
Abstract
Community-based exercise programs have demonstrated feasibility, yet many lack controlled studies examining their efficacy. This study examined the efficacy of a community-based exercise program, using a controlled design. Participants (N = 262, Mage = 74.0 years, SD = 8.4) were women (77%) and men recruited from senior centers served by the county Area Agency on Aging. Intervention participants (n = 133) were newly enrolled in classes. Controls (n = 129) were recruited from matched sites not offering classes. Validated measures of physical function, exercise self-efficacy, balance, and activities of daily living (ADL) confidence were administered at baseline and 3 months. Significant improvements in upper and lower body strength, aerobic endurance, mobility, exercise self-efficacy, and balance were found in the exercisers but not controls. No changes in ADL confidence occurred in exercisers, while significant decreases occurred in controls. Findings support the efficacy of the county-wide program. Building an evidence base for community-delivered programs should provide impetus for increased dissemination through state and national agencies thereby increasing program impact.
Recent estimates indicate that the number of U.S. adults aged 65 years and older will increase from 46.2 million, reaching approximately 98 million by 2060 (Colby & Ortman, 2015). The need to effectively address the risks and burden of disability and chronic disease often associated with aging is critical. Strategies fostering healthy aging will reduce the likelihood of diminished functional ability, loss of mobility, decreased quality of life, and loss of independence (Centers for Disease Control and Prevention [CDC], 2013).
Physical function is central to performing activities of daily living (ADL) and key to maintaining physical independence. Declines in ADL competence lead to an increased probability of dependence and institutionalization (Covinsky et al., 2003; Penninx et al., 2001). Hence, strategies to promote improved physical function are an integral part of maintaining health during the aging process. Physical activity has consistently been related to improved physical function and quality of life in older adults (Baruth et al., 2011; Bauman, Merom, Bull, Buchner, & Singh, 2016; Chih-Hsuan, Chueh-lung, & Ying-Tai, 2012). Yet, recent estimates indicate that older adults are among the most inactive with 26.9% of those aged 65 to 74 years, and 35.3% of those 75 years and older reporting no physical activity (Watson et al., 2016). Public health guidelines include physical activity as a key component for healthy aging (Office of Disease Prevention and Health Promotion, 2016; U.S. Department of Health and Human Services, 2008). The CDC Healthy Aging Research Network recommends that physical activity interventions increase health-related fitness, self-efficacy, and sustainability through the use of community resources (Prohaska et al., 2006). Community settings that encourage physical activity and provide access to safe activity experiences will enhance the likelihood of increased activity among older adults (Watson et al., 2016).
A variety of structured exercise interventions designed for older adults have improved physical function, reduced fall risk, and enhanced quality of life (Chang et al., 2004; Dunn et al., 1998; Gates, Fisher, Cooke, Carter, & Lamb, 2008; Levy et al., 2012). Yet, relatively few of these instructor-led programs have been integrated into services provided by state health and community agencies serving older adults (Sleet, Moffett, & Stevens, 2008) and they remain largely underused by agency constituents (Theis, Helmick, & Hootman, 2007). At the same time, agencies have called for strategies to effectively bridge research efforts to sustainable community programs (Estabrooks & Glasgow, 2006; Zaza, Briss, & Harris, 2005). The CDC is working to bridge this gap through the endorsement of community-delivered programs that have demonstrated efficacy for further dissemination. Although exercise programs for older adults are available in many communities, relatively few have provided this evidence. When recommending exercise programs appropriate for those with arthritis (about 60% of older adults) for adoption by state health departments with receipt of CDC funding, only four programs are available (CDC, 2016; Hootman, Helmick, & Langmaid, 2003). Clearly, to increase the impact of exercise interventions on the growing population of older adults, programs with high potential for successful translation and wide dissemination warrant efficacy studies to provide evidence of their effects. These steps increase the likelihood of adoption by state health agencies for further dissemination.
Some community-based exercise programs have demonstrated efficacy and feasibility in their delivery and acceptance (e.g., Belza et al., 2006). Many however lack controlled studies examining program efficacy, and few have used both objective and subjective measures of function. The purpose of the current study was to examine the efficacy of a county-wide disseminated exercise program for older adults in improving physical function, confidence in performing ADL and exercise self-efficacy, over a 3-month period. Confidence in performing ADL was examined due to their strong relationship to physical function and maintaining independence, and program content which also emphasized functional fitness. Exercise self-efficacy was of interest based on guidelines of the CDC Healthy Aging Research Network (Prohaska et al., 2006) and its consistent link to exercise adoption and maintenance in older adults (King, 2001; McAuley, Jerome, Marquez, Elavsky, & Blissmer, 2003; McAuley et al., 2011; Schutzer & Graves, 2004). We hypothesized that those in the exercise classes would evidence improved physical function, balance, and activity-related perceptions compared with controls over a 3-month period.
Method
Participants
Participants (N = 262, Mage = 74.0 years, SD = 8.4) were women (77%) and men recruited in collaboration with community partners from community centers (e.g., senior, faith-based, libraries) served by Aging and Independence Services (AIS), a division of the County of San Diego Health and Human Services Agency. AIS offers a variety of free services to older adults across the county including the Feeling Fit Club (FFC) exercise classes. The FFC exercise program has been offered county-wide since 1999 when it was first developed by a task force with expertise in exercise physiology, group fitness, and service provision to older adults. The FFC program was integrated into the cooperative meal service program offered by AIS across the county with classes initially held prior to lunch service. The FFC program is cost-free to participants and has grown to 29 classes offered county-wide. A full description of the FFC content and focus is described below. New FFC classes are periodically introduced at sites serving their constituency. Those in the intervention group (n = 133, Mage = 73.3 years, SD = 8.7) were recruited from FFC classes that were starting at seven centers, via study announcements prior to the start of the classes. Control participants (n = 129, Mage = 74.7 years, SD = 8.0) were similarly recruited from demographically (i.e., age, gender, ethnicity, site location within county) matched sites at which FFC classes were not offered. Inclusion criteria were the ability to ambulate without a wheelchair, and clearance to participate in physical activity based on “no” responses to the Physical Activity Readiness Questionnaire (PAR-Q, Canadian Society for Exercise Physiology, 2002), and no previous participation in FFC classes. Although not participating in FFC classes during the course of the study, control participants were encouraged to join a nearby FFC class once the study was concluded and provided FFC locations. The majority of participants were Caucasian (79%), with 7% reporting as Latino/Hispanic, 5% East Asian, 3% Black/African American, 3% Native American, and 3% Other. Participants reported being married/domestic partner (33%), divorced/separated (29%), widowed (20%), and single (18%). Participants were generally well-educated, with 73% having completed at least some college or vocational training, and less than 10% reporting less than completing high school. Participants were compensated with a US$20 gift card at each data collection. Approval for the study was obtained through the University’s Institutional Review Board for the protection of human subjects.
Measures
Measures of physical function were selected from the Rikli and Jones’s (1999) Senior Fitness Battery, based on their appropriateness, relationship to ADL, and their acceptable psychometric characteristics in the target population. Balance was assessed due to its relationship to fall risk and physical function (Jorgensen, Laessoe, Hendriksen, Nielsen, & Aagaard, 2013; Muir, Berg, Chesworth, Klar, & Speechley, 2010). Self-report measures of function related to independence and exercise self-efficacy, were also administered. Measurement personnel were specifically trained in the measurement protocol to ensure reliability. Initial training consisted of 2 days covering administration of physical and written measures and included role-playing, data collection, recording, and addressing potential participant questions. Booster measurement protocol trainings were held prior to each data collection period.
Physical function
Upper body strength and endurance, associated with daily tasks such as lifting, carrying, and general house and yard work were assessed with the arm curl test. While seated, participants complete as many arm curls as possible with their dominant arm in 30 s. Women use a 5-lb weight and men use an 8-lb weight (Rikli & Jones, 1999).
Lower body strength was measured using the 30-s chair stand in which participants start in a seated position with hands crossed on the chest and repeatedly rise to a standing position then sit. The score is the total number of sit-stands completed in 30 s. The test has successfully discriminated frailty in older adults with coronary artery disease (Purser et al., 2006).
Mobility, reflecting a combination of lower body strength, power, and dynamic balance, was assessed using the 8-ft up-and-go. Participants start in a seated position and on the signal “go” rise and walk as quickly as possible around a cone placed 8-ft away, returning to a seated position. Two trials are completed with the fastest trial time serving as the test score. The test has shown good predictive validity in discriminating older adult fallers from nonfallers (Rose, Jones, & Lucdhese, 2002).
Aerobic endurance was assessed using the 6-min walk. Participants walk a marked course for 6 min, with distance completed serving as an indicator of aerobic endurance related to common ADL. The test is widely used with older adults and has been more closely associated with ADL than other functional walk tests (Solway, Brooks, Lacasse, & Thomas, 2001).
Balance
Balance was assessed using the BTrackS Balance System (BBS; Balance Tracking Systems, n.d.). Participants stand on a portable 15.5″ × 23.5″ platform, supported on four adjustable legs approximately 2″ off the ground. The BBS is linked to a computer laptop via USB that runs custom software. In a manner similar to the scientific grade force plate, the BBS captures postural sway, reflecting anterior–posterior, and medial-lateral body movement away from one’s center of pressure (COP), in a variety of balance conditions. For the current study, participants stood as still as possible for three 20 s trials, feet shoulder width apart, hands on hips, in both eyes-open and eyes-closed conditions for a total of six trials. Mean trial COP in eyes-open and in eyes-closed served as scores, with lower scores reflecting better balance. This BBS protocol has been previously validated in community-dwelling older adults (Levy, Thralls, & Kviatkovsky, 2016).
ADL
The eight-item Instrumental Activities of Daily Living Scale (IADL; Lawton & Brody, 1969) was used to assess independent living skills. Participants report their level of proficiency in performance of activities of living (e.g., shopping, preparing a meal, housekeeping) with scores in each activity reflecting their highest level of function. Summary scores range from 0 to 8, with higher scores indicating greater function in ADL necessary for independence. The measure is specifically designed for and has been validated in older adults (Vittengl, White, McGovern, & Morton, 2006).
Exercise self-efficacy
Self-efficacy for exercise was measured using a six-item measure asking participants to report their degree of confidence in their ability to walk at a moderate-intensity without stopping for increasingly longer periods of time, ranging from 10 to 60 min, as suggested by Bandura (2006). The scale is a modification of the 5-min incremental self-efficacy for walking scale (SEW; McAuley, Courneya, & Lettunich, 1991), shortened to reduce participant burden. Walking was chosen as the activity as it is the predominant mode of aerobic activity in which older adults engage (Belza et al., 2004). Internal consistency reliability of the measure in the current study was excellent (α = .97).
Procedure
In collaboration with community partners (AIS), individuals signing up for new FFC classes were given study flyers as well as a brief description of the study. Interested individuals provided contact information. A member of the investigative team later contacted and screened those individuals per inclusion criteria. A measurement appointment was scheduled prior to the start of FFC classes. Recruitment, contact, and appointment set up occurred similarly with control participants at sites not offering FFC classes. Measures of physical function and balance were collected at baseline and at 3 months. Data collection occurred at the same site as recruitment. At baseline, participants were again screened to ensure that they met inclusion criteria, and completed informed consent. Physical function,balance, and self-report measures were collected by trained measurement staff and were completed in approximately 30 min for each participant.
FFC Class Content
The FFC is an ongoing exercise program designed to improve physical function and reduce fall risk in older adults. The goal of FFC is to provide a safe environment in which older adults can engage in physical activity and improve and maintain health-related fitness. The program emphasizes improvement and encourages social interaction and fun during classes. FFC classes met twice weekly, and were led by qualified instructors (previous exercise leadership experience with older adults) specifically trained in the FFC program components. Instructors were trained to incorporate principles of progressive overload and specificity to appropriately challenge participants to improve their physical fitness (Pescatello, 2014). Instructors were also trained to incorporate consistent and appropriate feedback to class participants, to help participants set challenging and achievable goals for themselves, and to acknowledge improvement, as a means to increase self-efficacy for exercise. Training emphasized instructor interaction and encouragement of class participants’ support for one another, and provision of a comfortable environment. Providing this sense of camaraderie included learning and using class members’ names, providing FFC t-shirts to class members, creating birthday boards to recognize class members’ birthdays, and encouraging holiday social gatherings.
All instructors were required to demonstrate a complete class and were evaluated by the senior FFC trainer to assure proficiency in FFC class leadership. Full day booster training sessions for instructors are given on a yearly basis and a lead FFC trainer for the program, an exercise physiologist, provides overall supervision of program instructors, including annual in-class evaluations and individualized feedback for each instructor.
FFC exercises are low-impact, emphasize proper execution of movement, and focus on core body stabilization and strength, static and dynamic balance, flexibility, strength training, and aerobic endurance. Each class targets four components of fitness (Pescatello, 2014) through (a) a warm-up to increase heart rate (cardiorespiratory fitness), (b) balance and core work (proprioception, postural alignment, balance), (c) resistance exercises using small weights and resistance bands (strength of main muscle groups), and (d) a cool down including flexibility (range of motion, joint mobility, flexibility). Exercises are modified to meet individuals’ varying ability levels. Classes met for 1 hr, twice weekly. Instructors provided cues for proper body position (e.g., “belly button toward spine,” “chin level with floor”) to participants to ensure understanding. Modifications to exercises were also provided such as performing an exercise in a chair or holding on to the back of a chair, with instructors appropriately challenging participants as they progressed through the program. Instructors also provided concrete examples of the link between exercises done in class and ADL. Equipment included small hand-weights, ankle weights, resistance bands, and sit disks. FFC class components, examples, and modifications for individualization are summarized in Table 1.
Feeling Fit Club Class Components, Duration, Purpose, Examples, and Modifications for Individualization.
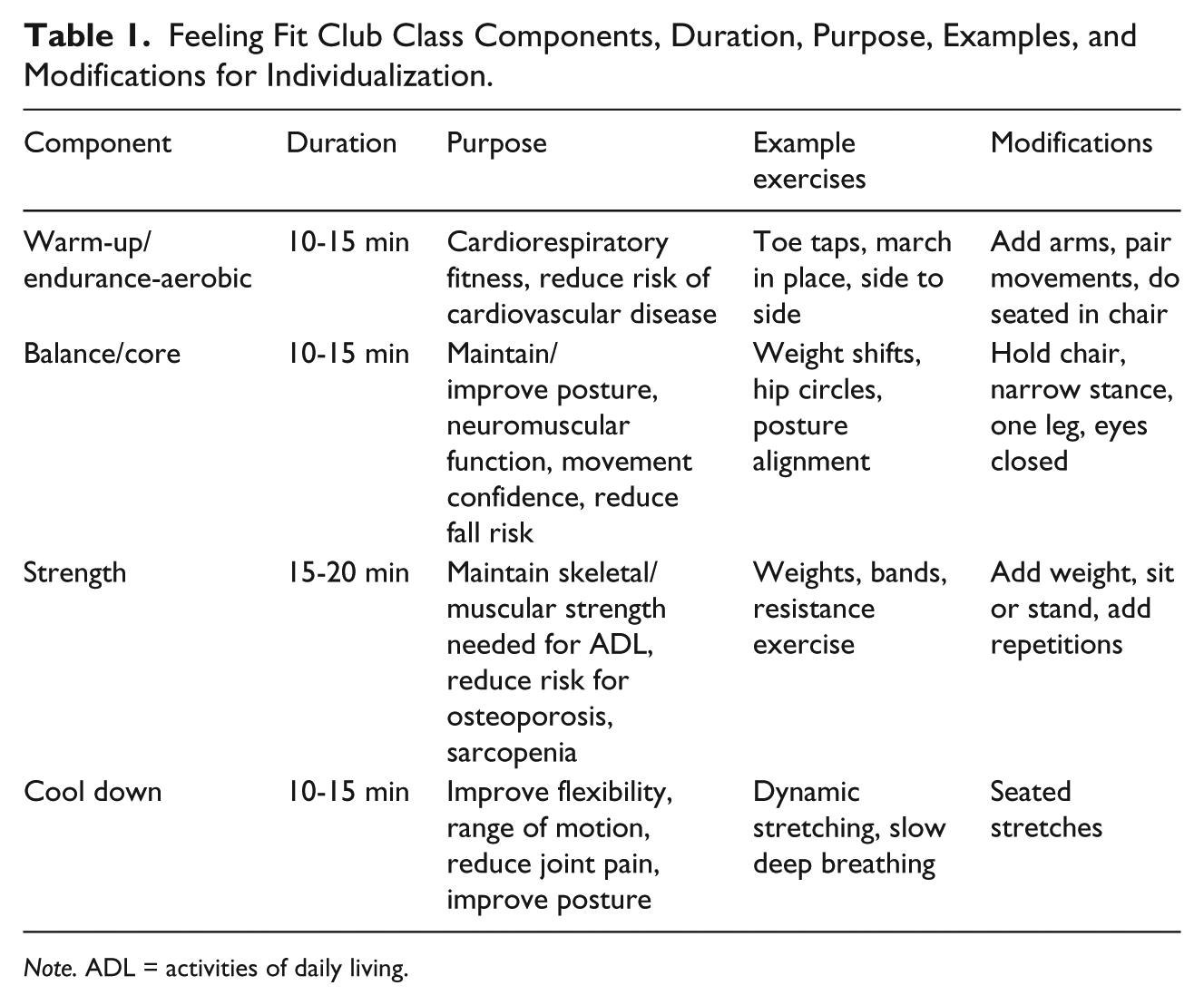
Note. ADL = activities of daily living.
Data Analyses
To test the hypothesis that FFC participants would show improved physical and activity-related function compared with those in the control group 2 (group) × 2 (time) mixed design ANOVAs were conducted. Baseline scores were evaluated for differences using one-way ANOVA. If present, data were were analyzed covarying for baseline values. Data for each variable of interest were initially examined for normality using standardized skewness and kurtosis and outliers (>3.3 SD units from mean) were removed from the analysis. When this approach did not satisfactorily address normality issues, data were log-transformed prior to analysis (Tabachnick & Fidell, 2001). Alpha was set at .05 for tests of significance. Follow-up to significant interactions included simple nested comparisons using the Bonferroni correction to protect against an inflated Type I error rate. Study completers were defined as completing measures at both time points for both groups. For the FFC group study completion was defined as attending 66% or more of all classes (Hawley-Hague, Horne, Skelton, & Todd, 2016; Sherrington, Tiedemann, Fairhall, Close, & Lord, 2011). Study completers were compared with noncompleters on demographic variables using independent samples t tests and chi-square analyses, as appropriate.
Results
Baseline characteristics for FFC and control participants are found in Table 2. Data for 110 FFC participants (83% of initial group) and 110 control participants (85% of initial group) completing measures at baseline and 3 months were compared in the main analysis. No significant differences (p > .05) were found in age, gender, ethnicity, education, or marital status in study completers and noncompleters in either the FFC or control group. No significant differences (p > .05) were found in age, gender, education, or ethnicity between FFC and controls. Significant differences (p < .001) were found in marital status. A greater percentage of FFC participants than controls reported being married or living together. Baseline and 3-month scores for physical function measures, ADL, and self-efficacy for FFC and control participants are found in Table 3.
Baseline Characteristics (M [SD or %]) of Feeling Fit Club and Control Participants With Study Completer/Noncompleter Comparisons.
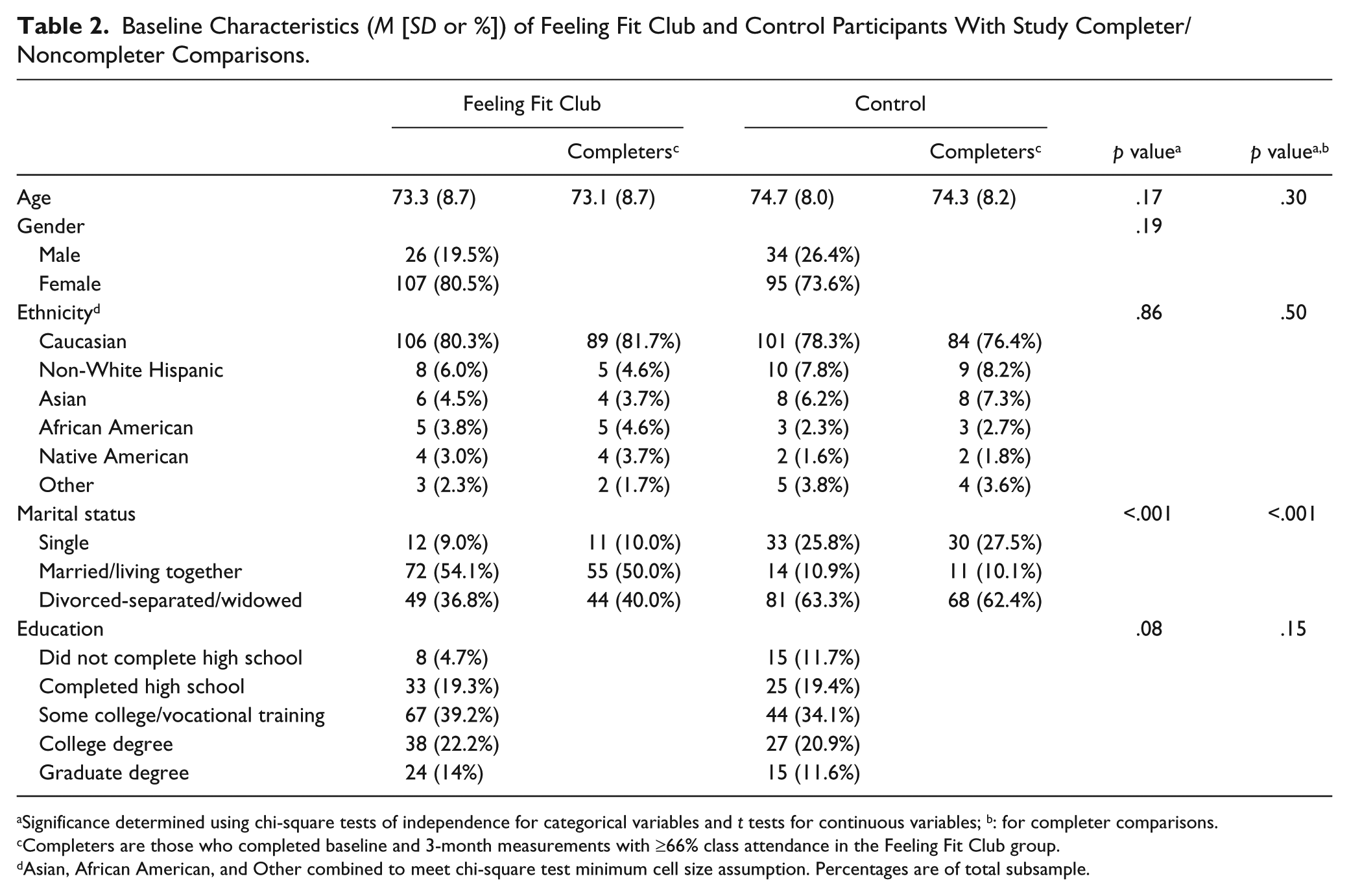
Significance determined using chi-square tests of independence for categorical variables and t tests for continuous variables; b: for completer comparisons.
Completers are those who completed baseline and 3-month measurements with ≥66% class attendance in the Feeling Fit Club group.
Asian, African American, and Other combined to meet chi-square test minimum cell size assumption. Percentages are of total subsample.
Means (Standard Deviation) and Change for Physical function, Balance, Activities of Daily Living, and Exercise Self-Efficacy for Feeling Fit Club and Control Participants.
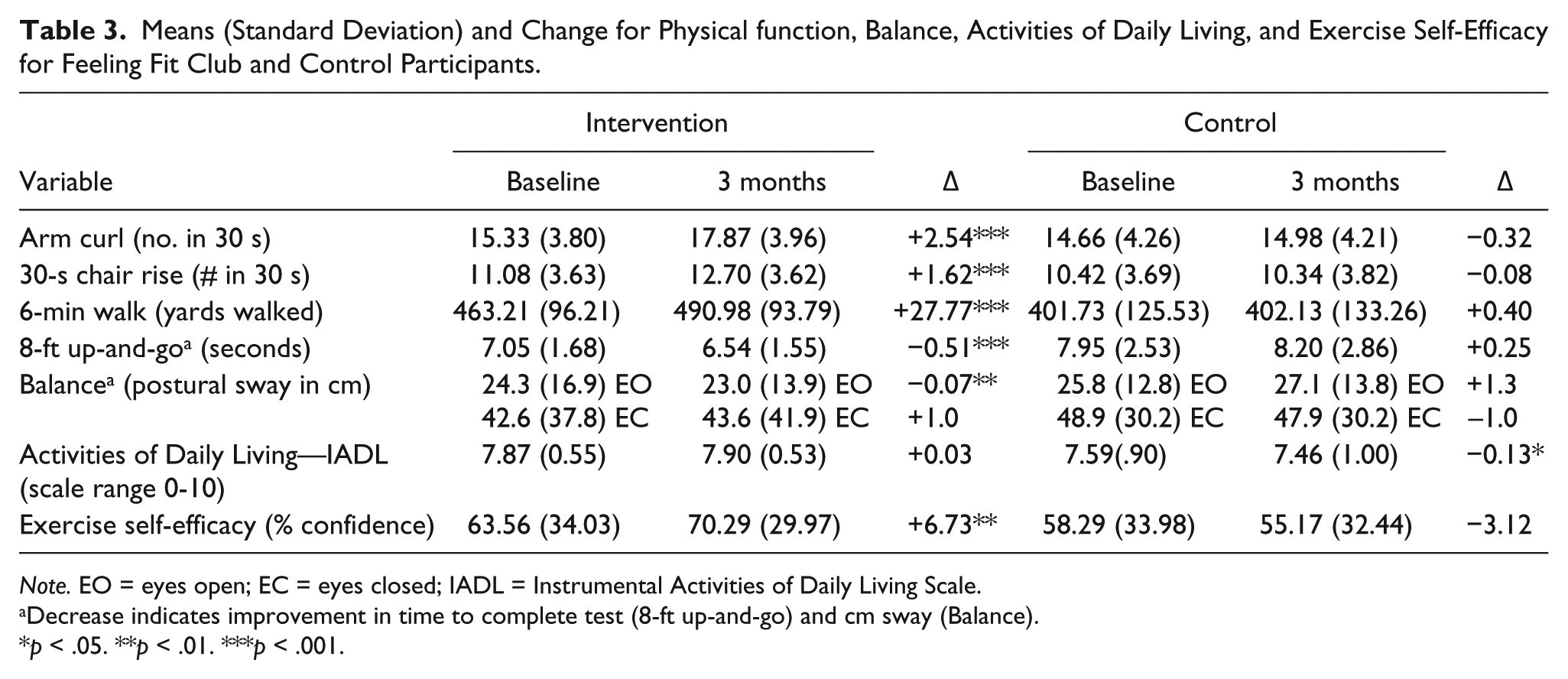
Note. EO = eyes open; EC = eyes closed; IADL = Instrumental Activities of Daily Living Scale.
Decrease indicates improvement in time to complete test (8-ft up-and-go) and cm sway (Balance).
p < .05. **p < .01. ***p < .001.
Arm Curl
Four outliers were identified (>3.3 SD units from the mean) at baseline (FFC, n = 3; Control, n = 1) and were removed from the analysis. A significant Group × Time interaction was found, F(1, 214) = 17.73, p < .001, as well as significant main effects for time, F(1, 214) = 29.47, p < .001, and group, F(1, 214) = 13.18, p < .001. Follow-up analyses revealed significant improvements in arm curl performance in the FFC group, F(1, 106) = 51.89, p < .001, η2 = .33, but not in the controls, F(1, 108) = .67, p > .41, η2 = .01.
30-Second Chair Rise
A significant Group × Time interaction was found, F(1, 218) = 20.29, p < .001, as well as significant effect for time, F(1, 218) = 16.57, p < .001, and group, F(1, 218) = 10.80, p < .002. Follow-up analyses revealed significant improvements in chair-rise performance in the FFC group, F(1, 109) = 32.77, p < .001, η2 = .23, but not in the controls, F(1, 109) = .11, p > .74, η2 = .001.
8-ft Up-and-Go
Scores for the 8-ft up-and-go were nonnormal for both the FFC and control groups at baseline and 3 months. Outliers (>3.3 SD units from mean) were identified in both the FFC (n = 3) and control (n = 4) groups. Removal of the outliers resulted in standardized skewness and kurtosis values ranging from 3.4 to 8.09, and 0.29 to 10.87, respectively. Therefore, prior to analysis, log natural values of the 8-ft up-and-go scores were calculated and effectively brought data into the normal range prior to analysis. To control for significant differences (p < .05) found in baseline scores, these were entered as a covariate. A significant Group × Time interaction was found, F(1, 209) = 29.38, p < .001, as well as significant main effects for time, F(1, 209) = 8.00, p < .01; and group, F(1, 209) = 20.59, p < .001. Follow-up analyses revealed significant improvements in 8-ft up-and-go performance in the FFC group, F(1, 105) = 25.28, p < .001, η2 = .19, but not in the control group, F(1, 105) = 2.99, p > .08, η2 = .03.
Six-Minute Walk
A significant Group × Time interaction was found, F(1, 213) = 15.53, p < .001, as well as significant main effects for time, F(1, 213) = 20.40, p < .001, and group, F(1, 213) = 15.53, p < .001, covarying for baseline values to control for significant group differences (p < .05) in baseline scores. Follow-up analyses revealed significant improvements in distance walked in the FFC group, F(1, 106) = 19.62, p < .001, η2 = .16, but not in the controls, F(1, 108) = .003, p > .95, η2 = .00.
Balance
A significant Group × Time interaction was revealed in the eyes-open condition, F(1, 153) = 5.50, p < .006. No significant main effects for time, F(1, 153) = .34, p > .70, or group, F(1, 153) = 3.68, p > .11, were found. Follow-up analyses indicated significant balance improvements in the FFC group, F(1, 70) = 4.40, p < .01, η2 = .06, but not in the control group, F(1, 83) = 1.56, p > .14, η2 = .03. For the eyes-closed condition, no significant interaction, F(1, 153) = .958, p > .76, or main effects for time, F(1, 153) = .54, p > .64, or group, F(1, 150) = .89, p > .20, were found.
ADL
After controlling for significant (p < .05) baseline differences in IADL scores, a significant Group × Time interaction was found, F(1, 216) = 8.27, p < .005. A significant main effect for time, F(1, 216) = 13.96, p < .001, and group, F(1, 216) = 8.26, p < .001, were also found. Follow-up analyses indicated no significant changes in IADL for the FFC group, F(1, 108) = .60, p > .44, η2 = .01, and significant decreases in IADL scores in the control group, F(1, 109) = 4.03, p < .05, η2 = .04.
Exercise Self-Efficacy
A significant Group × Time interaction, F(1, 202) = 7.95, p < .006, and significant group effect, F(1, 202) = 5.83, p < .02, were found. No significant main effect for time was found, F(1, 202) = 1.07, p > .30. Follow-up analyses indicated significant improvements in exercise self-efficacy in the FFC group, F(1, 102) = 7.40, p < .009, η2 = .07, and no change in the control group, F(1, 100) = 1.60, p > .20, η2 = .01.
Discussion
The current findings support the efficacy of the FFC community-delivered exercise program in improving physical function, independence-related ADL, and exercise self-efficacy. Compared with controls, those participating in FFC significantly improved in upper and lower body strength, mobility, aerobic endurance, balance (eyes-open, but not eyes-closed), and exercise self-efficacy. Improvements seen in FFC participants’ physical function were also meaningful as reflected in the variance accounted for over time (Vacha-Haase & Thompson, 2004). No significant differences were found in self-reported performance of ADL in the FFC participants; however, significant declines in ADL were reported by the controls.
Improvements in physical function have been reported in a variety of group exercise programs delivered to older adults (Callahan et al., 2008; Messier et al., 2004; Pahor et al., 2006). Few community-based and disseminated programs have been evaluated in controlled studies using both physical measures of function and self-report measures related to physical independence. EnhanceFitness was evaluated in a randomized control trial using self-reported SF-36 measures of physical function with participants reporting significant improvements in seven of the SF-36 subscales including physical role-limitation and general health perceptions but not overall physical function when compared with controls (Wallace et al., 1998). Although not widely disseminated, the Fit and Firm program comprised of structured exercise classes in conjunction with recommended home exercise (latter focused on brisk walking) resulted in chair-rise improvements over a 1-year period similar to those of the current study (Δ+1.4, women; Δ+1.1, men), though not significantly different from those engaged in a stretching program (King et al., 2000).
Several evidence-based programs have incorporated physical measures into effectiveness studies evaluating program dissemination in community settings. EnhanceFitness (Belza et al., 2006) and Active Living Every Day (Baruth et al., 2011) demonstrated significant improvements over time similar to those seen in the current study. Using three physical measures of function Belza and colleagues (2006) reported participant improvements at 4 months for the arm curl (Δ = 2.5), chair stand (Δ = 1.6), and 8-ft up-and-go (Δ = −0.4 s). Participants in Active Living Every Day, a part of Active Life®, similarly improved chair stand (Δ = 1.4) and 8-ft up-and-go times (Δ = −0.4 s; Baruth et al., 2011).
Few studies compared balance changes in response to exercise intervention with older adults using an objective measure of balance. A wide degree of variability exists in the types of measures used to assess balance changes in response to exercise interventions in older adults (Lewis, Peiris, & Shields, 2017). Both Tai-chi and a community-based balance-specific exercise programs improved static balance as measured using Biodex in an eyes-closed condition but not eyes open (Zhao, Chung, & Tong, 2016). Although the current study did see improvement in both balance conditions in the FFC group, neither of these changes exceeded recently established minimal detectable change values for the BTrackS (Levy et al., 2016). It is possible that longer periods of time are needed to see clinically meaningful changes in balance. Improvements in physical function but not balance have been reported for exercise programs of similar duration (Jorgensen et al., 2013; Mulligan, Tschoepe, & Smith, 2014). Participants in the current study were also generally healthy and variability in balance was high. Yet, most participants demonstrated postural sway below force plate determined values associated with high fall risk (Merlo et al., 2012). Thus, ceiling effects may have been an issue. Future work with individuals at greater risk for falls may reveal more meaningful balance improvements.
Interestingly, while objectively measured physical function significantly improved for FFC participants, self-reported confidence in performance of IADL were maintained over time and significantly declined in the control group. Significant declines in control group IADL compared with nonsignificant improvements in exercise intervention group IADL have been reported in nursing home residents over the same time period (Machacova, Vankova, Volicer, Veleta, & Holmerova, 2017). Similarly, declines in independently living older adults’ self-reported IADL over a 3-month period have been reported in those judged to be potentially “at risk” for functional decline based on visits to hospital emergency rooms over the previous year, with no hospital admission (Grimmer, Beaton, & Hendry, 2013). This finding is particularly telling and provides further evidence that programs like FFC are instrumental in healthy aging and avoiding ADL declines related to loss of physical independence (Covinsky et al., 2003; Penninx et al., 2001). The FFC program aligns with healthy aging recommendations for physical activity interventions for older adults, including attention to social support and exercise self-efficacy. Significant improvements in exercise self-efficacy were reported in the FFC but not controls and have been linked to exercise maintenance in older adults (King, 2001; McAuley et al., 2003; McAuley et al., 2011; Schutzer & Graves, 2004). In addition, instructors were trained to emphasize improvement and supported the social atmosphere and camaraderie provided in classes.
A strength of the current study was its use of physical measures of function in conjunction with self-report measures of function related to physical independence and exercise self-efficacy. Although self-report of physical function is widely used, physical measurement of function is important and may be preferable in assessment of some activities related to physical independence (Stratford, Kennedy, Pagura, & Gollish, 2008). Using both physical and self-report measures provides both stronger evidence of FFC efficacy than either alone and a stronger foundation from which to proceed to effectiveness studies of wider program dissemination.
There are limitations of the current study as well. Participants were generally healthy, ambulatory, and screened for physical activity readiness. Generalizing findings to individuals at high risk for falls such as nursing home or assisted-living residents should only be done with caution. As with many community-based exercise programs, the goal of FFC is to maintain physical independence among those currently independent. Future studies should examine how such programs might be best implemented with those in other contexts. Similarly, the majority of our sample was Caucasian; future studies should be conducted in more ethnically diverse samples. Finally, differences in motivation for physical activity may have existed between the FFC and control groups. However, physical activity itself was not an outcome, and no baseline differences in exercise self-efficacy were found suggesting motivational differences were not a factor in the outcomes of interest.
Increasing the number of evidence-based programs that have high potential for wide dissemination and translation to community settings is critical to healthy aging initiatives. Translation of instructor-led exercise programs into widespread community use is challenging, and can be limited by adequate space and equipment needs (Shubert, Apeter, & Busby-Whitehead, 2011; Williams & Ullmann, 2012). The FFC program demonstrated efficacy in improving physical function and measures related to maintaining physical independence, a key feature of healthy aging (Penninx et al., 2001; Prohaska et al., 2006). By design, FFC is efficient in both space and equipment need and has been successfully disseminated in multiple sites (>25) in a single county. Future studies should examine its effectiveness in broader dissemination as its characteristics suggest a strong probability of successful implementation by a wide range of community and state health organizations.
Footnotes
Authors’ Note
Daniel Goble is now affliated to Oakland University, Rochester, MI, USA. This study was approved by the San Diego State University institutional review board (IRB): Protocol 1655093.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: No conflicts of interest exist for Susan S. Levy, Katie J. Thralls, Taylor B. Krippes. Daniel J. Goble has an equity stake (i.e., stock options) in the parent company for the BTrackS device used to measure balance in this study. This conflict of interest was managed by Dr. Goble’s noninvolvement in all aspects of data collection and analyses.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.