
Abstract
Problem-solving skills in the context of technologically complex modern societies have become increasingly important to health management in later life. This study is designed to investigate the associations between problem-solving skills in technology-rich environments (PSTRE) and health, and to explore whether age differences exist. Using data from the 2012/2014 Program for the International Assessment of Adult Competencies (PIAAC), we used logistic regression to examine the relationship between PSTRE and self-reported health among a representative sample of American adults aged 35 years and older (N = 3,260). Overall, greater PSTRE (odds ratio [OR] = 1.012, p < .001) was significantly associated with better self-rated health even after adjusting for the sociodemographic characteristics. Yet, PSTRE was only partially predictive of health in some age groups. Our findings highlight the potential of PSTRE to reduce health disparities among middle-aged and older adults living in modern technology and information-rich societies.
Everyday problem-solving skills (PSS), or the ability to find effective solutions for everyday challenges, have been shown to be an important predictor of health status among aging adults (Mienaltowski, 2011; Thornton, Deria, Gelb, Shapiro, & Hill, 2007). Furthermore, age-related cognitive declines can contribute to difficulties in everyday problem solving that involve domains such as processing speed, working memory, and inductive reasoning (Mienaltowski, 2011; Schaie, Willis, & Caskie, 2004). In an era of digital technology, health-related information and patient–physician communications are increasingly being integrated through emerging technologies such as computerized systems, which may present unique challenges associated with managing one’s own health and navigating health care systems in later life (Gordon & Hornbrook, 2018). In the context of an aging society and given the increasing reliance on technology in health care settings and health management, PSS in an environment of fast-changing digital technology could influence the health of middle-aged and older adults by limiting access to, and use of, digitalized health information (Mackert, Mabry-Flynn, Champlin, Donovan, & Pounders, 2016).
Literature Review
Problem Solving and Health
PSS refer to individuals’ ability to draw from accumulated knowledge/experience and critical thinking skills to reach sound solutions and adapt to everyday challenging environments (Mienaltowski, 2011). Problem solving may require that individuals recruit different skills based on the nature of the “challenge” at hand. For instance, crystallized intelligence is knowledge or experience that is accumulated over time and remains as a person ages, such as language, or general knowledge. In contrast, fluid intelligence refers to the ability to solve unfamiliar problems and use critical thinking skills through processing speed, inductive reasoning, and working memory (Ziegler, Cengia, Mussel, & Gerstorf, 2015). Skills related to fluid intelligence have been shown to decrease, starting in the late 20s and mid-30s, whereas crystallized intelligence is thought to remain stable in midlife until there is a gradual decline in the seventies and eighties (Schaie et al., 2004). Thus, solving problems that require fluid skills (e.g., processing speed, inductive reasoning) can be more challenging in middle and older adulthood due to age-related cognitive declines. These age-related changes in strategies for problem solving can result in different individual outcomes across the life course (Artistico, Cervone, & Pezzuti, 2003; Burton, Strauss, Hultsch, & Hunter, 2006). For instance, differences in PSS can have important consequences for health and health behaviors later in life.
There is now evidence that PSS are moderately related to a number of health conditions and overall health status. Visser and colleagues (2015) found that among stroke survivors, greater PSS are associated with better health-related quality of life. PSS have been also studied in the context of diabetes self-care (King et al., 2010), mobility (Areán et al., 2015), and ability to complete activities of daily living (ADLs) or instrumental activities of daily living (IADLs; Kimbler, 2013). The positive relationship between PSS and health-related outcomes is generally consistent. These studies support that PSS are a predictor of health status. Similarly, problem-solving therapy (PST) has shown positive health-related outcomes such as reduced depressive symptoms in several clinical trials and interventions for older adults (e.g., Areán et al., 2010; Gustavson et al., 2016; Malouff, Thorsteinsson, & Schutte, 2007). PST is a problem-focused cognitive–behavioral intervention that promotes proactive problem-solving and positive coping strategies (Haley, 1987). Overall, this body of research supports a positive relationship between problem solving and health in middle and older adulthood.
Technology and Health
Although PSS have been associated with health, the roles of specific PSS components remain understudied (Kimbler, 2013). This is particularly the case for problem-solving skills in technology-rich environments (PSTRE). PSTRE refer to “using digital technology, communication tools and networks to acquire and evaluate information, communicate with others and perform practical tasks” (Organisation for Economic Co-operation and Development [OECD], 2012, p. 46). High PSTRE can facilitate the successful attainment and assessment of health information using digital sources, providing individuals with greater PSTRE with additional health-promoting opportunities and resources. Limited research has examined the direct influence of PSTRE and its effect on health. Among such studies, Prins, Monnat, Clymer, and Toso (2015) found that an increase in PSTRE was associated with 7.6% greater odds of reporting better self-rated health among adults aged 16 to 65 years. However, this relationship became nonsignificant after accounting for sociodemographic characteristics. Importantly, adults above the age of 65 were not included in their analysis. The second half of adult life is a life stage where individuals often experience declining health. Given the growing presence of technology in health care and health care management (Mackert et al., 2016), the use of PSTRE presents opportunities for promoting the health of middle-aged and older adults.
In an era of digital technology, health-related information and patient–physician communications are increasingly being provided through web-based modalities (Gordon & Hornbrook, 2018). For instance, eHealth, or consumer health information technologies, allow prompt access to patient–physician communication and health-promoting information (Gewald & Rockmann, 2016). The role of technology in health care is likely to continue expanding, which offers opportunities for health promotion by allowing individuals to take active control of their health management (Jacobs, Lou, Ownby, & Caballero, 2016). The Healthy People 2020 initiative calls for the use of health information technology as a tool for improving population health and health care quality (HealthyPeople.gov, n.d.). However, using these resources requires basic knowledge and the ability to adapt to emerging technologies (Czaja et al., 2006). Digital health literacy has been used to capture the skills required to use technology for health management and health information seeking (Norman & Skinner, 2006). Older adults may face a number of barriers that limit their digital health literacy. For instance, older adults may have less familiarity with the use of digital technology and may be less likely to use these resources (e.g., online health information management system) for health management (Gordon & Hornbrook, 2018). Differences in access to digital technologies and the ability to use these technologies to obtain health information can contribute to health disparities for middle and older adults.
Conceptual Model
Given a lack of conceptual scholarship involving a direct relationship between PSTRE and health, we draw from two relevant conceptual models: Paasche-Orlow and Wolf’s (2007) model linking health literacy to health outcomes, and Gewald and Rockmann’s (2016) model of enhanced eHealth use. Health literacy is defined as “the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions” (U.S. Department of Health and Human Services, 2010). However, PSTRE can be considered a specific type of general PSS. Given the increasing interest in health and digital technology in later life, we apply these conceptual models to examine the role of PSTRE in relation to self-rated health as an outcome. In view of Paasche-Orlow and Wolf’s (2007) model, PSTRE are one of several individual-level characteristics associated with health-related outcomes. Furthermore, problem solving is influenced by age, among other sociodemographic characteristics (Paasche-Orlow & Wolf, 2007). The second model by Gewald and Rockmann (2016) highlights the importance of computer self-efficacy, through the innovative use of information technology (i.e., PSTRE) for health care management. This model suggests that PSTRE is negatively associated with age and is expected to affect health outcomes via differing health information seeking, including the use of Internet, printed sources, as well as social networks. Ideas put forth by these models propose an important association between PSS, technology use, and health. We build on these two conceptual models by explicitly examining the direct association between a specific type of PSS (i.e., PSTRE) and self-rated health in the adult life.
Research Questions
This study formulated and addressed two research questions:
Method
Data
We obtained the data from the U.S. public use files of the 2012/2014 Program for the International Assessment of Adult Competencies (PIAAC). PIAAC provides data for adults from OECD nations. The overall goal of the PIAAC is to assess the skills of adults in economically developed societies. In particular, the PIAAC uses an interactive computer-based assessment to measure individuals’ PSTRE. The U.S. PIAAC uses a four-stage stratified probability method to recruit adults between the ages of 16 and 74. PIAAC provides final sampling and replicate weights to correctly estimate nationally representative results (The American Institutes for Research [AIR] PIAAC Team, n.d.). Additional technical information about PIAAC has been published elsewhere (National Center for Education Statistics, 2017). The current analysis uses data for adults above the age of 35. Our decision for this age cutoff is based on support for changes in cognitive skills (i.e., fluid intelligence indicators) that relate to problem solving that involves novel problems (e.g., emerging technologies). Of 4,532 eligible respondents, our final analytic sample consisted of 3,260 respondents who were randomly selected to complete the PSTRE module.
Variables
Outcome variable
Our outcome of interest is self-rated health. PIAAC respondents were asked the following question: “In general, would you say your health is excellent, very good, good, fair, or poor?” In light of the low number of fair and poor health responses, self-rated health was dichotomized as (1 = good health [excellent, very good, good] or 0 = poor health [fair, poor]).
Predictor variables
PSTRE was analyzed by a set of 10 statistically estimated means (i.e., plausible values; range = 0-500) based on the respondents’ performance on a select number of PSTRE-related tasks (OECD, 2012). PIAAC’s PSTRE domain measures and quantifies individuals’ ability to use digital devices and software applications to solve everyday tasks. More specifically, the PIAAC assesses PSTRE skills by presenting respondents with a set of computer-based tasks of increasing difficulty. These tasks incorporate adaptive response functions and are timed to rigorously assess individuals’ PSTRE skills. For example, a simpler task asks individuals to organize or sort large numbers of digital files according to their size, or adjust software program settings according to specific instructions (OECD, 2012). More complex tasks may involve locating an email, opening its attachments, and using the attached information to create simple graphics and tables (see chapter 5 of the OECD’s 2012 technical report for detailed information and additional sample items). Age was measured in two different ways: in 5-year intervals (i.e., 35-39, 40-44, 45-49, 50-54, 55-59, 60-65, 66-70, and 71+) and 10-year intervals (i.e., 35-44, 45-54, 55-65, 66+). Although the 5-year interval provides more detailed information and was used in the main analysis, the 10-year intervals were included in subgroup analyses, given the small sample size and distribution of two relevant covariates (health insurance and income) in older age groups. This decision was made based on PIAAC-specific recommendations, which suggests a minimum subgroup sample size of 62 to produce meaningful, reliable results (AIR PIAAC Team, n.d.).
Covariates
Sex was coded as 1 = female and 0 = male. Race/ethnicity was dichotomized to reflect whether a respondent identified as non-Hispanic White or some Other race/ethnicity (1 = non-Hispanic White and 0 = Other). The sample size for the specific race/ethnic groups was insufficient. Educational attainment was dichotomized to represent 1 = college degree or higher and 0 = less than a college degree. Income was categorized based on a 5-category scale developed by PIAAC to illustrate representative income quintiles (1 = lowest income to 5 = highest income). Nonemployed individuals, or those with no income, were aggregated to the lowest income quintile given PIAAC’s classification of the unemployed as nonearners. A dichotomous variable was used to denote whether a respondent had health insurance (1 = yes and 0 = no). Finally, based on Gewald and Rockmann’s (2016) conceptual model of technology and health, we included a variable to capture the use of the Internet for health information seeking. Based on the question “How much information about health issues do you get from the Internet?” and the responses, a lot, some, a little, and none, we dichotomized Internet use for health information seeking (1 = yes [a lot and some] and 0 = no [a little and none]) based on conceptual and distributional considerations.
Analytical Approach
We used the IDB Analyzer version 4.0.14, developed by the International Association for the Evaluation of Educational Achievement [IEA] (2017). The IDB Analyzer generates a macro program that can be executed using SPSS or SAS software to estimate representative figures with PIAAC data, and incorporates sampling weights (SPFWT0), replicate weights (SPFWT1-SPFWT80), and PSTRE plausible values into the statistical analysis (AIR PIAAC Team, n.d.; IBM Corp., 2017; SAS Institute Inc., 2013). Unweighted descriptive statistics were computed for all variables included in the final model. To address our first research question (Is there an association between PSTRE and self-rated health?), we used a fully adjusted binary logistic regression to model self-reported health (dichotomized given the skewed distribution and conceptual reasons for the meaningful groups [positive vs. negative health]) as a function of PSTRE values while adjusting for covariates (Wright, 1995). We also constructed unadjusted models to establish the baseline models.
To address our second research question (are there significant age differences in the relationship between PSTRE and self-rated health?), we conducted a series of logistic regression analyses for age groups based on the 5- and 10-year intervals. To explore meaningful age group specifications in the context of our research, age in 5- and 10-year intervals were used in separate analyses. Our decision to utilize both age categorizations (i.e., 5- and 10-year intervals) for the subgroup analysis was informed by the PIAAC guidelines requiring the use of subgroups with more than 62 observations to make accurate estimations (AIR PIAAC Team, n.d.). Due to the small sample sizes for those who were not employed and/or uninsured among older age groups, we eliminated income and health insurance from our covariates in the subgroup analysis. This way, the model specifications were consistent across the age groups and results were comparable. Because the objective of the subgroup analysis is to explore the relationship between the self-reported health and PSTRE across age groups, the comparable models were required.
Finally, given the conceptual relevance of health information seeking using the Internet, we tested an interaction between PSTRE scores and Internet use for health information seeking; results for this interaction were nonsignificant in our preliminary analysis. We also tested models that included the age and income variables measured in a series of dichotomous variables. We verified no major differences between these models, and final models were constructed with the age and income as ordinal measures. All analyses were conducted using SAS version 9.4 (SAS Institute Inc., 2013).
Results
Table 1 presents unweighted descriptive statistics (except for the PSTRE scores) for our analytic sample by health status. The majority (85%) of respondents in our sample reported good health. The average weighted PSTRE score was 265. Respondents with good self-reported health had, on average, higher PSTRE scores than those with poor health (268.415 and 265.432; t = 8.053, p < .05, df = 3,259). There were a smaller percentage of respondents in the two oldest age categories of 66 to 70 and 71 and above (10.726% and 5.782%, respectively). More than half of respondents were in the lowest income quintile (54.412%), mainly due to the employment status (i.e., unemployed or retired). Nearly half of the respondents were female (54.822%), whereas the majority (60.741%) had a high school–level education or less, identified as White (68.878%), and reported having health insurance (81.919%). Finally, more than 67.977% of participants reported using the Internet frequently for accessing health information.
Unweighted Descriptive Statistics for Adults Above Age 35 by Health Status.

Note. PSTRE significance test based on weighted values, other estimates based on unweighted values. PSTRE score estimate is weighted and calculated using plausible values and replicate weights. No unweighted score is available in the PIAAC. Ten-year age groups used in subgroup analysis only; p values based on chi-square and t tests. Good health = self-reported health (excellent: very good, good); poor health = self-reported health (fair, poor). PSTRE = problem-solving skills in technology-rich environments; PIAAC = Program for the International Assessment of Adult Competencies.
p < .05. **p < .01. ***p < .001.
Table 2 presents estimated odds ratios (ORs) from weighted binary logistic regression models that address our first research question. In the unadjusted model, PSTRE was a statistically significant predictor of good health status (OR = 1.012, p < .001). That is, a one-point increase in PSTRE score was associated with 1.012 times odds of reporting good health. This relationship remained significant in our adjusted model after accounting for covariates (OR = 1.006, p < .01). A one-point increase in PSTRE score was associated with 1.006 times odds of reporting good health. Importantly, only income (OR = 1.509, p < .001) and college education (OR = 1.371, p < .001) were statistically significant predictors of good health. On a related note, given the validity of self-rated health changes in later life (i.e., moderation effect by age; see Zajacova & Woo, 2016), we ran separate models for the life stages. For example, follow-up analysis of ages 35 to 49 and 50 and older showed that the estimated ORs of PSTRE (age = 35-49 years: OR = 1.007, p < .01; age = 50 and older: OR = 1.005, p < .01) were consistent with our final model (OR = 1.006). This is not to say that the interpretation of self-rated health by life stages is comparable, but its associations with PSTRE were consistent across age groups in our study.
Estimated OR From Weighted Binary Logistic Regression Models of PSTRE Scores Predicting Self-Rated Health (N = 3,260).
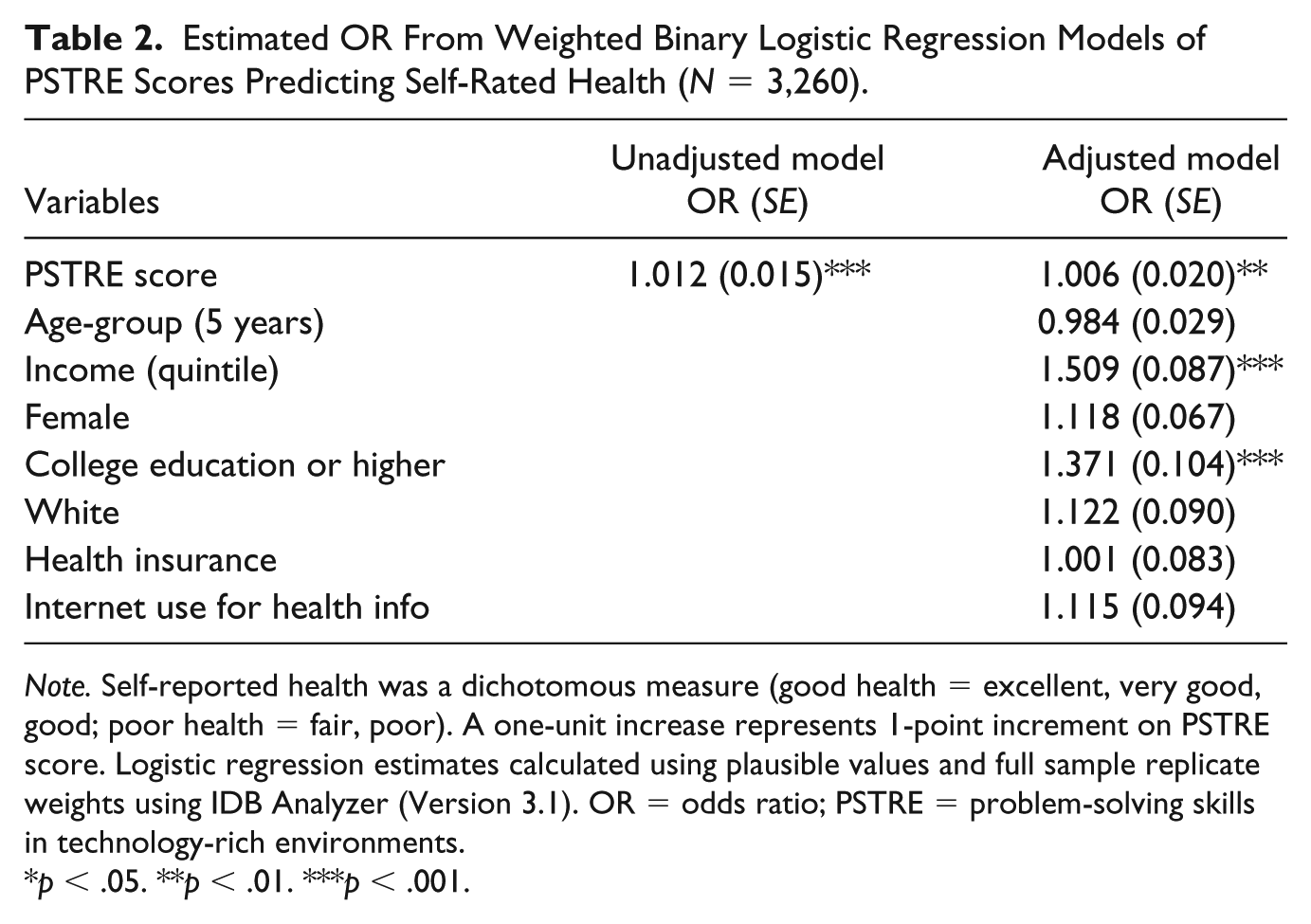
Note. Self-reported health was a dichotomous measure (good health = excellent, very good, good; poor health = fair, poor). A one-unit increase represents 1-point increment on PSTRE score. Logistic regression estimates calculated using plausible values and full sample replicate weights using IDB Analyzer (Version 3.1). OR = odds ratio; PSTRE = problem-solving skills in technology-rich environments.
p < .05. **p < .01. ***p < .001.
Table 3 presents adjusted logistic regression results for our subgroup analyses of 5- and 10-year age subgroups, which address our second research question. For the 5-year age categories, PSTRE was a statistically significant predictor of good health status among the 45- to 49-year-old age group (OR = 1.013, p < .01), the 60- to 65-year-old age group (OR = 1.007, p < .05), and the 66- to 70-year-old age group (OR = 1.008, p < .05). In the 10-year age subgroups analyses, PSTRE was a statistically significant predictor of good health status among all age groups: 35- to 44-year-old group (OR = 1.006, p < .05), 45- to 54-year-old age group (OR = 1.008, p < .01), 55- to 65-year-old age group (OR = 1.006, p < .05), and those 66 years or older (OR = 1.010, p < .05). College education was a significant predictor of self-reported health in the age groups 35 to 44, 45 to 54, and 55 to 65. All other covariates were not statistically significant in any of the 10-year age groups.
Estimated OR From Weighted Binary Logistic Regression Models Predicting Self-Rated Health by Age Groups.
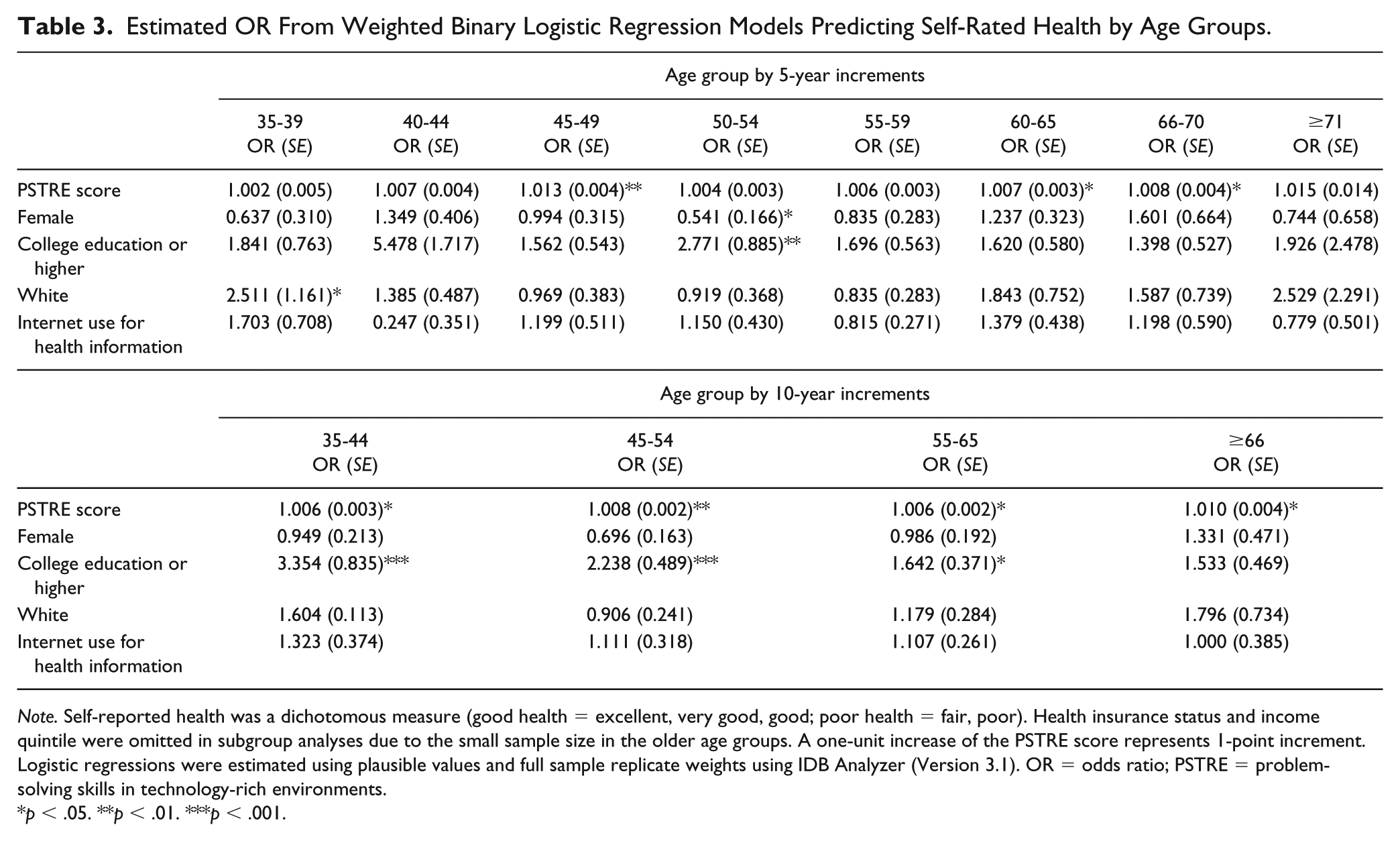
Note. Self-reported health was a dichotomous measure (good health = excellent, very good, good; poor health = fair, poor). Health insurance status and income quintile were omitted in subgroup analyses due to the small sample size in the older age groups. A one-unit increase of the PSTRE score represents 1-point increment. Logistic regressions were estimated using plausible values and full sample replicate weights using IDB Analyzer (Version 3.1). OR = odds ratio; PSTRE = problem-solving skills in technology-rich environments.
p < .05. **p < .01. ***p < .001.
Discussion
We addressed two research questions: (a) Is there an association between PSTRE and self-reported health? and (b) Are there significant age-related differences in the relationship between PSTRE and self-reported health? In support of our first research question, results from our analysis show that an increase in PSTRE was associated with better self-rated health. Unlike the previous studies of PSTRE and health of adults aged 16 to 65 (e.g., Prins et al., 2015), the PSTRE and health relationship persisted after introducing relevant sociodemographic characteristics among those aged 35 and 74. This relationship was partly explained by income and education. Income and educational status are well established social determinants of health in later life (Centers for Disease Control and Prevention [CDC] Online Newsroom, 2012).
With regard to our second research question about age-related differences in this association, subgroup analyses showed mixed findings. Consistent with the empirical and conceptual literature, which suggest age-related declines in the ability to solve novel problems such as those of emerging technologies (Mienaltowski, 2011), we expected to see age-related changes in the association between PSTRE and health in middle and older adulthood. However, we found limited and inconsistent support for significant age differences. Our two sets of subgroup analyses by 5- and 10-year categories yielded different results. PSTRE was the only statistically significant predictor of good health among 45- to 49-year-olds, 60- to 65-year-olds, and 66- to 70-year-olds in the first set of analyses. However, the second set of analyses showed that PSTRE was a significant predictor of good health for all age groups. Yet, it should be noted that there could be significant differences in the way older and younger cohorts utilize PSTRE skills for health-related information. Our study lays the groundwork for future research to further investigate this relationship as well as to disentangle age, period, and cohort effects.
In view of the empirical and conceptual scholarship, we expected age differences in the use of the Internet for health information seeking (Jensen, King, Davis, & Guntzviller, 2010). However, Internet use for health information seeking was not associated with reporting better health in any of our age subgroup analyses. This may suggest the use of alternative health information sources, such as health care professionals or books and magazines (Hall, Bernhardt, & Dodd, 2015; Yamashita, Bardo, Liu, & Cummins, 2018). Higher PSTRE may be related to the use of these multiple health information sources. Indeed, there is evidence that health information seeking can be influenced by education and health literacy, with higher education being associated with greater use of text-based information, and higher health literacy associated with less use of the Internet for health information (Feinberg et al., 2016; Yamashita et al., 2018).
Nevertheless, PIAAC’s PSTRE domain is a novel and complex measure that assesses cognitive ability through problem solving, as well as familiarity with technology (OECD, 2012). The integration of these two domains (cognitive ability and technology use) provides an informative new measure that bridges previous avenues of inquiries related to the assessment of online health information seeking in older adults (Berkowsky & Czaja, 2018). PSTRE can be considered one of the health literacy domains that is important for health in later life. Past studies have found positive relations between general literacy, numeracy, and self-rated health (e.g., Prins & Monnat, 2015). It should be noted that the PIAAC provides general literacy and numeracy in addition to the PSTRE skills assessment. Our decision to focus on PSTRE was based on a lack of inquiry on PSTRE as well as the relevance to the research needs on digital technology, health, and aging. Given the little understanding about the relationship between PSTRE and health, we did not include other competency measures such as literacy and numeracy to document the baseline effect of PSTRE. Given our findings and insights from the previous research, components of health literacy, such as literacy, numeracy, and PSTRE, are likely to contribute to health outcomes in different ways. Future research needs to identify such unique effect for informing health promotion programs targeting specific health literacy domains such as PSTRE. In addition, further research is needed to determine the subdomains of PSTRE (instead of a single-item indicator) and potential mechanisms by which PSTRE affects a variety of health-related outcomes among middle-aged and older individuals.
Limitations
This study should be considered in light of some methodological limitations. First, our analysis uses cross-sectional data, which limits the ability to make any causal inference. Second, we cannot rule out potential omitted variable bias. Particularly, traditional demographic characteristics such as marital status and other social network/support information would be helpful in future research although not available in the current PIAAC data. Third, the PIAAC public use files only provide age group information. In addition, age range in the PIAAC is limited to ages 16 to 74. Given the importance of age for PSS, future studies should consider extending the age range beyond 74 years old to more broadly capture age-related health declines in the context of a digital era. Fourth, our sample distribution and the suggested sample size requirements for using the IDB Analyzer restricted our analytic approach to control for two relevant covariates (income and health insurance status) in our subgroup analyses. Although the decision was appropriate for the examination of age group differences, omission of these covariates could have over- or underestimated the effect of PSTRE on health in general and, arguably, in older age groups with limited sample sizes. Finally, given our use of a dichotomous, self-reported measure of health, future research should consider more direct and objective indicators of health status.
Contributions
Despite the limitations, this study adds to the growing, yet limited, body of research on the malleable factors such as adult education and skill proficiencies (e.g., PSTRE), which are influential on health status among adults in multiple life stages (e.g., Paasche-Orlow & Wolf, 2007; Prins & Mooney, 2014). We address a gap in this literature by focusing on an understudied adult competency indicator of PSS (Kimbler, 2013). We are one of few studies to use nationally representative data to directly explore PSTRE and its association with self-reported health in middle-aged and older adults. Results from our adjusted logistic regression analysis provide support for the association between PSTRE skills and self-rated health even after accounting for the sociodemographic characteristics. These findings have the potential to inform the design of competencies-based health promotion as well as adult education programs that incorporate technological problem solving to address health disparities among middle-aged and older adults (Mackert et al., 2016; Tikkanen, 2017).
Implications
There are a few preliminary implications we can draw from the results of this study. Our results suggest that adult education programs could include problem-solving and technology skills interventions to better equip middle-aged and older individuals to effectively navigate health care systems and enhance health outcomes. Promoting PSTRE could be an efficient and autonomous (e.g., self-care) way to reduce health disparities. From a life course perspective, lifelong learning is no longer a means merely to acquire new knowledge and skills; it has become a critical process to obtain necessary skills (e.g., appropriate use of Internet as health information source) to navigate in this digital era (Tikkanen, 2017). In addition, our findings suggest that health care professionals can identify and provide additional support (e.g., customized instruction, recommendation for technology-related training) to individuals with limited technological proficiencies as a potential avenue to limit health disparities. As our findings suggest, individuals with low PSTRE skills could benefit from technology-related training programs to promote health outcomes. For example, enhanced PSTRE could improve health outcomes by allowing middle-aged and older individuals to take active participation in managing their health with the use of emerging digital technologies (Kiosses & Alexopoulos, 2014). At the same time, any intervention programs should consider age differences in skill sets as well as attitudes toward technology use. Finally, this study provides policy makers with a nationally representative profile of adults’ PSTRE, which, although understudied, seems to be important for health in middle and old age.
Conclusion
In an era of emerging digital technology in health care, practicing self-care and navigating health care systems is becoming increasingly dependent on technology-related PSS. Difficulty understanding and using the rapidly advancing technologies for health-related information and health management may exacerbate already existing health inequalities, particularly among older individuals. In this study, we find that PSTRE is positively associated with self-reported health among American adults. Furthermore, we find unique age group differences, with higher PSTRE skills being associated with better health at the differential degrees by life stages. Our findings highlight the importance of promoting technological PSS through lifelong education to promote the health of aging adults.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research reported here was supported by the Institute of Education Sciences, U.S. Department of Education, through Grant R305A170183 to Miami University and the University of Maryland, Baltimore County. The opinions expressed are those of the authors and do not represent views of the Institute or the U.S. Department of Education.