
Abstract
Background and Significance
As the population in the United States ages, the number of older adults requiring long-term services and support (LTSS) will increase substantially. More than half of all adults 65 years and above will develop functional deficits that will require assistance with activities of daily living as well as other health and social services over time (Congressional Budget Office, 2013; Favreault & Day, 2016; Reinhard, Kassner, Houser, & Mollica, 2011). In 2014, nearly seven million U.S. adults, aged 65 years and older, received LTSS assistance in a range of settings, including in their homes via community-based services (HCBSs), assisted living communities (ALCs), and nursing homes (NHs; Nguyen, 2017).
Age-related changes, complicated by frailty and multiple chronic conditions, contribute to high rates of health care transitions among LTSS recipients (Konetzka, Spector, & Limcangco, 2008). In one recent study of over 500,000 Medicare beneficiaries admitted to an NH for either long-term or short-term care, transitions between settings (e.g., hospital to NH, skilled nursing facility [SNF] to NH, NH to home) over a 12-month period occurred among 36.5% of the sample (Li, Middleton, Ottenbacher, & Goodwin, 2018).
Prior epidemiological studies characterize the incidence and predictors of individual transitions in care that predict the use of LTSS and what happens during LTSS use, such as hospital to home, rehabilitation center to home, and SNF to home (Greiner et al., 2014; Holden et al., 2015; Toles et al., 2014). Findings in observational studies of individual care transitions may underestimate the risk and burden experienced by older adults who have multiple transitions in care over multiple months or years, often starting prior to LTSS. Thus, determining baseline predictors of multiple health care transitions among those new to LTSS could provide important targets for intervening to optimize health and prevent burdensome transitions when possible, such as, avoidable hospitalizations or emergency department (ED) visits. Moreover, determining risk factors at the start of LTSS is essential for advising recipients and their families about the preferred plans of care.
Findings from prior studies reveal common sociodemographic and clinical characteristics that predict hospital admissions, including age, gender, race, socioeconomic status, and specific diagnoses such as heart failure, dementia, and cancer (Callahan et al., 2015; Fabius & Robison, 2017; Kind et al., 2014; O’Connor et al., 2016). Other factors were identified that contribute to differences in rates of hospitalization among this population, including (a) regional practice patterns, (b) quality of care in hospitals, post-acute care settings, NHs and ALCs, hospices, and (c) state Medicaid and federal Medicare NH payment policies (Goodman, Fisher, Chang, & Raymond, 2013; Gruneir, Miller, Intrator, & Mor, 2007; Intrator et al., 2007). Collectively, these factors contribute to frequent use of acute care services and LTSS by frail older adults who often experience negative changes in health status.
Although risk factors for rehospitalization, in general, have been characterized for older adults and older adults receiving LTSS, to the best of our knowledge, no studies to date have examined health care transitions across groups of new LTSS recipients, receiving support from diverse organizations, specifically ALCs, NHs, and HCBS. Although findings are available on specific types of health care transitions (primarily hospitalizations), prior research has been limited to specific transitions between settings of care (e.g., hospital to community, SNF/IRF to home; SNF to hospital; Holden et al., 2015; Toles et al., 2014). Limited attention has been paid to multiple health care transitions among older adults (Li et al., 2018; Wang et al., 2017), but even less is known about multiple health care transitions among ALCs and HCBS recipients. In addition, the relationship between multiple health related quality of life (HRQoL) domains and health care transitions among older adults new to LTSS has not been studied. Without this information, LTSS providers do not optimally anticipate the needs and effectively manage health services for this vulnerable and growing population.
In response to these gaps in knowledge, the purposes of this study were to describe health care transitions over time among a cohort of older adults new to receiving LTSS and to examine the relationships between these health care transitions and individual LTSS recipient sociodemographic and clinical characteristics at baseline.
Method
Framework
The Andersen Behavioral Model of Health Service Use guided this examination of individual and contextual factors contributing to health care use (Andersen, 1995); specifically, the relationship between characteristics of newly enrolled LTSS recipients (e.g., their need, access, and predisposing characteristics) and contextual factors (e.g., setting, health behaviors) that influence heath care transitions. Concepts in the Behavioral Model were defined as follows: (a) health service use was the total number of health care transitions (described in detail below); (b) predisposing factors were the clinical and nonclinical characteristics of new LTSS recipients; (c) enabling factors were characteristics of the health care environment, such as residence in an NH or ALC; and (d) need factors were self-reported health, social support, and quality of life of new LTSS recipients.
Data
This secondary analysis used data from the “Health Related Quality of Life (HRQoL): Elders in Long-Term Care” study (NIA/NINR R01AG025524; principal investigator: Mary D. Naylor). The specific aims of the parent study were to describe changes in multiple domains of HRQoL for a cohort of older adults who at the time of enrollment had just begun to receive LTSS in ALCs, NHs, or in their homes via HCBSs (e.g., Program of All-inclusive Care for the Elderly, Managed Long-Term Care, etc.), and followed for 24 months after enrollment or until withdraw or death. Purposive sampling was used to identify potentially eligible participants. Individuals were eligible to participate if this was their first experience receiving LTSS (e.g., no previous long-term care service use), they were within 60 days of the start of services, 60 years of age or older, and willing to complete in-person interviews every 3 months for 2 years in English or Spanish, and they had a Mini Mental State Examination (MMSE) score of 12 or higher (Folstein, Folstein, & Fanjiang, 2001; Folstein, Folstein, & McHugh, 1975). Individuals with severe cognitive impairment (e.g., MMSE < 12), those with an active impaired sense of reality (such as untreated or poorly managed paranoia or psychosis), or whose plan of care was focused on end-of-life care (e.g., considered terminally ill or enrolled in hospice) were not eligible to participate. According to the parent study, 1,311 older adults were referred as potential participants. Among the 1,311 referred, 480 (37%) did not meet study eligibility criteria (i.e., >60 days from start of LTSS, n = 260; prior LTSS experience, n = 144; MMSE < 12, n = 76). Among the remaining 831 referrals, 327 were screened, but declined to participate (n = 220), declined in-person visit (n = 99) or deferred to enroll and timed out of eligibility (n = 8); an additional 29 did not have someone to co-sign and provide informed consent on behalf of the participant assessed as having cognitive deficits (MMSE: 12-23) and 5 were dropped as a result of incomplete enrollment. A total of 470 older adults were enrolled in the longitudinal, observational parent study designed to assess changes in multiple HRQoL domains over time (ALCs, n = 156; NHs, n = 158; HCBSs, n = 156). Enrolled participants came from 11 organizations (59 locations) across three U.S. states (Pennsylvania, New Jersey, and New York). Additional details on eligibility and recruitment procedures for the original parent study data set are described in detail elsewhere (Naylor et al., 2016).
Three institutional review boards (IRBs)—the University of Pennsylvania (Protocol: 805326), the Philadelphia Veterans Medical Center (Protocol Number: 01033), and the Visiting Nurse Service of New York (Protocol Number: 212462-12)—approved the parent study and were the IRBs of record for the participating organizations. Written informed consent or assent was gathered from all enrolled LTSS participants. For each LTSS recipient who wished to participate but scored 12 to 23 on the MMSE (Folstein et al., 2001; Folstein et al., 1975), a designated responsible party was asked to provide written informed consent for their family member to participate. At each of the quarterly interviews, participants were reminded of the purpose of the study and asked if they still wished to be interviewed. This secondary data analysis of the parent study data set was reviewed and approved by the University of Pennsylvania IRB.
Measures
Counts of health care transitions (primary outcome) and several standardized measures of HRQoL were available from baseline and every 3 months through 24 months (a maximum of 9 data collection time points) for each respondent. Data used for this analysis came from both self-reported data documented by trained research assistants (RAs) at follow-up interviews and chart review abstraction.
Primary outcome—Total number of health care transitions
Similar to recent research on transitions in care (Li et al., 2018; Wang et al., 2017), health care transitions were operationalized as any of the following: (a) acute hospitalizations, (b) ED visits (e.g., transfer to ED that did not result in a hospitalizations), (c) admissions to skilled nursing facilities (SNFs) or inpatient rehabilitation facilities (IRFs), (d) changes in the type of LTSS (e.g., transitions between ALCs and NHs, NHs and ALCs, HCBS and NH), (e) enrollment in hospice, and (f) deaths. Among NH residents who were hospitalized and transitioned back to their NH where they received SNF level care, this was counted as a single transition. For HCBS or ALC residents who had a hospitalization followed by discharge to an IRF before returning home, this counted as two transitions (hospitalization and IRF stay). Data were collected via chart reviews from baseline (3 months prior to the start of LTSS) and then every 3 months through 24 months from the start of LTSS. The number of events for each type of transition noted above were summed into a count variable in each quarter through the end of the study. The average number of transitions and the total number of transitions from baseline to each quarter thereafter were calculated.
Baseline predictor variables
In the parent study, individual LTSS recipient characteristics were collected via face-to-face interviews conducted in both English and Spanish by trained RAs and documented on standardized data collection forms; data generated from chart reviews completed by these same RAs at baseline also were documented on such forms. Baseline data included age, sex, race, ethnicity, years of education, number of chronic conditions, number of medications, nutritional status (Nutrition Screening Initiative Checklist; Posner, Jette, Smith, & Miller, 1993), type of LTSS (i.e., ALCs, NHs, or HCBS), ambulation support (e.g., use of cane, walker, wheelchair, brace, etc.), and sensory support (e.g., glasses, hearing aids). Two items from the chart review were used to confirm the LTSS recipient had physicians’ orders to receive physical therapy (yes/no) or occupational therapy (yes/no) at the start of LTSS. Several valid and reliable tools were used to collect self-reported HRQoL domains at study enrollment: (a) overall quality of life (Godin, Keefe, Kelloway, & Hirdes, 2015), (b) cognitive status (MMSE; Folstein et al., 1975), (c) symptom status (Symptom Bother Scale; Heidrich & D’Amico, 1993), (d) emotional status—depressive symptoms (Geriatric Depression Scale Short Form [GDS-SF]; Conradsson et al., 2013; Yesavage et al., 1983) and self-rated mental health (Medical Outcomes Survey Short Form [SF-12] Mental Composite Score; Ware, Kolinski, Turner-Bowker, & Gandeck, 2002), (e) social support (Medical Outcomes Study Social Support Survey; Gomez-Campelo et al., 2014; Sherbourne & Stewart, 1991), (f) physical function (Katz Index of Independence in Activities of Daily Living; Katz, Ford, Moskowitz, Jackson, & Jaffe, 1963), and (g) general health perception (self-rated physical health, SF-12 Physical Composite Score; Ware et al., 2002).
Statistical Analyses
Counts of health care transitions at each data collection point formed the basis for the use of longitudinal multivariable Poisson regression modeling within a generalized estimating equation framework to examine the relationships between health care transitions and potential baseline predictors. The Poisson regression models incorporated an offset to accommodate varying days at risk within each time period. This approach considers censoring for those that drop out of the study. Potential covariates identified in simple main effects and two-way interaction-with-time models were reviewed and included in the building of a final model if the p value was ≤ .20 (Vittinghoff, Glidden, Shiboski, & McCulloch, 2005). An initial multivariable Poisson regression model was constructed for the primary outcome (i.e., total number of health care transitions) using covariates significantly associated with this outcome and the interaction with time, followed by sequentially eliminating interactions on the basis of least significance until all interaction effects demonstrating significance at the p ≤ .20 level remain. Covariates not included in the final interaction model but were significant in the main effect models at the p ≤ .20 were then added to the final multivariable interaction model and assessed similarly. The final multivariable Poisson regression model included only interaction terms and covariates demonstrating statistical significance at the p ≤ .05 level or based on the literature (i.e., age). Due to known confounding between LTSS type and race (White: ALC, 94%; NH, 33%; HCBS, 27%) and ethnicity (Hispanic: ALC, 2%; NH, 4%; HCBS, 54%) in this data set (Naylor et al., 2016), neither race nor ethnicity were included in the multivariable modeling. All analyses were performed using SAS 9.4 (SAS Institute, Inc., Cary, NC).
Results
Sample Characteristics at Baseline
Sociodemographic and clinical characteristics of the 470 LTSS recipients at study enrollment are presented in Table 1. On average, LTSS recipients were 81 years old (range = 60-98); female (71%), widowed (52%), and 85% had five or more chronic health conditions documented in their medical records. Fifty-one percent of the LTSS recipients were White, 34% African American, and 12% reported more than one race. Twenty percent of LTSS recipients identified as Hispanic, with 16% of interviews being conducted in Spanish. The majority (64%) of the LTSS recipients had 12 years of education or higher. LTSS recipients were evenly split between the three types of LTSS: NH, n = 158; ALC, n = 156, HCBS, n = 156. Twenty-one percent (101/407) of LTSS recipients reported being hospitalized in the 3 months prior to their starting LTSS. At study enrollment, 60% of LTSS recipients had little or no cognitive impairment (MMSE = 24-30), 24% had mild deficits in cognition (MMSE = 19-23), and the remaining 16% had MMSE scores in the moderate range (MMSE = 12-18). At baseline, LTSS recipients frequently (43%) reported depressive symptoms, indicated by GDS-SF Scale scores ≥ 5, suggesting mild to severe depression (Yesavage et al., 1983). Overall self-rated mental health, as measured with the SF-12 Mental Composite Score, had a mean score of 37, lower than the norm of 50. Overall general health perception, as measured by the SF-12 Physical Composite Score, was 49.0 (norm = 50). LTSS recipients reported on average 6 bothersome symptoms at baseline (range = 0-13). Thirty percent reported their overall quality of life “excellent” or “very good,” 33% reported their overall quality of life was “good,” and 35% reported their overall quality of life was “fair” or “poor.”
Sociodemographic and Clinical Characteristics of Older Adults Receiving Long-Term Services and Supports, n = 470.
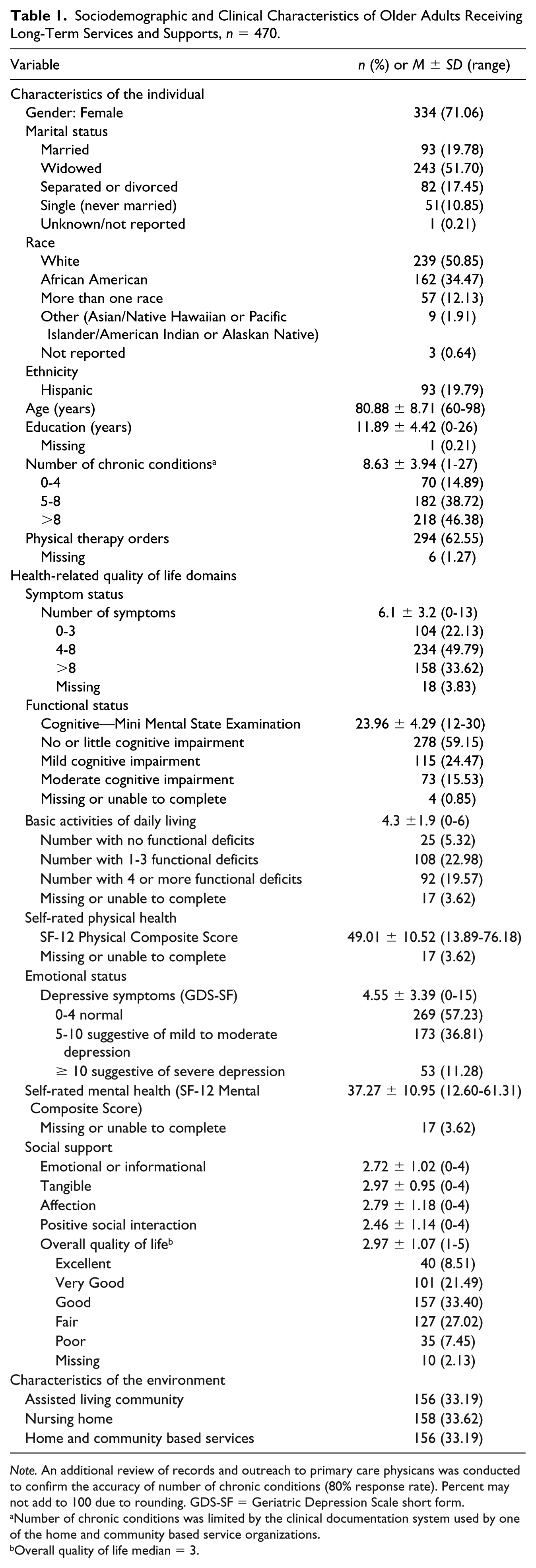
Note. An additional review of records and outreach to primary care physicans was conducted to confirm the accuracy of number of chronic conditions (80% response rate). Percent may not add to 100 due to rounding. GDS-SF = Geriatric Depression Scale short form.
Number of chronic conditions was limited by the clinical documentation system used by one of the home and community based service organizations.
Overall quality of life median = 3.
Total Number of Health Care Transitions
Counts by type of health care transition at each quarterly assessment are presented in Table 2. In the 3 months prior to the start of LTSS, both ALC and NH groups experienced slightly more health care transitions (ALC [mean ± standard deviation (SD)] = 0.7 ± 1.0, range = 0-5; NH = 0.7 ± 0.9, range = 0-4) than HCBS (mean ± SD = 0.3 ± 0.7, range = 0-5). A total of 1,294 health care transitions occurred among all LTSS recipients from the 3 months prior to LTSS through the 24 months follow-up period. The most common health care transitions were hospitalizations (654/1,195, 55%), followed by ED visits that did not result in a hospitalization (314/1,195, 26%) and transfers to SNFs or IRFs for short-term rehabilitation (133/1,195, 11%). The average number of transitions over the first 12 months was (M ± SD): NH = 2.0 ± 2.5; ALC = 1.4 ± 1.8; HCBS = 1.3 ± 2.0; and greater than 12 to 24 months were NH = 1.3 ± 2.0; ALC = 1.2 ± 1.7; HCBS = 1.3 ± 1.7. Over the full 24 months, the group that started in NHs had an average of 3.0 transitions (SD ± 3.5); ALCs had an average of 2.2 health care transitions (SD ± 2.6); and HCBS had an average of 2.4 health care transitions (SD ± 2.7). Very few people experienced transitions associated with increasing intensity of LTSS (57/1,195, 5%). The number of transitions to hospice care also was small, accounting for about 3% (37/1,195) of all transitions and only 8% of all LTSS recipients (37/470 recipients). A total of 100 participants died and 34 withdrew (7%) over the 24 months.
Counts of Health Care Transitions and Deaths Among LTSS Recipients Over Time (Months).
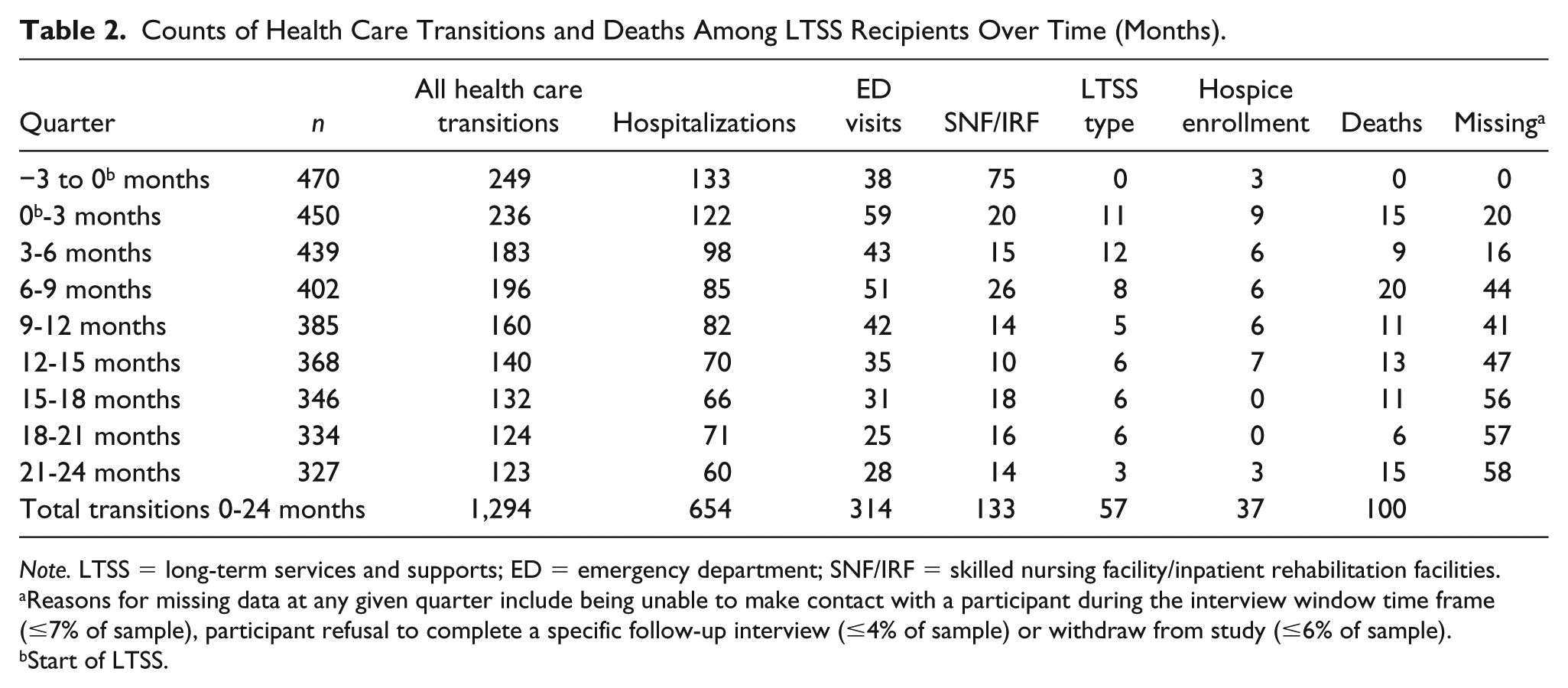
Note. LTSS = long-term services and supports; ED = emergency department; SNF/IRF = skilled nursing facility/inpatient rehabilitation facilities.
Reasons for missing data at any given quarter include being unable to make contact with a participant during the interview window time frame (≤7% of sample), participant refusal to complete a specific follow-up interview (≤4% of sample) or withdraw from study (≤6% of sample).
Start of LTSS.
Multivariate Regression Findings
The final multivariate Poisson regression model, as depicted in Table 3, revealed that several baseline covariates were associated with health care transitions in this sample. Overall, male LTSS recipients had a 32% higher risk of having health care transitions (male relative risk [RR] = 1.32; 95% confidence intervals [CI] = [1.07-1.63]; p = .009). For each additional chronic condition, LTSS recipients had a 3% higher risk of health care transitions (RR = 1.03; 95% CI = [1.00, 1.06]; p = .026). LTSS recipients with lower self-rated physical health had a higher risk of health care transitions (for every 10-point decrease in the SF-12 self-rated physical composite score, the risk of any transition increased 10%; RR = 0.90; 95% CI = [0.82, 0.99]; p = .03). Finally, LTSS recipients with lower ratings of self-reported overall quality of life had a higher risk of health care transitions (RR = 0.90; 95% CI = [0.81, 0.99]; p = .035). The number of transitions at the start of LTSS was highest for those who rated their quality of life as poor (the lowest rating) at baseline compared with those who rated their quality of life as excellent (highest rating); the latter group had the fewest number of transitions.
Multivariable Poisson Regression Model Results for Number of Transitions Over Time (Baseline to 24 Months by Quarter).
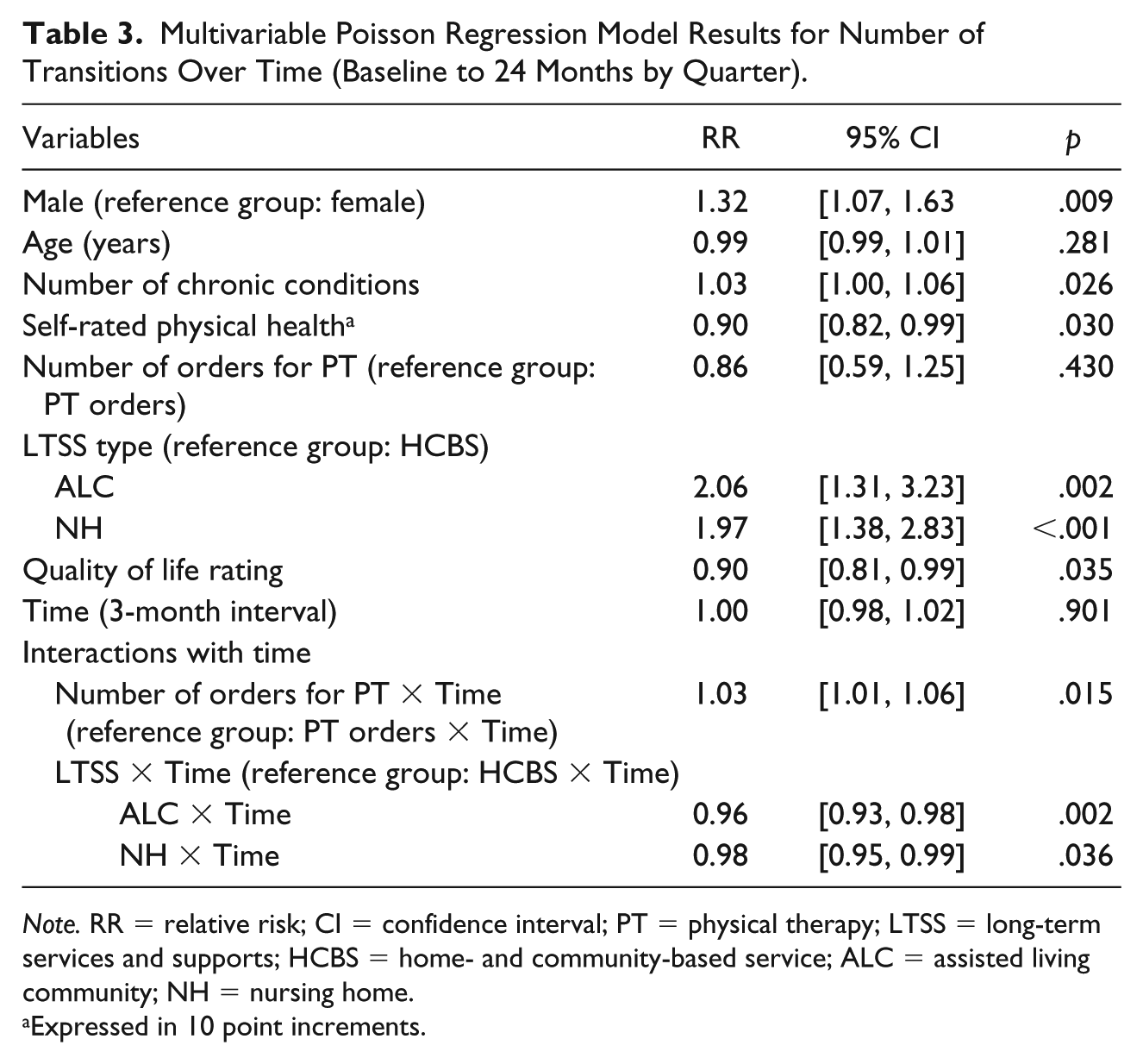
Note. RR = relative risk; CI = confidence interval; PT = physical therapy; LTSS = long-term services and supports; HCBS = home- and community-based service; ALC = assisted living community; NH = nursing home.
Expressed in 10 point increments.
Two baseline covariate interactions with time were statistically significant: having physician orders for physical therapy at the start of LTSS (Figure 1a) and initial LTSS type (Figure 1b). LTSS recipients who did not have physicians’ orders for physical therapy at the start of LTSS experience 3% higher risk of health care transitions with each additional month relative to LTSS recipients with a physical therapy order (RR = 1.03; 95% CI = [1.01, 1.06]; p = .015). As seen in Figure 1a, LTSS recipients who did not have physicians’ orders for physical therapy at baseline had fewer transitions during the first 12 months but demonstrated a slight increase in health transitions between months 12 and 24; whereas, those with physicians’ orders for physical therapy at baseline experienced an overall decline in health care transitions over time. Similarly, the baseline LTSS type was significantly associated with health care transitions over time (Figure 1b). The health care transitions profile among respondents who started in ALCs and NHs differs significantly from those who start LTSS in HCBS. Specifically, those in ALCs experience a 4% lower risk of health care transitions with each additional month relative to those in HCBS. Similarly, participants in NH facilities experience a 2% lower risk of health care transitions with each additional month relative to those in HCBS (RR = 0.96; 95% CI = [0.93, 0.98]; p = .002) or NH setting (RR = 0.98; 95% CI = [0.95, 0.99]; p = .036).

Interactions between baseline physical therapy and LTSS type over time: (a) Transitions over time by baseline physical therapy and (b) transitions over time by baseline LTSS type.
Discussion
As the population of older adults is expected to double in the coming years, so too will the number of LTSS recipients—a population with high risk for poor health outcomes resulting in transitions to acute hospitals (Ortman, Velkoff, & Hogan, 2016). In this study, framed with Andersen’s (1995) Behavioral Model of Health Service Use, the total number of health care transitions is described from prior to the start of LTSS through the first 2 years of LTSS for 470 English- and Spanish-speaking older adults and identified unique participant characteristics associated with health care transitions that predicted changes over time. These findings have several implications.
First, our findings suggest that LTSS recipients commonly experience health care transitions to and from both acute and non-acute settings of care. Although much of the health care transitions literature for LTSS recipients has focused on acute hospitalizations (Becker, Boaz, Andel, & DeMuth, 2012; Berish, Applebaum, & Straker, 2016; Cai & Temkin-Greener, 2015; McAndrew, Grabowski, Dangi, & Young, 2016; Sonnega, Robinson, & Levy, 2017), our study also examined non-acute care transitions (e.g., transitions to SNF/IRF settings, to hospice, between LTSS settings), which is a unique contribution to the literature. These non-acute care transitions accounted for 17% of the transitions occurring during the first 24 months of care for LTSS recipients. The prevalence of these transitions suggests the need for transitional care services in areas that are not commonly examined, yet have high risk for breakdowns in communication, poor hand offs, and limited care continuity (Becker et al., 2012; Cai & Temkin-Greener, 2015; Sonnega et al., 2017). In addition, in this prospective study, more health care transitions were observed among older adults in NHs (average 2.0) than in ALCs and HCBSs (averages 1.4 and 1.3, respectively) over the first 12 months period. A similar rate of health care transitions was found in a larger study of older adults who received both short- and long-term NH care (average 2.1 transitions; Li et al., 2018). We recognize that death is qualitatively different from the other health care transitions examined, however, the final outcome model with and without death changed only slightly, and the inclusion of death in the count resulted in a more clinically meaningful result.
Our findings suggest that, for LTSS recipients in residential settings of care, the number of health care transitions is higher at the start of services and decrease over time, while those receiving HCBS have a constant low number of transitions over the 2 years (Figure 1b). One implication from this finding is the need for detailed studies of care coordination and nursing care provided by HCBS programs and the impact on function and health care transitions. Moreover, additional examination of health care transitions over time for older adults, including non-acute health care transitions, will provide the basis to adapt transitional care interventions to meet the unique need of LTSS recipients.
Our findings support earlier studies demonstrating individual need, access, and predisposing factors that predict health care use (Becker et al., 2012; Grabowski, Stewart, Broderick, & Coots, 2008; O’Connor et al., 2016; Toles et al., 2014); specifically, important HRQoL domains and characteristics of LTSS recipients influence the number of health care transitions experienced among this population. Although available literature describes predictors of hospitalizations (Becker et al., 2012; Grabowski et al., 2008), this is the first study to find that older adults with physicians’ orders for physical therapy at the start of LTSS, compared with those without physical therapy orders, had fewer health care transitions. This finding suggests the hypothesis that targeting high-risk older adults and implementing preventive strategies, such as physical therapy services, may prevent avoidable health service use. Future research and quality improvement initiatives are necessary to explore this hypothesis. Similarly, LTSS recipients’ self-reporting higher quality of life at the time of LTSS enrollment was highly associated with the number of health care transitions over time. This finding suggests that using a single-item assessment of overall quality of life can provide valuable information for LTSS providers and identify LTSS recipients with the greatest need for intervention(s) to improve quality of life, such as focusing on maintaining autonomy, dignity, and spiritual well-being (Burack, Weiner, Reinhardt, & Annunziato, 2012).
Our finding that gender was associated with the number of transitions has not been seen in previous literature. There is limited research that supports that older male ALC and NH residents are at high risk of hospitalizations and that male HCBS recipients are at higher risk of transitioning to NHs and needing short-term SNF/IRF stays (Becker et al., 2012; Cai & Temkin-Greener, 2015; Grabowski et al., 2008). Furthermore, one study suggests the relationship with gender and long-term care transitions is associated with relationship status and available support in the community (Mudrazija, Thomeer, & Angel, 2015). More research into the relationship with gender and the number of health care transitions among LTSS recipients is needed.
Finally, our finding that lower ratings of general health perceptions and numbers of chronic conditions were significant predictors of the number of health care transitions is supported in the literature; however, participant age and symptoms were not statistically significant in this study, even though they were found to be influential in the transition to LTSS and use of health care resources in other studies (Becker et al., 2012; Grabowski et al., 2008; Menec, Nowicki, Blandford, & Veselyuk, 2009; Sonnega et al., 2017). Sensitivity analyses were conducted with the most common transition, hospitalizations, and no symptoms were statistically significant predictors of hospitalizations.
Limitations
This study has several limitations, which we attempted to mitigate. Both self-report and chart review data were used to capture the outcome. Although there are limitations to using solely self-report or chart review data, our approach using both types allowed us to capture as much data pertaining to a range of transitions in care as possible. The data set consisted of ALC, NH, and HCBS organizations on the east coast of the United States and a more geographically diverse, nationally representative sample may yield different results. The primary outcome, the count of health care transitions, counted each transition as a single event, which is consistent with other literature on hospitalizations and ED visits (Intrator et al., 2007; McAndrew et al., 2016; Wang et al., 2017). For example, a transfer from the ALC to the ED that resulted in a hospital admission, followed by the return to the ALC, was counted as a single health care transition. In addition, the duration (e.g., 1 hour, 1 week, 1 month) and intensity of a health care transition were not captured in the data set and, thus, a loss of granularity in the impact of these transitions on this population. Future research should capture these detailed data, which would add to the growing body of literature on multiple health care transitions as well as provide the basis for understanding individual health care transition patterns for this population. As noted in the methods, race and ethnicity were confounded with LTSS type in this data set. It is possible that differences by LTSS type may be highlighting unique differences by race and/or ethnicity and socioeconomic status. For example, the ALC group was 94% White and 2% Hispanic, and the NH group was 33% White and 4% Hispanic whereas within the HCBS group there was a great mix of race and ethnicity (27% White, 54% Hispanic). Therefore, subgroup comparisons were not possible due to the complete imbalance between race and ethnicity by LTSS type. Future prospective studies should make a concerted effort to balance on race and ethnicity in order to compare health care transition by LTSS type. Finally, the variable for chronic conditions was a total count of health conditions and not organized by specific conditions. Future research looking at specific conditions such as heart failure, diabetes, and dementia should be conducted to determine if there are any unique or common transitions patterns.
Conclusion
Our findings on the importance of gender, quality of life, number of chronic conditions, and self-rated physical health at the start of LTSS as predictors of future transitions in health care, support the need for LTSS providers to be especially vigilant in anticipating risk for LTSS recipients. By incorporating an assessment of self-rated physical health and quality of life in discussions about goals and preferences for care and in communication with primary care clinicians at the start of LTSS, potentially fewer health care transitions may be seen. As the population of older adults receiving LTSS services continues to grow, the need to understand the nature of health care transitions will also increase. These findings support the need to use a broader definition of “health care transition” to achieve more person-centered, effective, and efficient allocation of resources. In addition, the findings suggest next steps for minimizing the risk of potentially preventable transitions, such as evaluating the need for physical therapy consultations for newly admitted LTSS recipients. Finally, additional longitudinal studies are warranted to identify strategies to enhance transitions in care among LTSS recipients.
Footnotes
Acknowledgements
The authors would like to thank Bridget Daly for her assistance with initial statistical analyses. They would like to thank all the participants in this study and the multiple organizations that assisted in recruiting the study sample.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a pilot grant from the NewCourtland Center for Transitions and Health at the University of Pennsylvania School of Nursing. The data set used in these analyses was supported by a cosponsored grant from National Institutes of Health—National Institute on Aging and the National Institute of Nursing Research (R01AG025524), as well as the Marian S. Ware Alzheimer Program at the University of Pennsylvania.