
Abstract
Most of the 5.4 million people affected by Alzheimer’s disease and other forms of dementia (AD) are noninstitutionalized, receiving care by unpaid family caregivers and medically managed by a primary care provider (PCP). Health Information Technology has been recognized for its potential in improving efficiency and quality of AD care and support for AD caregivers. Simultaneously, smartphone technologies have become an increasingly common way to deliver physical and behavioral health care. However, little is known about how smartphone technologies have been used to support AD caregiving and care. This article highlights the current need for smartphone-based interventions for AD and systematically identified and appraised current smartphone apps targeting and available for AD caregivers. Findings indicate that individual available apps have limited functions (compared with the complex needs of caregivers) and little has been done to extend AD caregiving apps to Hispanic populations. Implications for research, practice, and policy are discussed.
Among the 5.5 million people affected by Alzheimer’s disease and other forms of dementia (AD; now labeled as neurocognitive disorders in the Diagnostic and Statistical Manual of Mental Disorders [5th ed.; DSM-5; American Psychiatric Association, 2013], but still commonly referred to by providers, patients, and caregivers as dementia), most are non-institutionalized, receiving care by unpaid family caregivers and medically managed by a primary care provider (PCP; Alzheimer’s Association, 2017; James et al., 2014). Health Information Technology (HIT) has been recognized for its potential in improving efficiency and quality of AD care and supporting AD caregivers (Vedel, Akhlaghpour, Vaghefi, Bergman, & Lapointe, 2013; Zulman, Piette, Jenchura, Asch, & Rosland, 2013). In addition, smartphone technologies have become an increasingly common way to deliver physical and behavioral health care (Boulos, Wheeler, Tavares, & Jones, 2011; Luxton, McCann, Bush, Mishkind, & Reger, 2011). However, little is known about how smartphone technologies have been used to support AD caregiving and care. This article will review the current need for smartphone-based interventions for AD caregivers, discussing the benefits and challenges to such technologies; review and appraise the current state of such technologies; and discuss ways of moving forward by bridging science, policy, and practice.
AD Care and Caregiving
The challenges of AD care and caregiving are well documented. Many providers have difficulty with collecting clinical information about AD patients, due to communication problems associated with their condition and limited time dedicated to medical visits with AD patients and their caregivers (Hinton et al., 2007). Simultaneously, AD caregivers often experience stress, burden, and depression from their caregiving activities, resulting in US$9.3 billion in health care costs for Americans in 2012 (Alzheimer’s Association, 2017). A meta-analysis of 17 studies found the aggregate prevalence of depression among AD caregivers was 33.9% and aggregate prevalence of anxiety disorders was 43.6% (Sallim, Sayampanathan, Cuttilan, & Ho, 2015).
Attributing to AD caregiver stress are a lack of support system for caregiving, overwhelmed or insufficient coping skills, low utilization of available services, and the behavioral problems that are common among AD patients (Alzheimer’s Association, 2017; Kelly, 2015). The current state of AD care is more dire for minorities, given the barriers and racial disparities found in health care services and outcomes for African American and Hispanic AD patients and caregivers (Alzheimer’s Association, 2017; Amatniek et al., 2006; James et al., 2014; Williams, 2005).
The Potential for Smartphones in Dementia Care and Caregiving
Smartphone technologies are ideal for health care interventions, because they include multiple functions, such as Internet access, mobile telecommunication, sensors, notifications, and the ability to install applications that are clinically focused (Putzer, 2012). In fact, mobile technologies have been shown to be an effective approach to health monitoring for adults with varying chronic medical conditions (Hardinge et al., 2015; Mallow, Theeke, Barnes, Whetsel, & Mallow, 2014; Schnall, Bakken, Rojas, Travers, & Carballo-Dieguez, 2015). Zhang, Ho, Cheok, and Ho’s (2015) review also reported that smartphone apps have been shown to support patient care in mental health settings for conditions including psychosis/schizophrenia, depression, bipolar disorder, and substance abuse. Specifically, such technologies have shown effectiveness in monitoring patient symptomology, facilitating patient self-management, screening patients for depression, and providing an adjunct to talk therapy. Smartphones also have demonstrated to be potentially useful for assessing cognitive function in older adults (Brouilette et al., 2013; Kwan & Lai, 2013) and delivering personalized reminiscence therapy (Zhang & Ho, 2017), and early research is currently examining the use of smartphone technologies for communication therapy in persons with neurological disorders (Ireland et al., 2016) and to help with safety monitoring for older adults (Sun et al., 2014).
In addition, access to smartphones and other smart devices has become increasingly widespread. In 2013, 80.7% of homeowners ages 35 to 44 years and 65.2% who are ages 45 to 64 years reported having a smart device in their household, with low-income, Hispanic, and African Americans reporting more likely than their non-Hispanic White, Asian, and higher income counterparts to rely only on a smart device for computer access (File & Ryan, 2014). Hence, smartphone-based technologies for AD caregiving may help in extending access to HIT to vulnerable populations that are digitally underserved. It is anticipated that as mobile technologies become more commonly used by older adults, they will increase their comfort with using mobile devices, similar to computer use trends (American Association of Retired Persons [AARP], 2016). Findings also show that training older adults to use mobile devices can increase their technological literacy and competency (Delello & McWhorter, 2017).
As smartphone-based HIT has become more common in the delivery of health care, smartphone apps have targeted the issue of dementia, though the majority of applications have targeted people with AD, such as apps that support memory or safety (Armstrong, Nugent, Moore, & Finlay, 2010). Little technology has been developed to support AD caregivers or link them with the providers of the people they provide care for, and a MEDLINE search revealed that there currently is limited evidence to establish the efficacy of smartphone app technology for improving AD care or caregiver outcomes. While smartphone apps targeting AD caregivers exist, they are mostly designed to monitor the AD care recipient’s location (Thorpe et al., 2016) or activities (Stucki et al., 2014).
Improving Access and Quality of Care
There are a number of problems with AD care that can be addressed through smartphone technologies. Currently, effective AD caregiver interventions exist for improving the emotional health and well-being of caregivers (Alzheimer’s Association, 2017), although most of these interventions are too time-intensive, costly, and/or burdensome for busy caregivers to widely disseminate (Health Council of South Florida, 2010). Smartphone platforms may create evidence-based (Zhang et al., 2016), low-cost, and flexible options for supporting and educating AD caregivers. Smartphone technologies may also increase the quality and quantity of information shared among AD caregivers and providers. Caregivers offer a wealth of knowledge about AD patients’ behavioral and psychosocial status (e.g., depression symptoms, conditions of the home environment) that could be helpful to providers in clinical decision making, but are not typically collected through existing HIT (Glasgow, Kaplan, Ockene, Fisher, & Emmons, 2012). Such information could be reported to providers through smartphone technologies in real-time and at their convenience. Research has also demonstrated that communication between in-home health providers and patient’s physicians, especially across institutions, is limited and often inefficient (Ruggiano, Brown, Hristidis, & Page, 2013; Elhauge, 2010; Eloranta, Welch, Arve, & Routasalo, 2010; Fairchild, Hogan, Smith, Portnow, & Bates, 2002). To improve clinical decision making, there is a need for in-home and other providers to share such information securely and easily across institutions (Diamond & Shirky, 2008). This could be achieved through mobile technologies that caregivers use in partnership with in-home providers to share appropriate information with the AD care recipient’s physician.
Supporting Rural AD Caregiving
Smartphone-based interventions may be a particularly valuable resource in rural areas, where geographic distance may impede timely access of medical records or the receipt of health care services. While broadband Internet access has lagged in many rural areas, 95% of individuals worldwide were covered by a mobile-cellular network in 2015 (ICT Data and Statistics Division Telecommunication Development Bureau International, 2015). Hence, smartphone technologies may provide opportunities for rural caregivers to access HIT in regions of the United States where Internet access is limited or unavailable, but cellular coverage is available. Indeed, an Alabama Alzheimer’s Disease Task force (2015) identified health technology as a strategy for providing education and support for AD care for those in rural underserved areas of Alabama. Mobile health technologies may be particularly helpful in reducing the long distances that older adults and their caregivers need to travel for care (Morgan et al., 2011). Providers have reported interest and acceptance in using mobile technologies for health care in rural settings (Carter-Templeton & Wu, 2015), and a national survey found that rural primary care settings used a broader range of electronic medical record capabilities than those in urban settings and reported no difference in Internet connectivity (Singh, Lichter, Danzo, Taylor, & Rosenthal, 2012). However, costs of HIT has shown to remain a barrier for implementing HIT in rural settings (Agency for Healthcare Research and Quality [AHRQ], 2008, n.d.), and a lower proportion of rural hospitals have received federal incentive payments relative to their urban counterparts for establishing HIT for meaningful use (Sandefer, Marc, & Kleeber, 2015), which only serves to exacerbate existing disparities. Hence, the potential for smartphone technologies to offer cost-effective ways of integrating technology in AD care and caregiving should be further explored.
Need for Current Review
Despite the potential opportunities for improving AD care and caregiving, there is little knowledge about smartphone technologies targeting the needs of AD caregivers. In fact, a review of the literature revealed that there has been a dearth of clinical trials of such technologies. Therefore, an initial step in assessing the current state of technology is to review the availability and content of smartphone apps for AD caregivers that are currently available on the market. The aims of this review were to (a) assess the availability of smartphone apps for AD caregiving and (b) evaluate the content and features of AD caregiving apps to assess which AD caregiving activities they support.
Method
A review of caregiver smartphone apps was conducted in January 2017. Given the lack of smartphone app research in the academic literature, two investigators (E.B., J.L.) independently conducted Internet searches using Google (see Figure 1). Key search terms used included “dementia caregiver and smart phone app,” “dementia caregiver and app,” “Alzheimer’s disease and smartphone app,” and “Alzheimer’s disease and app.” In addition, apps were identified through multiple sources including Google Play, Apple’s App Store, Internet blogs and articles, app web sites, and organizational web sites. To qualify for inclusion in the study, a smartphone app needed to be in English, downloadable (Google Play or Apple’s App Store), and have a primary function of supporting and/or educating caregivers consistent with self-perceived needs of dementia family caregivers (McCabe, You, & Tatangelo, 2016). AD caregiver support and education function were defined as app features that address one or more challenges reported by AD caregivers, including lack of information about AD, lack of a support system for AD caregiving, overwhelmed or insufficient coping skills, low-utilization of available services, and/or difficulties in managing care recipient mood and behavioral disturbance (AARP, 2016; Alzheimer’s Association, 2017; Kelly, 2015; McCabe et al., 2016; Parker, Mills, & Abbey, 2008). Evaluation of whether the app met eligibility criteria was made by the consensus of two investigators (E.B., J.L.).

Flow chart of smart phone apps searched and screening procedures: Organized with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) template.
Two investigators (E.B., N.R.) qualitatively assessed the characteristics and features of the identified apps, and there was strong agreement (96% interrater reliable agreement) in categorizing and describing the app characteristics and features that were identified and assessed for apps (see Table 1). Disagreements in the assessments were discussed and resolved. The text appearing on the supporting website pages associated with the included smartphone apps was also assessed for readability. These websites were accessed to obtain information about app features including introductory information and details about use and navigation. There is evidence that AD caregivers need introductory information and support in utilizing electronic caregiver interventions (Gaugler, Reese, & Tanler, 2016; Brown et al., 2016). Readability was assessed with the Automated Readability Index Calculator (http://www.webpagefx.com/tools/read-able/automated-readability-index.html) for text on website. A grade-level indicator is provided by the readability calculator for the U.S. grade school system. To calculate the grade-level indicator, six unique readability assessments were calculated and summarized in making the grade assessment including the Flesch Kincaid Reading Ease, Flesch Kincaid Grade Level, Gunning Fog Score, SMOG Index, Coleman Liau Index, and the Automated Readability Index.
Characteristics and Features Assessed Among AD Caregiving Apps.

Note. Note that a few of these categories may not to be mutually exclusive. For example, a “reminder” to take a medication can also be viewed as helpful for “medication management.” Decisions in categorizing features were made through investigator consensus. AD = Alzheimer’s disease and other forms of dementia.
The Mobile App Rating Scale (MARS) was also used to assess the quality of the apps. Twelve apps were assessed (one app could not be accessed) by two investigators working independently. The MARS is a reliable measurement tool for evaluating the quality of mobile apps that are health-related (Stoyanov et al., 2015). Prior to the review, both reviewers watched the Youtube MARS training video (https://www.youtube.com/watch?v=25vBwJQIOcE) made available by the first author of the article establishing properties of the MARS (Stoyanov et al., 2015). As suggested in the MARS training, the reviewers discussed potential issues of conducting MARS assessments for dementia caregiver apps, and general information regarding dementia caregiving challenges was provided before starting the assessment. The MARS (Stoyanov et al., 2015) multidimensional measure assessment items are organized across four domains: engagement (five items), functionality (four items), aesthetics (three items), and information quality (seven items). In addition, an overall app quality score is calculated. It should be noted that the assessment of information quality provides the option for the rating of “not available” for five items which is not to be included in the score. Each of the 19 MARS items is rated using a 5-point scale (1 = inadequate, 2 = poor, 3 = acceptable, 4 = good, 5 = excellent). As the purpose of the current review is to assess the current market of available AD caregiver apps, rather than compare and contract individual apps, an aggregate score of MARS was generated for the apps included in this analysis.
Results
A total of 30 caregiver apps were initially identified by the two investigators in January 2017. However, only 13 apps met eligibility criteria (see Appendix A in Supplementary Material). Eight of the apps did not have a caregiver focus; several of these apps were focused on personal medical records, other health conditions, and hospice support. Seven of the identified apps were not available to be downloaded at the Google Play or Apple’s App Store. One app had two unique names and therefore only one version was included in the review. One was web-based without a smartphone app. Descriptive findings about the included apps are provided below.
App Characteristics: Development and Availability of Smartphone Apps
Of the 13 apps reviewed, 53.8% (n = 7) were developed in the private sector, two were developed by a nonprofit foundation, one by a government entity, one by an academic institution, and in two cases, the type of developing entity was unidentifiable. Most of the apps were developed in the United States, 53.8% (n = 7); one was developed in Canada; one in Sweden; one in Australia; and one in the United Kingdom. In two cases, the country of development was unidentifiable. All 13 apps were available in English (as per eligibility criteria). In addition, two of the apps were available in multiple languages including Dutch and German. One app was available in Chinese. Eleven of the apps were downloaded at the Apple’s App Store and two were downloaded at the Google Play Store. Four apps were available at both Google Play and Apple’s App Store. Most of the apps were updated in 2016 or 2017 (n = 10); three were updated in 2015 or earlier. All of the apps were free in English with the exception of one that had a cost of US$2.99. One app had a cost of US$0.99 for an alternative language version.
Features: Content and Functions of Caregiver Apps
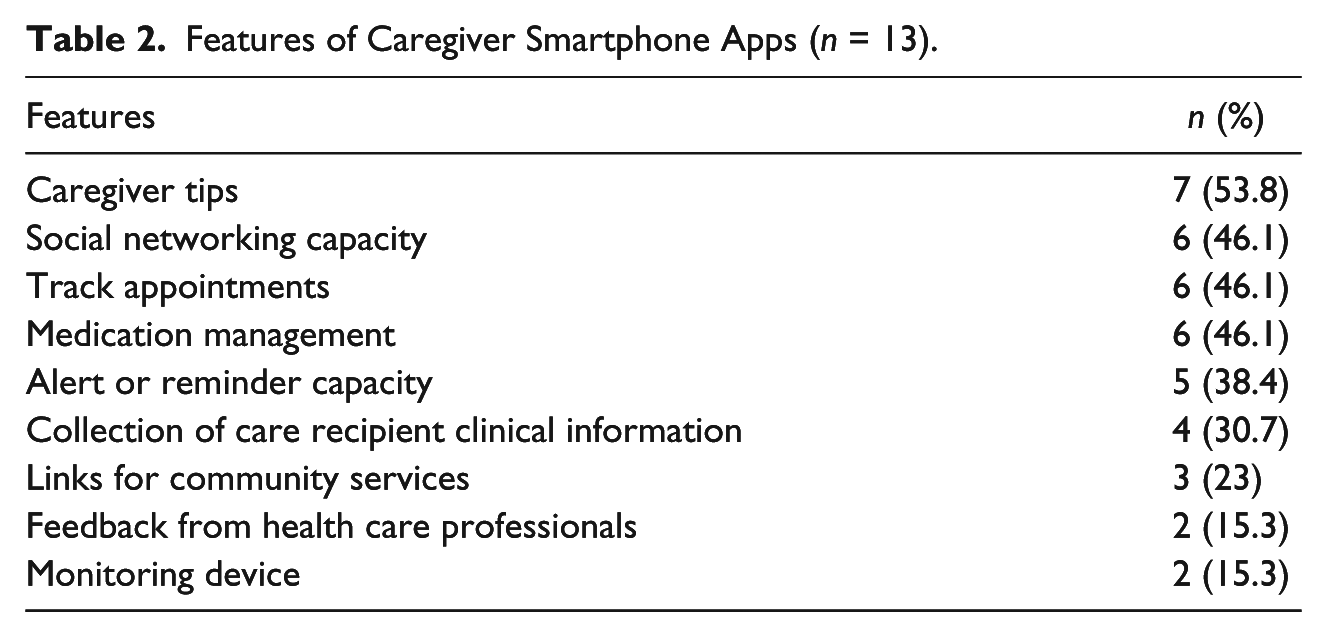
On average, each app had 3.07 features (SD = 1.18) with a range of 1 to 5 features. Table 2 provides the number and percentage of features for the 13 apps reviewed. The most common feature was caregiver tips. Only two apps interfaced with wearable devices to monitor the care recipient sleep, position, or activities. In addition, only two apps provide feedback from clinicians or dementia care experts. In one case, this feedback is through a Help Line (i.e., a link a phone number) and the other through an algorithm. The Help Line resources were provided through a nonprofit association. This type of free resource most often includes live 24/7 assistance by individuals trained to respond to questions about dementia, services, and resources. In the second case, an algorithm automatically generates a response without interaction with a live provider. To use this resource, the caregiver is required to select from a list of “common concerns” when caring for a person with dementia.
Features of Caregiver Smartphone Apps (n = 13).
Readability of Smartphone Apps
The text on 12 app website pages was available and analyzed for readability. Most of the websites (n = 4) were readable by persons in the eighth grade with an overall mean of 8.25 (SD = 3.38). The other websites were readable by persons in the ninth grade (n = 2), fifth grade (n = 2), 17th grade (n = 1), 11th grade (n = 1), seventh grade (n = 1), and fourth grade (n = 1).
MARS Assessment
A MARS assessment was completed for each app and the averages and standard deviations were generated for each domain of the measure. The mean for Overall Quality was 3.61 (SD = 0.91), the mean for Engagement Score was 2.7 (SD = 0.91), the mean for Functionality Score was 4.2 (SD = 1.22), the mean for Aesthetics Score was 3.7 (SD = 1.06), and the mean for Information Quality Score was 3.7 (SD = 1.05).
Discussion
AD caregiving is often complex and involves a number of challenges for AD caregivers. However, the primary finding from this study was that most smartphone apps available for AD caregivers have limited features and do not provide the multiple features required to meet the complex needs of AD caregivers (AARP, 2016). Caregiver Tips was the most common smartphone app feature identified. This was not surprising as providing information about AD and caregiving is consistent with many caregiver interventions and the self-identified need of caregivers for information and knowledge (McCabe et al., 2016). A 2016 Florida state survey reported 10% of all Florida caregivers, and 21% of a minority population subsample, were interested in specifically receiving caregiver information and training (Florida Department of Elder Affairs, 2016). It should not be interpreted that the more features an AD caregiving app has, the better quality it is. Although, the more functions an app has, the more likely an AD caregiver can address complex, multiple, and changing caregiving needs with a single app, rather than rely on numerous apps with varying features.
In addition, the results from the MARS assessment indicated that overall, the currently available AD caregiver apps are acceptable in quality, but their ratings for engagement are poor-to-acceptable. This has troubling practical and clinical implications. An app with limited or uninteresting features or limitations to interactivity and customization may be less likely used. If AD caregivers do not express enthusiasm about the use of smartphone apps, clinicians may be reluctant to use apps as a component of care management. In addition, the MARS items for information quality are not specific to dementia, and none of the apps provided evidence of usability or impact of use. Therefore, it is unclear whether AD caregivers would find the existing information and features to be appropriate to integrate into dementia care management (i.e., caregiver support and information). Further research with outcome evidence is needed.
A Need for Culturally Competent Apps
A second finding from this study was that none of the 13 smartphone apps reviewed offered a Spanish language option, and few were available in languages other than English. This is problematic for a number of reasons. AD impacts Hispanics disproportionately (Alzheimer’s Association, 2017; Amatniek et al., 2006; James et al., 2014), and English proficiency remains a problem for a large proportion of foreign-born Hispanics (Pew Research Center, 2013). At the same time, Hispanics are more likely than other ethnic groups to rely only on a smart device for computer access (File & Ryan, 2014). Also, a recent Nielsen Company (2015) survey found that Hispanics use their smart mobile phones more than any other ethnic group, with bilingual and Spanish-only speaking Hispanics using their phones the most. Unfortunately, Hispanics have historically been categorized as being “digitally underserved” compared with non-Hispanic Whites, in accessing digital health-related information (Lorence & Park, 2008). Victorson et al. (2014) emphasized the need for e-health interventions that are culturally competent for Hispanic users, but caution that cultural competence for Hispanics encompasses more than just English to Spanish translation. In addition to language, specific technology needs have been identified for this population that include considerations of: acculturation status and nationality, cultural beliefs about illness and gender, preferences for physicians as messengers of health information, and the role of family and religion. Developers of culturally sensitive caregiver apps should consider including representative persons in development work and “taking in account differences in age, gender, culture, ethnicity, knowledge, and literacy” (Szczerba, 2014, para 4).
The Need to Integrate AD Apps Into Clinical Care
Another notable finding is that none of the available apps connect AD caregivers with care recipients’ providers. As stated earlier, there is evidence that PCPs do not feel prepared to provide AD care and face barriers to communicating with patients, caregivers, and other providers to gather information for clinical decision making. Smartphone apps and smartphone technology provide the ability to collect and organize information and promote true family-centered care by facilitating shared information and decision making between providers and caregivers. Unfortunately, searches on Medline and other databases suggest that although existing AD caregiver apps have undergone basic testing (Stucki et al., 2014; Thorpe et al., 2016), they have not been integrated into care delivery or existing electronic health record systems. Therefore, it is unknown if improved health care delivery efficiency or outcomes are possible by linking caregivers and providers through such technology. Smartphone app features that promote family-centered care by actively involving the caregiver in care planning should be considered. In a related issue, most of the caregiver apps did not provide the ability for the caregiver to observe and document symptoms with a valid measure. For example, one app provided a measure of mood that lacks established, validated properties. Use of established reliable and valid measurement tools embedded within apps should be considered to assist health care providers in making clinical decisions. Foreseeable barriers to developing and promoting such features include the fact that there is currently no model for reimbursement for this adjunct to care delivery, and health care providers may be concerned about security of patient information and related liabilities for advising patients or caregivers to use the Internet and/or smartphone apps for patient care.
Supporting Varying Levels of Literacy and Computer Literacy
For apps to be accessible and usable by caregivers, they must be designed with users’ literacy in mind. According to Centers for Medicare & Medicaid Services (CMS; 2010), if the readability of text is at ninth grade or greater, half of population will have difficultly reading words, sentences, and materials. This study found that for most of the webpages associated with the included apps (eight out of 12), the text describing the app features and navigation would be interpreted as “average difficulty” or easier using readability scoring. However, reading level score does not guarantee understanding, and the text may not be culturally appropriate, the usefulness of the material may be unclear, or the text may not hold the reader’s interest (Centers for Disease Control and Prevention [CDC], 2009; CMS, 2010). Readability assessments should be considered for webpages associated with apps as well as part of an overall assessment. However, the use of titles, headings, and bullet points (i.e., not full sentences) within apps would provide invalid results for computer-based readability assessments (CMS, 2010). Unfortunately, there are no standard measures to quantify the ease of use of an app user interface, except through user studies. There is currently a dearth of both user feasibility studies and subsequent impact studies for caregiver apps, and therefore, clinicians may be hesitant to incorporate this health technology into care deliver.
There are many other factors that can impact how written content is received and understood. Text appearance (font size, colors, layout of information) should be considered in developing health education materials, and visual images can improve understanding. Cultural or the ethnic norms can affect how information is received and interpreted (CDC, 2009), and appropriate language translation and back translation are needed to ensure quality of translation. Translation procedures need to take into account that subgroups of minority populations may differ, for example, “Mexican Americans . . . may respond differently than Cuban Americans to certain words, colors, and symbols” (CDC, 2009, p. 25).
Funding and the Future of AD Smartphone Apps
Although the need for health technology (i.e., electronic medical records) to improve the safety and efficiency of health care delivery has been identified, funding to develop smartphone apps may not be readily available. Most of the apps were developed in the private sector and only one of app was developed by a government entity (outside the United States). A reason for a lack of academic involvement in app development may in part be due to the small amount of funding available for translational research activities in this area (Gitlin et al., 2015). Policy makers deciding about AD caregiver intervention research funding should consider that 71% of caregivers are interested in technology to support their caregiving tasks and specifically are interested in sensors, notifications, and health monitoring (AARP, 2016).
Limitations
A limitation of this study is that although the investigators were able to determine if “Caregiver Tips” and “Social Networking Capacity” were present, the investigators did not assess if the information provided through these apps was reliable. Caregiver-related online forums and the information exchanges were not critically analyzed. Future research is planned to examine the value of the information exchanged. Furthermore, a second limitation of this study was that the MARS assessment did not include the following criteria: the frequency and date of latest update, presence of sponsor (e.g., pharmaceutical company), and declaration of conflict of interest (Zhang, Ho, Hawa, & Sockalingam, 2016). A third limitation is the eligibility criteria that the apps be in English. It is assumed but unknown if apps are available in other languages (not English), therefore, would not be identified in this review. However, this review did not identify apps in Spanish which is a concern. Finally, there may be smartphone apps that were not identified in this review. However, two investigators conducted searches independently, and it is unlikely that AD caregivers looking for an app would find one that our extensive search did not locate.
Conclusion
In conclusion, smartphone app innovators and researchers should consider developing apps (i.e., both Android and IOS platforms) that are multifunctional, culturally sensitive to minority populations, easy to read and use, and facilitate sharing information within families and between providers and AD caregivers. Given the growing number of AD caregivers and their interest in using technology, funding agencies and foundations should consider expanding available resources. Research is needed to assess the feasibility and potential of integrating apps seamlessly into health care delivery and assessing the impact of their use on caregivers’ emotional health and well-being and on care recipient outcomes. Furthermore, once developed, smart phone-based apps are inexpensive to implement and, therefore, offer great potential to provide a sustainable, low cost approach to provide information and support for caregivers confronted with the responsibilities of caring for a loved one afflicted with AD.
Footnotes
Acknowledgements
The researchers would like to thank Pooja Remanan and Reeta Kumari for their assistance and technical support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.