite bad pain, 4 = very bad pain, and 5 = the pain is almost unbearable). Patient pain was rated by both the PWD and the caregiver.
Geriatric Depression Scale (GDS)
The GDS consists of 30 yes/no questions that the caregiver answers indicating how the PWD felt over the past week. After reverse scoring where appropriate, scores were summed to create a total PWD depression score that ranged from 0 to 30, with scores above 10 suggestive of depression (Yesavage et al., 1983). Internal consistency and test–retest reliability are acceptable (Stiles & McGarrahan, 1998).
Burden Interview
The caregiver of the PWD completed the Burden Interview (Zarit, Reever, & Bach-Peterson, 1980), a 22-item instrument that assesses the perceived impact of caregiving on the caregiver’s financial status, physical status, physical health, emotional health, and social activities. This instrument was included as a measure of caregiver well-being.
Mutuality Scale
Caregiver–patient relationship quality was assessed by having the caregiver complete the 15-item Mutuality Scale (Archbold, Stewart, Greenlick, & Harvath, 1990), which examines the caregiver–PWD relationship.
Data Analyses
We first conducted a confirmatory factor analysis (CFA) to evaluate the applicability of a one-factor structure of the PES frequency of Enjoyment scale in a predominately male sample of Veterans with dementia (N = 220). Fit of the model to the data, percentage of variance in each item accounted for by the model, and correlation residuals were examined to evaluate the model. To determine goodness of fit, the comparative fit index (CFI), the Tucker–Lewis index (TLI), and the root mean square error of approximation (RMSEA) were estimated. According to Kline (1998), CFI and TLI values greater than 0.90 reflect good model fit. For the RMSEA, values below 0.05 indicate good fit. Chi-square is also reported (with significant values representing poor fit). However, it is important to note that, with large samples, chi-square may be significant even when all other fit indices illustrate an adequate fit (Tabachnick & Fidel, 2001).
We subsequently conducted a first-order exploratory factor analysis to identify the optimal number of factors to describe the associations among items. Two methods were used: an examination of the scree plot of eigenvalues and a parallel analysis, an empirically supported retention procedure involving simulation that retains factors that have an eigenvalue extracted from the correlation matrix that are greater than the 95th percentile of the distribution of eigenvalues obtained from random uncorrelated data (Hayton, Allen, & Scarpello, 2004). The factors were estimated with an unweighted least-squares method, extracted with a principal components solution, and then rotated with a promax oblique rotation. Items were retained if they displayed simple structure (i.e., loadings of at least .50 on a factor and twice as high on one factor relative to all other factors).
Cronbach’s alpha coefficient was used to evaluate the internal consistency reliability among the items that loaded onto any given factor. Construct validity of each factor was then assessed with both univariable and multivariable methods. We first used univariate linear regression models to examine the ability of (a) patient demographics (i.e., age, education, ethnicity, race, income), (b) caregiver demographics (i.e., age, education, ethnicity, race, income, and relationship to patient), and (c) cognitive impairment to predict each PES factor. For each factor, predictors individually associated with the factor at p ≤ .25, were then included simultaneously in a multivariable model (Bendel & Afifi, 1977). Education was coded such that 0 represented those with a high school education or less and 1 represented those with at least some college education; race was coded such that 0 represented Caucasian and 1 represented non-Caucasian; and the caregiver’s relationship with the PWD was coded such that 0 represented spouse and 1 represented other family member. We then used multiple linear regression models to examine frequency of engagement in active and social events as unique predictors of PWD and caregiver well-being. Specifically, we conducted three models, each with active and social PES predicting (a) PWD depression, (b) PWD–caregiver mutuality, and (c) caregiver burden. All factor analytic analyses were conducted in Mplus version 5.21 (Muthén & Muthén, Los Angeles, CA), whereas analyses assessing internal consistency reliability and construct validity were conducted with SAS version 9.4 (SAS Institute, Cary, NC).
Results
Sample
PWD were predominately male and were an average of 79.15 years of age (SD = 8.48 years). Nearly half had mild cognitive impairment to moderate dementia (FAST score between 2 and 5), and slightly more than half had moderately severe dementia (FAST score of 6). Most caregivers were women, and the majority were the PWD’s spouse, followed by son/daughter and other relative. See Table 1 for demographic and clinical characteristics of PWDs, and Table 2 for demographic characteristics of caregivers.
PWD Demographics and Clinical Characteristics (N = 220, Unless Otherwise Noted).
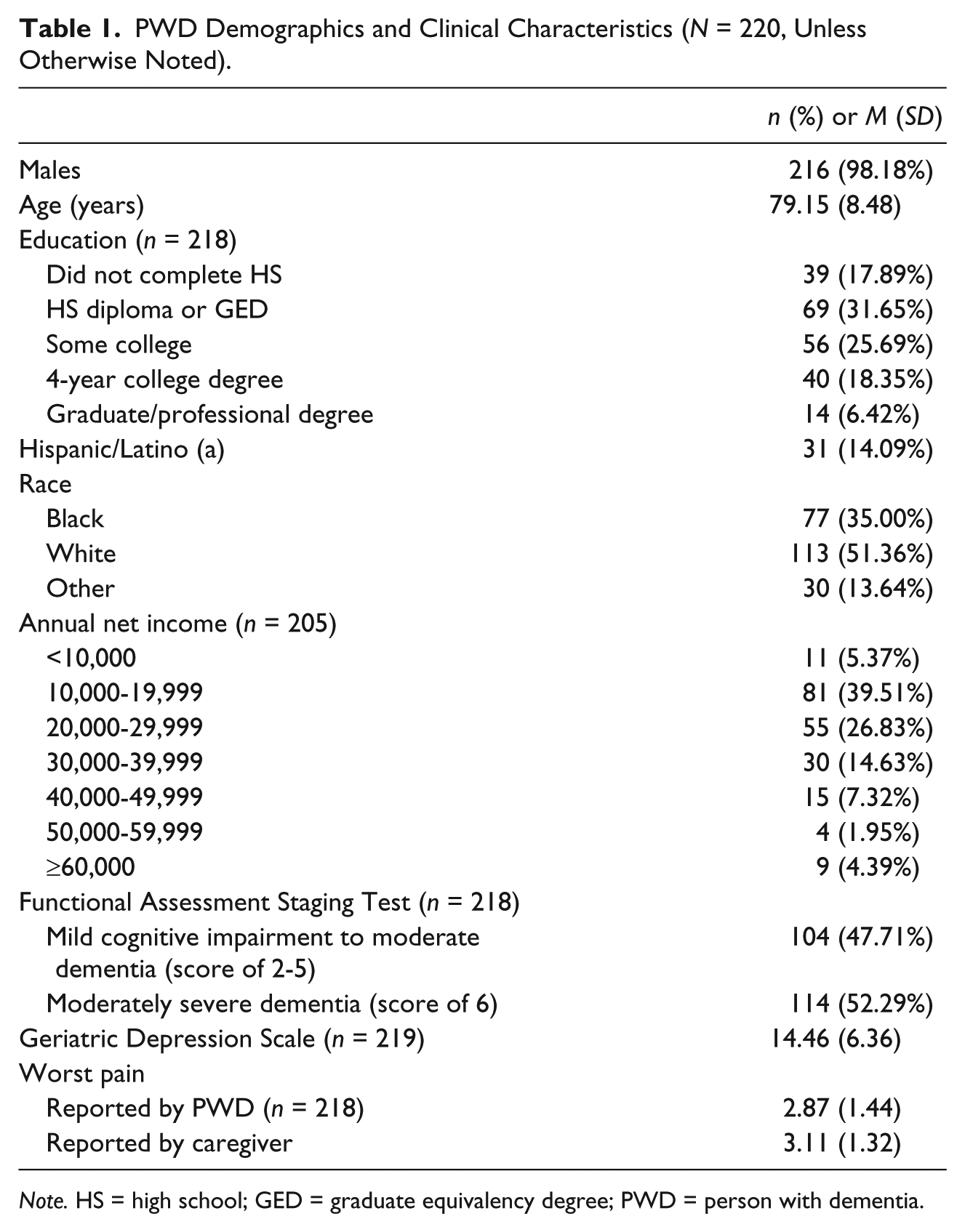
Note. HS = high school; GED = graduate equivalency degree; PWD = person with dementia.
Caregiver Demographics (N = 220, Unless Otherwise Noted).
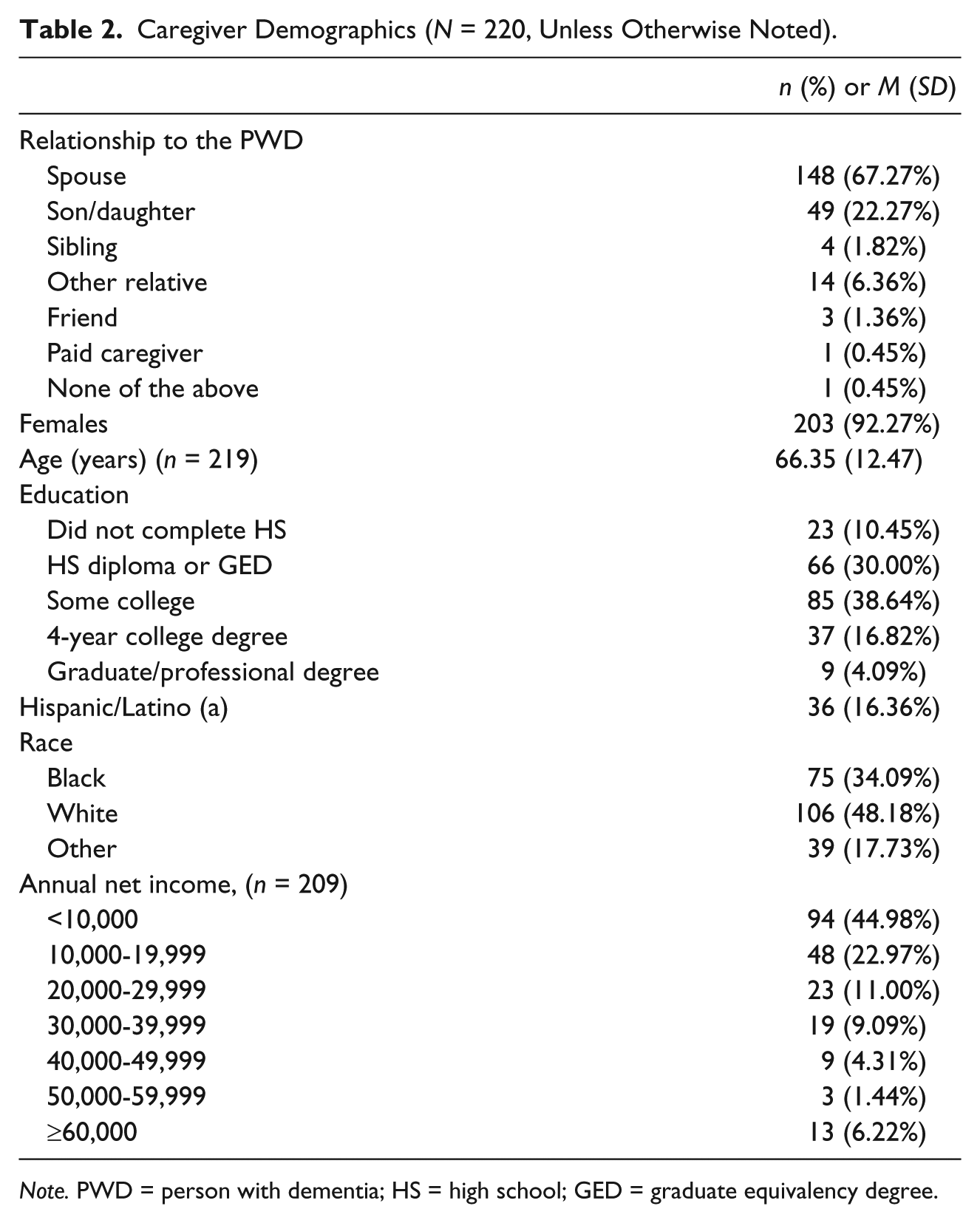
Note. PWD = person with dementia; HS = high school; GED = graduate equivalency degree.
CFA
The CFA revealed that a one-factor structure was not a good fit to the data, χ2(76, N = 220) = 159.39, p < .0001, CFI = 0.82, TLI = 0.86, RMSEA = 0.07. The amount of variance in each item accounted for ranged from 7% to 46%, with only one item above 40%. Many of the bivariate residuals were higher than ideal. Nearly a third (31.67%) were equal to or greater than 0.10, and nearly two thirds (64.44%) were equal to or greater than 0.05. These results suggest that a one-factor structure is inadequate for representing PES-AD Short Form frequency of engagement in enjoyable activities among this sample of dementia patients that consisted mostly of men.
Exploratory Factor Analysis
Whereas the examination of eigenvalues (5.23 and 2.00, respectively) and the scree plot suggested retention of two factors, the parallel analysis suggested retention of three factors. The loadings for the three-factor solution are presented in Table 3. Factors 1 and 2 appear to capture predominately active and social pleasant activities, respectively. Six items load strongly and uniquely onto Factor 1 (e.g., shopping /buying things, helping around the house, exercising) and four items load strongly and uniquely onto Factor 2 (e.g., being with family, laughing, having meals with family or friends). Frequency of enjoyment for only one item (Getting/sending letters, cards) loads strongly and uniquely on Factor 3. Frequency of enjoying this event was low (with only 5% of respondents indicating that they have enjoyed it at least 7 times in the last month). Given that this factor (Factor 3) is underrepresented and potentially a product of low endorsement, we dropped Factor 3 from subsequent evaluation. Nine items that cross-loaded on multiple factors (i.e., did not display simple structure) or that did not load strongly onto one factor were also dropped. A follow-up CFA revealed that the 10-item, two-factor model provided an excellent fit to the data, χ2(25, N = 220) = 0.63, CFI = 1.00, TLI = 1.00, and RMSEA = 0.00. The first factor captures enjoyment in active events and the second factor captures enjoyment in social events.
Results of Exploratory Factor Analysis for Frequency of Enjoyment, With Full 20 Items.

Note. Bolded items represent items that load strongly (≥.50) and uniquely onto one factor (at least 2 times as high on the factor than any other factor). PES = Pleasant Events Schedule.
Factor 3 is represented by only one item, and is, therefore, underrepresented and dropped from subsequent analyses. (Note that it likely loads by itself because of the extremely low level of endorsement.)
Evaluation of Frequency of Enjoyment in Active and Social Events
The internal consistency reliabilities of these short subscales were borderline acceptable at 0.70 for the active factor and 0.67 for the social factor. However, applying the Spearman–Brown prophecy formula, reliabilities would be .89 and .91, respectively, if these subscales were the length of the original PES-AD Short Form. Total active and social frequency of enjoyment in pleasant event scores were calculated by taking the sum of the frequency of enjoyment scores for each item within that factor. Total scores range from 0 to 12 for the frequency of enjoyment of active events and from 0 to 8 for the frequency of enjoyment of social events. Mean frequency of engagement scores were 5.92 (SD = 2.92) for active events and 5.88 (SD = 1.80) for social events. The bivariate correlation between the two factors was r = .31, p < .001, indicating that the active and social factors are similar while still providing unique information.
Predictors of Frequency of Engagement in Active and Social Events
Enjoyment in active events
In univariable regression models, PWDs who had caregivers with at least some college education (vs. a high school education or less) and those with a caregiver who was a nonspouse family member (vs. a spouse) had a greater frequency of enjoyment in active events (both ps < .05; see Table 4). In addition, PWDs with moderately severe dementia (vs. less severe dementia) had a lower frequency of enjoyment in active events (p = .002). In the multivariable model, caregiver education and PWD cognitive ability remained unique predictors of frequency of enjoyment in active events, whereas the relationship between the caregiver and PWD was no longer a significant predictor.
Univariable and Multivariable Regression Models for the Active Pleasant Events Factor (Factor 1).
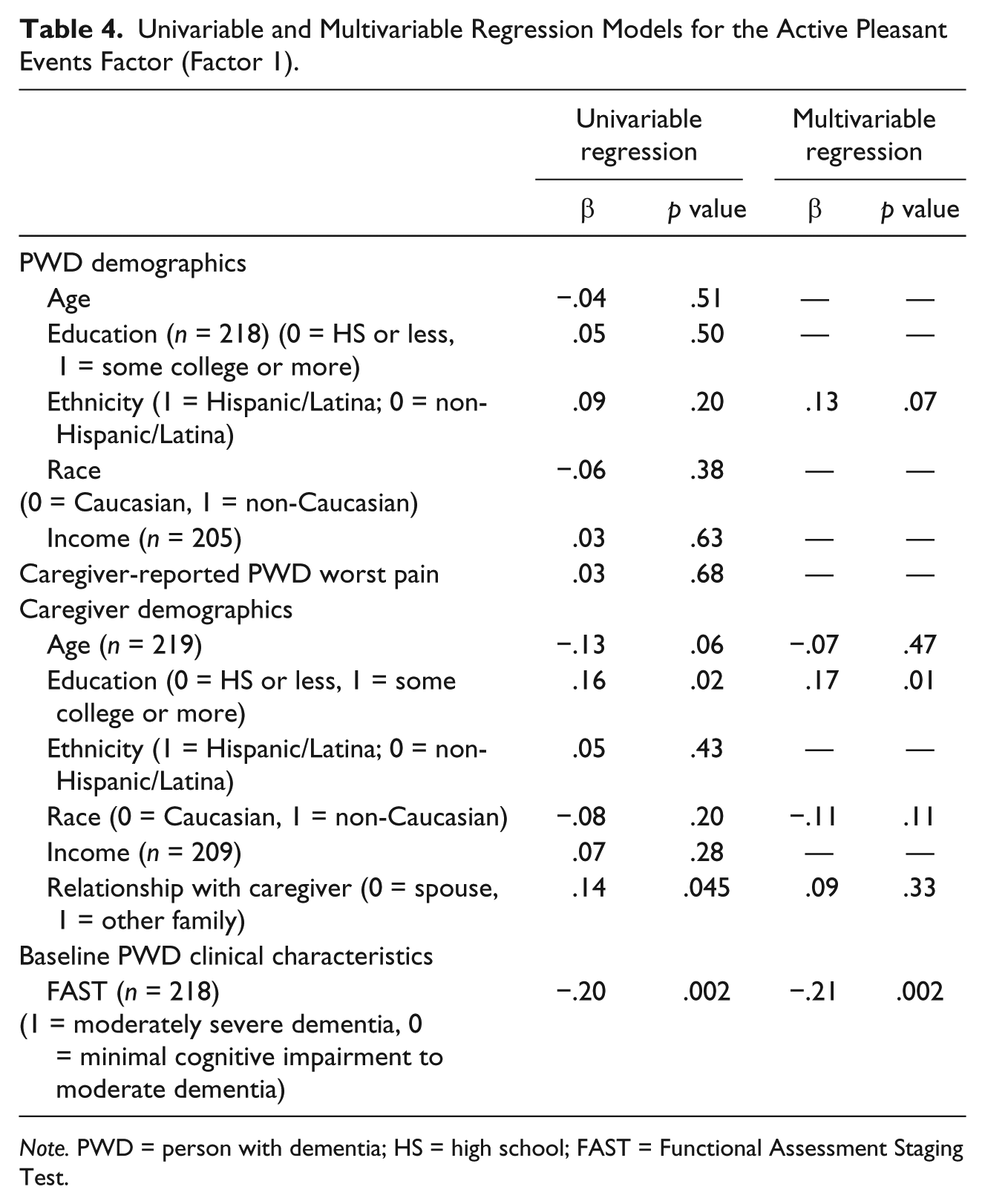
Note. PWD = person with dementia; HS = high school; FAST = Functional Assessment Staging Test.
Enjoyment in social events
In univariable regression models, PWDs with at least some college education (vs. a high school education or less), PWDs with greater income (vs. lower income), and PWDs with nonspousal family caregivers (vs. a spouse) had a greater frequency of enjoyment in social events (all ps < .05; see Table 5). In addition, PWDs with caregivers who were older had lower frequency of enjoyment in social events than those with younger caregivers (p = .002). In the multivariable model, each of these variables remained unique predictors of frequency of enjoyment in social events, with the exception of caregiver age.
Univariable and Multivariable Regression Models for the Social Pleasant Events Factor (Factor 2).

Note. PWD = person with dementia; HS = high school; FAST = Functional Assessment Staging Test.
Active and Social Events as Unique Predictors of PWD and Caregiver Well-Being
Frequency of engagement in both active and social events were uniquely associated with less PWD depression (active: β = −.30, p < .0001, social: β = −.28, p < .0001) and less caregiver burden (active: β = −.16, p = .02, social: β = −.14, p = .04). However, although frequency of engagement in social events was uniquely associated with greater PWD–caregiver mutuality (β = .37, p < .0001), frequency of engagement in active events was unrelated to mutuality (p > .05, Table 6).
Multiple Linear Regression Models Separately Predicting GDS, Mutuality, and Burden.
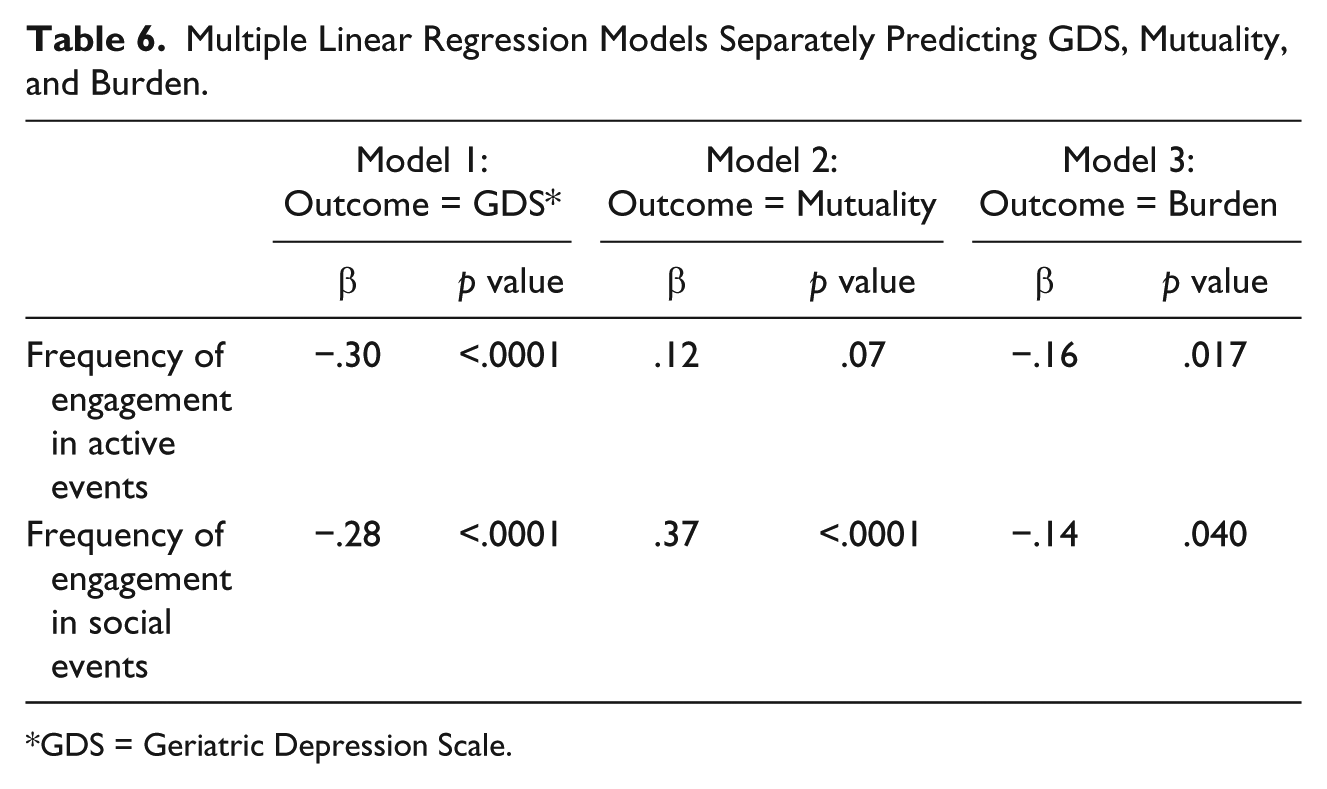
GDS = Geriatric Depression Scale.
Discussion
Exploratory factor analysis yielded two readily interpretable scales for the PES-AD Short Form, with borderline acceptable internal consistency reliability and some evidence of construct validity for this predominately male Veteran population with mild-to-moderate dementia and pain. Scoring the PES-AD Short Form as a 10-item, two-factor scale (with an Active scale and a Social scale) departs from the original scoring and item composition of the PES-AD Short Form, which included only a single factor of enjoyment of pleasant activities that consists of all 20 items.
The current work reveals that frequency of engagement in active and social events is neither uniformly predictive of PWD and caregiver well-being outcomes nor are PWD and caregiver characteristics uniformly related to the frequency with which the PWD enjoys both social and active events. Furthermore, associations with depression and cognitive impairment are not always consistent with what was found with the single-dimension scoring of the PES-AD. Prior work that examined the PES-AD Short Form as a single 20-item factor indicates that less depressed and less cognitively impaired PWDs engage more frequently in pleasant events in general than those who are more depressed and more cognitively impaired (Logsdon & Teri, 1997). Similarly, we found that greater engagement in both active and social events was uniquely associated with less (relative to more) depression among PWDs. However, those with greater cognitive impairment (relative to those with less cognitive impairment) engaged less frequently in active events only, as cognitive impairment was unrelated to frequency of engagement in social events.
Furthermore, the current results suggest that when the caregiver has at least some college education, PWDs more frequently engage in active events than when the caregiver has only a high school education or less. This makes sense given those with greater education tend to be more active across a variety of domains (Baum & Payea, 2005) and therefore, may encourage the PWD to be active. Furthermore, when the PWD has at least some college education, the PWD has a higher income (relative to lower income), or the caregiver is a nonspouse family member (relative to a spouse), PWDs more frequently engage in social events. Relative to spousal family caregivers, nonspouse family caregivers (e.g., sons/daughters, siblings) who oftentimes do not live with the PWD may have an augmented perception of the extent to which their loved one engages in various social activities. Importantly, although greater frequency of engagement in both active and social events were associated with reduced caregiver burden, only greater engagement in social events was associated with increased PWD–caregiver mutuality. These results are consistent with studies among seniors that indicate a negative relationship between frequency of social activities and relational loneliness (e.g., Gilmour, 2012). There are both measure- and practice-focused implications of these findings.
The current findings are consistent with both the theoretical justification for selecting both social–nonsocial and active–passive items for the PES-AD and the previous psychometric work on the original PES (MacPhillamy & Lewinsohn, 1982), each suggesting a multidimensional factor structure. That said, there appears to be value in abandoning the use of the frequency of enjoyment score on the PES-AD Short Form as a single factor and scoring it instead as two separate factors: a social factor and an active factor. The two-factor PES-AD Short Form eliminates activities that do not load strongly and uniquely onto either the active or social factor, resulting in 10 activities, which is a relatively more parsimonious measure for PWDs and their caregivers.
The active and social factors are related, but not strongly and are differentially related to PWD and caregiver characteristics, which has important implications for clinical practice. If a clinician is aware of a dyad’s demographic profile up front, these findings can guide selecting activities that the PWD may find enjoyable. For example, if the PWD is only mildly cognitively impaired and mildly depressed, the clinician might recommend active events, such as exercising or going on outings. However, if the PWD has at least some college education and the caregiver is younger, the caregiver might recommend more social events that involve being with family, such as having meals with family or friends.
Based upon our findings, implications for future research and clinical application include several possibilities. In terms of further study, one option is to update the measure to solely include the 10 active and social items. However, due to the small number of items in each factor (i.e., four and six), the internal consistency reliability is not ideal. A few additional activities could be added to both the active and social factors in an effort to boost the internal consistency reliability of these scales. Furthermore, the activities listed in the PES-AD Short Form may need to be updated to include activities that pertain to technology and social media (e.g., emails, Facebook, texting). If the construct of pleasant events conceptually encompasses more than just active and social events among PWDs, removal of the 10 items of the PES-AD Short Form that do not load onto these two factors may result in failure to adequately and fully capture the construct of engagement in pleasant events. For example, reading/writing may be an important activity domain independent from the others, as suggested by the original three-factor solution. However, the factor was underrepresented in the current analysis. In this case, additional items would need to be developed to measure reading/writing and then subsequently undergo psychometric evaluation. The 10-item PES-AD Short Form may be a good starting point for identifying frequency of engagement in some common active and social events that could then be followed up with open-ended interviews to capture frequency of engagement in other activities the PWD may find enjoyable.
For health care professionals, analyzing an activity for its “active” and “social” value has practice implications. Knowing what leisure activities are appealing to PWDs with specific characteristics (regarding education, depression, and relation of caregiver) enables personalizing activity selection and individualizing the treatment focus. It negates the “one-menu” activity calendar or limited range of activities typically offered to PWDs.
There are a few characteristics of the sample that limit the generalizability of the findings. First, as this study predominately consisted of male Veterans, it would be of value to evaluate the PES-AD Short Form with a sample of women or, at least, one with equal representation of gender, as well as within the general community Second, the sample included only persons diagnosed with dementia; broadening the sample to include other diagnoses or even a “normal” older adult population would provide wider generalization of its utility. Third, both active and (to a lesser extent) social PES scores in this sample may be somewhat restricted relative to the general population of patients with dementia given this sample consisted of PWD who were experiencing at least minimal pain. Furthermore, a deeper examination of how the individual items function overall and between groups using item response theory and differential item functioning would be an important future step in evaluating the PES-AD Short Form.
Over the years, the PES, in all its varied formats, has proven useful in research among older adult populations. Substantial evidence exists of the value of engagement in pleasurable activities by the caregiver dyad and as an indicator of quality of life and positive mood. A notable example of its use was in the Tailored Activity Program (TAP) by Gitlin and colleagues (2008), where the PES-AD was used to identify previous and current activity interests and an activity prescription served as an integral part of the intervention with caregivers and PWDs. They found that tailoring activities to the skill level of the PWD and training families in using pleasurable activities reduced problem behaviors and caregiver burden. Furthermore, there is evidence that incorporating daily pleasant experiences into caregiving routines reinforces the positive aspects of caregiving (Au et al., 2015). This current analysis adds a unique perspective to the usefulness of the PES-AD Short Form, with the intent of contributing to its psychometric soundness as well as of highlighting the importance of meaningful activity among PWD.
Footnotes
Authors’ Note
The National Institutes of Health had no role in the design and conduct of the study; the collection, management, analysis, and interpretation of the data; or the preparation, review, or approval of the article. The opinions expressed are those of the authors and not necessarily those of the National Institutes of Health, the National Institute of Nursing Research, the Department of Veterans Affairs, the U.S. government or Baylor College of Medicine.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This material is the result of work funded by the National Institutes of Health, National Institute of Nursing Research (Grant R01-NR014657-01A1), and use of facilities and resources at the Houston VA HSR&D Center for Innovations in Quality, Effectiveness and Safety (CIN13-413).