
Abstract
Caregiving for older adults with cognitive impairment can be more difficult as caregivers are required to perform medical/nursing tasks at home. Little is known about medical/nursing tasks and their relationship to caregivers’ characteristics and their effects on caregiver burden. Secondary data analyses were conducted with 423 caregivers of individuals with cognitive impairment from the 2015 National Alliance for Caregiving (NAC) and American Association of Retired Persons (AARP) data. In terms of the caregiving context, caregivers who performed medical/nursing tasks lived with the care recipients and provided longer hours of care than caregivers who did not perform medical/nursing tasks. When caregivers delivered medical/nursing tasks, they were 2 times more likely to experience higher levels of caregiver burden. Medical/nursing tasks can exacerbate caregiver burden. Health care providers’ explanations of the needs and the benefits of performing medical/nursing tasks, as well as education and training for the tasks, are needed to reduce caregiver burden.
Introduction
Caregiving, generally by family members, friends, or neighbors, is critical for older adults, especially those with cognitive impairment. Older adults with cognitive impairment have a noticeable decline in one of the intellectual domains, such as memory, language, or executive functioning (American Psychiatric Association, 2013). Up to 42% of adults, aged 65 years or older, have cognitive impairment (U.S. Preventive Services Task Force, 2016). Due to the cognitive decline, older adults with cognitive impairment often need more assistance in their day-to-day functions, such as balancing a checkbook, driving a car, or finding housing (Geda, 2012). In addition to these tasks, caregivers of individuals with cognitive impairment (ICI) may be asked to perform medical/nursing tasks because there have been increasingly shorter hospital stays, increased complexity of acute and chronic disease management, as well as improvement in medicine and technology. As a result, caregivers are being asked to do more (Keeling, 2014; Reinhard, Levine, & Samis, 2012). Medical/nursing tasks are skilled activities, such as dealing with wound and ostomy care, incontinence care, complex medication regimen, as well as handling assistive mobility devices and medical equipment (Reinhard et al., 2012). Performing medical/nursing tasks may add difficulty and burden to the caregivers’ experience as those tasks require caregivers to balance the risks and benefits of medication and the management of the acute exacerbation of the chronic diseases of care recipients (Poland et al., 2014; Sadak, Zdon, Ishado, Zaslavsky, & Borson, 2017).
Research shows that caregivers’ involvement in medical/nursing tasks is prominent when caring for cognitively impaired older adults. Two recent studies analyzed a national sample of older adults and both reported that when older adults received help with a physician’s visit and medication management, the older adults were more likely to have cognitive impairment (Wolff & Spillman, 2014; Wolff, Spillman, Freedman, & Kasper, 2016). Moreover, those with cognitive and behavioral conditions more frequently visited acute care services (Reinhard et al., 2012). Finally, another national report suggested that care recipients with cognitive and behavioral conditions more often had caregivers involved in medical/nursing tasks (Reinhard et al., 2012).
Review of Relevant Literature
Delivering medical/nursing tasks for older adults with cognitive impairment can be more challenging than providing medical/nursing tasks for older adults without cognitive impairment. Caregivers of ICI are 2 times (22% vs. 11%) more likely to report difficulty in performing medical/nursing tasks than caregivers with other chronic diseases (National Alliance for Caregiving [NAC] & Alzheimer’s Association [AA], 2017). The notable difficulty of completing medical/nursing tasks among caregivers of ICI may originate from care recipients’ unique disease process and comorbidities. Cognitive impairment causes forgetfulness of important information, difficulty with counting, having distorted visual images, and making poor decisions (AA, 2018). Due to those limitations, caregivers of ICI may have to be involved not only with simple tasks, such as daily living activities, but also with more complicated tasks. One study reported that caregivers of ICI needed to be hypervigilant and be constantly engaged in medication management, such as refilling prescriptions, reminding to take medications, and being watchful to follow instructions from the pharmacist (Gillespie, Harrison, & Mullan, 2015).
In addition, given that age is the greatest risk factor in cognitive impairment, most ICI are older and have increased chronic conditions, such as stroke/hypertension, diabetes, cardiac disease, musculoskeletal disabilities, and hearing or vision problems (AA, 2018; Reinhard, Samis, & Levine, 2014). The average age of ICI has been reported as 77.2 years, which was 5 years older compared with care recipients without cognitive impairment (NAC & AA, 2017). According to a study that analyzed Medicare beneficiary data, older adults with cognitive impairment have more comorbidities (8.1 vs. 6.5) compared with the same age group of older adults (Zhao, Kuo, Weir, Kramer, & Ash, 2008). Similar to that study findings, another study reported that caregivers of ICI manage an average of nine medical conditions and administer more than 10 medications to the care recipients (Erlen et al., 2013). The higher comorbid conditions can influence caregivers to manage not only multiple medications but also frequent procedures and treatments.
In addition, nearly half of ICI tend to have challenging behaviors, such as being agitated, aggressive, suspicious, and depressed (Reinhard et al., 2014), and caregivers of ICI said that they experienced at least one challenging behavior weekly (Hansen, Hodsgon, Budhathoki, & Gitlin, 2020). Caregivers of ICI reported that they were considerably upset by the behaviors, and they were not confident in managing those behaviors (Hansen et al., 2020). When care recipients had challenging behaviors, caregivers often faced resistance from the care recipients for helping with the medical/nursing tasks (Reinhard et al., 2014). In more severe cases, caregivers reported that sometimes care recipients were being paranoid about taking medications or thinking pills are poisonous (Kaasalainen et al., 2011).
Finally, 53% of caregivers of ICI perform the tasks without training (NAC & AA, 2017). Without proper support and training from health care professionals, caregivers of ICI may not have confidence in completing medical/nursing tasks or sometimes may even find their decisions have caused harm to the care recipients (Ball et al., 2015; Poland et al., 2014). Caregivers reported that more training would be particularly helpful in medication and wound management (Reinhard et al., 2012), and training may enable frontline caregivers to minimize errors and adverse events in patient safety issues (Thomas & Classen, 2014).
Although daily and personal care in relation to caregiver burden and caregiving context have been extensively researched, there is limited evidence about medical/nursing tasks performed by the informal caregivers of ICI (Reinhard et al., 2012). To date, several studies found that having reduced cognitive functioning was a marked incidence for caregivers’ involvement in medical/nursing tasks but their findings were descriptive (Reinhard et al., 2012; Wolff & Spillman, 2014; Wolff et al., 2016). As stated above, the existing literature provided some linkage between medical/nursing tasks and caregiver burden, such as care recipients’ memory loss, challenging behaviors, older age, comorbidities, frequent health care use, and lack of training from health care providers. However, the literature has yet to clearly address whether medical/nursing tasks are burdensome for the caregivers of ICI.
In summary, comparison analysis on those who perform medical/nursing tasks versus those who do not perform medical/nursing tasks is lacking and may provide some distinctive insights on the caregivers’ characteristics and needs from health professionals related to medical/nursing tasks. The quantitative effect of performing medical/nursing tasks for ICI on caregiver burden is vague, even though qualitative caregiving literature clearly reports the negative impact of performing medical/nursing tasks, such as experiencing anxiety, worry, and stress when performing medical/nursing tasks (Ball et al., 2015; Poland et al., 2014).
Aims
The aims of the study are (a) to examine differences in caregivers’ background characteristics and caregiving context between the group performing medical/nursing tasks versus the group not performing the tasks and (b) to investigate the effect of performing medical/nursing tasks on caregiver burden.
Conceptual Framework
Pearlin’s stress process model was used as the underpinning conceptual framework for this study (Pearlin, Mullan, Semple, & Skaff, 1990). The stress process model was developed to understand a caregiver’s stress, particularly when caregivers take care of ICI. According to the model, stress occurs over time and is interrelated with multidimensional domains, such as the caregivers’ backgrounds, primary stressors, and secondary stressors. Backgrounds included caregivers’ sociodemographic characteristics and influence on the degree of caregiver stress as they interrelate with caregivers’ role and resources in social and economic aspects. The primary stressors are related to the care recipients’ status and caregivers’ subjective appraisal on caregiving. Primary stressors may increase when care recipients have severe symptoms because the caregiving loads are heightened. Moreover, when caregivers perceive the caregiving role as burdensome, the primary stressors become intensified. Secondary stressors are the consequences of the primary stressors, such as struggle with family, job, and social life. Caregiver burden is the most common and major psychological outcome and encompasses caregivers’ physical, emotional, and financial aspects.
Using this conceptual framework, caregivers’ backgrounds and primary stressors (caregiving context) were examined in this study to explain caregiver burden (Figure 1). As this study used secondary data analysis, variables were selected within the availability of the data set. Specifically, the variables used for caregivers’ backgrounds included age, gender, educational level, annual income, health status, and relationship to care recipients. The primary stressors as caregiving context variables included average weekly hours of care provided, length of time care provided, living with care recipients, and having a choice about caregiving.
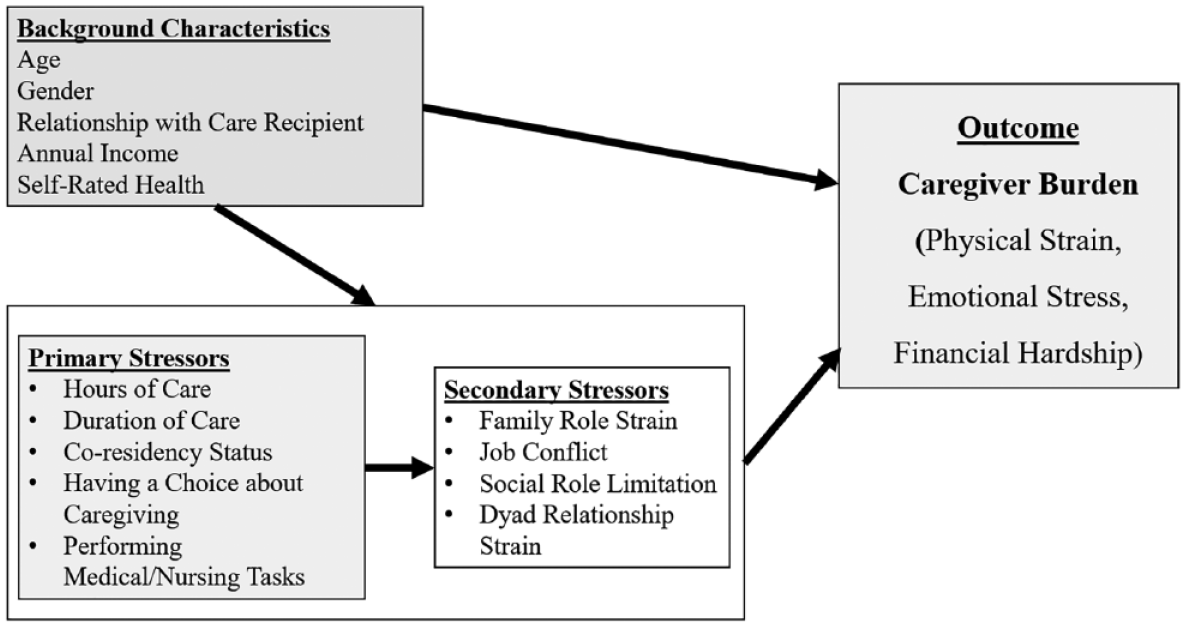
Conceptual framework.
Method
This cross-sectional and correlational study was conducted by using secondary data analysis. The original data were collected by the NAC and the American Association of Retired Persons (AARP) and released in 2015.
Data Collection
The 2015 NAC/AARP data consist of 1,248 nationally representative caregivers in the United States (NAC & AARP, 2015). A professional market research institute, Growth from Knowledge (GfK), recruited family and friend caregivers from September 18 to November 5, 2014. The GfK selected the possible participants by a random selection of telephone numbers and residential addresses as well as by oversampling of racial and ethnic minority groups (African Americans, Hispanics, and Asian Americans). The caregiver participants were included if they met the following inclusion criteria: (a) informal caregivers (who provide unpaid care), (b) adult (age equal to and older than 18 years), (c) providing care within the last 12 months at the time of original data collection, and (d) caring for household members or friends in the community, but caregivers did not need to live with the ICI, although they could do so. Those who were randomly selected and met the inclusion criteria were invited as part of a KnowledgePanel® by participating in an online interview.
Subjects
In this study, cognitive impairment is defined as a decline in memory, because memory loss is the most common symptom and the first symptom recognized in cognitive impairment diseases as intellectual domains of the brain weaken (AA, 2017; Jahn, 2013). Thus, the 2015 NAC/AARP data analysis included informal caregivers who reported that their care recipients needed care because of a memory problem (n = 451). The selected sample for this study was examined for the amount of missing data and the missing mechanism. The missing data were small (<5%) and the missing data were completely missing at random (Little’s test of missing completely at random, p = .262). List-wise deletion was performed, and given that there was no bias of list-wise deletion with missing data, it was determined that data were completely missing at random (Peugh & Enders, 2004). After the list-wise deletion for missing data was adjusted, the total sample size was 423 (Figure 2).
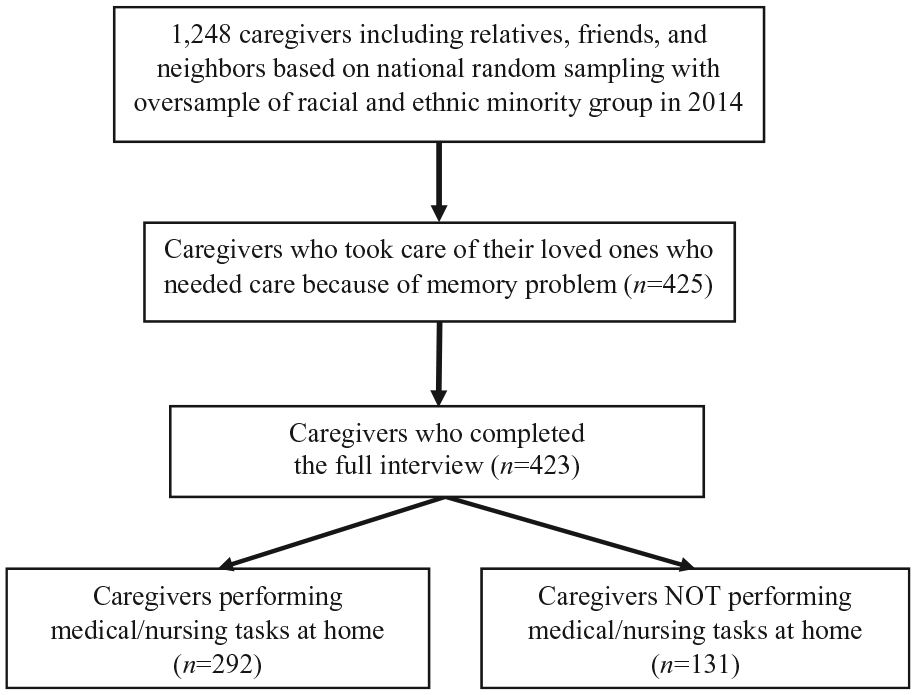
Flowchart of sample with the unweighted final sample (n = 423).
Measures
Caregivers’ background characteristics
Informal caregivers’ background characteristics included age, gender, educational level, annual income, health status, and relationships to care recipients. Relationships to care recipients were categorized into parents or grandparents, spouse or partner, other relatives, and friends or neighbors. Caregivers’ educational level was classified as high school or less, and some college or higher. Annual income was dichotomized at US$50,000, based on the 50th percentile income of the United States (DeNavas-Walt & Proctor, 2015). Caregivers’ health status was measured by a 5-point Likert-type scale of self-rated health. The Self-Rated Health scale validly and sensitively reflected the current health status of caregiver and ranged from 1 = poor, 2 = fair, 3 = good, 4 = very good, and 5 = excellent (Mavaddat, Parker, Sanderson, Mant, & Kinmonth, 2014).
Caregiving context
The caregiving context included average weekly hours of care provided, length of time care provided (years), whether the caregivers lived with the care recipients (co-residence, yes/no), whether the caregivers felt they had a choice in engaging in the caregiving role (yes/no), and performing medical/nursing tasks (yes/no). A caregiver was considered to perform medical/nursing tasks, if he or she reported that he or she managed medications (i.e., pills, eye drops, or injections), prepared food for special diets, administered tube feedings, managed wound care, monitored blood pressure or blood sugar, helped with incontinence, or operated medically necessary equipment (NAC, 2015).
Caregiver burden
The NAC and AARP developed a set of caregiver burden questionnaire using three items. The three items were physical strain, emotional stress, and financial hardship. Each item used a 5-point Likert-type-scale that ranged from 1 to 5 (not a strain at all = 1, very much of a strain = 5). Sum scores were created for each participant by adding the three items together for an overall burden score. To separate caregivers with higher versus lower burden group, the mean of overall burden score was used (M = 8.21, SD = 3.03, range = 3-15). Overall score ≤8 was categorized into lower burden group and overall score >8 was categorized into higher burden group. Using this brief scale, the reliability coefficient was high for this study data set (Cronbach’s α = .74) and was consistent with a previous study using these same items (Kim, Chang, Rose, & Kim, 2012).
Data Analysis
Mean comparison using independent t tests and chi-square tests
Descriptive statistics were performed to describe caregivers’ background characteristics and caregiving context using means with standard deviations (SDs) and percentages for categorical variables. Independent t tests and chi-square tests were conducted to compare the difference of caregivers’ background and caregiving context between the group performing medical/nursing tasks versus the group not performing medical/nursing tasks. The length of time provided care (years) was transformed using a natural log function to adjust for its univariate abnormality.
Logistic regression
Binary logistic regression (Nelder & Wedderburn, 1972) was used to identify significant predictors of being in the higher caregiver burden group. Dementia caregivers’ background characteristics and caregiving context were used, and the statistical model for Pi (ith participant’s probability of being in the higher caregiver burden group), can be written as follows.
where β1 is a slope coefficient for the relation between the logit of Pi and age, β2 is for gender, β3 is for relationship to the care recipient, β4 is for annual income, β5 is for self-rated health, β6 is for weekly hours of care provided at average, β7 is for length of time provided care, β8 is for living with care recipient, β9 is for caregiving without choice, and β10 is for performing medical/nursing tasks. There was no multicollinearity among independent variables (variance inflation factors [VIF] < 1.35) and no abnormality in the multivariate normal distribution. The level of significance of .05 and two-tailed test were used.
Weighting
A single-stage weighting was used to produce representative estimates for national caregivers at the population level. The used data set for the study had oversampled the ethnic minority groups; thus, the weight was applied to yield the same distribution on demographic descriptive results as the population (Kish & Frankel, 1974). In the same way, the weighting was applied into the estimation of regression models particularly when the sampling selection process is nonignorable (Kott, 2007). When applying weights, the inferential statistics can provide unbiased and representative coefficients. The NAC and AARP (2015) released the weight variable within the data set and the weight was based on age, sex, and race/ethnicity from the Current Population Survey performed by the U.S. Census Bureau. IBM SPSS Version 23 (IBM Corp., 2015; Armonk, NY) was used for all data analyses.
Results
Caregivers’ background and caregiving context
Caregivers’ background characteristics and caregiving context are presented in Table 1. The average age of caregivers was 56.99 years (SD = 17.27 years). The majority of caregivers were female (60.7%) and White (68.8%). About half of the caregivers took care of parents or grandparents (55.2%), had some college or higher education (66.1%), and had more than a US$50,000 annual income (54.6%). The average self-rated health was 3.24 (SD = 0.99), which meant caregivers reported their overall health a little higher than good.
Descriptive Statistics (Weighted): Demographics.
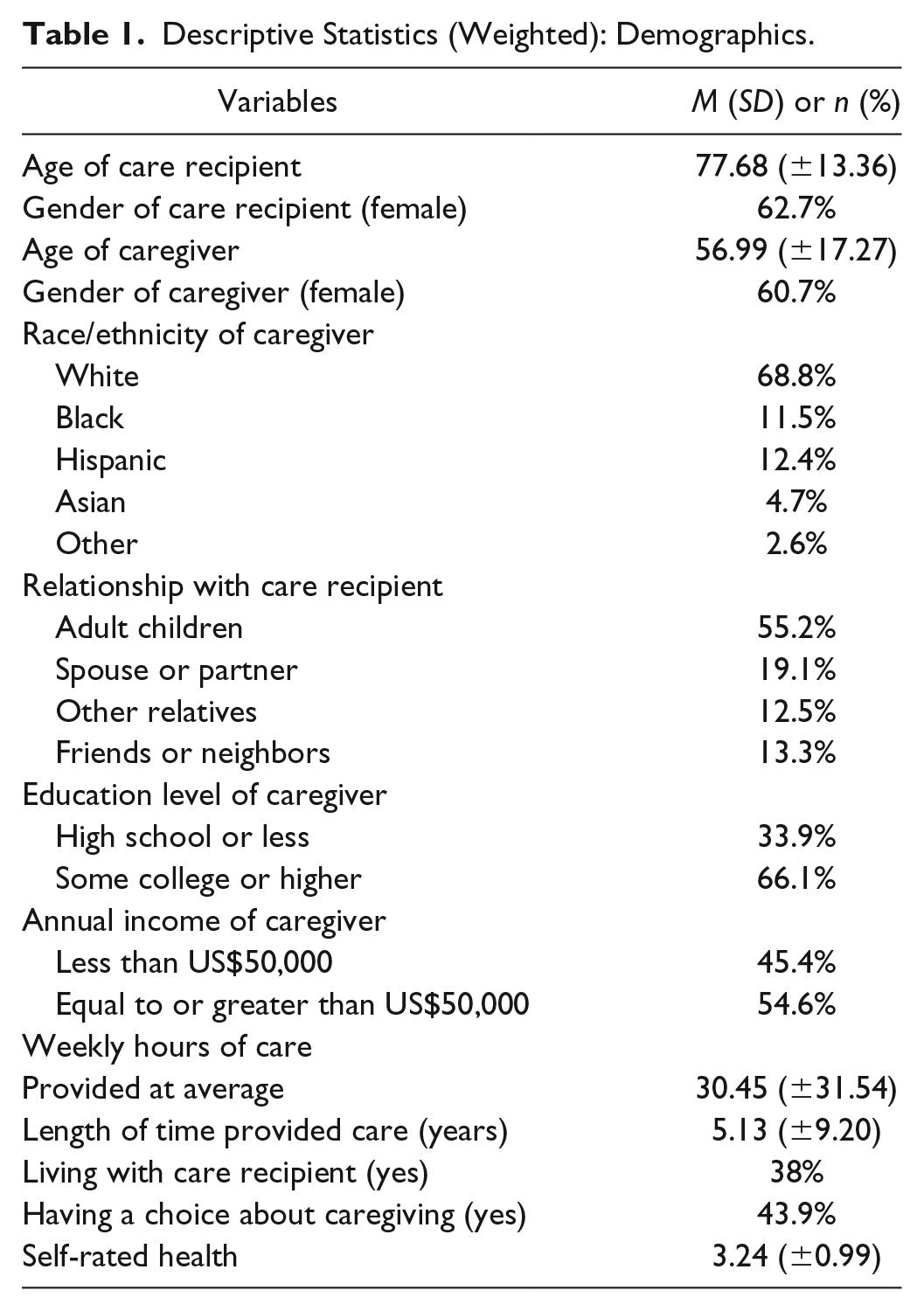
The average weekly hours of care were 30.45 hr (SD = 31.54 hr) and the average length of care was 5.13 years (SD = 9.20 years). Approximately one third of the caregivers lived with the care recipients (38%), more than half of caregivers felt they “had no choice” of caregiving (56.1%), and about two thirds of caregivers performed medical/nursing tasks (69%). The average caregiver burden was 8.21 (SD = 3.03) and the range was 3 to 15.
Comparison between performing medical/nursing tasks group versus not
As shown in Table 2, the group difference between the group performing medical/nursing tasks versus the group not performing medical/nursing tasks is presented. The caregiver’s relationship to the care recipient was significantly different between the groups (χ2 = 27.503, p < .0001). Specifically, caregivers who performed medical/nursing tasks were more likely to be a spouse or partner of the care recipient (24.6% vs. 6.4%), whereas caregivers who did not perform medical/nursing tasks were more likely to be a friend or neighbor (23.9% vs. 8.7%). There was no significant difference in age, gender, income, or self-rated health between the two groups.
Comparison of Sociodemographic Characteristics of Informal Caregivers in Performing Medical/Nursing Tasks Group Versus Not (Weighted).
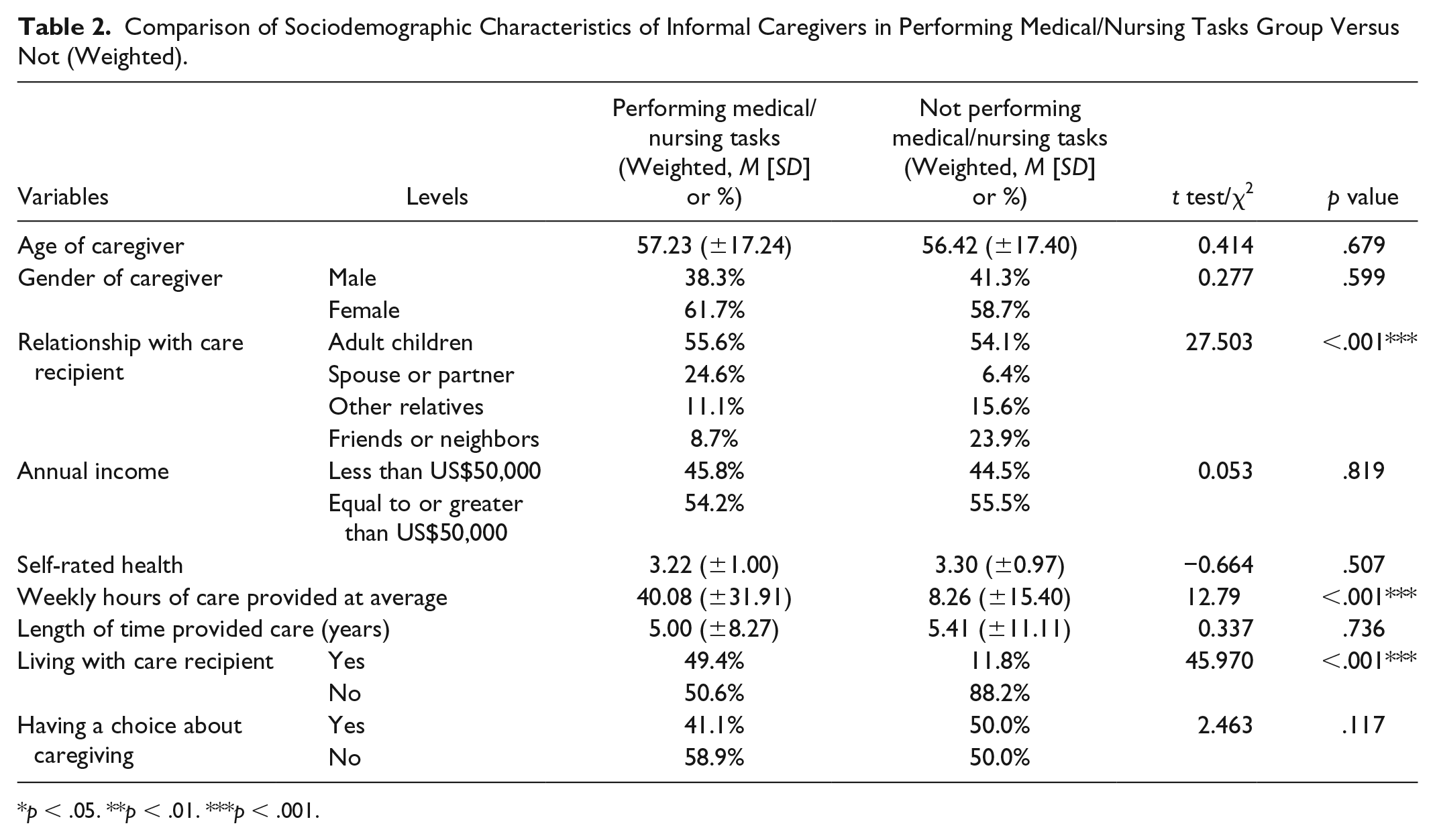
p < .05. **p < .01. ***p < .001.
Significantly, more caregivers who performed medical/nursing tasks lived with care recipients (49.4% vs. 11.8%; χ2 = 45.970, p < .0001) and they provided longer hours of weekly care (40.1 vs. 8.3 hr; t = 12.79, p < .0001). There was no significant difference in length of time providing care (years) and having a choice about caregiving between the two groups.
Factors associated with predictors of being in the higher caregiver burden group
As presented in Table 3, the odds ratios (ORs) and unstandardized beta coefficients (b) of the binary logistic regression analyses of the effects of caregivers’ backgrounds and caregiving context on caregiver burden are reported.
Binary Logistic Regression Models of the Effects of Caregivers’ Background Characteristics and Caregiving Context on Caregiver Burden (Weighted).
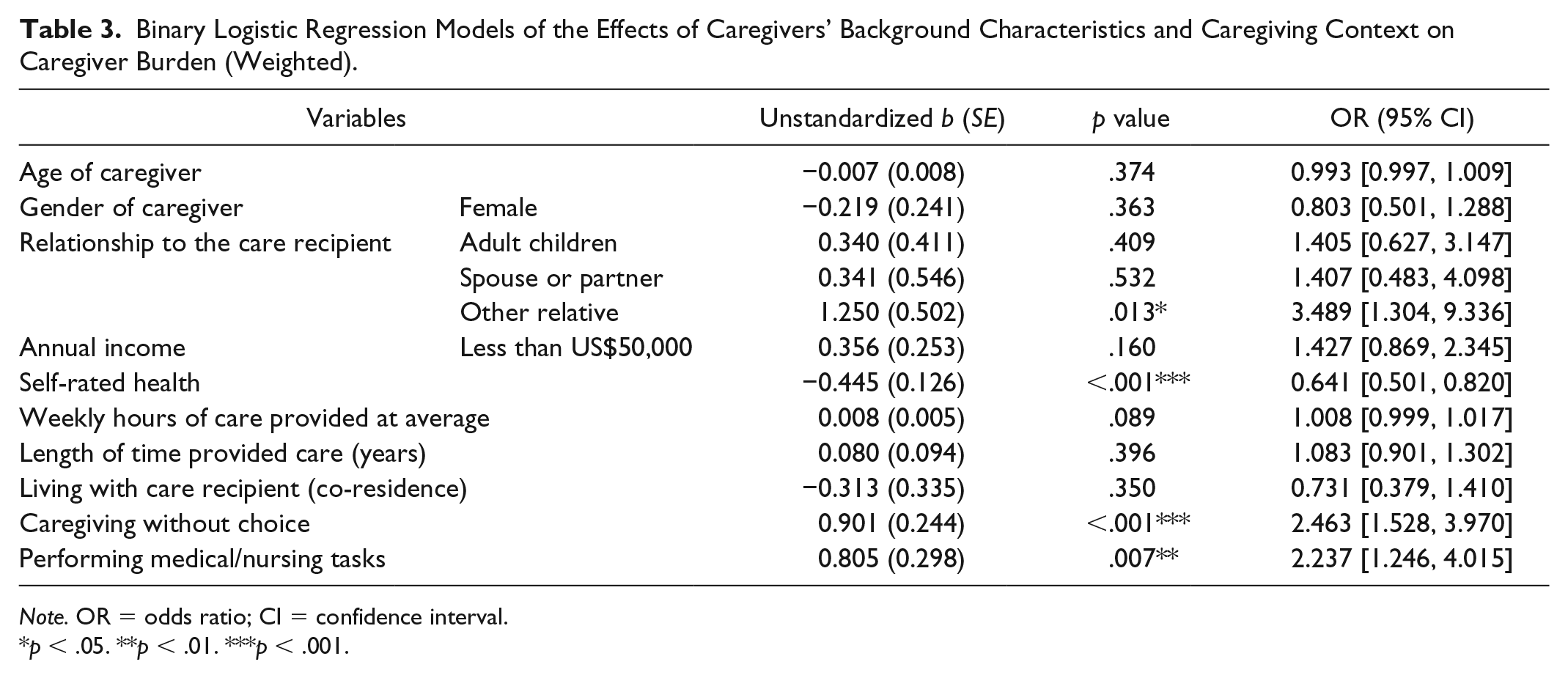
Note. OR = odds ratio; CI = confidence interval.
p < .05. **p < .01. ***p < .001.
Relationships between caregivers and care recipients were identified as a significant factor of being in the higher caregiver burden group. Compared with nonfamily caregivers, when caregivers of ICI took care of other relatives than spouse/partner or parents/grandparents, they were 3.49 times more likely to be in the higher caregiver burden group (OR = 3.489, b = 1.250, p = .013). Self-rated health was a significant factor of caregiver burden. When caregivers reported better self-rated health, they were 35.9% less likely to be in the higher caregiver burden group (OR = 0.641, b = −0.0445, p < .0001). Caregivers’ age, gender, or annual income were not significant factors for predicting the higher caregiver burden group.
Having a choice and performing medical/nursing tasks were significant factors for predicting inclusion in the higher caregiver burden group. When caregivers did not have a choice about caregiving, they were 2.46 times more likely to be in the higher caregiver burden group (OR = 2.463, b = 0.901, p < .0001). Caregivers who performed medical/nursing tasks were 2.24 times more likely to be in the higher caregiver burden group (OR = 2.237, b = 0.805, p = .007). Weekly hours of caregiving, length of care (years), and living with care recipients were not significant factors for predicting the higher caregiver burden group.
The model significantly explained 21.8% (R2 of Nagelkerke) of the variance of being in the higher caregiver burden group. The overall model prediction was 70.0% with 73.7% of specificity and 65.8% of sensitivity.
Discussion
This study provides the first nationally representative results of the effect of medical/nursing tasks on caregiver burden as well as the unique features of backgrounds and caregiving context when caregivers of ICI perform medical/nursing tasks. This study reveals that when the caregivers performed medical/nursing tasks, they were more than 2 times as likely to be in the higher burden group. This finding is in line with previous studies reporting that any type of medical/nursing tasks increased the burden in paid home caregivers (Moorman & MacDonald, 2013), and the number of medical/nursing tasks was associated with heightened physical caregiver stress (Polenick, Leggett, & Kales, 2017). Medical/nursing tasks can be difficult because they involve physical strain (e.g., lifting or moving), technical handling, diagnostic reasoning, hazard from bodily fluids, and possible harm to care recipient (Moorman & MacDonald, 2013; Polenick et al., 2017). Along with those risks and demands, caregivers may have little support in the form of receiving education about the diseases’ condition, resources for the tasks, and skills training for home care responsibilities (Grady & Rosenbaum, 2015).
Caregivers of ICI who perform medical/nursing tasks are usually in close relationships with care recipients who may have greater care needs. This study determined that more caregivers who performed medical/nursing tasks took care of close family members, such as parents/grandparents and spouse/partner (80.2%). In contrast, almost a quarter (23.9%) of caregivers who did not perform medical/nursing tasks, took care of nonfamily members such as friends or neighbors. Close family caregivers may assume the duties, when the medical/nursing tasks are needed and have benefits for care recipients, although the tasks may require considerable responsibility and attention (McDonald, McKinlay, Keeling, & Levack, 2015). Caregivers who are not in a close relationship with care recipients may resist performing medical/nursing tasks because they may be worried about managing the tasks alone or they may be concerned that they will eventually have to conduct more tasks (McDonald et al., 2015).
In this study, caregivers who performed medical/nursing tasks and lived with care recipients provided greater intensity of care (5 times more weekly hours of care) compared with those who did not perform medical/nursing tasks. This finding is in line with a previous study that reported if caregivers of older adults managed medications or had direct interactions with health care professionals for care recipients, the caregivers were more likely to live with older adults and provide more hours of caregiving compared with those who did not (Wolff et al., 2016). Close family caregivers may opt to live with care recipients, and the co-residency often generates greater amounts of time devoted to caregiving (Carretero, Garcés, Ródenas, & Sanjosé, 2009; Chiao, Wu, & Hsiao, 2015). Furthermore, the severity of care recipients’ cognitive impairment may require living together and produce longer hours to meeting daily care needs.
Not having a choice about caregiving may be one of the strongest factors contributing to caregiver burden. Caregivers of ICI may be willing to take the caregiving role when caregivers have a good precaregiving relationship with care recipients, with the choice more likely to be based on affection, closeness, and reciprocity (Quinn, Clare, & Woods, 2010). However, when there is pressure from other family members, from cultural norms (filial piety), or from moral obligation, caregivers may feel no choice about providing caregiving. Lack of choice can be a barrier to having positive motivation and to finding the meaning of caregiving, resulting in feeling strain and powerlessness (Quinn et al., 2010).
In this study, when caregivers of ICI took care of relatives (uncles, aunts) other than a spouse/partner or parents/grandparents, the caregivers were more likely to be in the higher burden group. This result was supported by the current literature that shows when caregivers can predict their caregiving responsibility such as supporting parents or grandparents, they are less likely to be burdened (Kim, Lee, Cheon, Hong, & Chang, 2018). In addition, weak family ties or poor current relationships with care recipients may also put caregivers in the higher burden category (Kim et al., 2018; Richardson, Lee, Berg-Weger, & Grossberg, 2013).
Finally, in this study, caregivers’ better health status (higher self-rated health) lowered the chance of being in the higher caregiver burden group. It is known that poor caregivers’ health is related to greater burden and it is thought that the preexisting physical or psychological health conditions might hinder caregivers from managing stress adequately (Chiao et al., 2015; Roth, Fredman, & Haley, 2015). Half of caregivers have at least one preexisting medical condition and their health is even declining due to the caregiving duties (Grady & Rosenbaum, 2015). Future research is needed to investigate the determinants of poor health among caregivers and interventions to reduce those factors (Grady & Rosenbaum, 2015).
Limitations
This study has several limitations that should be taken into consideration when interpreting the results. First, this study cannot draw causal inference, given that the primary data set was cross sectional, although this data set did provide a rich analysis into caregivers performing medical/nursing tasks. Second, care recipients’ cognitive impairment was based on caregivers’ self-reported response. Although this method is often used in caregiving survey research, the lack of objective diagnosis makes it impossible to specify particular disease type, such as mild cognitive impairment, Alzheimer’s disease, or other types of dementia. Third, this study did not include severity of the care recipients’ disease or medication effects, such as the frequency of disruptive behaviors, the decline of functional status, and the severity of cognitive decline. Therefore, it was difficult to ascertain how the type of memory loss or the severity of care recipients’ disease status specifically influenced the understanding of caregiving burden of performance of medical/nursing tasks. Fourth, this study analyzed only available variables in the primary data set, so all the concepts in Pearlin’s stress process model were not able to be included in the data analysis. Although the primary data set comprehensibly collected various variables related to caregivers, several variables such as family role strain, social role limitation, and relationship strain in the secondary stressors in Pearlin’s model were not collected. Finally, the potential influence of having medical/nursing training to the caregiving role was not clear due to the limited information in the data set. Investigating the specific benefits of receiving training and education for medical/nursing tasks should be further investigated in future studies.
Relevance to Clinical Practice and Policy Makers
Health care professionals may support caregivers of ICI to reduce the burden from performing medical/nursing tasks by providing education and training regarding the tasks. Caregivers are more likely to assume the responsibility willingly when they comprehend the reasons and benefits of medical/nursing tasks (McDonald et al., 2015). While explaining the purpose and benefits of medical/nursing tasks, health care providers may reframe caregivers’ conflicting feelings and negative perceptions related to the tasks (McDonald et al., 2015). Although medical/nursing tasks at home can be stressful and challenging, at the same time, the tasks are critical, and direct help for care recipients is crucial (Polenick et al., 2017). When caregivers successfully manage the medical/nursing tasks through learning skills and obtaining knowledge, the caregivers experience positive caregiving gains, such as becoming closer to care recipients or feeling satisfaction with the care recipients’ care (Polenick et al., 2017). Health care professionals should also receive education regarding the needs of caregivers in medical/nursing tasks as well as the strategies for delivering the instructions and demonstrations efficiently and effectively.
Researchers should consider the importance of medical/nursing tasks in designing future interventions to help caregivers decrease caregiver burden. Specifically, providing medical information as well as skills-based instructions for caregivers to gain confidence in medical/nursing tasks should be integrated into discharge planning or caregiver education. In 2018, a study tested the effectiveness of a web-based educational intervention that provided 50 common medical problems, such as constipation, pain, and dehydration and how to solve the problems (Zimmerman et al., 2018). This study demonstrated that caregivers of ICI could benefit from educational intervention regarding medical/nursing tasks, as the study showed that intervention increased caregivers’ confidence in signs/symptoms management and decreased caregiver strain.
Clearly, rigorous studies, specifically randomized controlled trials with multiple sites, large samples, multiple time points, and subjective as well as objective outcomes (e.g., health care expenditure) are needed for further support of interventions to reduce caregiver burden. Methodologically sound interventions are needed to confirm the benefits of training—not only at the caregivers’ educational level but also at the anticipated level of caregiver burden obtained by initial quantitative assessment. In addition to further study of how to best present immediate care related to medical/nursing tasks to reduce strain, further study of how to effectively provide guidance to the caregiver about what changes to expect in the recipient’s care over various periods of time may help the caregiver better accept the stages of care as well as help reduce the burden of that care if the recipient’s care progresses.
Policy makers should take into account how to assist caregivers further in the delivery of medical/nursing tasks. To date, 39 U.S. states and territories have enacted the Caregiver Advise, Record and Enable Act (CARE Act) that requires the hospital to provide caregivers instructions on medical/nursing tasks at the time of discharge (Reinhard & Ryan, 2017). As a further step, special attention is needed on how to support multicultural caregivers, especially those with language barriers, to better understand discharge information as well as how to assist rural area caregivers in accessing resources for medical/nursing tasks (Reinhard & Ryan, 2017).
Conclusion
This study investigated how caregivers’ background characteristics and caregiving context are different for those performing medical/nursing tasks as well as determined the effects of medical/nursing tasks on caregiver burden among caregivers of ICI. By comparing two groups performing versus not performing medical/nursing tasks, the medical/nursing tasks were frequently delivered by closer kin, requiring co-residential status with their care recipients, and resulting in longer hours of care. In addition, the delivery of medical/nursing tasks put caregivers at twice the risk for caregiver burden.
To address caregiver burden, this study has highlighted the need for health care providers to better understand the vulnerability and extra challenges generated by medical/nursing tasks upon caregivers. When health care providers explain the purpose and the benefits of medical/nursing tasks, the caregivers may be more motivated to take on the extra tasks. Offering step-by-step instructions and hands-on training for the medical/nursing tasks that they need to deliver at home may increase caregivers’ ability, confidence, and feeling of less burden. Further research is warranted to help caregivers within complex and multicultural families to perform medical/nursing tasks for immediate and long-term home care.
Footnotes
Author Contributions
M.L., PhD, MSN, RN, is the primary author and has contributed to the conception, design, and data analysis/interpretation. J.H.R., PhD, has contributed to data analysis/interpretation and writing the manuscript. C.C., PhD, RN, has been involved in the conception, design, and revision of the manuscript. P.J.H., PhD, RN, FAAN, has been involved in the conception, design, and revision of the manuscript. I.C.W., PhD, FGSA, has been involved in the conception, data analysis/interpretation, and revision of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB Approval
Given that the study used publicly available and de-identified data set, IRB approval was exempt.