
Abstract
Introduction
Age-related hearing loss is the third most prevalent chronic condition among older adults, affecting more than 120 million people worldwide (Corna, Wade, Streiner, & Cairney, 2009; Li-Korotky, 2012; Strawbridge, Wallhagen, Shema, & Kaplan, 2000). A large proportion of these individuals will have significant losses that result in a hearing impairment. Approximately 65% of Canadians aged 70 years and older have a hearing impairment, with both incidence and prevalence rates rising with each decade of life (Feder, Michaud, Ramage-Morin, McNamee, & Beauregard, 2015).
Despite the widespread prevalence of hearing impairment among older adults, it is often underestimated and unrecognized due to the gradual progression of the disease (Allen et al., 2003; Li-Korotky, 2012). Hearing impairment is known to be correlated with difficulty communicating and interacting with others. Problems maintaining and following conversation may lead to frustration, a loss of self-esteem (Huang & Tang, 2010), depressive symptoms (Gopinath, Hickson, et al., 2012), and the desire to withdraw from social settings (Arlinger, 2003). Other negative outcomes associated with this impairment include difficulty completing activities of daily living (ADLs) and instrumental ADLs (IADLs; Chen et al., 2015; Slaughter, Hopper, Ickert, & Erin, 2014), which can reduce one’s ability to live independently. There is also a growing body of research that suggests that age-related hearing impairment may also be linked to an increased risk of cognitive decline (Lin, Yaffe, et al., 2013). A number of risk factors are associated with age-related hearing loss, including being male (Helzner et al., 2005; Lin, Thorpe, Gordon-Salant, & Ferrucci, 2011), and exposure to occupational noise (Helzner et al., 2005; Palmer et al., 2002). Males are likely at a greater risk of age-related hearing loss due to time spent in a noisy occupation (Palmer et al., 2002). Additional risk factors include increasing age (Cruickshanks et al., 2010; Linssen, van Boxtel, Joore, & Anteunis, 2014) and multiple chronic conditions (Kramer, Kapteyn, Kuik, & Deeg, 2002; Stam et al., 2014). Diabetes, arthritis (other than osteoarthritis and rheumatoid arthritis), and dizziness causing falling are all associated with poor hearing ability (Stam et al., 2014).
The prevalence and incidence rates of hearing impairment have been well documented in the literature; however, there are limited studies that have examined the progression (worsening) of hearing impairment over time. Cruickshanks and colleagues (2003) examined the 5-year prevalence and incidence of hearing loss in a sample of community-dwelling older adults. Approximately 53.3% of those with baseline hearing impairment experienced at least a 5-dB increase in pure-tone average when reexamined at the 5-year follow-up period. Age was the only factor that was found to be related to the progression of hearing impairment over time (Cruickshanks et al., 2003).
It is estimated that between 30% and 60% of older adults living in the community have hearing impairment (Allen et al., 2003; Corna et al., 2009). Many of these individuals will also have multiple chronic health conditions (e.g., hypertension, diabetes, cardiovascular disease, etc.) and require formal home care services. These chronic conditions have been linked with an increased risk of hearing loss in older adults (Helzner et al., 2005; Yamasoba et al., 2013). Home care is an increasingly important part of the publicly funded health care continuum, yet relatively little is known about this population when it comes to hearing health. Currently, in Ontario, roughly 400,000 adults over 65 years of age receive publicly funded home care, with an annual budget of CAN$2.4 billion (Home Care Ontario, 2015; Ministry of Health and Long-Term Care, 2015), and the need for these services is anticipated to increase with population aging (Kadowaki, Wister, Chappell, 2015).
There is little information about older adults living in the community that have a hearing impairment and are receiving home care services. As the need for home care services is continually growing, it becomes vital to learn more about these individuals and how they are functioning in terms of hearing health. The key goals of the current study was to investigate the prevalence of hearing impairment, the potential factors associated with how it progresses over time, and the relationship it has between health and psychosocial well-being in a cohort of older home care recipients. Based on our review of the literature, we anticipated that older adults were more likely to experience a deterioration in hearing over time due to factors such as increasing age, being male, and experiencing cognitive difficulties.
Method and Materials
Data Source
This study utilized secondary data collected on home care clients in Ontario who were assessed with the Resident Assessment Instrument for Home Care (RAI-HC). The RAI-HC is a government-mandated assessment for all long-stay clients in Ontario (clients expected to receive care for over 60 days; Ministry of Health and Long-Term Care, 2006). The assessment is part of a suite of assessment instruments, which are used as a base for care planning, measuring quality issues, and outcomes of care (Hirdes, Freeman, Smith, & Stolee, 2012). Assessments are completed on enrollment and typically every 6 to 12 months thereafter (Hirdes, Poss, Mitchell, Korngut, & Heckman, 2014). The assessment contains just over 300 items covering domains such as cognition, communication, and functional ability. Assessments are completed by trained care coordinators (typically registered nurses) and include information collected from the client, their caregivers, and as needed, consult with other health care professionals, and clinical records (e.g., including medical tests for hearing). Missing data within the RAI-HC are typically nonexistent as care coordinators are not able to close and finish the assessment unless all fields have been completed. We did examine the rate of missing data across all of the variables under consideration, and the amount of missing never exceeded 10%.
Sample
The sample included all Ontario long-stay home care clients aged 65+ years who had at least two assessments completed between 2010 and 2011 (n = 59,188). Assessments chosen for the analysis were completed within 12 months of each other, in keeping with the mandated reassessment interval of 6 to 12 months in Ontario, and represented the two most recent assessments for each unique individual. The data were made available to the research team from the Canadian Institute for Health Information (CIHI) that maintains a database for all RAI-HC assessments completed across Ontario. This time period was chosen because it represented the most recent fiscal year of data available from CIHI when the study began. The Research Ethics Board at Wilfrid Laurier University reviewed and approved the design of this study prior to the researchers being granted access to the data (REB #: 4184).
Measures
Individual items on the RAI-HC have been found to be valid and reliable, with documented evidence of criterion validity (Poss, Jutan, et al., 2008), and good interrater (average kappa = 0.74; Morris, Fries, et al., 1997) and test–retest reliability (Hirdes et al., 2008; Poss, Jutan, et al., 2008). A number of studies have examined the validity of the instrument by evaluating the health index scales that are embedded within the assessment (Landi, Tua, et al., 2003; Morris, Fries, & Morris, 1999).
The main outcome variable of this study was the development of incremental hearing deterioration between a client’s two most recent assessments. Hearing impairment was classified by a single item on the RAI-HC, which scores hearing ability on a 4-point scale with response options of 0 (hears adequately), 1 (minimal difficulty), 2 (hears in special situations only), and 3 (highly impaired). This item has been found to have good interrater reliability (kappa = .83; Guthrie et al., 2011). The care coordinator determines a client’s hearing status based on the combination of self-assessment by the client, information provided by the informal caregiver, consultations with other health care providers (e.g., primary care physician), and review of relevant medical records (e.g., auditory tests, professional assessments). The hearing item on the assessment is capturing not only the perception of how the client feels their hearing is, but also the combined response between the client, informal caregiver, and as necessary, the perspective of other health care providers. If there is a disagreement between how the client and other members of the client’s circle view their hearing status, then a decision will be made by the care coordinator as to the final rating of the client’s hearing status. A difference score was calculated between the two assessments to determine if a deterioration in hearing occurred. A client was classified into one of four categories, which included no deterioration, a 1-point deterioration (e.g., a 1-point increase on the hearing item), 2-point deterioration, or 3-point deterioration. If a client’s score remained the same between the two assessments, regardless of the actual degree of impairment, or if their hearing improved, they were classified as having no deterioration. We conducted preliminary analysis comparing clients who remained the same and clients who improved and found that these two groups were very similar (less than a 10% difference) across several characteristics such as age and sex (data not shown) and therefore we chose to keep them in one group. Within the RAI-HC, there is no information on whether a client owned or regularly used an assistive device such as a hearing aid. However, according to the RAI-HC manual, assessors are instructed to assess hearing with hearing appliances in place, so it is assumed that if the client had a hearing aid, the assessor would complete the assessment once the hearing aid was in place (Morris et al., 2009).
Three variables within the RAI-HC measure communication abilities in relation to hearing status. Expressive communication was measured by a single item on the RAI-HC, which is scored from 0 (understood by others) to 4 (rarely/never understood by others). Similarly, a single item on the assessment was also used to score receptive communication, again ranging from 0 (understands others) to 4 (rarely/never understands others; kappa = .75; Hirdes et al., 2008). Finally, an overall decline in communication (making self-understood or understanding others) in the previous 90 days was measured using a single dichotomous item.
Within the RAI-HC, there are six health index scales embedded within the assessment. Functional performance is measured using two scales. The first, the ADL Self-Performance Hierarchy Scale (ADL-SHS) examines a client’s physical functioning in personal care activities such as eating, locomotion, bathing, and dressing. Functioning on these items is rated on a scale from 0 (independent) to 6 (total dependence) (Cronbach’s α = .94; Kim et al., 2015; kappa = .89; Guthrie et al., 2011). The second scale, the IADL Capacity Scale, rates three IADLs (meal preparation, phone use, and ordinary housework) on a scale of 0 (independent) to 6 (great difficulty in all three IADLs) (Cronbach’s α = .94; Kim et al., 2015; kappa = .83; Guthrie et al., 2011). A cut point of 2 or higher on both of these scales was used for this study and identifies clients with at least mild impairment (Morris et al., 1999).
The Cognitive Performance Scale (CPS) includes items pertaining to short-term memory, decision-making, expressive communication, and independence in eating. The CPS ranges from 0 (intact) to 6 (severe impairment) and has been validated against the Mini Mental State Exam (Morris et al., 1994). A cut point of 3 or higher was used to identify clients with moderate to severe cognitive impairment. The frequency and intensity of pain was assessed using the 4-point Pain Scale, which ranges from 0 (no pain) to 3 (severe daily pain), where a cut point of two indicates those with severe and/or daily pain (Cronbach’s α = .93; Kim et al., 2015). Symptoms of depression was rated on the 14-point Depression Rating Scale (DRS), which combines seven items relating to mood and seven items relating to behavior. A score of 3 or greater is indicative of at least mild/moderate depressive symptoms (Martin et al., 2008; Cronbach’s α = .76; Kim et al., 2015). Finally, the Changes in Health, End-Stage Disease, and Signs and Symptoms Scale is used to identify those experiencing health instability or are at risk of mortality. Scores range from 0 (no health instability) to 5 (severe health instability) with a cut point of 2 or higher indicating moderate to severe instability (Hirdes et al., 2014).
Analysis
Multinomial logistic regression was used to calculate unadjusted odds ratios (ORs) and 95% confidence intervals (95% CIs), which were used to determine statistically significant variables associated with hearing deterioration. We chose to perform multinomial logistic regression instead of ordinal logistic regression due to the four levels of the outcome variable.
We recognize that there are multiple ways that a client could be categorized into the 1-point deterioration group (e.g., client’s hearing score goes from a 0 to a 1 or increases from a 2 to a 3, etc.). We explored these differences by splitting each hearing deterioration group into subgroups based on their baseline hearing level. However, due to small sample sizes in one subgroup (n = 153), we were unable to compute meaningful ORs, therefore we decided to collapse all 1-point deteriorations together.
Home care clients with no deterioration were compared descriptively with clients with each of the different degrees of hearing deterioration with respect to demographic characteristics (e.g., age and sex), social, psychological, and physical items, and across the health index scales. All potential explanatory variables were based on the first assessment. A stratified analysis was completed to better understand the relationship between hearing deterioration and communication decline in the presence of a cognitive impairment. Variables capturing a clinical diagnosis of either Alzheimer’s disease or other dementias were used to identify the presence of a cognitive impairment. Multinomial logistic regression analyses were then performed to examine important risk factors associated with experiencing a hearing deterioration. Results from the univariate analysis and relevant literature were used to identify important covariates. These covariates included age, sex, education, the presence of Alzheimer’s disease or another dementia, the DRS scale, the ADL-SHS scale, the Pain scale, the IADL scale, a decline in communication in the last 90 days, and history of a stroke. We decided to include a diagnosis of Alzheimer’s disease or other dementias instead of the CPS score as a measure of cognitive impairment because the CPS score includes a measure of communication. Including the CPS score and the communication decline variable would likely result in multicollinearity, therefore we chose to keep communication decline in the model as the RAI-HC includes other measures of cognitive impairment. The preliminary model showed no issues of multicollinearity or confounding. Model fit was based on the Akaike Information Criterion (AIC) where a lower AIC value indicates better model fit. All analyses were conducted using SAS software (version 9.2, SAS Institute Inc., Cary, NC, USA). The study followed the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) guidelines (von Elm et al., 2007).
Results
At the time of their first assessment, 51.3% (n = 30,194) of clients experienced no difficulty in their hearing, 31% (n = 18,540) of clients had minimal difficulty with their hearing, 16.7% (n = 9,894) had mild/moderate difficulty, and 1% (n = 560) had a severe impairment in their hearing. Clients who had a higher degree of impairment were more likely to be older, female, and unmarried (data not shown).
The mean time between a client’s two most recent assessments was 5.8 months (SD = 2.8). When examining the change in hearing impairment between the two assessments, 92% (n = 54,364) of clients did not experience a deterioration in hearing, 7% (n = 4,243) had a 1-point deterioration, and 1% had a combination of either a 2-point (n = 540) or a 3-point (n = 41) deterioration in hearing (Table 1). At the time of the most recent assessment, the mean age of the sample was 83.5 years (SD = 7.5), two thirds were female (66.5%), almost half of the clients were widowed (49.3%), and the majority did not complete high school (61.4%). The degree of impairment across most variables was progressively worse with each level of hearing deterioration. This was true for items including age, communication decline, receptive and expressive communication, and across the majority of the health index scales (Table 1).
Demographic and Other Characteristics Comparing Clients With No Deterioration and Across Multiple Levels of Hearing Deterioration.

To compute meaningful ORs, clients in the 2-point and 3-point deterioration groups were combined to create one group due to the low sample size in the 3-point deterioration group (n = 41). The multinomial unadjusted ORs, comparing those who experienced a deterioration in their hearing with those who did not, showed that age was an important factor for hearing deterioration (Table 2). Compared with clients between the ages of 65 and 74 years, being aged 75 to 84 years increased the odds of a 1-point hearing deterioration by 58% (OR = 1.58; 95% CI = [1.41, 1.77]) and a 2/3-point deterioration by 45% (1.45; CI = [1.09, 1.94]); being 85+ years increased the odds of a 1-point deterioration (2.16; CI = [1.94, 2.41]) and a 2/3-point deterioration (1.94; CI = [1.46, 2.56]). Clients who were male (1.09; CI = [1.02, 1.16]) or widowed (1.10; CI = [1.03, 1.18]) were significantly more likely to have a 1-point deterioration in hearing, but not a 2/3-point deterioration.
Unadjusted Demographic and Other Characteristics Comparing Clients With No Deterioration (n = 54,364) to Two Different Levels of Hearing Deterioration.
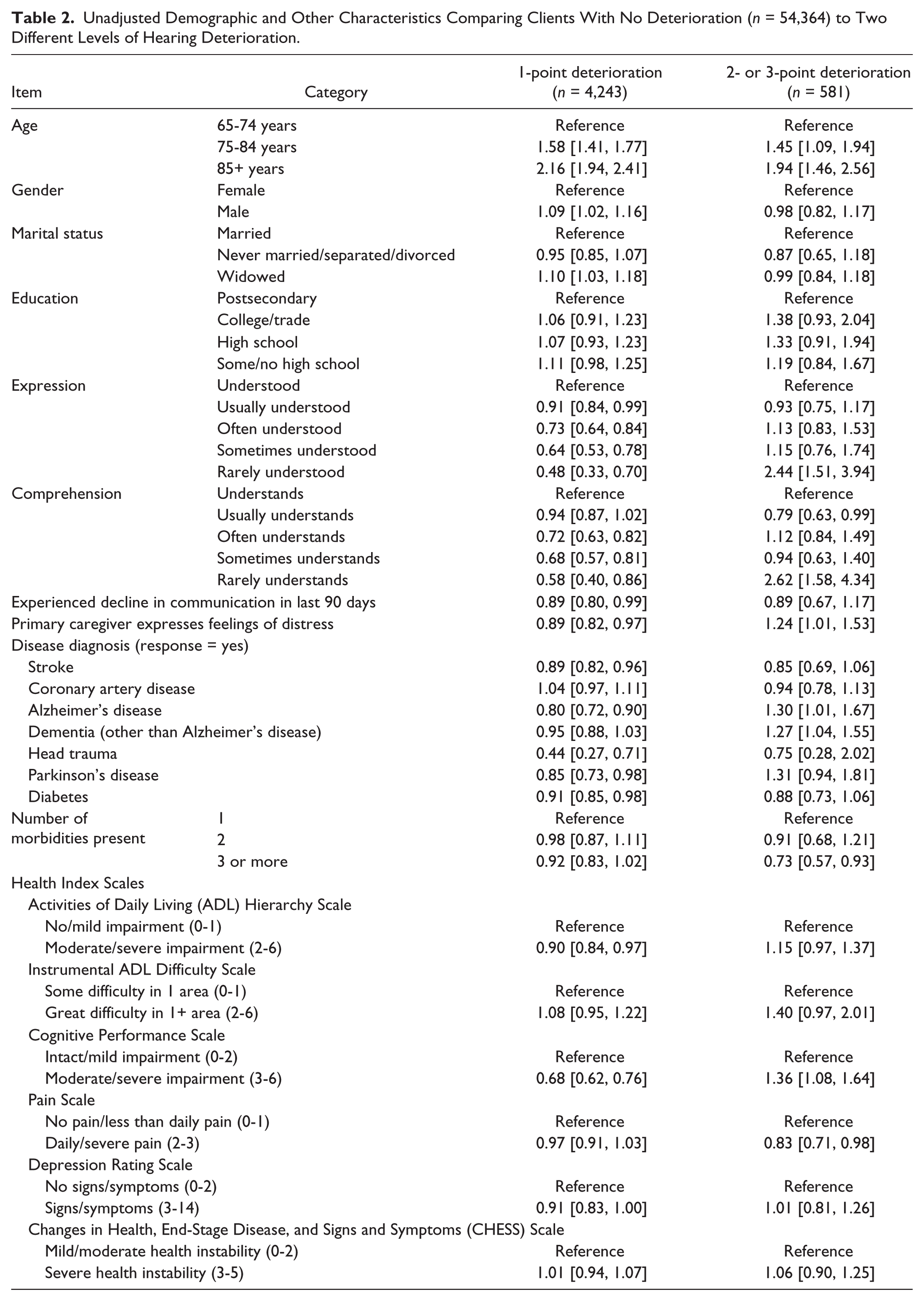
Both a 1-point and a 2/3-point hearing deteriorations showed an important link to items capturing the client’s ability to make themselves understood (expression) and their ability to understand others (comprehension). If a client had any difficulty expressing themselves to others, they were less likely to experience a 1-point deterioration in hearing. This was true for being usually understood (0.91; CI = [0.84, 0.99]), often understood (0.73; CI = [0.64, 0.84]), sometimes understood (0.64; CI = [0.53, 0.78]), and rarely understood (0.48; CI = [0.33, 0.70]). Conversely, clients were 2.44 times (2.44; CI = [1.51, 3.94]) as likely to experience a 2/3-point deterioration in hearing if they were rarely understood by others. Similar results were found when examining the comprehension variable. Clients who often understand others (0.72; CI = [0.63, 0.82]), sometimes understand others (0.68; CI = [0.57, 0.81]), and rarely understand others (0.58; CI = [0.40, 0.86]) were less likely to experience a 1-point deterioration in hearing. Clients who rarely understand others were 2.62 times (2.62; CI = [1.58, 4.34]) as likely to be at risk of a 2/3-point deterioration in hearing over time. A decline in communication over the last 90 days was protective for developing a 1-point deterioration (0.89; CI = [0.80, 0.99]), but was not associated with a 2/3-point deterioration (0.89; CI = [0.67, 1.17]).
The presence of a distressed caregiver was protective against developing a 1-point deterioration (0.89; CI = [0.82, 0.97]), while having a distressed caregiver increased the risk of developing a 2/3-point deterioration by 24% (1.24; CI = [1.01, 1.53]). A history of a previous stroke (0.89; CI = [0.82, 0.96]), a diagnosis of Alzheimer’s disease (0.80; CI = [0.72, 0.90]), head trauma (0.44; CI = [0.27, 0.71]), Parkinson’s disease (0.85; CI = [0.73, 0.98]), and diabetes (0.91; 0.85, 0.98) were all protective of developing a 1-point deterioration. A diagnosis of Alzheimer’s disease (1.30; CI = [1.01, 1.67]), or other types of dementia (1.27; CI = [1.04, 1.55]) showed the greatest risk of developing a 2/3-point deterioration. Finally, clients who had three or more chronic health conditions were less likely to experience a 2/3-point deterioration (0.73; CI = [0.57, 0.93]). The number of chronic conditions did not seem to be an important risk factor for clients who developed a 1-point deterioration (Table 2).
Across all of the health index scales, moderate/severe impairment on the ADL-SHS (0.90; CI = [0.84, 0.97]) reduced the risk of experiencing a 1-point deterioration. The only scale that increased the risk of developing a 2/3-point deterioration in hearing was the CPS score. Clients were 36% more likely (1.36; CI = [1.08, 1.64]) to develop a greater degree of impairment in their hearing if they had moderate/severe impairment in cognition. Clients were 32% less likely (0.68; CI = [0.62, 0.76]) to develop a 1-point deterioration if they had an impaired CPS score.
When looking at the stratified analysis, the OR changed very little in the presence of a cognitive impairment. The OR between hearing deterioration and communication decline never changed by more than 0.04 when a diagnosis of Alzheimer’s disease was present. The same was also true when a diagnosis of dementia other than Alzheimer’s disease was present (data not shown). Therefore, it appears that cognitive impairment is not confounding the relationship between hearing deterioration and communication decline.
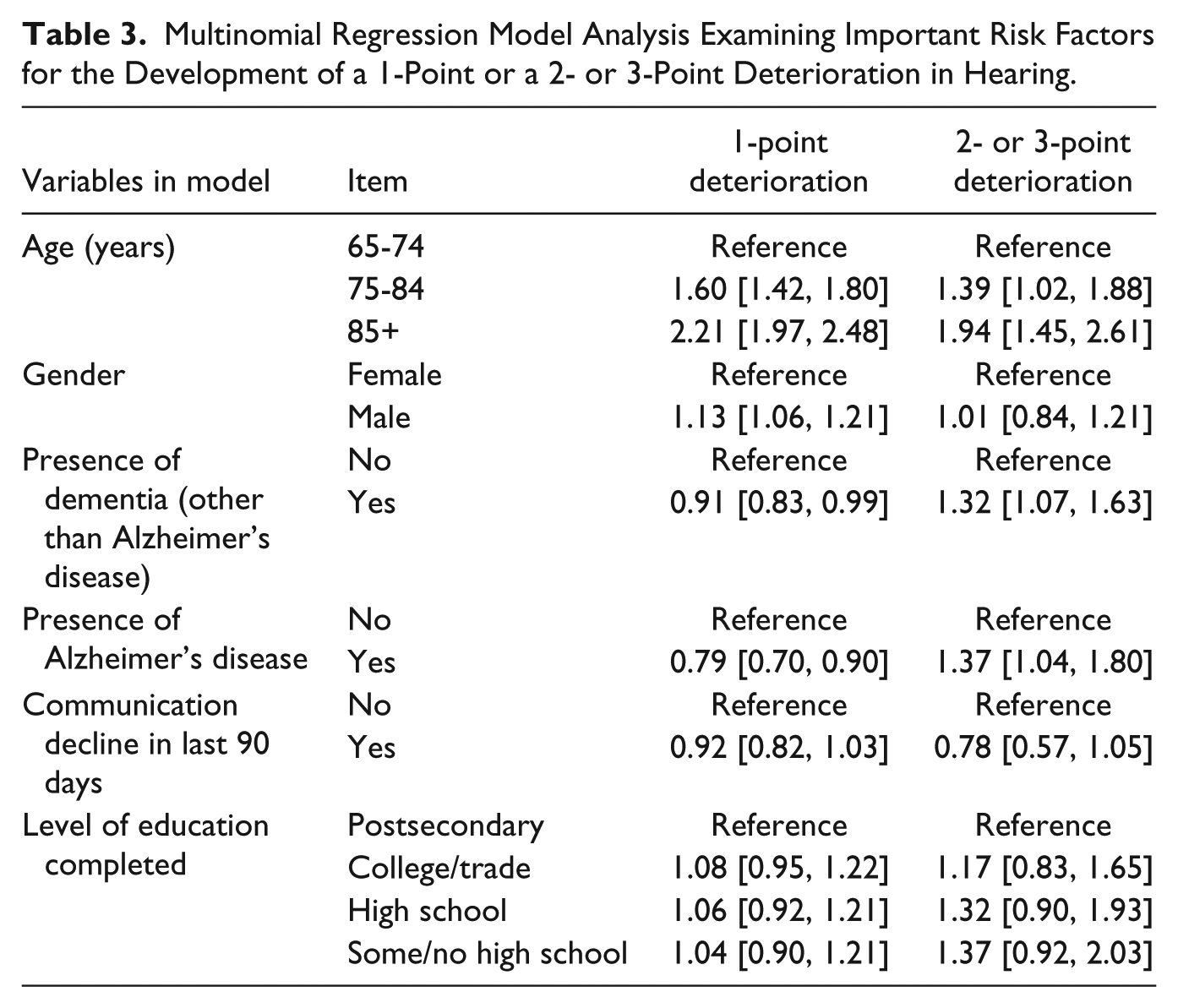
In the multinomial logistic regression model, increasing age was significantly associated with the risk of developing both a one- and a 2/3-point deterioration even after adjusting for the other covariates in the model. Compared with those aged 65-74 years, clients aged 75-84 years had a 60% greater risk (1.60; CI = [1.42, 1.80]) of developing a 1-point deterioration and a 39% risk (1.39; CI = [1.02, 1.88]) for a 2/3-point deterioration. Similarly, being older than 85 further increased the risk of a 1-point deterioration (2.21; CI = [1.97, 2.48]) and a 2/3-point deterioration (1.94; CI = [1.45, 2.61]). After adjusting for all other covariates, clients with a diagnosis of Alzheimer’s disease (1.37; CI = [1.04, 1.80]) or another dementia (1.32; CI = [1.07, 1.63]) were at a greater risk of developing a 2/3-point deterioration. Conversely, a diagnosis of Alzheimer’s disease (0.79; CI = [0.70, 0.90]) or another dementia (0.91; CI = [0.83, 0.99]) were both protective against a 1-point deterioration. Finally, being male increased the risk of a 1-point deterioration by 13% (1.13; CI = [1.06, 1.21]; Table 3). Communication decline did not seem to have a significant influence on the development of a 1-point or a 2/3-point deterioration, however, when it was not included in the model, the effect of Alzheimer’s disease and other dementias was not as pronounced (data not shown).
Multinomial Regression Model Analysis Examining Important Risk Factors for the Development of a 1-Point or a 2- or 3-Point Deterioration in Hearing.
Discussion
To our knowledge, this is one of few studies to look at the prevalence of hearing impairment in a sample of older adults receiving home care services. We found that 50% of clients had some difficulty in their hearing at the start of the study, and 8% experienced some degree of deterioration over 1 year. Overall, clients who experienced any degree of deterioration in hearing were more likely to be at least 75 years of age. Clients with a 2/3-point deterioration experienced greater difficulties on items involving communication compared with clients who only had a 1-point deterioration. In addition, clients were at a greater risk of developing a 2/3-point deterioration if they had a distressed caregiver or a diagnosis of Alzheimer’s disease or another type of dementia.
Strawbridge and colleagues examined the influence of varying levels of hearing impairment at baseline on health and psychosocial functioning 1 year later and found a dose–response relationship where older adults with increasing degrees of hearing impairment had reduced levels of physical and social functioning compared with those with no hearing impairment (Strawbridge et al., 2000). In the current study, we found that clients with a 1-point hearing deterioration were less likely to have difficulties with physical functioning and communication abilities, whereas those with a 2/3-point deterioration were much more likely to have reduced physical functioning and communication abilities.
Generally, within the literature, increasing age has been associated with a greater risk of hearing impairment (Arlinger, 2003; Boi et al., 2011). In the current study, the highest proportion of clients with any level of deterioration was 75+ years, with the greatest risk of deterioration occurring in the oldest age group. Similarly, Cruickshanks and colleagues (2003) also found that the only factor associated with the progression of hearing deterioration over time was increasing age. In addition, Hietanen, Era, Sorri, and Heikkinen (2004) found that significant hearing deterioration occurred after 80 years of age in a group of community-dwelling older adults after a 10-year follow-up period (Hietanen et al., 2004).
In terms of gender differences, we found only a small increase in the odds of hearing deterioration for males. It is well cited throughout the literature that males tend to have a higher prevalence of hearing impairment compared with females (Strawbridge et al., 2000, Linssen et al., 2014; Feder et al., 2015). However, some studies have shown a higher prevalence of hearing impairment in females, especially with increasing age. For example, Wiley, Chappell, Carmichael, Nondahl, and Cruickshanks (2008) looked at the 10-year progression of hearing threshold and found that men were less likely to experience a decline in their hearing compared with women. They suggested that men may experience worse hearing at baseline with a more gradual decline, whereas women may experience a delayed onset and then continue to decline more rapidly with age (Wiley et al., 2008). At the time of the first assessment, there were a higher proportion of females across all levels of hearing deterioration. This likely reflects the fact that females are much more likely to be enrolled in home care services compared with males (Lo, Gruneir, Bronskill, & Bierman, 2015; Sinha & Bleakney, 2014).
Overall, variables measuring communication appeared to be some of the most important factors related to hearing deterioration. Communication difficulties have been shown to be one of the main problems experienced by older adults with a hearing impairment (Huang & Tang, 2010; Strawbridge et al., 2000). Older adults who experienced a 1-point deterioration in hearing were less likely to have experienced difficulties with both expressive and receptive communication, whereas clients who had difficulties in these areas were more likely to experience a 2/3-point deterioration.
The use of assistive devices (i.e., hearing aids) can improve communication ability and in turn, has the potential to improve other areas of difficulties such as overall quality of life, ADL and IADL impairments and symptoms of depression (Brink & Stones, 2007; Bürge, von Gunten, & Berchtold, 2013; Dalton et al., 2003; Mulrow et al., 1990). It has been suggested that hearing aids improve communication ability and because of the link between communication and tasks related to IADLs (e.g., shopping and telephone use), the use of hearing aids will not only improve quality of life and mood, but also can be a conduit to improving a client’s functional status (Dalton et al., 2003; Gopinath, Schneider, et al., 2012). Despite the wealth of literature around the benefits of using hearing aids/assistive devices, their uptake among older adults is still quite low. This has been attributed to factors such as demographic characteristics, associated costs, and sources of motivation (Knudsen, Oberg, Nielsen, Naylor, & Kramer, 2010). What appears to be missing is a clear population-level strategy to address these factors in an effort to increase their use and minimize the negative consequences of untreated hearing loss. Underdetection and undertreatment of hearing loss can lead to multiple negative outcomes, including social isolation, loneliness, and loss of independence.
Screening for hearing difficulties and deterioration over time is vital as there are potential benefits that can result from having the proper devices and supports in place, a key step in improving health status and independence. The information collected from an assessment, such as the RAI-HC, allows home care professionals to identify hearing impairments and connect the individual with the appropriate interventions, programs, and supports. Older adults who receive these types of interventions have been found to have improvements in their hearing as well as other health-related outcomes such as increased quality of life (Boi et al., 2011), reduced social isolation (Weinstein, Sirow, & Moser, 2016), and improved communication abilities (Hickson, Worrall, & Scarinci, 2007; Mamo, Reed, Nieman, Oh, & Lin, 2016). Screening older home care clients for hearing impairments and implementing the necessary aural rehabilitation interventions can help ensure that their level of independence and their quality of life is optimized as clients continue to age.
In the multinomial logistic regression model, increasing age was found to be an important risk factor for experiencing any degree of hearing deterioration, even after adjusting for all other covariates in the model. Although increasing age was an important risk factor for both deterioration groups, it was even more pronounced for clients who experienced a 1-point decline. In addition, clients who had a previous diagnosis of Alzheimer’s disease or other dementia were at a greater risk of experiencing a 2/3-point deterioration, but not a 1-point decline. Clients with a 1-point deterioration do seem to have a slightly different pattern of results compared with those with a 2/3-point deterioration. This may be because the clients in the 1-point deterioration group were not homogeneous. The clients within this group had varying baseline hearing levels. Although their overall degree of deterioration was the same, their hearing level overall may be quite different. The presence of any form of dementia was actually protective of experiencing a 1-point decline. The relationship between hearing impairment and cognitive difficulties is complicated as a hearing impairment can further exacerbate a cognitive impairment and vice versa. There are similarities between hearing and cognitive impairments including difficulty in understanding speech, word-finding problems, and social isolation (Slaughter et al., 2014). It is therefore possible that the presentation of a new and minimal change in hearing (e.g., a 1-point decline) may actually be masked by the presence of cognitive difficulties. When someone cannot hear properly, it may be mistaken for not actually understanding what is being said and could be interpreted as a cognitive issue, rather than as an issue with hearing. This could potentially explain the finding that individuals with Alzheimer’s disease, or another form of dementia, had a reduced risk of a 1-point deterioration in the current analysis.
In the current model, communication decline did not seem to be an important risk factor for hearing deterioration; however, when communication decline was not in the model, the presence of Alzheimer’s disease and other dementias were not as big of a risk factor for hearing deterioration. It seems that a decline in communication is not predictive of hearing deterioration over time; however, there does seem to be an important link between cognitive impairments, communication, and hearing deterioration. The stratified analysis showed similar results as the relationship between hearing decline and communication decline did not change by more than 0.04 when a diagnosis of Alzheimer’s disease or other dementia was present. There is emerging evidence within the literature looking at the relationship between hearing impairment and cognitive decline. Individuals who experience cognitive decline also have difficulties with communication. Communication difficulties may become further exacerbated when cognitive and hearing impairments coexist, therefore it is important to diagnose and treat hearing impairments early in an attempt to reduce the associated negative outcomes. To better tease out the influence of communication decline, a more sophisticated study design would be needed, which was beyond the scope of this project. Future studies could follow various cohorts (e.g., those with cognitive impairment, varying levels of hearing loss, etc.) over time to examine how their communication changes in relation to each cohort.
The current study has several strengths including our outcome of interest, which looked at hearing deterioration over time and a large sample size. To our knowledge, this is one of the only studies completed in Canada that has looked at hearing impairment, how it progresses over time, and the relationship hearing deterioration may have on items such as physical functioning and communication. In addition, we analyzed data collected from a RAI-HC assessment, which is a standardized assessment used in multiple regions of Canada, the United States, and in many other countries. Utilizing data from a standardized assessment allows for direct comparisons to be made not only within each country, but between countries. Within Ontario, the RAI-HC is a mandated assessment that each long-stay client receives on enrollment, which means that clients are being screened for hearing and communication issues. If a hearing impairment is identified, this provides home care professionals with real-time information that can assist them in developing care plans and making appropriate referrals to other specialized clinicians (e.g., audiologists).
One limitation to this study is the small number of clients who experienced a 3-point deterioration (n = 41). The 12-month time frame that was chosen may not have the ability to pick up on large deteriorations in hearing; however, we chose this time frame because it is in line with the typical reassessment protocol for home care clients in Ontario (Ministry of Health and Long-Term Care, 2006). Due to the limited number of clients in each deterioration group, we were not able to separate out each possible combination of hearing deterioration. Despite this limitation, it appears that clients with a 3-point deterioration are different than clients with a 2-point deterioration. Clients with a 3-point deterioration consistently experienced greater difficulties in items relating to communication and were also more impaired on a number of the health index scales. In addition, we also had to lump each 1-point deterioration group together due to small sample sizes. Preliminary analysis showed that these subgroups were not homogeneous; however, we could not compute meaningful statistics when they were separated due to small sample sizes. Hearing was measured using a single item on the RAI-HC which is based on a combination of discussions between the care coordinator, the client, their informal caregivers, and other health care professionals (e.g., primary care physician) to make an appropriate decision regarding hearing status. The true severity of the hearing impairment in the current study may actually be underestimated; however, we suspect that the degree of bias is relatively small. A study by Dalby and colleagues (2009) found a high correlation between the functional hearing item and alerting to sounds within the environment (rho = 0.77) (Dalby et al., 2009). In addition, a geriatric assessment is part of the gold standard for understanding the health and functioning of older adults. Therefore, by utilizing the RAI-HC assessment, the current study was able to capture the relationship between a decline in hearing and the effect this may have on physical and psychosocial functioning (Phillips et al., 1998; Schroll, 1997). Finally, the RAI-HC does not include information as to whether the client wore/actively used hearing aids; however, care coordinators are instructed to complete the assessment only once the hearing aid is in place.
Sensory loss rarely occurs in isolation. It is often accompanied by a number of other age and health-related changes. It is not uncommon for a decline in hearing to translate into limitations in participation within the community. The World Health Organization (WHO) developed the International Classification of Functioning, Disability and Health (ICF), which provides a framework to describe a wide range of information regarding a number of health domains (WHO, 2001). The ICF makes distinctions between diagnosis, functioning, activity limitation, and restrictions to participation, which helps to better understand the complex nature of a hearing impairment. Crews and Campbell (2004) used this conceptual framework when examining older adults with hearing, vision, and combined hearing and vision impairments. They found that older adults experiencing any kind of sensory impairment were more likely to also experience activity and social participation limitations compared with those without sensory impairments (Crews & Campbell, 2004).
Hearing impairment is one of the most prevalent chronic conditions in older adults, yet it often goes unrecognized and untreated. Several beneficial rehabilitative interventions exist, including hearing aids (Boi et al., 2011; Davis et al., 2016), communication programs (Hickson et al., 2007), and perceptual training (Woods et al., 2015). It is therefore essential for older home care clients to have a standardized assessment as it provides valuable information about impairments/deteriorations in hearing. It is important to promote increased awareness of how a hearing impairment can affect overall quality of life and can have a negative impact on both social and physical functioning. The cornerstone of good patient-centered care is continued two-way communication between the client and health care provider. Communication can be complicated by the presence of a cognitive impairment; therefore, it is essential for home care providers to continue to assess both hearing and cognitive impairments by using a standardized assessment, such as the RAI-HC, as it can help assist them in establishing good two-way communication to ensure the client’s goals are met and their quality of care and quality of life is optimized. A decline in communication may not only limit a client’s access to health care services, but may also lead to the potential of miscommunication in regard to important health information. Screening older home care clients for hearing impairments and implementing the necessary aural rehabilitation interventions can help ensure that their level of independence and their quality of life are optimized as clients continue to age.
Footnotes
Acknowledgements
The authors would like to acknowledge the Canadian Institute for Health Information (CIHI) for providing the data.
Authors’ Note
N.W. provided statistical analysis and drafted the manuscript. D.M.G. contributed to the conception, interpretation of results, and critical revisions of the work. K.F. and L.E.G. contributed to the conception of the work and also provided critical revisions. J.G.S.D. helped write the “Method” and “Results” section of the article and provided critical revisions. All authors discussed the results and implications and commented on the manuscript at all stages.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: D.M. Guthrie is supported by the Lloyd Carr-Harris Foundation; L. E. Griffith is supported by a Canadian Institutes of Health Research New Investigator’s Award and the McLaughlin Foundation Professorship in Population and Public Health.