
Abstract
In car-dependent societies like New Zealand, getting the right balance between mobility and safety could improve outcomes for older people but will require changes to policy and practice. Driving cessation is a major life transition with many impacts, and adult children are frequently involved in both the transition to non-driving and maintaining mobility afterward. This cross-sectional study (N = 675) sought perspectives of family members of drivers aged 65 or older enrolled in a longitudinal study. Most (94%) were adult children, two thirds were women, and 19% were moderately to extremely anxious about their parent’s driving. Loss of independence, driving’s role in identity, and reluctance to rely on family were recognized as important barriers to driving cessation. Most (80%) felt that families, as well as older drivers, would be adversely affected by driving cessation. Families identified accessible local information and services, alternative transport, and community-based programs for drivers and families as assistance most needed.
Introduction
For the majority of older adults in New Zealand and other car-dependent societies, the private car is the main means of transport (Ministry of Transport, 2014; Shen et al., 2017), and the ability to continue to drive is seen as key to maintaining mobility, independence, and quality of life (Ministry of Social Development, 2013). However, options for safe mobility beyond driving are also needed to support engagement in social and community life when driving is no longer an option, and to enable the decision to stop to be made at the right time.
Ceasing to drive and the loss of independent mobility can have serious consequences for older people, including depression (Ragland et al., 2005), poorer physical functioning and performance, general health decline (Edwards et al., 2009), and social isolation (Mezuk & Rebok, 2008). This must be balanced with maintaining a reasonable level of driving safety, for the driver’s well-being and that of others. Although they have relatively few crashes, older drivers have high fatality rates in crashes due to frailty (Ministry of Health, 2013), especially those aged 75 years or older (National Injury Query System, 2014).
The proportion of New Zealanders aged 65 years or above is increasing rapidly and is projected to be one in four by 2036 (Statistics New Zealand, 2011). Road traffic fatalities and injuries in this age group are estimated to increase by 71% in this same period, due to population aging, growth in traffic, and growth in the number of workers over 65 (Frith et al., 2012). Compared with previous generations, older drivers now drive more often and for longer distances, and rely on private car transport to meet virtually all transport needs (Ministry of Transport, 2015).
Driving cessation can follow a period of consideration or happen suddenly in response to an incident, but it represents both a substantial change in behavior and a life transition (Liddle et al., 2008). To maintain and improve the well-being of the aging population, we need to better understand the process of transitioning to non-driving, how to ameliorate the impacts on drivers, and how to maintain safe mobility.
The process and consequences of driving cessation are not usually experienced by older drivers alone, but in the context of their families. Adult children may be the first to notice safety issues but can find it difficult to contribute effectively to their parents’ transition (Adler, 2010; Liddle et al., 2008). They may need to intervene if their parent continues to drive when they consider it to be unsafe (Kouabenan, 1998), but may also be unduly protective of their parents, over-estimating the dangers and under-estimating the benefits of continuing to drive. The dynamics of communication with parents in these circumstances are unfamiliar and can be difficult to manage (Liddle et al., 2013). Regardless of how driving cessation has come about, adult children usually provide increased practical and emotional support.
Little is known about the nature of involvement of adult children in decisions about their parents’ driving in New Zealand (New Zealand Transport Agency, 2018) and how best to support families with the process. Internationally, there is a body of qualitative research involving family members of drivers with dementia, which provides some insights, but this context has its own unique issues (Lloyd et al., 2001). There are few studies of the more common situation where adult children get involved in decisions about a parent’s driving as they age, and then assume new responsibilities as a consequence of their parent’s driving cessation.
Research exploring adult children’s perspectives on the meaning of driving in older people’s lives, and their own roles in driving reduction or cessation, have so far used qualitative methods, and have found some consistent themes, particularly about difficulties the adult children face. In the southern United States, Ralston et al. (2001) interviewed eight drivers (aged 70–90 years) who were well and had recently stopped driving, eight younger generation family members, and one brother. Four of the older drivers had decided to stop themselves, three were encouraged by their family, and one stopped on doctor’s advice. All felt negative impacts of inability to drive (loss of freedom, independence, role, and occupation), and all felt a burden to their family. Family’s perceptions of the process focused on the complexity of the decision (the reasons, the decision makers, the older driver’s feelings), their additional obligations, the “reversal” in roles experienced when guiding the process, and some minimizing the importance of driving. Only one family depicted congruent perspectives between the driver and the family member. The older drivers’ reactions ranged from indifference to devastation, and the family perceptions of the effect on the driver ranged from no impact to life-altering change.
Sterns et al. (2001) conducted a series of focus groups with family members in the Midwest of the United States, with a view to increasing their capacity to identify, and intervene with, “at-risk older drivers” to improve road safety. They identified barriers to involvement by family similar to those seen by Ralston—conflicts over perceived role reversal where the adult child now gives the guidance, feelings of guilt or disrespect about intervening, and perceived inability to meet the need for assistance with transport post-cessation.
In Queensland, Australia, Liddle et al. (2008) interviewed nine voluntarily retired drivers aged 73 to 88 years, three family members and six service providers, to gain understanding of the cessation process to assist with adjustment. They identified three phases of adjustment as pre-decision, decision, and post-cessation, each with its own challenges. In the pre-decision phase, family members often reported earlier awareness of difficulties than the drivers. In the decision phase, drivers largely heard the concerns of family and friends as useful, and discussed their decision with family. Post-cessation, family members were dealing with the new level of dependency, sometimes trying to conceal the extent of the burden on them from the ex-driver.
Focus group interviews of family members were also undertaken as part of a broader study of driving reduction and cessation in Michigan (USA; Kostyniuk & Shope, 2000). Kostyniuk et al. (2009) and Connell et al. (2012) reported findings from 30 adult children and seven grandchildren with concerns about the driving of 38 current older drivers and 14 former drivers. Themes represented three aspects of the families’ perspectives: communication and dynamics, taking action to stop parent’s driving, and post-cessation reflection. Issues of family dynamics included discussion and planning, avoidance and passivity, resignation, burden and reciprocity, and role reversal. Actions to cease the parent’s driving included appeals to a third party, for example, doctor, and taking away access to the car. Following driving cessation, adult children reflected on their relief, and some social benefits from increased interaction, but also ongoing resentment, depression, and anger among some parents, triggering feelings of guilt.
Research to date has found consistent differences, but also overlaps, in the perceptions of older drivers and their families, and barriers to cooperative planning for driving cessation. To understand how adult children do, or could, effectively assist their parents’ transition toward non-driving, we need to know more about their views and experiences, where most difficulties arise, and how commonly problems occur. To improve outcomes for older people, we will also need to identify what help families need and how this might be provided at both a population level and an individual level.
In this research, we developed an interviewer-administered questionnaire for adult children of older drivers, guided by previous studies of older drivers themselves, and the existing qualitative investigations with family members. Our aims were to
describe the views, concerns, and experiences of adult children who have an aging parent driver, and what assistance would be useful in the transition to not driving.
compare views of older drivers and their adult children on the importance and safety of continued driving.
This study was nested in a large mixed-methods study of older drivers, families, and general practitioners in New Zealand, aiming to inform policy and practice about driving cessation, which balances mobility and safety needs and maximizes the well-being of aging drivers and non-drivers. In New Zealand, drivers must be relicensed at age 75, 80, and then every 2 years. This requires a medical certificate from a family doctor who will check general health and eyesight, and who may request an on-road test as a condition of licensure (New Zealand Transport Agency, 2018).
Method
Study Design
We conducted a cross-sectional study of adult children of community-dwelling older drivers who were participating in longitudinal research on self-regulation and cessation of driving (New Zealand Prospective Older Adult Transport and Health Study [NZPATHS]). The NZPATHS participants were a stratified random sample of people 65 years and older on the New Zealand electoral roll, with oversampling of Māori (indigenous population of New Zealand) and drivers ≥75 years old.
Participants
Current drivers in NZPATHS were asked at the end of their interview whether they had a son, daughter, or other member of their immediate family, whom they were willing for us to contact about participating in the Family Study. To be eligible, they needed to be a younger generation close relative (e.g., adult child) currently living in New Zealand.
Data Collection
Recruitment and questionnaire administration were completed using a computer-assisted telephone interview system. Family Study data were collected and managed using Research Electronic Data Capture (REDCap) tools hosted at the University of Otago (Harris et al., 2009), in December 2016 to May 2017. The majority of items were closed questions. All open-ended questions were coded for common themes within the responses and checked by a second coder. Methods were very similar to the interviews of the older drivers, conducted in July 2016 to April 2017. The older driver and their family member were allocated different interviewers.
Measures
Demographic data were self-reported. Ethnicity data collected using the 2013 NZ Census question were prioritized to assign a single ethnic group (Ministry of Health, 2008).
Family members’ views on their parent’s driving were largely elicited using questions with response scales of 1 to 5 or 1 to 7. Items about driving importance, ability, and safety were adapted from previous research with older drivers (Li et al., 2017; Molnar et al., 2014). Items on challenging driving tasks were derived from Croston et al. (2009) and used a 3-point scale (not at all, somewhat, very challenging). Anxiety about the parent’s driving was measured on an 11-point scale used previously to measure driving anxiety, categorized as none (0), mild (1–4), and moderate to extreme (5–10) (Taylor et al., 2007).
Family members’ views on driving cessation used items adapted from older drivers’ questions about contemplation of cessation (not at all, little, some, a lot; Charlton et al., 2006) and the likely barriers to cessation (Croston et al., 2009).
Older drivers had themselves answered some questions on their driving and views on cessation worded and scored in an equivalent way that have been used for comparison.
At the end of their interview, we asked, “What assistance or help would be useful for you if you were helping a family member who was having difficulty with their driving or having to adapt to no longer being able to drive?” Responses were coded for common themes.
Analysis
We used numbers and proportions to characterize the participants and their views on their parent’s driving. Proportions were unweighted, and no statistical testing was used, as the Family Study participants were not a probabilistic sample representing a defined population. Prevalence of family members’ views on parent’s driving and driving cessation was stratified by age of the older driver (<75 years, 75+ years).
When comparing the participants of NZPATHS with and without representatives in the Family Study, weighted proportions were used to account for the stratified sampling design in NZPATHS.
Differences in the older drivers’ and family members’ views of the current situation with respect to driving were assessed using responses of older driver–family member pairs to seven questions that were common to both questionnnaires. To enable this, raw scores on the seven questions were scaled to a common metric of 1 to 7 points, and differences were calculated for each pair on each question, ranging from 0 to 6 points. Mean differences were calculated for (a) each question across all pairs and (b) each pair over the set of seven questions. Ordinary least squares regression estimated the association of the difference in scores over the seven common questions with (a) the gender of the family member, (b) the proximity of residence, and (c) the age group of the older driver, with adjustment for the other two factors.
Results
There were 1,181 drivers above 65 years of age participating in NZPATHS. Of these, 200 did not have a family member eligible for the Family Study, that is, there were no younger family members or they lived overseas. Of the remainder, 731 nominated a family member from the next generation to take part and 250 declined to have their family involved. There were 56 nominated who did not participate (47 declined, one was ineligible, and eight not contactable) resulting in 675 NZPATHS members with a corresponding family member who was interviewed (57.2% of the older driver sample). A flowchart of participant recruitment is presented as Supplemental Material, which can be accessed online through the Journal of Applied Gerontology.
Demographic characteristics and self-rated health of older drivers with participating family members were very similar to those without, apart from being a little more likely to be currently partnered. Drivers represented in the Family Study were also more likely to report that their driving may become a problem within 5 years, but no more likely to have thought about stopping or planned for it (Table 1).
Characteristics of NZPATHS Participants With and Without Family Members Participating in the Family Study.
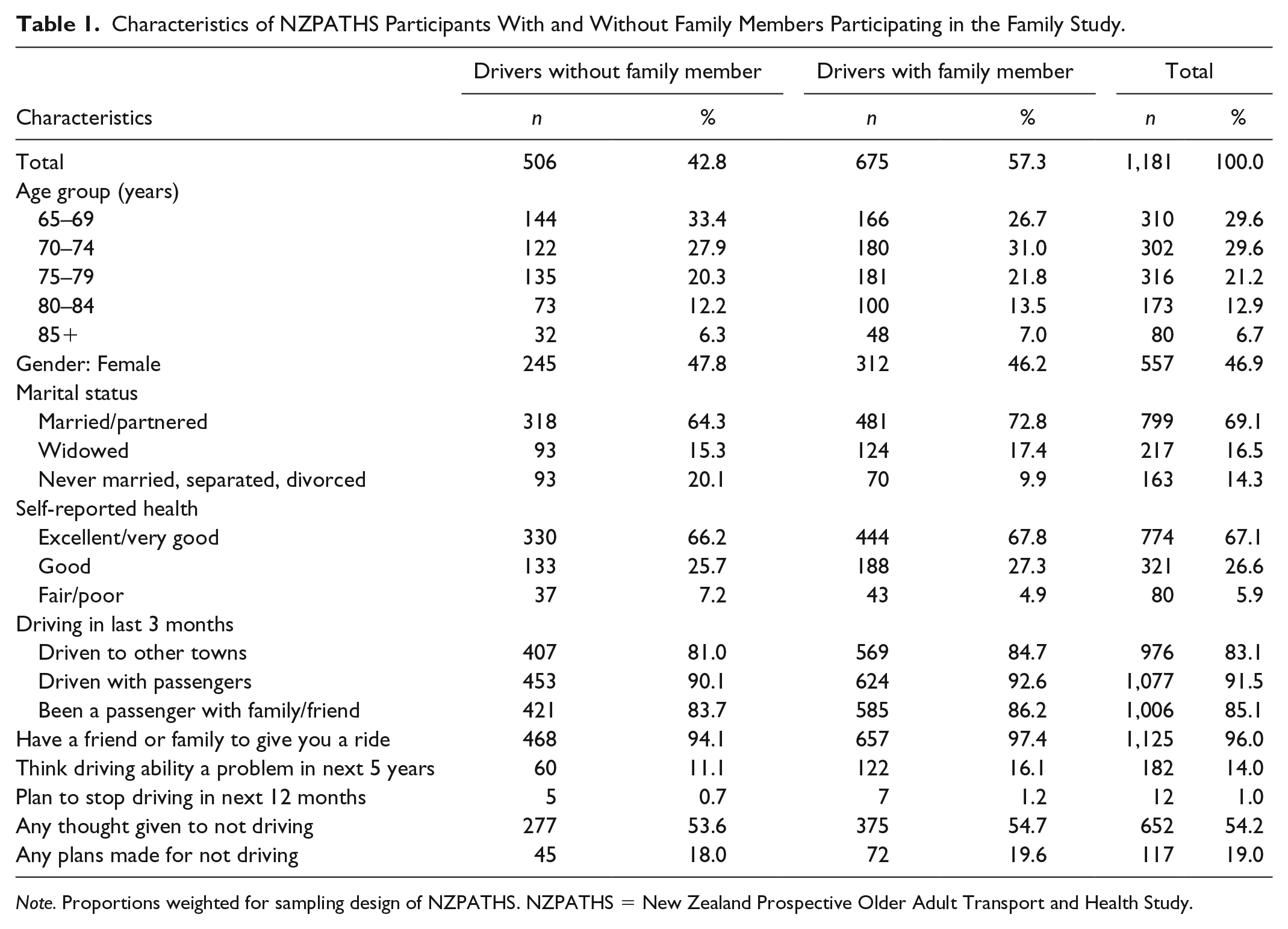
Note. Proportions weighted for sampling design of NZPATHS. NZPATHS = New Zealand Prospective Older Adult Transport and Health Study.
Most participants were sons and daughters of the older drivers (93.6%), and while only 8% lived in the same household, 58.3% lived in the same town or city (see Table 2). More than three quarters of the participants were aged 40 to 59 years, nearly two thirds were women, and most were in paid work at the time of the interview. Only 12% said they never traveled as a passenger with their older driver, but another 73% reported being a passenger infrequently (once a month or less; Table 2).
Characteristics of Family Members.
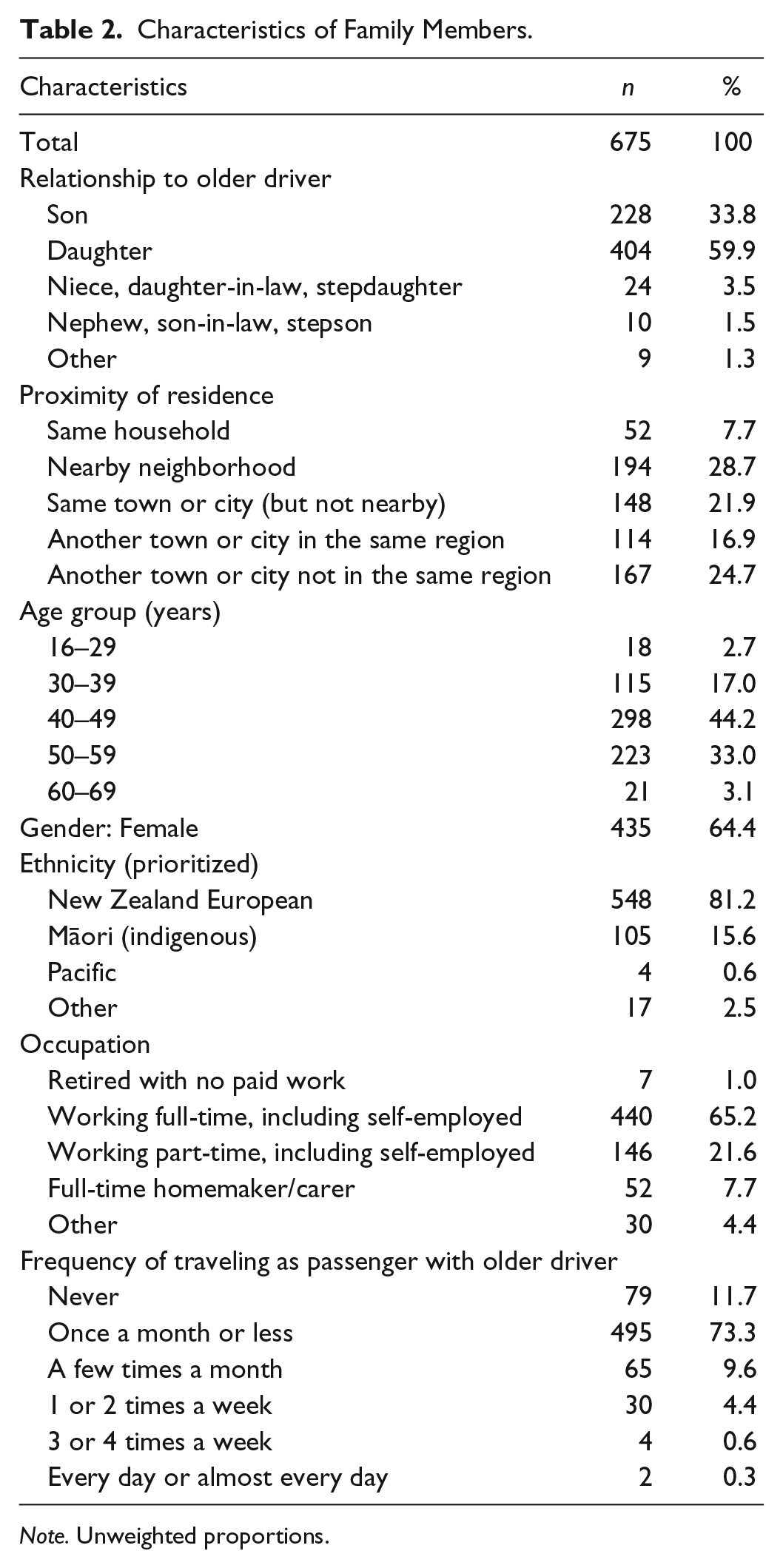
Note. Unweighted proportions.
Views About Parent’s Driving
Table 3 contrasts participants’ views about drivers, 65 to 74 years of age with those 75 years or older. Overall, 40% thought that driving ability could become a problem within 5 years, but only 12% anticipated problems within a year. Prevalence was higher when the driver was ≥75 years. Concern about being a passenger, and allowing children to be passengers, was also higher with the older group, and moderate-to-extreme levels of anxiety about the parent’s driving were twice as common. Nevertheless, three quarters of adult children of drivers ≥75 years still reported no more than mild anxiety about their driving.
Family Member Views and Concerns About Parent’s Driving, by Driver Age Group.
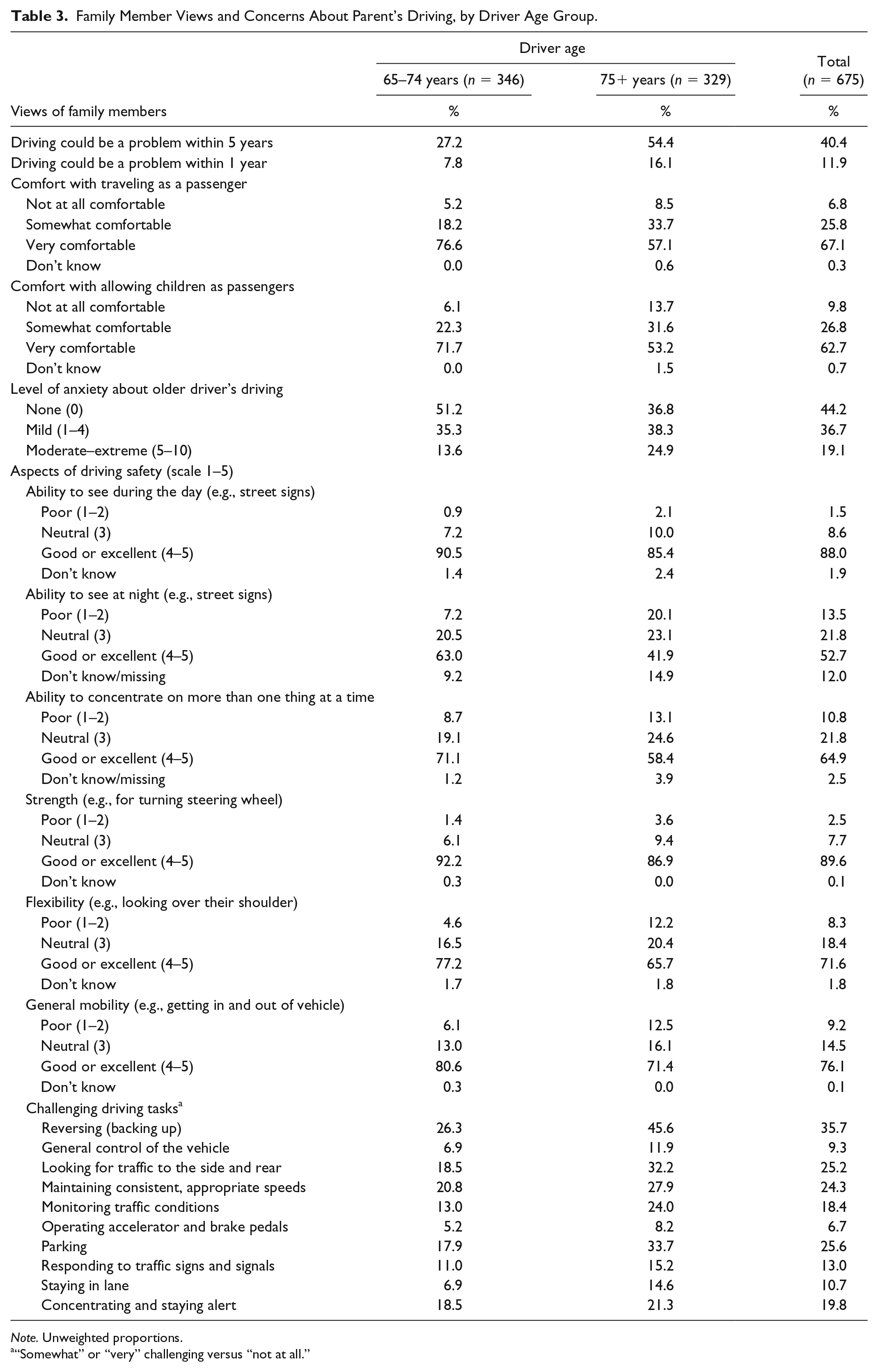
Note. Unweighted proportions.
“Somewhat” or “very” challenging versus “not at all.”
The aspects of their parent’s driving safety most often scored as poor were ability to see at night (14%) and ability to concentrate on more than one thing at a time (11%). All safety concerns were more common for the older group of drivers.
Reversing (backing up) was the driving task most commonly reported as challenging for older drivers (36%; see Table 3). Looking for traffic to the side or rear, maintaining an appropriate speed, and parking were also reported as somewhat or very challenging by a quarter of participants. Nearly half of drivers, ≥75 years, were thought to be challenged by reversing the car.
Open-ended questions were asked about participants’ main concerns about their parent’s driving and concerns of others. Almost half (48%) reported no concerns, and the only issue that was mentioned by more than 10% of family members was poor driving awareness or ability to judge the situation (14%). Other issues mentioned by more than 5% of participants were: lack of concentration/easily distracted (9%), lack of confidence/anxiety (8%), mobility/health issues including fatigue (7%), and aggressive or over-confident driving (5%). One in five reported that other family members (partners, siblings, children, or “everyone”) had concerns that were similar to their own.
Views About the Prospect of Driving Cessation
A third of participants reported that their older driver had not given any thought at all to the prospect of not driving one day (Table 4). However, about 10% of older drivers were thought to have given cessation a lot of thought, and the same proportion had made plans for cessation (n = 68). These plans included moving house to be closer to public transport (n = 23); becoming familiar with public transport (n = 32); exploring transport alternatives (n = 38); exploring use of mobility scooter (n = 19); moving nearer family, friends, and health services (n = 35); and sharing the driving (n = 28).
Family Members’ Views About Driving Cessation, by Driver Age Group.
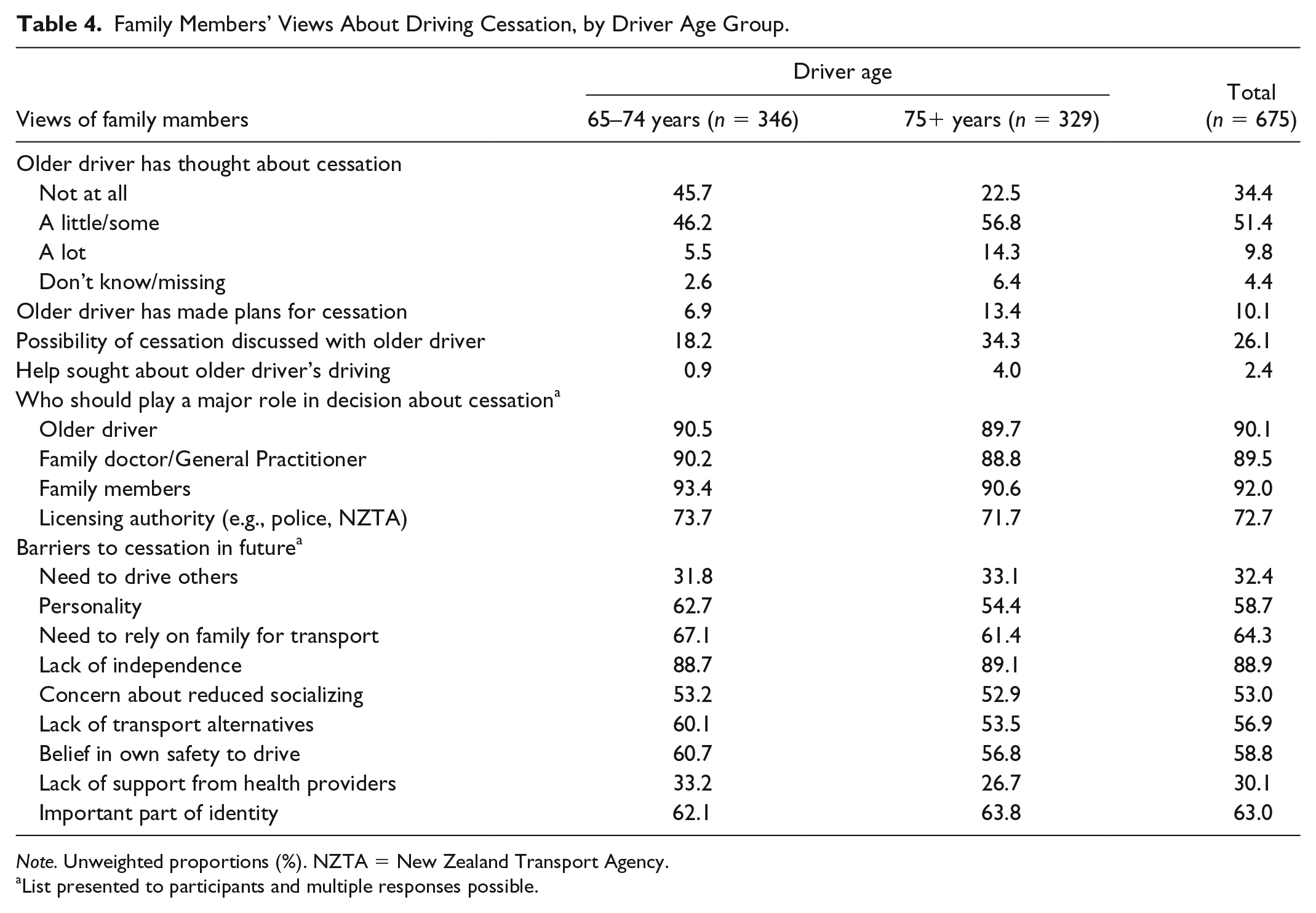
Note. Unweighted proportions (%). NZTA = New Zealand Transport Agency.
List presented to participants and multiple responses possible.
A minority of family members (26%) had discussed driving, or the possibility of giving up some day, with the older driver, and 80% of them felt alright about this. The others had found it difficult or frustrating, or that the older driver was avoiding the topic. Most felt that these discussions had no impact on their relationship, but 15% felt it had a negative impact, and a few felt it was positive. For participants yet to have such a discussion, 69% thought that when the need arose it would be OK/comfortable, and 23% thought it would be uncomfortable/difficult. While 80% felt it would not affect their relationship, 16% felt it could have a negative impact.
Views on potential barriers to driving cessation are summarized in Table 4. The meaning of driving to their parent was strongly endorsed as a reason for them not wanting to give up, reflected in loss of independence, not wanting to rely on others, part of their identity, and enabling of social connections.
In open-ended questions about the drawbacks and benefits if the older driver could no longer drive, family members saw the main drawbacks for the ex-driver as loss of independence/freedom (53%); limits on socialization (35%); negative impact on state of mind/self-worth (13%); inability to shop, run errands, and attend appointments (12%); and limits on work and volunteering (9%). Only 3% reported no drawbacks. Most felt the family would also be negatively affected (80%), with main concerns being more time providing transport and organizing things (40%), concern about the loss of well-being of the ex-driver (11%), reduction in family contact (8%), and dealing with the ex-drivers’ unhappiness (6%).
Half of the participants felt there would be no benefits for the older driver of stopping driving, while 16% anticipated a safety benefit and 10% mentioned a cost saving. Other benefits mentioned by 3% to 5% of family members were less stress about driving, more time to spend with family/friends, more walking, and more time to relax.
About half saw no benefits for the family, but 37% thought it would be less worry, and 6% thought that more involvement with the ex-driver would be a benefit.
How Did the Views of Older Drivers and Families Differ?
Figure 1 shows that, generally, the responses of adult children were less positive than their parents’ assessments, when asked the same question.
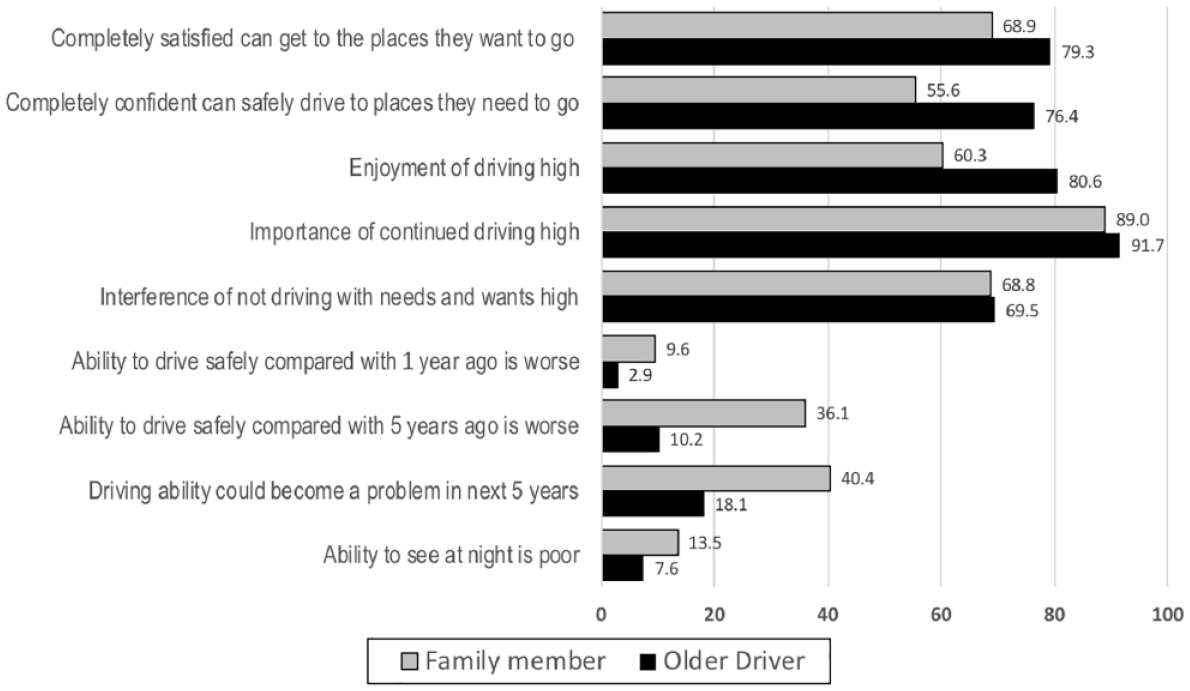
Responses of older drivers and their family members to the same questions about the older driver’s driving.
The differences in actual scores given by the older drivers and their family members to the first seven of these questions (i.e., broad assessment of the current situation) were calculated to determine where responses were most different across all pairs of participants. In order from greatest to least, the mean differences in scores (from 0 to 6) were “Interference of not driving with needs and wants” (1.13; 95% confidence interval [CI] = [1.03, 1.23]), “Enjoyment of driving” (1.04; 95% CI = [0.96, 1.12]), “Confidence in driving safely to where they need to go” (0.81; 95% CI = [0.73, 0.89]), “Ability to drive safely compared with 5 years ago” (0.74; 95% CI = [0.67, 0.81]), “Satisfaction they can get where they need to go” (0.59; 95% CI = [0.51, 0.66]), “Importance of continued driving” (0.57; 95% CI = [0.49, 0.64]), and “Ability to drive safely compared with a year ago” (0.26; 95% CI = [0.21, 0.31]).
We also considered whether discrepancies varied systematically with the gender of the family member, the distance apart they lived, or the age group of the driver. The analysis reported in Table 5 suggests concordance was greatest when the family member was a woman, or lived further away, and less when the older driver was ≥75 years, but differences were not substantial.
Association of Difference in Scores Between Older Driver–Family Member Pairs With Gender of Family Member, Age of Driver, and Proximity of Residence.
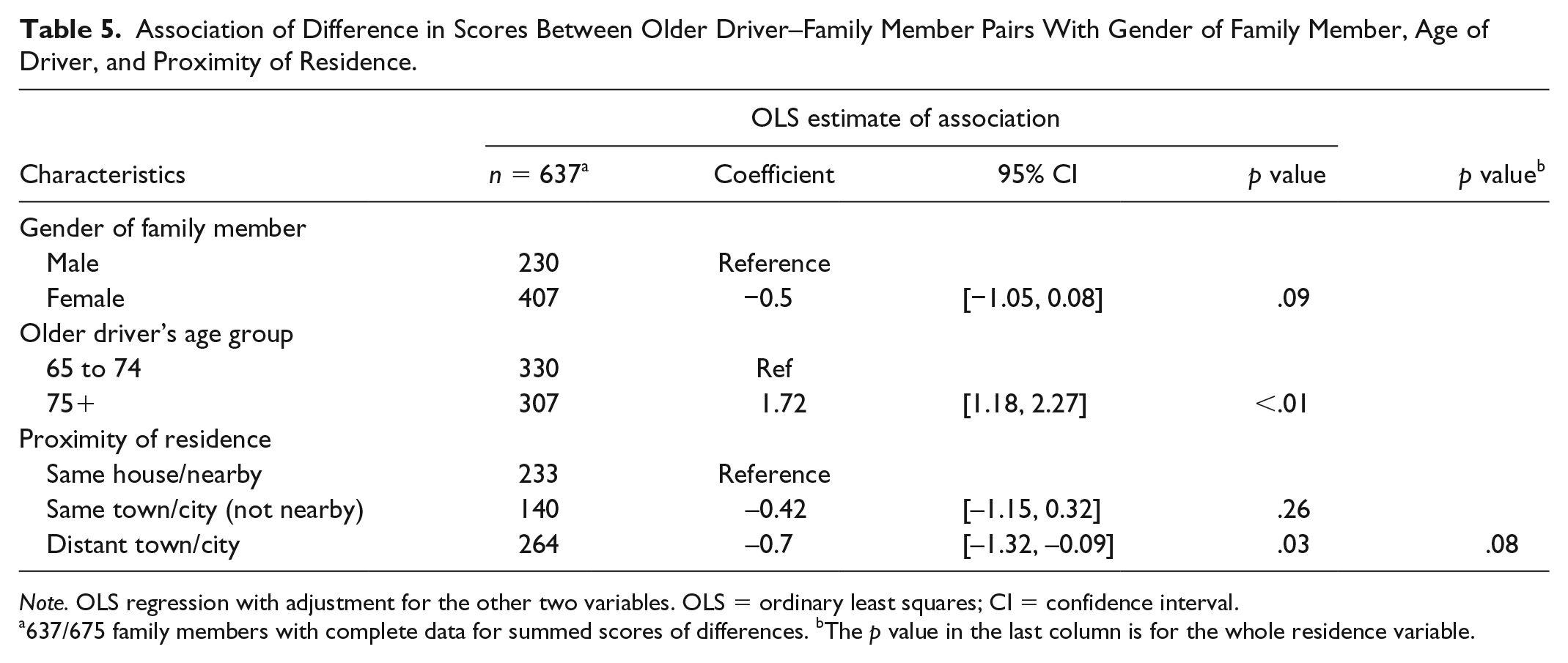
Note. OLS regression with adjustment for the other two variables. OLS = ordinary least squares; CI = confidence interval.
637/675 family members with complete data for summed scores of differences. bThe p value in the last column is for the whole residence variable.
Views About Assistance Needed
Only 2.4% (n = 16) of the participants had sought help about their parent’s driving (Table 4). They were largely the children of drivers ≥75 years, and they had asked family members, doctors, or driving instructors for assistance. Most received support and discussion, while three had organized a health or driving assessment, and one received help with transport.
At the end of the interview, all participants were asked what assistance they thought would be useful, and their responses are represented in Figure 2. Most participants contributed to only one of these themes but 172/675 participants contributed to two.

Types of assistance considered helpful by family members of older drivers when managing driving difficulties or cessation.
Suggestions addressed three broad aspects: better local community-based services and amenities and provision of alternative transport, external assistance with making decisions about safety or cessation, and support services for both older drivers and their families in the transition and afterward.
Discussion
In this study, we have extended the previous qualitative work on the involvement of family members in driving cessation, with quantitative research conducted in a general population setting. This provides novel insights into the nature and frequency of issues arising in families during this major transition, and will inform practice and policy to support healthy aging.
Our participants were largely middle-aged employed people, and two thirds of them were women. This busy time in people’s lives is sometimes referred to as the “sandwich generation,” providing care for both children and older adult parents while working (Hawke et al., 2014). Although nearly 60% lived in the same town, 85% of the adult children rode with the older driver infrequently and so had little firsthand experience of their driving. Concern they expressed about their parent’s driving was clearly higher when the driver was 75 years or older, the age where regular relicensing begins, overseen by a family doctor. The commonest concerns about driving ability are related to aspects of behavior noticeable in a non-driving environment, such as reduced ability to multitask, less acute awareness and judgment, and poorer night vision. For most families, anxiety over driving was quite low, with only one in five more than mildly anxious about the current situation.
In anticipation of driving cessation, a third of family members of drivers aged 75 or older had discussed this prospect with them, but less than 15% reported that the older driver had thought a lot about it and had made any plans for managing the change. This suggests that opportunities for discussion are being missed or avoided by families, since the change in status of licensing for these drivers means it has already been brought to the older driver’s attention in their fitness-to-drive assessment.
Family members may have good reason to be hesitant about introducing a discussion with an aging parent about driving. Previous studies have found that it can be upsetting and uncomfortable for both parties (Liddle et al., 2013; Stern et al., 2008) and in a minority of cases may continue over a long period, straining relationships. Hesitancy about starting a discussion means that even when children have problematic driving, they may initially keep the discussion to themselves rather than approach the parent to start a dialogue (Connell et al., 2012). Sometimes adult children come to feel that talking with the older driver is pointless when the parent ignores or discounts their advice and may withdraw from attempting to help (Connell et al., 2012). In our study, 17% of those who had engaged in discussion found it difficult or frustrating, and most of that small group felt it harmed their relationship. The work of Liddle et al. (2008) in Australia suggests that timing of the discussion is important and that family members’ views on driving ability are easier to assimilate once the driver has accepted the need for planning. The Michigan study (Kostyniuk et al., 2009) found that both older drivers and adult children were often reluctant to openly discuss declining driving ability. Even when concerned about safety, family members hesitated to discuss their parents’ driving. The “parents’ resistance to interference from others and unwillingness to relinquish driving or become more dependent” were seen to reinforce this reluctance. After cessation, some drivers did not seem to get beyond their negative feelings about having to stop driving, and continued to blame the family for their loss.
In our interviews, driving cessation was often seen as raising important and difficult issues for both the driver and the family, and not balanced by substantial benefits for either party. For families, the biggest issue was providing and organizing transport. Less concern about the parent’s driving was likely to be replaced by concern about the parent’s loss of autonomy and how they would deal with that.
Having different views of the safety of the older driver continuing to drive is a potential source of discomfort and conflict. When we compared parents and children, children’s responses were less positive than their parents’ about driving ability, but there was a similar level of acknowledgment of the importance of driving, and how cessation would interfere with the driver’s needs and wants. With little direct experience of their parent’s driving, participant’s concerns were largely extrapolated from observations in a non-driving environment. It is likely that when families start noticing changes in their parent’s abilities and it brings the parent’s aging to attention, they may over-estimate the effect on driving. On the contrary, more positive scores from older drivers may also reflect a lack of awareness or acceptance of age-related decline. The extent to which views differ could plausibly relate to characteristics of the parent–child relationship, the parent’s age, and how much contact the pair usually had. In our sample, women’s views were more concordant with their parents’ than men’s, and differences were greater with the oldest drivers. Surprisingly, we also found that living further apart was related to more concordance. It is possible that these adult children are more dependent on their parent’s view as their source of information.
When participants were asked what would help with managing driving difficulties or cessation, the most common responses were population-based and structural: accessible community-based information and services, and alternative affordable transport. Given that this life transition confronts the majority of families eventually, the absence of community amenities is notable. Suggestions also touched on the way decisions about cessation are made, suggesting it could be taken out of the families’ hands, and decided by clear guidelines, objective feedback on driving, an external authority, or some kind of definitive medical or driving assessment. It was also noted by Sterns et al. (2001) that family members expected support from both legal and medical authorities but found it largely lacking. Finally, support to aid the emotional and practical transition was suggested, in the form of counseling or support groups for drivers, and support services for families. This is consistent with previous research, where families expressed their lack of preparedness for the situation they were in and were often unsure about who to go to for advice. Sometimes advice was confusing and conflicting (Connell et al., 2012; Liddle et al., 2013). Older drivers without any family support, who were not included in our study, are likely to be even more in need of such services.
Following on from qualitative studies that identified a range of relevant issues, this larger study has been able to estimate how common these issues are. Participants were nominated by a population sample of older drivers and reflect considerable diversity, although not completely representative of the population. Older drivers with and without family members included in the study had similar demographic characteristics, health and driving status, but it seems unlikely that they had similar levels of social support, and so this sample is likely to overrepresent families with closer ties. In addition, unless they have had experience with another aging relative, most participants are commenting on a scenario that is still hypothetical.
In this sample, our participants can see issues about the parents’ driving on the horizon but little planning was going on. There is an expressed need for clearer advice and assistance with the transition to not driving and meeting their parent’s future mobility needs.
In the face of concern about decreased driving ability and uncertainty about how to proceed, family members in previous studies of older drivers have employed a range of tactics, including emphasizing the risks from continuing, such as crashing or being fined for infringements (Liddle et al., 2013). Some have helped to monitor their parent’s driving and reduce the range of driving undertaken (Adler, 2010). Others attempted to limit driving without discussing it with the driver, by refusing to be a passenger, reducing the need or opportunities for driving, or by taking away access to the car altogether (Adler, 2010; Connell et al., 2012). However, it is unclear how effective family intervention is, and the decision to stop or continue driving may also be influenced by peers, by the availability of other transport options, and by the need to drive others (Dickerson et al., 2019).
There are gaps in service provision that could make a difference to concerned families and the outcomes for their parents, from population to individual level. At a structural level, moving away from such heavy reliance on personal car transport and putting more emphasis on walkability and public transport will make this transition easier in the future. However, current older drivers in car-dependent countries are largely unfamiliar with any transport alternatives and this makes adaption difficult. Public transport can be made more attractive to older people, but it needs to be available, accessible, acceptable, affordable, and adaptable (Kerschner & Harris, 2007), and volunteer driving services could also fill in gaps if well-organized (Dickerson et al., 2019). Family members are asking for identifiable community-level services that can provide reliable advice and support. Information and guidance that is consistent between drivers, families, and family doctors could reduce confusion about balancing mobility and safety, and position driving cessation as a normal but challenging transition. Development of programs to successfully facilitate the transition and reduce adverse impacts (Dickerson et al., 2019) will need to include families.
What this sample can tell us is limited until they come to the point where their parents are facing driving cessation. For this reason, we intend to follow up these pairs of older drivers and family members through the next few years, as part of the NZPATHS longitudinal study, to identify modifiable factors that contribute to better experiences and outcomes, and clarify the nature of assistance required to achieve this.
Supplemental Material
Supplementary_figure – Supplemental material for Older Drivers and Their Future Mobility: Views and Involvement of Their Adult Children
Supplemental material, Supplementary_figure for Older Drivers and Their Future Mobility: Views and Involvement of Their Adult Children by Jennie Connor, Rebecca Brookland and Ari Samaranayaka in Journal of Applied Gerontology
Footnotes
Acknowledgements
We would like to acknowledge the Health Research Council of New Zealand for funding this work, and the Longitudinal Research on Aging Drivers (LongROAD) project sponsored by the AAA Foundation for Traffic Safety (Washington, D.C.), for items used or adapted from their questionnaires. Brandon de Graaf and Dave Barson provided data management support, and Sarah Beaumont managed the data collection. We also thank the team of interviewers and the participants for their contribution to the study.
Author Contributions
Rebecca Brookland is the principal investigator of the NZPATHS project and is responsible for the data collection, Ari Samaranayaka conducted the analysis, and Jennie Connor wrote the first draft of the paper. All authors contributed to the design of the study and the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The research was approved by the University of Otago Human Ethics Committee (Health) Ref H15/080. Prior to telephone contact, a copy of the consent form was sent to potential participants outlining the study, their rights as a participant, and that informed oral consent would be obtained prior to their interview.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Health Research Council of New Zealand [HRC15/261; 2015-2018].
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.