
Abstract
We aimed to understand the relationships between care recipients’ profiles and home- and community-based services (HCBS use patterns. Data were from the 2010 to 2013 Long-Term Care Service Management System in Taiwan (N = 78,205). We used latent class analysis and multinomial logistic regression analyses. Three HCBS use patterns were found. Care recipients who lived alone, lived in less urbanized areas, and had instrumental activities of daily living disabilities were more likely to be in the home-based personal care group. Those in the home-based personal and medical care group were more likely than others to have a primary caregiver. Care recipients who had poorer abilities at basic activities of daily living and cognitive function, better household income, and lived in a more urbanized area were more likely to be in the non-personal care multiple services group. The findings suggest that policymakers alleviate barriers to accessing various patterns of HCBS should be encouraged.
Introduction
The proportion of Taiwan’s population aged 65 years and older increased by 30% in the past decade, from 10.21% in 2007 to 13.55% in 2017 (Ministry of the Interior in Taiwan, 2017). In 2007, a landmark year when the proportion of older people in Taiwan first surpassed 10%, the government introduced the National 10-Year Long-Term Care Plan (10-Year LTC Plan). The 10-Year LTC Plan is a government-subsidized action plan which provide home- and community-based services (HCBS) that would help older people age in place (Ministry of Health and Welfare in Taiwan, 2007). Under the 10-Year LTC Plan, between 2008 and 2016, the number of people using personal care services doubled and the number of people using adult day care services increased 10-fold (Ministry of Health and Welfare in Taiwan, 2016).
HCBS are services provided to older adults in their home and community, rather than in nursing homes or other institutional long-term care facilities. Studies have shown that the benefits of HCBS include delaying institutionalization and preventing hospitalization among older people (Gaugler, Kane, Kane, & Newcomer, 2005; Segelman et al., 2014; Tomita, Yoshimura, & Ikegami, 2010). Yet researchers have suggested that a better understanding of the profiles of care recipients and the patterns of the services they receive would help the long-term care system deliver services more efficiently (L. F. Liu & Yao, 2014). Generally, older people with severe physical dysfunction have been found more likely to use home-based services, due to their mobility limitations. Older people who live in urban areas have used more community-based services, which are more accessible in urban than rural areas (Beeber, Thorpe, & Clipp, 2008; Dabelko & Balaswamy, 2000). However, patterns of use of long-term care services and the profiles of HCBS care recipients in Taiwan are still not clear to researchers or policy makers.
Andersen’s Behavioral Model of Health Services Use provides a conceptual framework for simplifying the multiple factors that influence individuals’ health care use (Andersen, 1968, 1995). Predisposing factors, including personal characteristics such as gender and household membership, have been found to affect older adults’ HCBS use (Borrayo, Salmon, Polivka, & Dunlop, 2002; Lehning, Kim, & Dunkle, 2013). Researchers have suggested that need factors play an important role in determining service use, including use of health services (Al Snih et al., 2006) and long-term care services (Borrayo et al., 2002; Kempen & Suurmeijer, 1991; Park, 2015). Enabling factors have also been found to have an impact on different types of HCBS use by older adults (Beeber et al., 2008; Lehning et al., 2013).
The initial version of the 10-Year LTC Plan in Taiwan has now been in place for 10 years, yet research on the relationships between care recipients’ profiles and those recipients’ HCBS use has been limited (L. F. Liu & Yao, 2014). However, one of the criticisms of the plan has been fragmented services: most users reported unmet need due to lack of flexibility in service delivery (Ministry of Health and Welfare in Taiwan, 2016). In 2017, a new long-term care policy, referred to as the National 10-Year LTC Plan Version 2.0, began. It emphasizes developing integrated HCBS and encouraging disabled people who live in the community to use multiple HCBS services (Ministry of Health and Welfare in Taiwan, 2016). An understanding of care recipients’ profiles and HCBS use patterns under Taiwan’s first National 10-Year LTC Plan can provide practical guidelines for the Version 2.0 plan. This study aimed to (a) identify the different patterns of HCBS use among Taiwanese care recipients and (b) understand the relationships between these care recipients’ profiles and their HCBS use.
Method
In the current study, we adopted Andersen’s Behavioral Model of Health Services Use as a guide for selecting variables. We then applied latent class analysis to examine the associations among care recipients’ profiles and their HCBS use patterns, using national data from the National 10-Year LTC Plan in Taiwan. Data were from Long-Term Care Service Management System and were provided by the Ministry of Health and Welfare in Taiwan (2010-2013). The Long-Term Care Service Management System is an online system that collected both evaluation and prescribed service information for those who received care through the National 10-Year LTC Plan. The information was collected by case managers who were well-trained specialists and who took responsibility for evaluating care recipients, prescribing long-term care services, and reassessing the care recipients’ information every 6 months regularly. Detailed information about delivering the National 10-Year LTC Plan in Taiwan can be found in past study (L. F. Liu & Yao, 2014; Ministry of Health and Welfare in Taiwan, 2010).
The evaluation section of Taiwan’s Long-Term Care Service Management System includes care recipients’ demographics, socioeconomic status, level of disability in basic activities of daily living (BADL) and in instrumental activities of daily living (IADL), and physiological and psychosocial status. The prescribed service section of the Long-Term Care Service Management System includes the long-term care services prescribed for each care recipient. This prescription is based on case manager’s evaluation and care recipients’ and/or caregivers’ agreement to the plan. Final agreement on a services plan is therefore based not only on the objective evaluation of care needs and other potential environmental factors external to the care recipient but also on the preferences of the care recipient and/or caregivers. Our study extracted baseline evaluation information, which was the first time care recipients were assessed and prescribed HCBS, to examine the relationship between the care recipients’ profiles and their prescribed services. We excluded those care recipients whose data included only their prescribed HCBS but no demographic information (due to incomplete records in the national data set). To avoid potential systematic bias, we compared patterns of prescribed HCBS for the group of care recipients with available demographic information and those without. We found no significant differences in HCBS patterns between these two groups of people. As a result, we included 78,205 recipients for analysis in the study.
The HCBS offered through Taiwan’s National 10-Year LTC Plan included personal care services, adult day care services, home-based respite care, institution-based respite care, visiting nurses, home-based rehabilitation, and transportation. Institution-based respite care is a kind of HCBS services in Taiwan which offers short-term stay in an institution if caregivers need respite care. For analysis, each service was dichotomized as either use (1) or no use (0). Predisposing factors considered for the care recipients were age, gender, living alone (1) or with other people (0), and having (1) or not having (0) a primary caregiver.
Household economic status and the degree of urbanization of the town in Taiwan where the care recipient lived were considered enabling factors. Household economic status was categorized as low-income (1), low- to middle income (2), and regular-income (3). In Taiwan, levels of household income are measured by dividing the joint household income by the number of persons living in the household. On average, a household with a monthly income range of US$340 to US$520 per person is categorized as a low-income family, whereas a family with a monthly income range of US$520 to US$740 per person is categorized as a low- to middle-income family (Ministry of Health and Welfare in Taiwan, 2017). Degree of urbanization was classified into seven levels (1-7), with higher numbers representing a greater degree of urbanization (C. Y. Liu et al., 2006). Data on both household income level and degree of urbanization were collected from the evaluation section of Taiwan’s Long-Term Care Service Management System.
The care recipients’ need factors were assessed by four indicators. First, the number of comorbidities (0-18), counted as the presence or absence of 18 disorders (hypertension, diabetes mellitus, heart disease, stroke, gastrointestinal disease, chronic obstructive pulmonary disease, renal disease, spinal cord injury, musculoskeletal disorder, urinary tract infection, Parkinson’s disease, immune disorder, dementia, communicable diseases, cancer, pulmonary disease, cerebral palsy, and other disease). Second, the Barthel Index score (0-100), which represents ability in BADL, such as eating, transferring from bed to chair, grooming, bathing, managing indoor mobility, going up and down stairs, dressing, toileting, and managing bowels and bladder incontinence (Mahoney & Barthel, 1965). Third, eight items assessing IADL capability (scores of 0-24), including shopping, transportation, preparing meals, housekeeping, doing laundry, using the telephone, taking medicine, and managing finances. Fourth, a cognitive health score (1-4) as assessed by the Short Portable Mental Status Questionnaire. Higher BADL, IADL, and cognitive health scores represented better physical and mental function in care recipients.
Latent class analysis was used to specify the underlying subgroups of care recipients in the National 10-Year LTC Plan who were following similar patterns of HCBS use. Latent class analysis is a model-based approach to clustering individuals into distinctive groups, based on their responses to a set of selected variables. The determination of service users in a given HCBS subgroup is based on a set of indicators (in our study: personal care services, adult day care, home-based respite care, institution-based respite care, visiting nurses, home-based rehabilitation, and transportation). Latent class analysis identifies subgroups based on estimated posterior membership probabilities (Collins & Lanza, 2010). Goodness of fit indices, such as the Bayesian information criteria (BIC) and entropy, has been suggested for testing the optimal number of latent classes in a model: a lower BIC value represents a better model fit, and entropy with values approaching 1 indicates better latent class separation (Collins & Lanza, 2010). The software package used for this analysis was Mplus Version 7 (Muthén & Muthén, 1998-2012). In addition, we confirmed the best solution of the subgroup memberships (first determined by the latent class analysis statistical approach) based on conceptually reasonable HCBS categories summarized in textbooks on home-based and community-based services (Kane, Kane, & Ladd, 1998).
To examine the association of care recipient profiles with the subgroups based on HCBS use, we conducted a series of hierarchical multinomial logistic regression analyses and estimated the odds ratio (OR) and the 99.9% confidence interval (CI) for each variable in the equation. This was done due to the study’s large sample size. We chose hierarchical multinomial logistic regression to test the impact of predisposing, enabling, and need factors independently from one another, based on the conceptual framework in Andersen’s Behavioral Model (Andersen, 1968, 1995). Multiple imputations were applied for missing data, as recommended for dealing with missing survey data (Rubin, 2004). For the multiple imputation analyses and the regression analyses, we used SAS software, Version 9.2, of the SAS System for PROC LOGISTIC and PROC REG (SAS Institute Inc., Cary, NC, USA).
Results
We specified between two and four latent classes to identify the different subgroups of care recipients by the pattern of their HCBS use. The BIC values declined fairly steadily as the number of classes increased, with values of 498,852.62 (two classes), 491,715.50 (three classes), and 485,138.13 (four classes). Entropy was highest with three classes, at 0.835, compared with 0.681 in two classes and 0.796 in four classes. To choose the optimal number of latent classes, we considered both BIC and entropy indices, as well as reasonable explanations for each of the patterns of HCBS use in the distinct subgroups, and determined that the best model included three classes of HCBS users in Taiwan.
Table 1 and Figure 1 show the patterns of HCBS use among three subgroups of care recipients. Most of the recipients (n = 41,336; 52.86%) were identified in a group named for home-based personal care (home-based PC) services. The group identified by home-based personal and medical care (home-based PC/MC) was the smallest (n = 16,583; 21.20%), whereas the non-personal care multiple services (non-PC multiple services) group was in the middle (n = 20,286; 25.94%). Home-based PC refer to services with non-skilled daily tasks, such as performing BADL and IADL, whereas home-based medical care services are skilled help provided by medical professionals in care recipients’ home, examples include rehabilitative training provided by physical or occupational therapists and skilled nursing provided by visiting nurses. All care recipients in both the home-based PC and home-based PC/MC groups had high use of personal care services. However, care recipients in the home-based PC/MC group used more medical related services, such as visiting nurses (n = 5,725; 34.25%) and home-based rehabilitation (n = 9,255; 55.81%), in addition. Care recipients in the non-PC multiple services group used multiple HCBS, but none of the recipients in this group used personal care services. Older recipients identified in the non-PC multiple services group had the highest percentage of receiving adult day care (n = 2,315; 11.41%) among three HCBS-use subgroups.
Long-Term Care Services Used by Three Subgroups of Care Recipients in Taiwan (N = 78,205).
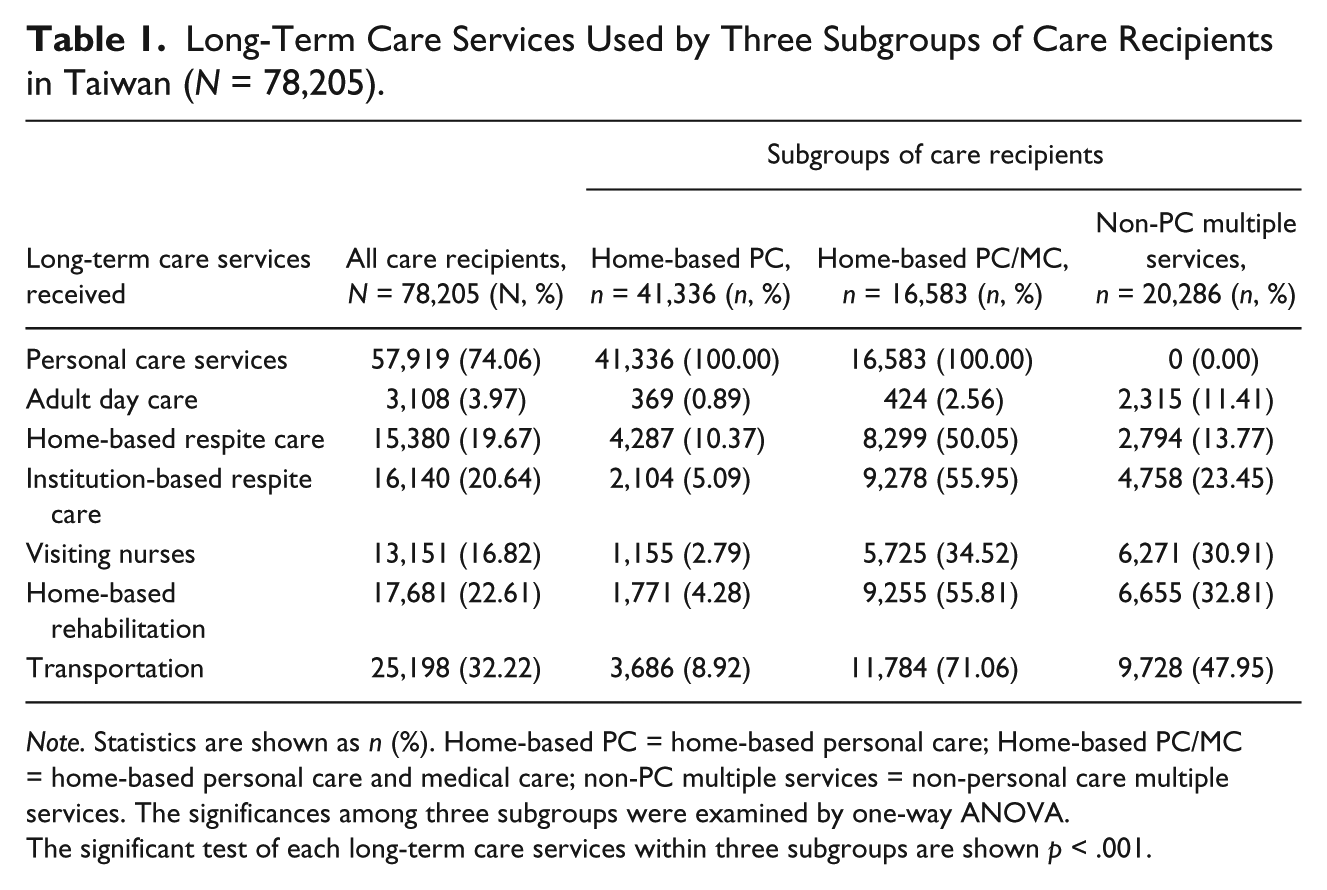
Note. Statistics are shown as n (%). Home-based PC = home-based personal care; Home-based PC/MC = home-based personal care and medical care; non-PC multiple services = non-personal care multiple services. The significances among three subgroups were examined by one-way ANOVA.
The significant test of each long-term care services within three subgroups are shown p < .001.
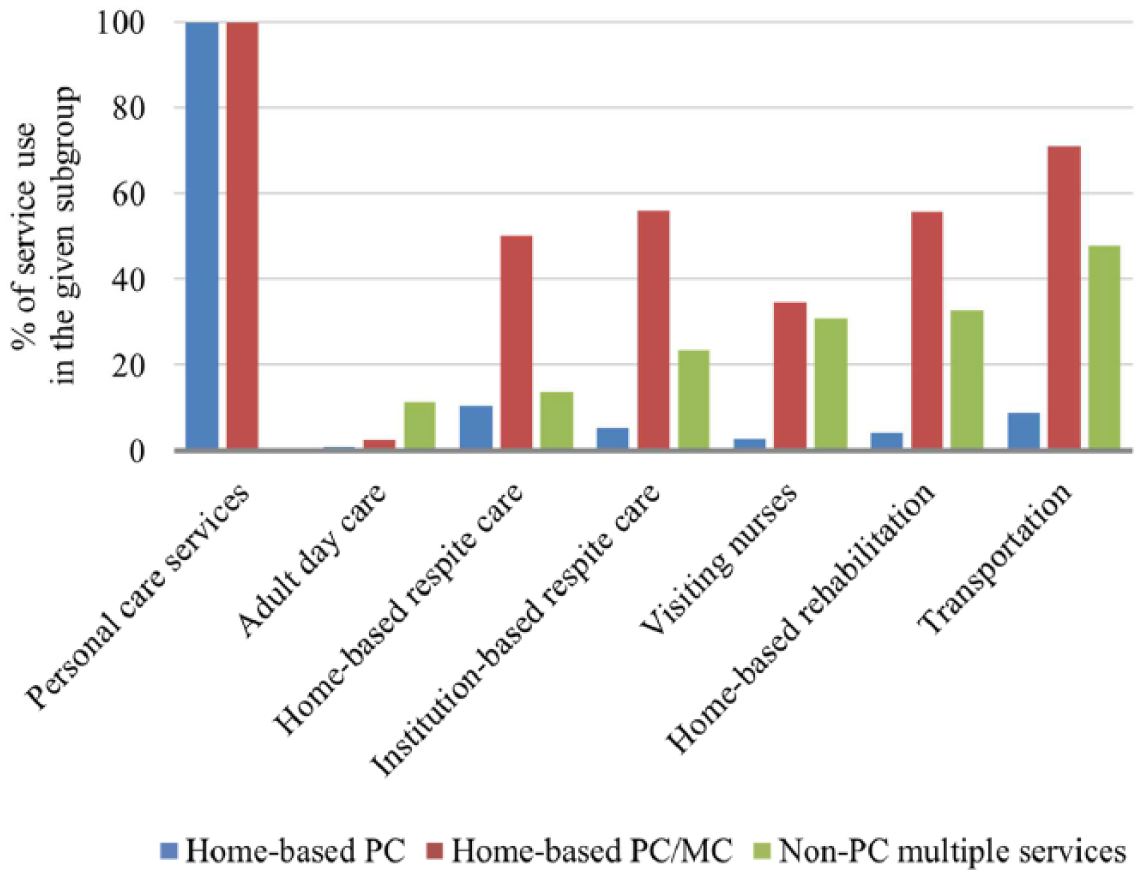
Long-term care services used by three subgroups of care recipients in Taiwan.
Table 2 shows the descriptive data of care recipients’ profiles among three HCBS use subgroups in Taiwan. For predisposing factors, the mean age of all care recipients was 79.52 years (SD = 7.95) with the highest age found in the non-PC multiple services group (M = 80.36 years; SD = 8.00). Female care recipients were the majority in all the three subgroups, with the highest percentage of females found in the home-based PC group (n = 24,151; 58.43%). The percentage of care recipients who lived alone was also highest in the home-based PC group (n = 10,781; 26.08%). Care recipients who had a primary caregiver were more likely to be in the home-based PC/MC group (n = 15,999; 96.48%) and non-PC multiple services group (n = 19,004; 93.68%). For enabling factors, care recipients in the non-PC multiple services group had the highest level of both household economic status (M = 2.86; SD = 0.46) and degree of urbanization (M = 5.24; SD = 1.63). For need factors, care recipients in the home-based PC/MC group had the highest number of comorbidities (M = 3.36; SD = 1.46) compared with the other two groups. However, care recipients in the home-based PC group showed the highest scores in the Barthel Index, IADL ability, and cognition, which indicated that these older adults had better physical and mental health than those in the other two groups.
Profile Factors of Three Subgroups of HCBS Care Recipients in Taiwan (N = 78,205).
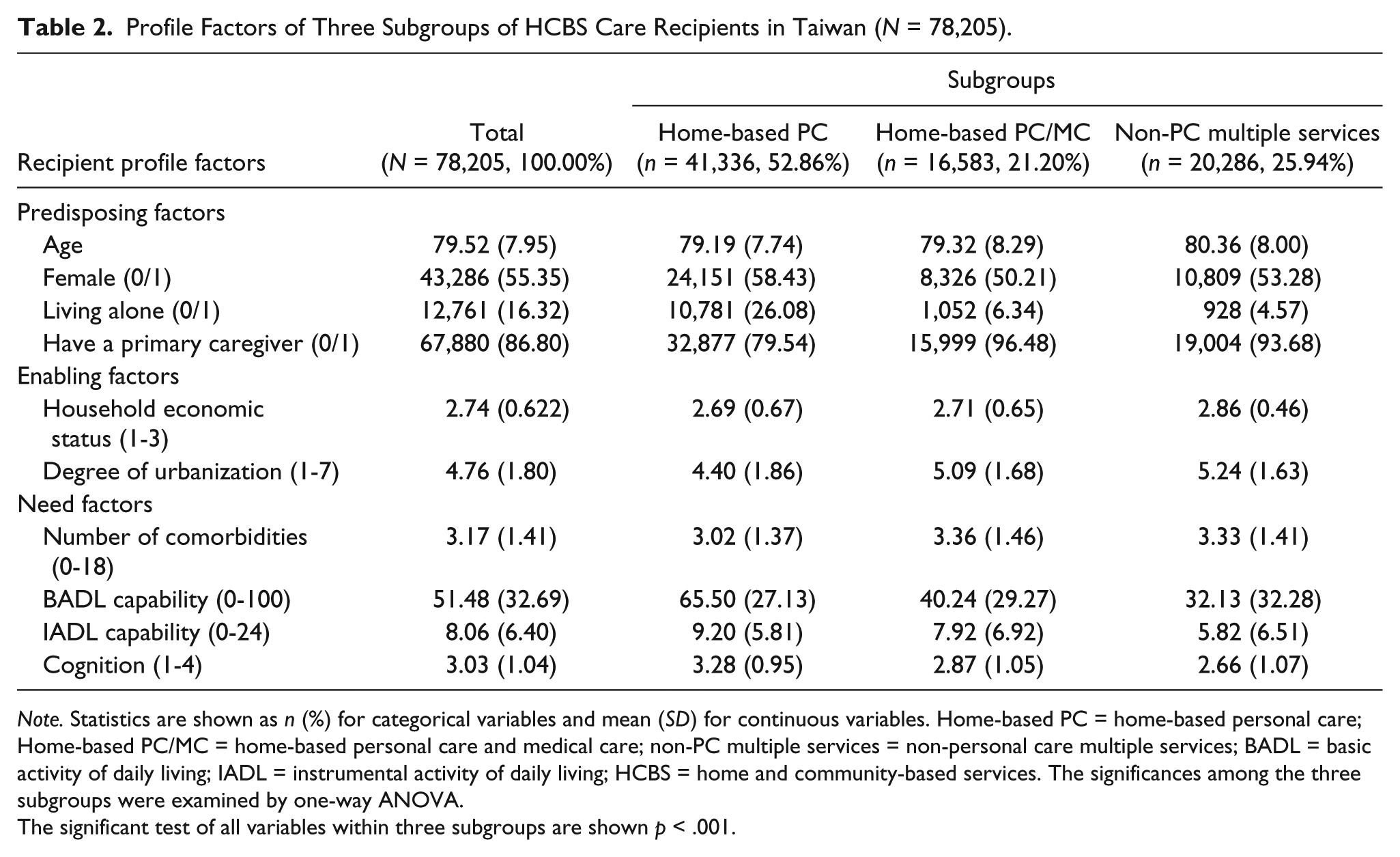
Note. Statistics are shown as n (%) for categorical variables and mean (SD) for continuous variables. Home-based PC = home-based personal care; Home-based PC/MC = home-based personal care and medical care; non-PC multiple services = non-personal care multiple services; BADL = basic activity of daily living; IADL = instrumental activity of daily living; HCBS = home and community-based services. The significances among the three subgroups were examined by one-way ANOVA.
The significant test of all variables within three subgroups are shown p < .001.
Table 3 shows the associations found between the predisposing, enabling, and need factors in the three subgroups of HCBS care recipients in Taiwan. In Model 1, we included only the predisposing factors, and this explained about 11.92% of the variance in the model. In Model 2, we added enabling factors to Model 1, and the enabling factors accounted for an additional 39.51% ([0.1663 − 0.1192] / 0.1192) of the variance from Model 1. In Model 3, need factors were added to Model 2 and found to account for 89.12% ([0.3145 − 0.1663] / 0.1663) of the variance in Model 2. The results of the regression analysis in Model 3 showed differences between the three subgroups in predisposing, enabling, and need factors. For this analysis, the home-based PC group was set as the reference group.
Relationships Among Predisposing, Enabling, and Need Factors and the Three Subgroups of HCBS Care Recipients in Taiwan (N = 78,205).

Note. Statistics are shown as OR [99.9% CI]. Home-based PC = home-based personal care; Home-based PC/MC = home-based personal and medical care; non-PC multiple services = non-personal care multiple services; HCBS = home and community-based services; BADL = basic activity of daily living; IADL = instrumental activity of daily living; OR: odds ratio; CI: confidence interval. The home-based PC group was set as the reference group in the multinomial logistic regression.
The significant level of significance was set as .001.
The relationships among predisposing, enabling, and need factors and the three subgroups of HCBS care recipients in Taiwan are shown in Table 3. For predisposing factors, when compared with the home-based PC group, the care recipients in both the home-based PC/MC group and the non-PC multiple services group were more likely to be males (OR = 0.786, CI = [0.736, 0.840] in home-based PC/MC; OR = 0.887, CI = [0.831, 0.947] in non-PC multiple services), live with a family member (OR = 0.508, CI = [0.448, 0.577] in home-based PC/MC; OR = 0.397, CI = [0.348, 0.454] in non-PC multiple services), and have a primary caregiver (OR = 3.472, CI = [2.960, 4.072] in home-based PC/MC; OR = 1.268, CI = [1.114, 1.444] in non-PC multiple services).
For enabling factors, recipients in both the home-based PC/MC group and the non-PC multiple services group were more likely than the home-based PC group to live in towns with higher urbanization scores (OR = 1.241, CI = [1.217, 1.265] in home-based PC/MC; OR = 1.281, CI = [1.257, 1.306] in non-PC multiple services). However, the care recipients in the home-based PC/MC group had lower levels of household economic status (OR = 0.879, CI = [0.834, 0.927]) than the home-based PC group, whereas the recipients in the non-PC multiple services group had higher household economic status (OR = 1.408, CI = [1.323, 1.499]).
For need factors, compared with those in the home-based PC group, the care recipients in both the home-based PC/MC and the non-PC multiple services groups had higher numbers of comorbidities (OR = 1.108, CI =[1.082, 1.134] in home-based PC/MC; OR = 1.064, CI = [1.010, 1.089] in non-PC multiple services), worse BADL function (OR = 0.974, CI = [0.973, 0.975] in home-based PC/MC; OR = 0.970, CI = [0.968, 0.971] in non-PC multiple services), and worse cognitive status (OR = 0.872, CI = [0.841, 0.904] in home-based PC/MC; OR = 0.832, CI = [0.803, 0.861] in non-PC multiple services). We noted that the recipients in both home-based PC/MC and non-PC multiple services groups had better IADL function than those in the home-based PC group (OR = 1.064, CI = [1.058, 1.071] in home-based PC/MC; OR = 1.027, CI = [1.020, 1.033] in non-PC multiple services).
Discussion
This study explored the descriptive profiles of three groups of HCBS care recipients in Taiwan. These recipient groups are being called the home-based PC, home-based PC/MC, and non-PC multiple services groups. The study provides information regarding existing HCBS use patterns in Taiwan as well as useful guidelines for improving integration of HCBS during the National 10-Year LTC Plan Version 2.0. We applied Andersen’s Behavioral Model of Health Services Use and found that need factors played an important role in the association between care recipients’ profiles and HCBS use. Care recipients who lived alone, lived in less urbanized areas, and had IADL disability were more likely to be in the home-based PC group. The recipients in the home-based PC/MC group were more likely to have a primary caregiver compared with those in the home-based PC and the non-PC multiple services groups. Care recipients who had worse BADL and cognitive function but had better household income and lived in areas with a higher degree of urbanization (i.e., Taipei City) were more likely to be in the non-PC multiple services group.
Andersen’s Behavioral Model has been widely used to examine the association of multiple factors with long-term care service use in older adults (Beeber et al., 2008; Borrayo et al., 2002; Kempen & Suurmeijer, 1991; Lehning et al., 2013; Park, 2015). We extended past knowledge and found that these factors played different roles in determining which care recipients used which different kinds of HCBS. Need factors had the most important effect on HCBS use, providing the largest proportion of explanation of the variance in the model. This finding was in line with past studies that found need factors contributed the most variance to the use of long-term care services (Borrayo et al., 2002; Kempen & Suurmeijer, 1991; Park, 2015). Enabling factors, which are related to an individual’s ability to access long-term care services, were also important to care recipients’ choices of home-based or other types of long-term care services in both our study and other studies (Beeber et al., 2008; Lehning et al., 2013). In comparison to a previous study that used health care services as an outcome indicator and found that need factors accounted for the greatest effect on older adults’ use of services (Al Snih et al., 2006), our study highlights the importance of enabling factors in determining whether older adults use home-based or multiple long-term care services in Taiwan.
Care recipients in the home-based PC group were more likely to live alone and had higher levels of IADL disability, yet better BADL and cognitive function, than care recipients in the other two groups. This possibly could be because the Taiwanese government took responsibility for caring for older individuals who lived alone as a social welfare benefit (Ministry of Health and Welfare in Taiwan, 2007), even if those individuals had only mild physical dysfunction (i.e., IADL disability). Another possibility is that care recipients in the home-based PC group were healthier than their counterparts in the other groups and thus more likely to live alone. However, it is important to note that apart from personal care services, care recipients in the home-based PC group were less likely to use other kinds of HCBS. If care recipients in the home-based PC group did have better health status, they might not have needed additional services. It is also possible, however, that they lacked caregivers to help coordinate multiple services.
As the care recipients in the home-based PC group were more likely to live in an area with lower degree of urbanization, it might also contribute their disadvantage in accessing multiple services. Study has shown geographic disparities in disability prevalence among older Taiwanese (Chen, Chou, Lin, Wu, & Lin, 2012). It was noted inequality of delivery of long-term care services among different administrative areas in Taiwan (Ministry of Health and Welfare in Taiwan, 2016). Our study adds to the knowledge that care recipients who live in areas with a lower degree of urbanization are less likely to use multiple services, which shows inequality in long-term care service accessibility. Receipt of multiple care services at home can reduce unnecessary health care utilization and the risk of dying at home for frail older people (Di Pollina et al., 2017), and lack of multiple care services may thus widen the disparity in disability in different geographic areas in Taiwan. Removing such disparities should be a priority for the Taiwanese government, especially, as Taiwan will be facing the challenge of a rapidly aging population in the next couple of decades. Now with the knowledge that older adult with these characteristics might be disadvantaged to access multiple HCBS, it is recommended that future care professionals and case managers should consider promoting multiple services when they work with older adults who lived alone, lived in less urbanized area, and had no primary caregiver. However, how to better coordinate services and not to rely on primary caregivers to coordinate care remains a challenge for the National 10-Year LTC Plan Version 2.0 in Taiwan.
The presence of a primary caregiver played an important role in determining whether the care recipients in this study used medical related HCBS such as visiting nurses and home-based rehabilitation. Informal caregivers, especially, family caregivers in Taiwan, play an important role in coordinating care between care recipients and the formal long-term care system. Family caregivers in Taiwan take responsibility not only for helping individuals perform daily activities but also for managing and coordinating care for their disabled family members within the formal long-term care system (Lu, 2005). Primary caregivers would expect help from medical professionals for care recipients to improve their physical function. Thus, we were not surprised that the care recipients in the home-based PC/MC group, who were likely to have a primary caregiver, also were more likely to use medical related HCBS. Similar findings were reported in another Asian society, Singapore, in a study that also pointed out the critical role of caregivers in determining how care recipients use HCBS (C. Y. Liu, Eom, Matchar, Chong, & Chan, 2016). In addition, better coordination between informal caregivers and formal health care providers has been found to result in better health outcomes of care recipients (Weinberg, Lusenhop, Gittell, & Kautz, 2007). Thus, we strongly recommend future research to investigate the impact of coordination between primary caregivers and formal providers on care recipients’ health outcomes and health care costs in Taiwan, as well as to examine whether formal long-term care services help relieve family caregivers of the burden of caring for their family members.
The older Taiwanese adults who use multiple HCBS in Taiwan tend to live in cities and have a higher level of household economic status. These individuals had relatively high financial resources and greater access to multiple services and were more likely to be found in our non-PC multiple services group, even though their BADL and cognitive function tended to be worse than those of care recipients in the home-based PC and home-based PC/MC groups. Past findings have suggested that enabling factors, such as rural–urban disparities and financial dependency, affect both unmet long-term care need and actual service use in older adults (Beeber et al., 2008; Zhu, 2015). In our study, we also found that during the National 10-Year LTC Plan, the care recipients in the non-PC multiple services group who received adult day care services were not simultaneously prescribed any personal care services. One possibility for this finding was that care recipients who received adult day care services might also have received personal care services at the care center. However, most adult day care centers in Taiwan do not routinely provide personal care, such as bathing services and personal hygiene. We assume that some personal care services would still have to be provided by family caregivers to meet the care recipients’ needs. The current findings suggest that the strategy of combining recommendations for both home-based PC and community-based adult day care services has not yet been developed in Taiwan, despite being common in integrated long-term care models (Morikawa, 2014). The benefits of coordinating provision of both adult day care in a care center and personal help at home should be further investigated in Taiwan.
Compared with the care recipients in the home-based PC and home-based PC/MC groups, older adults in the non-PC multiple services group used a variety of HCBS but no personal care services. This might be due to Chinese filial piety: providing personal support and care for disabled older family members has been a traditional responsibility of Chinese families (Yu, Chen, Chiang, Tu, & Chen, 2015). However, it is important to pay more attention to whether family caregivers become overstressed when care recipients do not have personal care services prescribed for them. A review study has shown that both respite services and psychoeducational programs are useful to family caregivers to relieve burnout (Garces, Carretero, Rodenas, & Aleman, 2010). Thus, it is important to further investigate whether family caregivers receive enough support when care recipients use multiple services but not personal care services and whether this use pattern is due to family caregivers’ preferences or their lack of knowledge about accessing services or negotiating with care managers. We suggest that future policy of 10-Year LTC Plan Version 2.0 in Taiwan should not only acknowledge the contribution of family caregivers but also encourage family caregivers to understand their own unmet needs when caring for older disabled family members.
Several limitations should be noted in this study. First, we measured only nationally funded HCBS. Private hire of foreign caregivers to care for disabled adults and perform daily activities in the home is known to be an issue in Taiwan (Lee et al., 2013), but this information was not included in this study. This omission may lead to underestimation of the situation as a whole regarding use of formal HCBS in Taiwan. Furthermore, the important contribution of informal caregivers is something we could not recognize within this study. We recommend that future studies include this kind of care to better understand the profiles of care recipients and their families and better match their care needs.
A second limitation is that supplementary services, such as environmental modification services and home meal delivery, were also excluded from the study. It was common policy in Taiwan to allow only one provision of environmental modification for each care recipient (Ministry of Health and Welfare in Taiwan, 2007), and thus, we decided that this service did not fit the definition of long-term use of HCBS we were interested in studying. Home meal delivery was another issue we excluded from the study because it seemed to be provided as a social welfare subsidy in Taiwan. We further analyzed the data and found that meal delivery services were correlated with individuals who had low socioeconomic status but better BADL function than the individuals we did include in the study. Future studies are recommended to examine home meal delivery provided to this low socioeconomic group of older adults in Taiwan.
Third, our study measured the association of the first-time needs assessment and the prescribed HCBS at that time point for each included care recipient. We suggest a future study to examine transitions in individuals’ needs assessments and the related services that are prescribed over the long run to better understand whether current long-term care services meet the needs of care recipients and their families in Taiwan.
Fourth, it is important to keep in mind that some potential enabling factors in Andersen’s Behavioral Model, which might affect use of HCBS, were not included due to the limitations of secondary data analysis. Future research should include service availability as well as other environmental factors which would be likely to influence HCBS access.
Conclusion
In summary, it is now time for Taiwan to transition from the previous National 10-Year LTC Plan policy to the current 10-Year LTC Plan Version 2.0 (Ministry of Health and Welfare in Taiwan, 2016). Understanding the profiles of care recipients and their service use patterns in the existing data can provide useful guidelines for the new 10-Year LTC Plan Version 2.0 policy, which emphasizes integration of HCBS and use of multiple HCBS. We found that latent class analysis provided a practical approach for identifying distinct subgroups of care recipients with distinct patterns of HCBS use in Taiwan. Based on our findings, we recommend that a flexible long-term care policy that promotes use of integrated services and alleviates barriers to accessing multiple types of services should be encouraged in the future.
Footnotes
Author Contributions
Hsiao-Wei Yu made a substantial contribution to the design of current study and drafted the article. Yu-Kang Tu was consulted by his expertise in latent class analysis and helped for the interpretation of data. Po-Hsiu Kuo helped for acquisition of the data and revised the draft critically for important content. Ya-Mei Chen took responsibility for the interpretation of data and approved the version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors wish to express their gratitude to the Ministry of Science and Technology in Taiwan (MOST105-2410-H-002-214-MY3, MOST-105-2811-H-002-042) and the Health and Welfare Data Science Center for its gracious help with data access (H104146). The current study has been approved by the Research Ethics Committee of National Taiwan University (201508093W).