
Abstract
Older adults frequently experience adverse consequences as the result of unmet care needs, including not getting dressed and going without food when hungry. Previous studies have noted that characteristics of the caregiver network may be associated with unmet needs. Using National Health and Aging Trends Study data, I modeled the association between care configurations and unmet needs for men and women. In generalized linear models, formal care was not associated with unmet need among women or men. Compared with recipients of spousal care, men receiving care from one nonspousal caregiver, and men and women receiving care from any other configuration, had higher odds of unmet needs. The level of difficulty with daily tasks was strongly associated with unmet needs. These findings support monitoring older adults not receiving spousal care, increasing access to formal care, and regularly assessing level of difficulty with daily tasks in clinical and research settings.
Introduction
During the aging process, the accumulation of cognitive and physical limitations can make it difficult to independently complete tasks such as preparing meals, getting dressed, or getting around inside and outside the home. To carry out these important daily functions, older adults in the United States rely primarily on unpaid assistance from family and friends (Gibson & Houser, 2007; Hagen, 2013). A number of trends, however, threaten older adults’ continued reliance on this source of care, including labor force participation, fertility rates, divorce, and geographic mobility. These trends suggest that there will be fewer potential informal caregivers relative to care recipients, and also that these potential caregivers will face more competing demands on their time than caregivers in previous generations (Wolff & Kasper, 2006). In addition, the care needs of community-residing individuals, particularly those who might have been candidates for nursing home placement in the past, have increased. Not only do older adults require more assistance to remain in their homes, that assistance is also increasingly complex due to advances in medical care. For example, today’s caregivers manage a large number of medications and provide a great deal of wound care to their care recipients (Reinhard, Levine, & Samis, 2012). In sum, family and friend caregivers will need additional support to continue meeting the needs of an aging population (Miller, Allen, & Mor, 2008).
Given the potential strain on older adults’ caregiver networks, the concern that older adults might not obtain necessary daily assistance has received substantial attention. The absence of needed assistance is known as unmet care need, or simply unmet need. One study found that 32% of older adults who have difficulty with or receive help performing daily activities have recently experienced negative consequences (e.g., not getting dressed, going without food when hungry) directly related to unmet needs (Freedman, Spillman, & Kasper, 2014). The prevalence of such consequences is even greater among certain high-risk groups, such as those who are eligible for both Medicare and Medicaid (Allen, Piette, & Mor, 2014). In addition to these direct consequences, unmet needs have also been linked to other adverse outcomes, including a heightened risk of falls (Allen & Mor, 1997; LaPlante, Kaye, Kang, & Harrington, 2004), emergency department visits (Hass, DePalma, Craig, Xu, & Sands, 2015), hospital readmission (DePalma et al., 2013), nursing home placement, and death (Gaugler, Kane, Kane, & Newcomer, 2005).
Older adults’ caregiving networks differ along important dimensions, including size, relationship, age, gender, and proximity of their members (Fast, Keating, Otfinowski, & Derksen, 2004; Fiori, Smith, & Antonucci, 2007; Keating & Dosman, 2009), and these networks may be related to unmet needs. Previous studies that have investigated the relationship between these care configurations, as I will call them here, and unmet needs have not reached consensus. For example, indicators of inadequate informal care access, such as living alone, have been associated with a greater likelihood of unmet need (Desai, Lentzner, & Weeks, 2001; LaPlante et al., 2004), but other studies have found that unmet need is higher among informal care recipients than among formal care recipients (Rogero-García & Ahmed-Mohamed, 2014). Receiving formal care after a hospital discharge has been associated with better recovery of functional capacity (Arbaje et al., 2008; Penrod, Kane, Finch, & Kane, 1998), and improved capacity should logically reduce the need for care. Receiving inadequate care has been associated with a high level of functional limitation, whereas access to formal and informal care, including unmarried status, fewer family members, and lack of insurance, is associated with the receipt of no care (Lima & Allen, 2001).
Sex has also been considered as a predictor of unmet need. Although findings have not been consistent (Kennedy, 2001), many studies have shown that women were more likely than men to report unmet need (LaPlante et al., 2004; Li, Kyrouac, McManus, Cranston, & Hughes, 2012). It has been further hypothesized that the predictors of unmet need differ for men and women, because women are theoretically more likely to have been socialized into a caregiving role (Rosenthal, 1985), and may be more able to perform that role for their husbands than their husbands can for them (Allen, 1994; Lima & Allen, 2001). Therefore, spousal care might be more beneficial for men than for women. Despite its theoretical and intuitive appeal, empirical studies of this hypothesis have been limited. Two decades ago, Allen (1994) found no difference in the unmet personal care needs of married men and married women in a relatively small sample of patients undergoing treatment for cancer in three Northeastern states. In a larger study of a nationally representative sample, Lima and Allen (2001) found no significant interactions involving sex when modeling unmet needs.
These older studies remain influential, and this exact hypothesis has not received much attention since then. However, a growing body of research has continued to document differences in the way male and female caregivers approach their roles, including differences in male caregivers’ help-seeking behaviors, in the hours of care they provide, and in their tendency to relinquish a caregiving role more quickly than women (Allen, Lima, Goldscheider, & Roy, 2012; Baker & Robertson, 2008; Daire, Torres, & Edwards, 2009). This would seem to suggest that older women and older men may not receive the same benefit from spousal care, for example. This is difficult to reconcile with the earlier finding that the predictors of unmet need are the same for men and women. It is, therefore, worth reexamining the possibility that the relationship between care configurations and unmet need differs for men and women.
Conceptual Framework
Andersen’s behavioral model of health service utilization (Aday & Andersen, 1974; Andersen, 1968, 1995; Andersen & Newman, 1973) posits that the use of health services results from three types of characteristics: predisposing, enabling, and need. Predisposing characteristics include those characteristics that predispose an individual to seek care, enabling characteristics are those resources that are necessary to obtaining desired care, and need characteristics are those characteristics, including health conditions and functional limitations, which create a need for care. Here, my focus is on care configurations, an enabling factor, and, therefore, it is also important to account for factors that may predispose a care recipient to seek greater services (e.g., age, education), as well as need factors (e.g., health and function, cognitive impairment).
Viewed within the framework of the behavioral model, Litwak’s (1985) task-specificity model and Cantor’s (1979) hierarchical-compensatory model of caregiving both focus on enabling characteristics. However, these two models lead to conflicting predictions about the relationship between care configurations and unmet need. The task-specificity model suggests that different caregivers, based on their characteristics, might be well suited to different types of assistance. In this model, one would expect a relationship between care configurations and unmet need if there is a mismatch between the attributes of available caregivers and the needs of care recipients.
In contrast, the hierarchical-compensatory model suggests that caregivers are, to some extent, interchangeable. This model emphasizes that caregiving is the result of a commonly understood hierarchy of caregivers, typically beginning with the care recipient’s spouse, followed by the care recipient’s children, then by other relatives, and finally friends and neighbors. If care is not provided by a relative near the top of the hierarchy, then others are likely to step in. In this theoretical model, there should be little or no relationship between the care configurations and unmet needs, because caregivers step forward to provide care precisely for the purpose of meeting care-recipient needs that are not being met by other potential caregivers. By testing the hypotheses stated below, I also produced evidence of the relative value of these two theories of caregiving.
Research Question
Using newer data and a nationally representative sample of older adults, I aimed to determine whether care configurations were associated with unmet needs, and whether that association was moderated by sex. Previous research on caregiving networks has identified dimensions that distinguish caregiving networks, including gender, relationship, size, age, and proximity (Fast et al., 2004; Fiori et al., 2007; Keating & Dosman, 2009). I focused on the first two of these variables, to test the hypotheses that informal care would benefit men and women differently, and that spousal care would benefit men more than women. I hypothesized that some care configurations would be associated with higher probabilities of unmet needs than others. However, the direction of the association was theoretically ambiguous, given that informal care might be more effective at reducing unmet need in older adults with frequent, but straightforward care needs, whereas formal care might be helpful in reducing unmet needs for medically complex care recipients. Because previous evidence suggested that male caregivers, who are often spouses, are reticent to seek needed help and feel less comfortable in their role than female caregivers, I further hypothesized that men would benefit more from informal care provided by spouses, but that women might benefit more from formal care, and from nonspousal informal care.
Method
Data
I used data from the first four waves of the National Health and Aging Trends Study (NHATS) public use data. NHATS is sponsored by the National Institute on Aging through a cooperative agreement with the Johns Hopkins Bloomberg School of Public Health (NIA U01AG032947). NHATS is an annual survey of a nationally representative sample of Medicare beneficiaries above age 65, beginning with 8,245 participants in 2011. Among the advantages of NHATS for this study are its detailed questions on participants’ functioning, the in-depth information it provides on potential informal caregivers, and the number of annual follow-ups.
Sample
Table 1 demonstrates how the analytic sample was derived from the full NHATS sample. I restricted the sample to individuals reporting difficulty with at least one self-care and/or mobility task; by definition, individuals with no such difficulties do not have unmet needs and, therefore, are not “at risk” of the outcomes. In addition, noting Lima and Allen’s (2001) observation that the determinants of no care are meaningfully different from the determinants of inadequate care, and observing that the vast majority of individuals reporting unmet needs were receiving some care, I excluded individuals receiving no care for any activity in which they were limited. It is worth noting that this decision limits the extension of my findings to some groups of older adults at risk of unmet need, such as older adults who live alone (LaPlante et al., 2004). Similarly, I included only community-residing individuals because the predictors of unmet need in a nursing home or other residential care setting are likely to be quite different than predictors of unmet need for community residents. To evaluate my hypothesis that different factors were associated with unmet needs in men and women, I stratified the sample by sex for all analyses.
Derivation of the Analytic Sample.
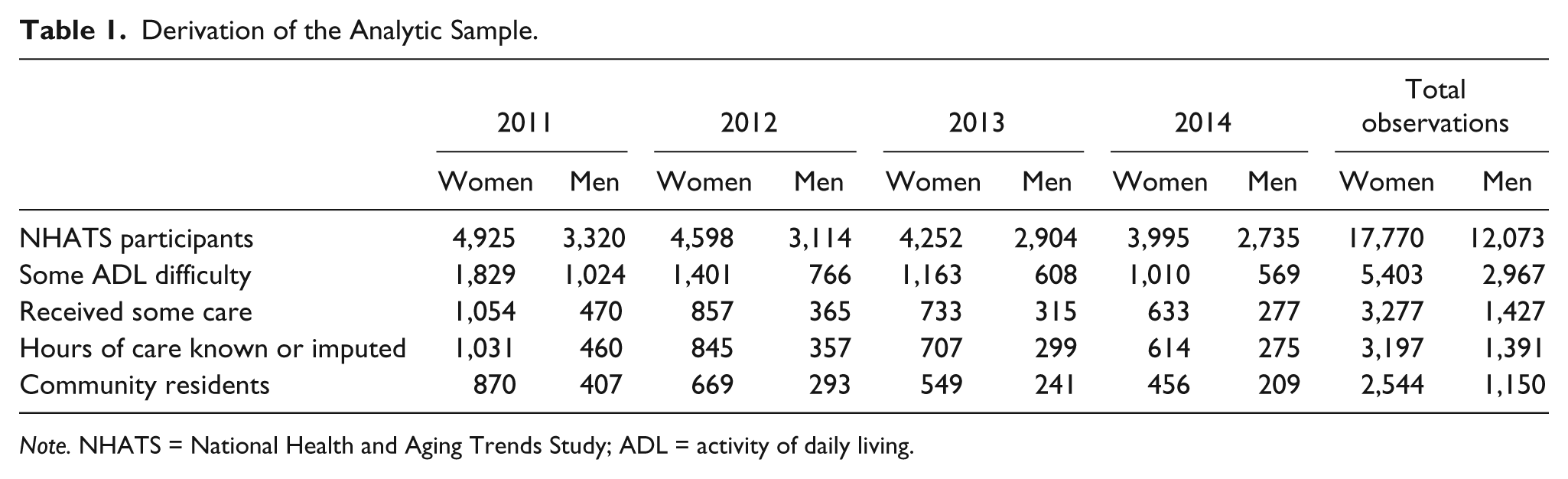
Note. NHATS = National Health and Aging Trends Study; ADL = activity of daily living.
Primary Outcome
Unmet need was defined as an NHATS respondent’s experiencing an adverse consequence relating to his or her inability to perform a task when help was unavailable. NHATS respondents reported their level of difficulty performing four self-care tasks (bathing, dressing, eating, and toileting), as well as three mobility tasks (going outside, getting around inside, and getting out of bed). Respondents who reported any difficulty with a task were then asked whether they experienced a consequence related to their inability to perform that task when help was unavailable. I excluded the question on getting around outside because it is the only one of the seven questions to focus on tasks that require leaving the home, and is far more subject to environmental and climactic variations that could complicate the relationship between the availability of care and older adults’ ability to perform this task. Also, early results including this item were highly suggestive of reverse causality (i.e., more hours of care was associated with higher risk of unmet need). Participants were considered to have unmet need for assistance if they reported that they did not conduct one or more of the remaining six activities at any time in the past month, either due to lack of assistance or, for those who did not receive any assistance, because it was too difficult.
Focal Predictors
The key independent variables were indicators for each of several care configurations. In addition to gender and caregiver relationship, it was important to consider the size of caregiver networks because women and men are not equally likely to have large caregiver networks (Cornwell, 2011), and therefore, this could bias any attempt to distinguish predictors of unmet need in men and women. Caregiver age and proximity were not included in the model because, in this sample of adults above age 65, caregiver age was highly collinear with their relationship to the care recipient, and because a measure of proximity was not available in the data.
Therefore, I used two sets of care configurations to conduct the analyses presented here. The first set of care configurations was very simple, consisting of an indicator of whether an older adult had multiple caregivers and a continuous variable consisting of the percent of care provided by formal caregivers. I categorized caregivers as “informal” if they were identified by the NHATS participant as having some type of relationship other than simply a caregiving relationship, 1 and categorized caregivers as “formal” if they were identified as paid aide/housekeeper/employees, staff person at the place the participant lives, or any other nonrelative who was paid for providing care.
The second set of care configurations accounted for the unique role of spouses as default caregivers for married older adults. Therefore, this set of care configurations did not distinguish between formal and informal care, but rather between spousal and nonspousal care. By combining this distinction with the distinction between networks with one caregiver and those with multiple caregivers, I obtained indicators for each of the following care configurations: one spousal caregiver, one nonspousal caregiver, a spouse and other caregivers, and multiple nonspousal caregivers.
Covariates
I adjusted for predisposing and need characteristics that might confound the relationship between care configurations and unmet need. Predisposing characteristics included several demographic variables that predispose care recipients toward certain care configurations (age category, sex, race/ethnicity, and educational attainment). Due to sample size and a relatively high amount of missing data, the race/ethnicity categories were collapsed to Black, White, Hispanic, and Other.
To adjust for need characteristics, I developed several measures of care recipients’ health and function. I categorized activity limitations by the level of difficulty reported by NHATS participants. This resulted in four counts of activity limitations—a count of activities with which an individual reported “a lot” of difficulty, “some” difficulty, “a little” difficulty, and activities the participant had not completed by herself or himself in the past month. I also created an indicator for each of the nine health conditions about which NHATS participants are asked: heart attack, heart disease, high blood pressure, arthritis, osteoporosis, diabetes, lung disease, stroke, and cancer. To identify individuals with probable dementia, I used an NHATS-provided computer program for classifying individuals’ cognitive functioning based on proxy responses and participants’ performance on cognitive assessment tests (Skehan & Spillman, 2013). I also included indicators for fair or poor self-rated health.
Finally, I adjusted for hours of care. This variable was derived from NHATS participants’ responses to questions on each helper’s number of days per week or per month, and the number of helping hours per day of help, using NHATS software that estimates monthly hours of care and imputes a small number of missing values, based on responses about the hours of care provided per day of help, days of help per week or per month, and other characteristics of the care provided (Freedman et al., 2014). I created five categories for the hours of care provided per month to roughly approximate quintiles of hours of care.
Statistical Analysis
To address the questions of whether care configurations and unmet needs were associated, and whether that association differed for men and women, I modeled the likelihood of unmet need using a generalized linear model with a logit link. I used generalized estimating equations to account for multiple observations of the same individual in different years. I modeled the association between care configurations and unmet needs, stratifying my analysis by sex, and testing for statistically significant differences between the parameters resulting from models that included only men, and those including only women. To reduce the possibility that other predisposing and need characteristics might confound these results, I adjusted for care recipients’ level of difficulty with self-care and mobility tasks, for the demographic and health covariates described above, and for hours of care. In sensitivity analysis, I excluded hours of care as a covariate, but the results did not change. I repeated this analysis using each set of care configurations described above. Analyses were weighted for the complex survey design of NHATS and for nonresponse bias (Montaquila, Freedman, Spillman, & Kasper, 2012).
All analyses were conducted using Stata 13.0 (StataCorp, College Station, TX). The University of Iowa Institutional Review Board determined that this research, which consists entirely of secondary analyses of a deidentified, publicly available data set, did not constitute human subjects research (IRB ID 201510799).
Results
Table 2 displays characteristics of the analytic sample, stratified by sex and comparing observations in which unmet need is reported with those in which no unmet need is reported. Because I combined 4 years of observations to generate these descriptive statistics, individuals could contribute up to four observations each to the analysis, although observations were only included as long as the individual was alive and met the other criteria for inclusion in the sample. Individuals with unmet needs were more likely to have multiple caregivers than those without unmet needs, and received more hours of care per month. This was true for both men and women, but men were more likely to receive care from a single informal caregiver than women, regardless of unmet needs. Differences in the demographics of those with unmet needs did not follow any consistent pattern, with Hispanic women composing a large share of the women with unmet needs, whereas Black men were overrepresented among men with unmet needs. The age distribution of participants with unmet needs was not different from the age distribution of those without unmet needs. As expected, men and women with unmet needs had poorer health and functioning, reported more self-care and mobility difficulties, lower self-rated health, and were more likely to be classified as having probable dementia. Women with unmet needs had higher prevalence of lung disease and stroke than women without unmet needs, whereas men with unmet need displayed higher prevalence of heart disease, high blood pressure, and stroke.
Characteristics of the Analytic Sample.
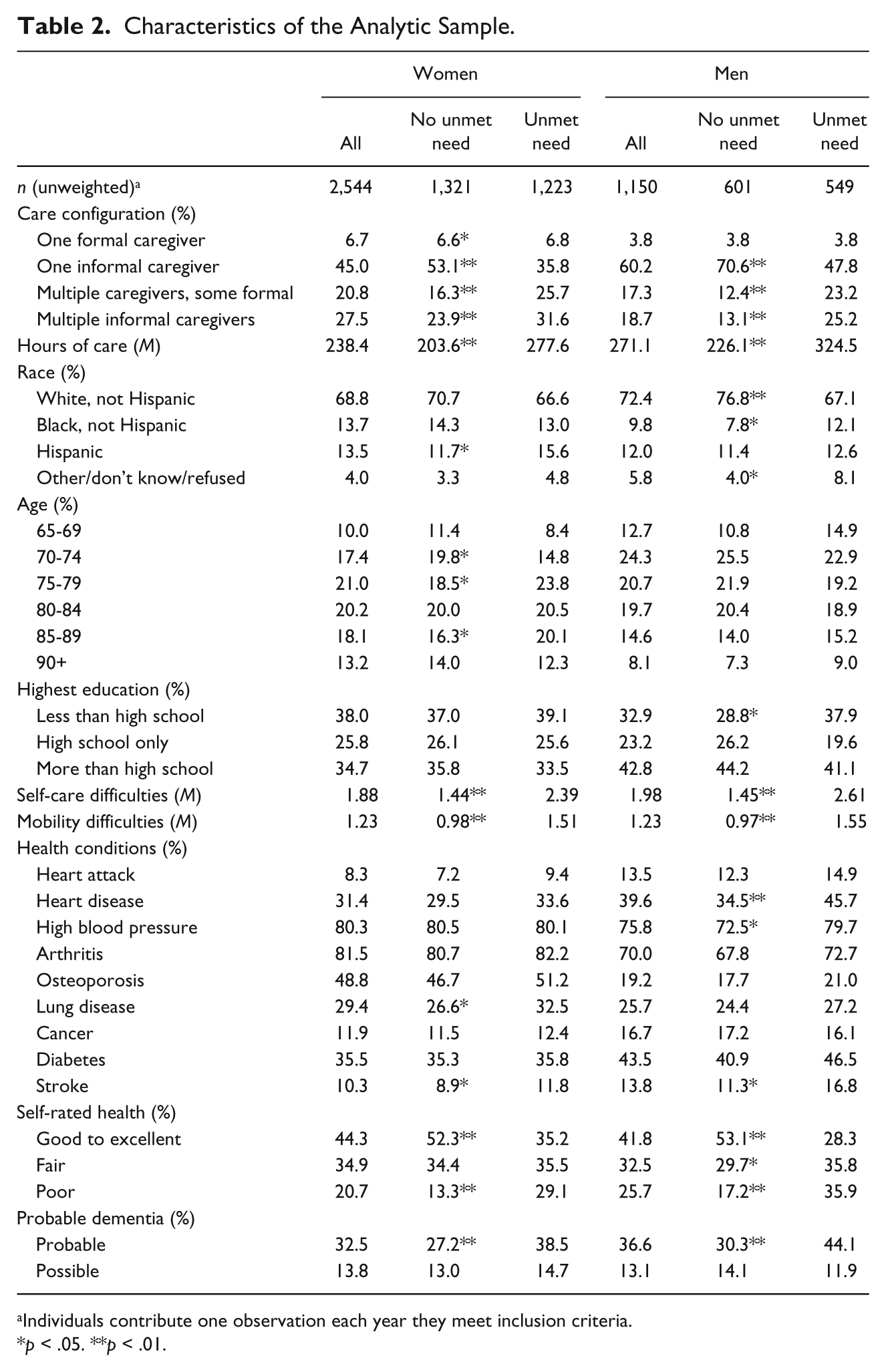
Individuals contribute one observation each year they meet inclusion criteria.
p < .05. **p < .01.
Table 3 shows the adjusted odds ratios obtained from generalized linear models that measure the association between simple care configurations and unmet needs in women and men. Multiple caregivers are associated with higher levels of unmet needs. The percentage of care provided by formal caregivers is not associated with unmet needs, for either men or women. The level of activity of daily living (ADL) difficulty is a very strong predictor of unmet needs for both men and women. There may be a trend toward lower levels of unmet need in older men that is not apparent in older women. There is heterogeneity in the association between unmet needs and race/ethnicity and education in men and women. Specifically, there is a more negative association between being Black and having unmet needs, and a more negative association between having less than a high school education and unmet needs, for women than for men. Men with more than a high school education are also more likely to have unmet needs, unlike women with the same educational attainment. Finally, fair or poor self-rated health is a predictor of unmet needs.
Adjusted Odds Ratios From the Generalized Linear Models of Unmet Needs on Care Configuration and the Percent of Care Provided by Formal Caregivers, by Sex.
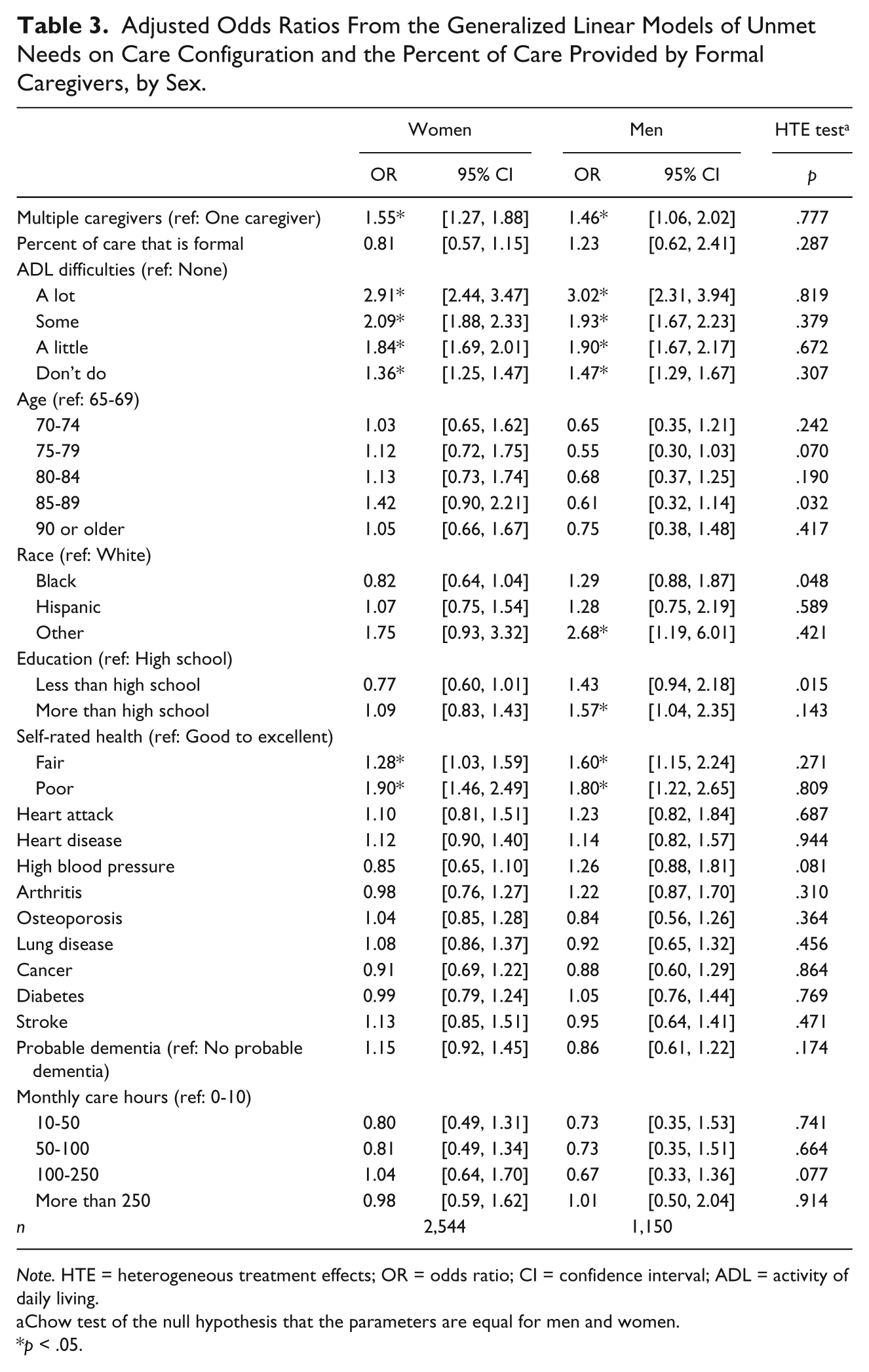
Note. HTE = heterogeneous treatment effects; OR = odds ratio; CI = confidence interval; ADL = activity of daily living.
Chow test of the null hypothesis that the parameters are equal for men and women.
p < .05.
Table 4 presents the results of a similar model, but with care configurations coded to compare spousal with nonspousal caregiving. Men receiving care from a caregiver other than their spouse have 1.96 times the odds of unmet needs as those who receive care from a spouse. Although there is no similar difference in women’s unmet needs when care is provided by a single nonspousal caregiver as opposed to a spouse, the Chow test for the difference between the coefficients for men and women is not statistically significant (p = .128). The parameter estimates for other care configurations do not have statistically significant differences for men and women, but it is worth noting that all other care configurations are associated with higher unmet need than spousal care, regardless of the sex of the care recipient. The fully adjusted estimates for other variables are very similar to the estimates shown in Table 3.
Adjusted Odds Ratios From the Generalized Linear Models of Unmet Needs on Spousal and Nonspousal Care Configurations.
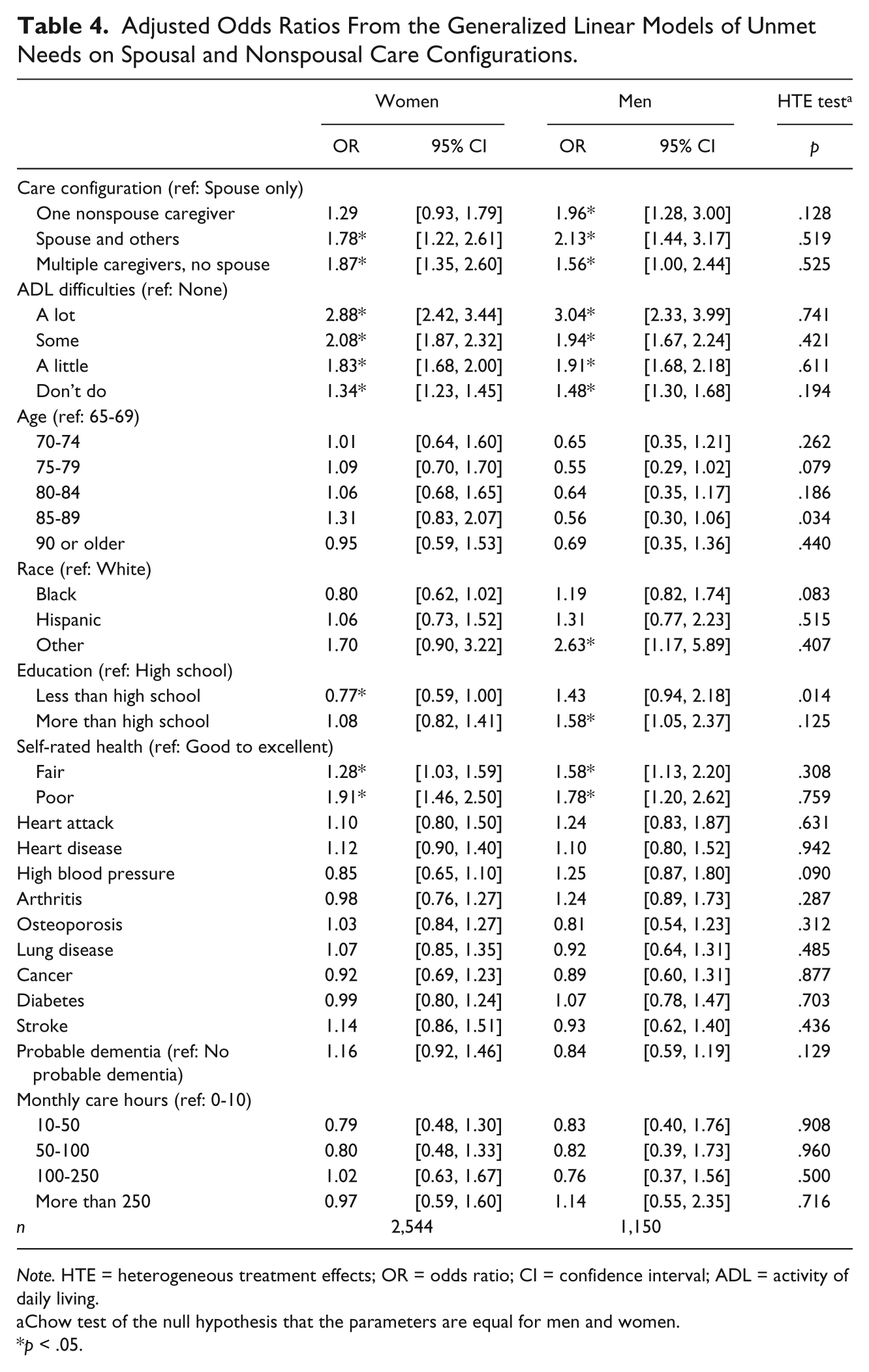
Note. HTE = heterogeneous treatment effects; OR = odds ratio; CI = confidence interval; ADL = activity of daily living.
Chow test of the null hypothesis that the parameters are equal for men and women.
p < .05.
Discussion
This analysis updates and expands previous research considering whether unmet needs are associated with different factors for women than for men. I benefited from the use of a large, nationally representative sample of Medicare beneficiaries above age 65. In addition, the NHATS data include unusually detailed questions about older adults’ caregiving environment and level of difficulty faced by participants in conducting self-care and mobility activities. This permitted me to effectively adjust for important potential confounders in regression models.
I found only limited evidence that sex moderates the relationship between care configurations and unmet needs. Formal care was not associated with significantly lower risk of unmet need in either men or women, and there was no significant difference between men and women in spousal care’s association with unmet needs. However, some demographic predictors of unmet need differed for men and women, including age and race. It should be noted that these results are generalizable to older adults receiving some care, but not to those who receive no caregiving assistance at all. Also, unmarried individuals cannot avail themselves of spousal care, so the applicability of the findings on spousal care is limited with respect to unmarried, widowed, or divorced older adults.
Older women are seemingly at greater risk of experiencing unmet need than older men (LaPlante et al., 2004). Women who need care tend to be older, have fewer financial resources at their disposal, and are more likely to be widowed than men receiving care. It has been previously theorized that older men are generally not socialized into taking on a caregiving role, and do so only reluctantly. In this case, they may also perform poorly, possibly suggesting that there would be value in developing support services and outreach strategies targeted to male caregivers. To the extent that older women in this study appeared to benefit from receiving spousal care as much as older men, my results are not consistent with this hypothesis. My finding that there are no differences in unmet needs between men and women receiving spousal care from 2011 to 2014 is consistent with other research that has shown no difference in the quality of care provided by sons compared with that provided by daughters (Van Houtven & Norton, 2008). Although the earlier study’s findings could result from the fact that sons and daughters self-select into elder caregiving based on their preparedness for the task, this selection is less common for spouses, who serve as on-site caregivers by default, and thus, self-selection is less likely to explain the results presented here. Notwithstanding the apparent similarity in quality of care, other disparities may exist nonetheless; for example, descriptive results consistently show that daughters continue to provide several times more caregiving than sons (Van Houtven & Norton, 2008; Wolff & Kasper, 2006), and Allen et al. (2012) found that sons were more likely to transition out of a caregiving role than daughters.
For both men and women, receiving care from a spouse was the care configuration associated with the smallest risk of unmet needs. One implication is that health professionals and policy makers should recognize the risk that older adults who do not receive care from a spouse will have unmet needs, and that it may be necessary to monitor such individuals more frequently to prevent undesirable consequences. Increasing access to formal care may be a particularly valuable intervention, and my findings indicate that those older adults who rely more heavily on formal care are not at greater risk of unmet needs.
This analysis provides some evidence in support of Litwak’s task-specificity theory. With only one exception (women receiving care from one nonspousal caregiver), both men and women were less likely to have unmet needs when receiving care from care from a spouse, compared with those receiving care from any other care configuration. This suggests that spousal caregivers are not easily replaced by other caregivers, in contrast to what Cantor’s hierarchical-compensatory theory might predict. In future research that explores the competing implications of Litwak’s and Cantor’s models, it may be valuable to recall that men’s and women’s networks of potential caregivers are not always constructed through similar processes, and therefore, a care recipient’s sex may be related to the caregiver network’s tendency to behave more or less like a hierarchy.
Finally, there was a very strong relationship between the level of difficulty reported on self-care and mobility tasks and the probability of unmet need. This is generally consistent with a tendency in previous studies for need variables to be most predictive, a trend which Andersen himself has noted (Andersen, 1995). Previous analyses have generally relied on binary indicators of ADL difficulty, rather than a measure of the level of difficulty; with the more detailed information provided by NHATS participants, my analyses suggest that the level of difficulty has additional explanatory power. This finding suggests that severity of need should be regularly collected when attempting to assess or study unmet needs. It may also be valuable to develop enhanced measures of unmet needs that better characterize severity of unmet need. Moreover, although much of the literature on unmet needs has focused on predicting unmet need using measures of access to formal and informal care, this finding implies that the concept of unmet need may be simpler. Researchers should carefully consider the possibility that unmet need may be a better measure of care recipients’ needs than of caregivers’ success in meeting those needs. Future research to quantify the percentage of variation that can be explained by need alone would be useful in disentangling the contributions of care-recipient need and adequate caregiving. Such studies might involve comparisons across multiple data sets, to test whether the predictive value of need variables depends on how unmet need is measured.
Limitations
The primary limitations in this descriptive study are the possibility of unobserved confounding and reverse causality. In particular, although I have included several measures of care recipients’ health status, it remains possible that unobserved health conditions might be associated with unmet needs as well as older adults’ care configurations. Similarly, unmet needs may trigger a change in care configurations, rather than the other way around. Either possibility would result in a positive association between unmet needs and more intensive care configurations. Indeed, I did find evidence that unmet needs are higher among individuals with multiple caregivers, compared with individuals receiving care from just one caregiver. There is no compelling reason to expect that this confounding, however, would be more or less present for men than for women, and my interpretation is focused on this distinction. In previous studies, family characteristics (e.g., number of daughters, marital status) have served as instrumental variables for informal care (e.g., Van Houtven & Norton, 2008). However, the use of this method requires that the instrumental variable not have an independent effect on the outcome in question. There is reason to doubt that these variables satisfy that criterion with respect to unmet need, because available family members may directly influence unmet need without providing care themselves. I have, therefore, not chosen to use instrumental variables in my analyses.
There are several other potential limitations that I could not fully address in this study. First, the potential for nonrandom measurement error in the self-reported measures used in this analysis is substantial. In particular, NHATS participants’ assessment of the number of hours another person provides care is concerning because the error in these reports may be associated with the configurations themselves. Second, my ability to test for moderating variables (other than sex) and to include all potential confounders has been limited by concerns about sufficient statistical power and multiple hypothesis testing. In particular, I have interpreted the effects of spousal care in conjunction with models that compare formal and informal care; however, marital status alone may have an impact on unmet needs. Because more than 98% of married care recipients received care from a spouse, I was unable to distinguish the effects of spousal care from other possible impacts of being married through sample restrictions or interactions involving marital status and care configuration. Finally, the decision to exclude older adults without a caregiver may lead to bias because women are more likely to have no caregivers as a result of being older and having fewer financial resources than men needing care. Any resulting bias is unlikely to be extensive, however, given that few individuals were excluded on the basis of this criterion.
Conclusion
I found evidence that unmet needs are generally less likely among older adults receiving care from a spouse, but no difference in unmet needs between those receiving more or less formal care and no differences between men and women in the association between care configurations and unmet needs. Health professionals and policy makers seeking to reduce unmet needs should focus on improving the care of older adults who do not receive care from their spouses, and on improving access to formal care as an acceptable substitute for informal care. The level of difficulty performing daily tasks was a strong predictor of unmet needs, and should be measured by clinicians, policy makers, and researchers whenever possible.
Footnotes
Acknowledgements
I am indebted to Fred Wolinsky for his extensive feedback throughout the course of this research. I also wish to thank the other members of my dissertation committee – Kitty Buckwalter, Keith Mueller, Padmaja Ayyagari, and Kanika Arora – for their feedback on an earlier draft.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.