
Abstract
Skilled nursing facilities (SNFs) have received regulatory attention in relation to their emergency preparedness. Yet, assisted living settings (ALs) have not experienced such interest due to their classification as a state-regulated, home- and community-based service. However, the growth in the number of ALs and increased resident acuity levels suggest that existing disaster preparedness policies, and therefore, plans, lag behind those of SNFs. We examined differences in emergency preparedness policies between Ohio’s SNFs and ALs. Data were drawn from the 2015 wave of the Ohio Biennial Survey of Long-Term Care Facilities. Across setting types, most aspects of preparedness were similar, such as written plans, specifications for evacuation, emergency drills, communication procedures, and preparations for expected hazards. Despite these similarities, we found SNFs were more prepared than large ALs in some key areas, most notably being more likely to have a backup generator and 7 days of pharmacy stocks and generator fuel.
Introduction
The aftermath of the Hurricanes Katrina and Rita first brought attention to the importance of emergency preparedness of skilled nursing facilities (SNFs); 103 residents died what were deemed avoidable deaths due to poor planning and response efforts (Dobalian et al., 2010). Although most SNFs have emergency plans, inadequate plans remain an area of federal concern. Two reports from the Office of the Inspector General (OIG) documented gaps in preparedness among SNFs including such areas as maintaining contracts with a transportation provider and having plans to maintain certain staffing levels during an emergency (Levinson, 2012). In response, a federal rule was put into effect in 2015 and expanded in 2017 by the Centers for Medicare & Medicaid Services (CMS) that detailed specific requirements of emergency plans that SNFs must follow regarding the transportation of residents during evacuations, emergency supplies, specific staffing levels, and shelter-in-place procedures among other components (CMS, 2016a, 2016b, 2017b).
However, limited literature has examined the preparedness of assisted living settings (ALs), a growing and critical component of the long-term services and support (LTSS) system. In Ohio, the licensing category of residential care facilities (RCF) is synonymous with “assisted living” (that includes what other states may refer to as board and care homes, personal care homes, etc.; Berish et al., 2018). ALs provide housing and personal care with unique operational philosophies highlighting independence, autonomy, choice, and dignity (Walters, 2012), but they do not provide the same 24-hr skilled nursing care as SNFs (Caffrey et al., 2012; Walters, 2012). A retrospective survey of 217 SNFs and ALs that experienced Hurricanes Katrina and Rita found that all settings reported problems related to evacuation (Castro et al., 2008). During Hurricane Harvey in Texas, it was reported that residents in ALs were neglected, abandoned, or did not receive timely medical care (AARP Texas, 2018). In response to tragedy or constituent concerns, Florida and Oklahoma have proposed or passed legislation requiring ALs to have backup generators to protect and ensure the comfort of residents, often individuals above the age of 80 years (Carter, 2012; Fink & Stevens, 2017). Given that neither ALs nor SNFs are on priority lists for emergency agencies, generators are critical; state policy would need to drive change among ALs (Carter, 2012). Due to a lack of federal oversight, the plans of ALs may lag behind those of SNFs.
Changes in the AL Population
Over the last two decades in the United States, a marked increase in the growth of ALs as a home- and community-based services (HCBSs) alternative to SNFs has occurred (Caffrey et al., 2012; Caffrey & Sengupta, 2018). In Ohio, there were 265 ALs in 1995; in 2015, there were 655 (Mehdizadeh et al., 2017). Currently, there are more than 720 ALs in Ohio (Ohio Department of Health [ODH], 2018c). The utilization of assisted living is only expected to increase as a result of population aging, pressure on state agencies to expand HCBS options, and the preference of many older adults to age within the community (Johnson & Appold, 2017). Nationwide, the AL Medicaid Waiver programs have also grown over the last decade (Hahn et al., 2011); these waivers allow residents who are nursing home eligible to receive Medicaid in ALs, making emergency preparedness a federal concern. The trend also suggests that older adults with physical and cognitive limitations are increasingly residing in settings known to be more home-like and community-based.
Furthermore, AL residents are more disabled than in the past (Lerner et al., 2017). In Ohio, 43% of all AL residents on any given day have two or more functional limitations, representing an increase from 17% in 2009 (Mehdizadeh et al., 2017). Approximately 29% of residents have cognitive impairments, a 17-percentage point increase from 2009 (Mehdizadeh et al., 2017). National statistics on the burden of impairment in ALs parallel what has been documented in Ohio. Approximately 40% of residents in ALs had Alzheimer’s disease (AD) compared with 50% of residents in SNFs (Harris-Kojetin et al., 2016). Thus, memory care services and units are increasingly part of the levels of care available in ALs to meet this growing need (Carder, 2017). The literature indicates that individuals in long-term care are at risk of mortality following evacuation (Willoughby et al., 2017); people with dementia are particularly vulnerable (Brown et al., 2012). These aspects of the evolution within the LTSS system underscore the need to ensure that appropriate measures are taken to prepare for emergencies.
Different regulatory structures could cause ALs not to be as prepared for emergencies as SNFs. ALs are less regulated than SNFs (Castro et al., 2008). While SNFs are regulated by state and federal entities, ALs are primarily regulated at the state level (Walters, 2012). With much of the emergency regulatory work happening at the federal level, this discrepancy has resulted in ALs not having as many emergency preparedness regulations (Carder et al., 2015). Therefore, there may be structural lag between the increase in AL resident acuity and the regulations for emergency preparedness.
To date, however, few studies have examined the preparedness of ALs for emergencies (Brown et al., 2015; Castro et al., 2008). In one example, using mixed methods, Brown and colleagues (2015) investigated challenges faced by Florida administrators of ALs who experienced a hurricane. Approximately one quarter reported not having adequate generator support. Administrators also reported difficulty in deciding whether to evacuate or shelter in place (Brown et al., 2015). Due to a lack of attention in literature, the purpose of this study was to compare the regulations for emergency preparedness between Ohio SNFs and ALs.
Policy Comparisons
Overall, there is a layering of policies for SNFs that pertain to emergency preparedness. At the time our data source, the Ohio Biennial Survey of Long-Term Care (LTC) Facilities, was administered, Ohio SNFs were required to adhere to rules found in the Ohio Administrative Code and Revised Code (ODH, 2017b, 2018a, 2018c) as well as to the federal State Operations Manual and Life Safety Code because they are state and federally regulated (Allen, 2016; CMS, 2017a). In 2007, CMS distributed a checklist with items to help SNFs prepare for emergencies (CMS, 2016a; Lane & McGrady, 2018). These items later helped to form a final rule on emergency preparedness, often referred to as the “mega rule” by providers, that went into effect in 2017 (CMS, 2016b, 2017a); this rule incorporated a 17-item checklist, an emergency plan, a training and testing plan, policies and procedures, and a communication plan. By contrast, Ohio ALs are licensed and inspected by the ODH and adhere only to state codes (ODH, 2018b, 2018d). Of significance, ALs were not provided the CMS checklist and, thus, may be less likely to follow or be aware of the suggestions.
At the state level, there are numerous similarities in emergency regulations between ALs and SNFs (ODH, 2018b, 2018c). For example, all settings must have a written disaster preparedness plan, a 1-week supply of staple food, a 2-day supply of perishable food, and written transfer agreements with other facilities. Every setting’s plan is required to specify evacuation procedures: transportation provisions, fire protection and fire control and evacuation, procedures for locating missing residents, procedures during severe weather, and procedures related to being a setting located in close proximity to areas known to have specific disaster potential. In addition, on an annual basis, facilities are required to conduct 12 fire exit drills and two disaster preparedness drills, as well as train all staff in fire prevention. A monthly fire safety inspection is mandated. Both ALs and SNFs must also establish agreements with emergency service providers who can make timely repairs to systems (e.g., air conditioning, AC). This requirement supports the need to maintain a safe and comfortable temperature and humidity level, regardless of setting type. Despite differences between ALs and SNFs on aspects of staffing, both must have a plan for “adequate” staffing during emergencies.
Four key differences in emergency preparedness policies were evident in 2015 (see Table 1). First, the SNF written plan must spell out evacuation provisions for residents with physical or cognitive impairments, whereas the AL policy leaves out residents with cognitive impairment. A second difference is who receives training. AL regulation specifies that residents and staff must receive training in emergency and disaster preparedness, whereas SNF residents are not expected to receive training (only staff, volunteers, and consultants). Third, policies for SNFs require the maintenance of a routine and emergency drug supply and necessitate work with a licensed pharmacist, whereas policies for ALs stipulate that the setting must work with a pharmacist to maintain an emergency drug supply. Finally, setting types differ on generator requirements. Generators provide power for life support services like ventilators and emergency systems such as lighting (Allen, 2016; Ohio Health Care Association [OHCA], 2012, 2018). CMS articulates that an emergency generator is required for nursing homes that use life support systems. Ohio state rules do not specify a provision for requiring generators in ALs.
Key Policy Differences Between Ohio ALs and SNFs in 2015.
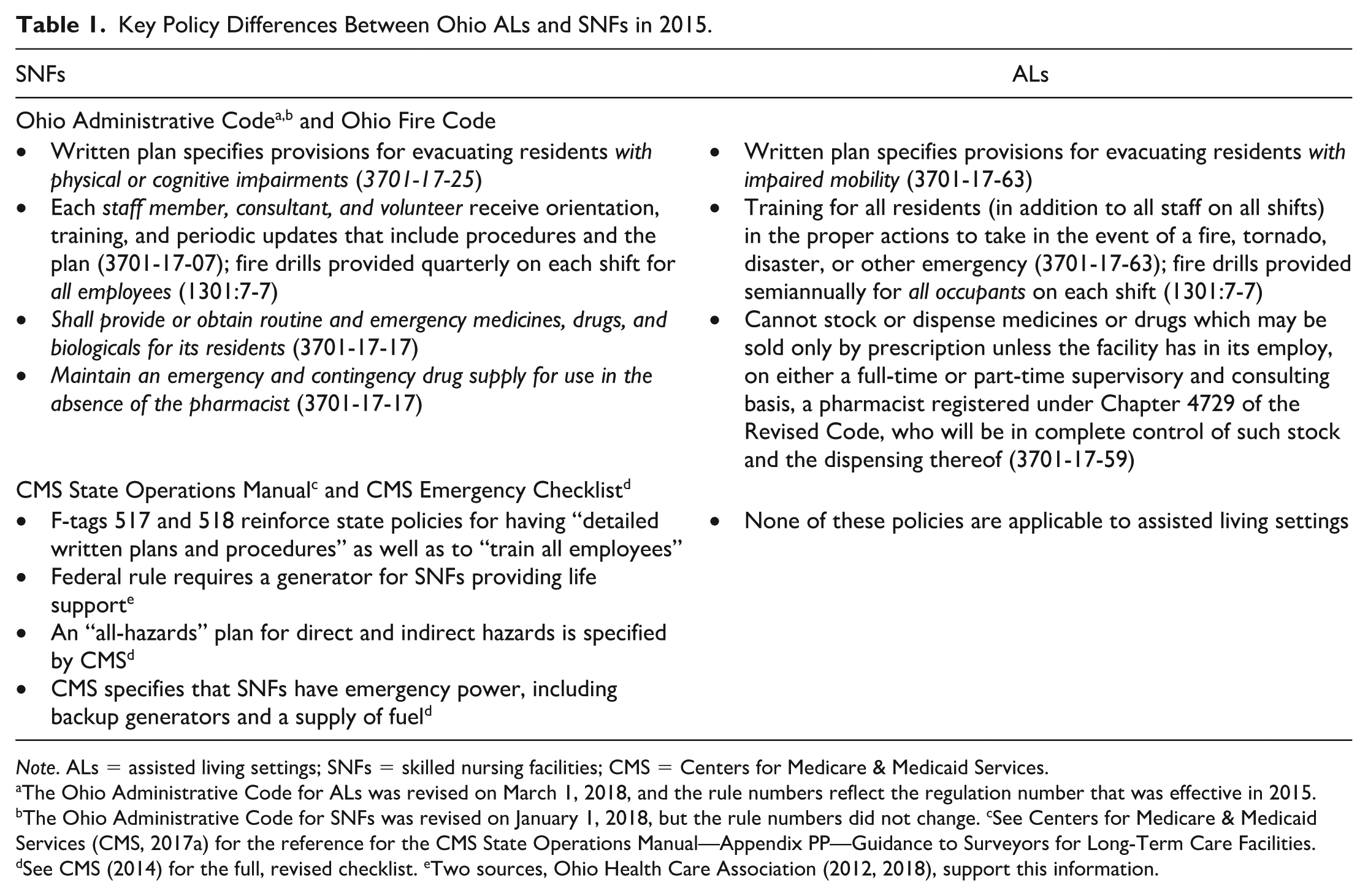
Note. ALs = assisted living settings; SNFs = skilled nursing facilities; CMS = Centers for Medicare & Medicaid Services.
The Ohio Administrative Code for ALs was revised on March 1, 2018, and the rule numbers reflect the regulation number that was effective in 2015. bThe Ohio Administrative Code for SNFs was revised on January 1, 2018, but the rule numbers did not change. cSee Centers for Medicare & Medicaid Services (CMS, 2017a) for the reference for the CMS State Operations Manual—Appendix PP—Guidance to Surveyors for Long-Term Care Facilities. dSee CMS (2014) for the full, revised checklist. eTwo sources, Ohio Health Care Association (2012, 2018), support this information.
Additional policy differences emerged from the emergency checklist (CMS, 2016a) administered to SNFs in 2007 that consisted of the suggestions to work with a health care coalition (HCC), discuss the emergency plan with the ombudsman, and create decision criteria for executing plans to evacuate and shelter in place. Items from this checklist were retained for later federal rules. In 2015, SNFs had to follow two particular regulations within the Medicare State Operations Manual Appendix PP that dealt with having an all-hazards written emergency plan and implementing training and drills to prepare adequately with periodic review of these procedures (CMS, 2017b). Due to the administration of the checklist, we expected additional differences in preparedness between ALs and SNFs to emerge.
In sum, the increased number and scope of requirements for Ohio SNFs may provide more protections when it comes to emergencies. Particularly, Ohio ALs may be more vulnerable to unforeseen events because (a) they are not beholden to federal standards, (b) state-by-state standards differ and lack specificity on topics like sheltering in place, and (c) the acuity level of residents in AL has increased. Moreover, the classification of ALs and SNFs into different health care occupancy groups in the Ohio Fire Code (ODH, 2017a) underscores the structural lag in policy which has not factored in the decline in cognitive and functional ability of the AL population.
The Current Study
The current study describes the state of emergency preparedness of ALs in Ohio during the year 2015 as compared with SNFs. Results may identify gaps in AL preparedness. We expected SNFs to report better adherence to emergency preparedness checklist items than ALs.
Design and Methods
We used the 2015 wave of the Ohio Biennial Survey of LTC Facilities, a survey of all SNFs and ALs in the state. Data for this online survey were collected in 2016 by the Scripps Gerontology Center. An online survey was sent to 958 SNFs and 655 ALs. The response rate was 95% for SNFs and 90% for ALs (Mehdizadeh et al., 2017). Response rates for this survey were high because the Ohio legislature required it and because Scripps performed extensive follow-up with administrators.
The emergency preparedness module was asked of all facilities as part of the 2015 Biennial Survey. The module was modeled after the CMS checklist that was distributed to SNF administrators in 2007 (CMS, 2016a). Some questions were altered slightly for the online survey format. Response rates were slightly lower for the emergency preparedness module; 570 ALs (87.02% response rate) and 869 SNFs (90.71% response rate) completed this particular module. A description of setting types is given in Table 2. Most LTC settings in our sample were of proprietary ownership, located in an urban area, and had more than 50 beds. Approximately 8% of small ALs and 40% of large ALs reported a memory unit. However, many ALs likely also serve residents with dementia, and many cases of dementia are underrecognized in ALs. Thus, the proportion with some sort of memory impairment is likely much higher (Zimmerman et al., 2014).
Characteristics of the Long-Term Care Settings (%).
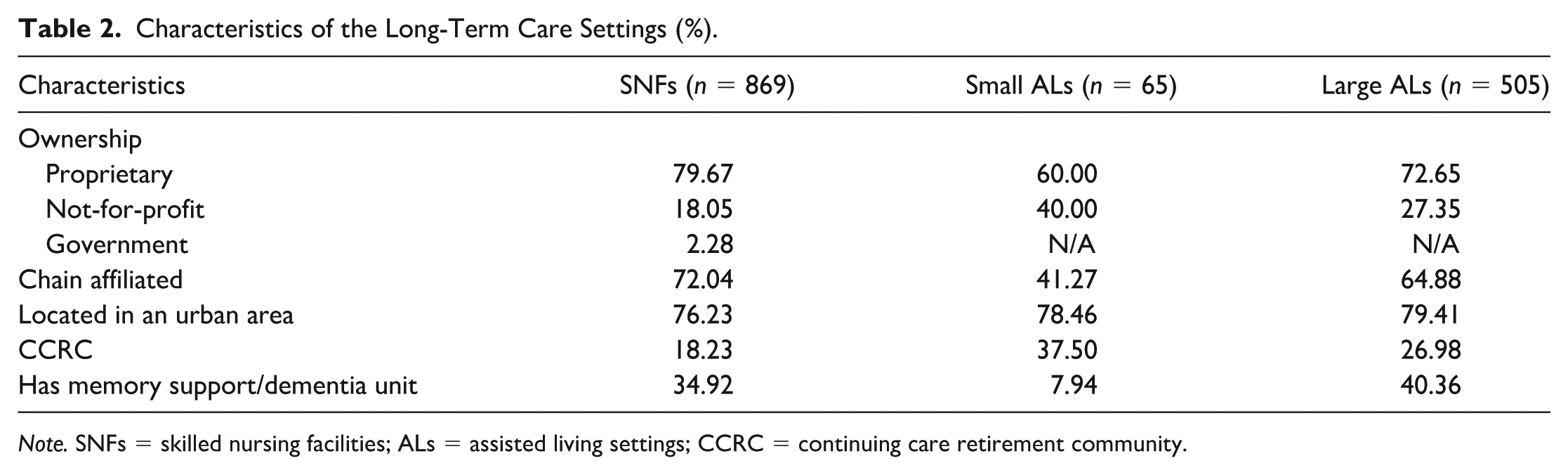
Note. SNFs = skilled nursing facilities; ALs = assisted living settings; CCRC = continuing care retirement community.
Similar to previous work, we stratify ALs by whether they have less than 25 beds (e.g., Thomas et al., 2018). Comparisons between setting types on responses to the emergency preparedness module were made using chi-square tests. Post hoc analysis using chi-square tests was performed to compare settings that completed the survey with those that did not; results indicated that those that did not complete were not statistically different than those that did complete based on bed size, chain membership, urban area location, or continuing care retirement community (CCRC) membership (p < .10) (see Supplementary Material).
Results
Responses to the Biennial Survey indicated that the vast majority of settings had some sort of emergency plan. Less than 1% of SNFs and ALs reported not having any plan in place. Administrators were asked about specific components of their evacuation and shelter-in-place plans; these responses are described in Table 3. The majority (98%) of SNFs and ALs had evacuation plans. However, there were differences in the plans by setting type. For example, 76% of SNFs and small ALs reported having agreements with hospitals compared with 60% of large ALs (p < .001). In addition, approximately 69% of SNFs compared with 61% of small ALs and 65% of large ALs reported having agreements with transportation providers (p < .01).
Components of Shelter-In-Place and Evacuation Plans for Ohio’s SNFs and ALs (%).
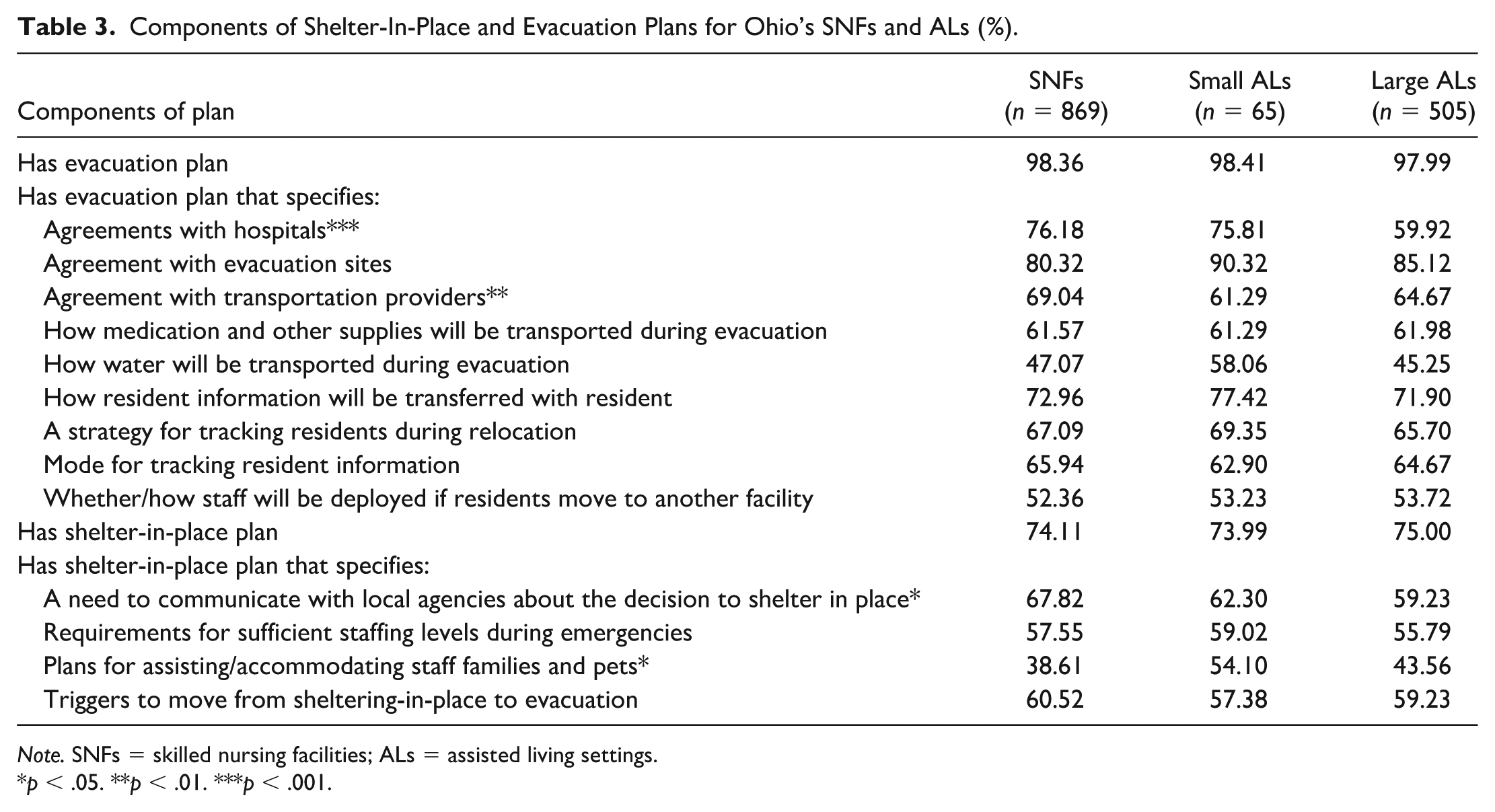
Note. SNFs = skilled nursing facilities; ALs = assisted living settings.
p < .05. **p < .01. ***p < .001.
The settings did not otherwise differ in the components of their evacuation plans. Approximately three quarters of SNFs and ALs had plans in place for how resident information would be transferred with the resident in the case of an emergency. A little over half of the SNFs and ALs in the study had detailed a plan for how staff would be deployed if residents moved to another LTC setting. Less than half of SNFs and ALs reported having plans for how water would be transported during an emergency.
Fewer administrators reported having a shelter-in-place plan than had an evacuation plan. Approximately three quarters of SNFs and ALs reported having shelter-in-place plans. SNFs were more likely than ALs to have plans that detailed a need to communicate with local agencies about a need to shelter in place. Approximately 68% of SNFs compared with 62% of small ALs and 59% of large ALs included this detail in their plans (p < .05). Another difference among the setting types was that ALs were more likely to report having plans for assisting or accommodating staff families and pets; compared with 39% of SNFs, 54% of small ALs and 44% of large ALs reported this component of their plan (p < .05). Other differences between the plan types were not statistically significant.
Figure 1 presents differences in emergency supplies comparing SNFs with ALs. There were statistically significant differences in supplies by setting type. Most notably, there was a 22-percentage point difference in the number of SNFs that reported having a backup generator as compared with large ALs. Compared with 76% of large ALs and 87% of small ALs, approximately 98% of SNFs reported having a backup generator (p < .001).
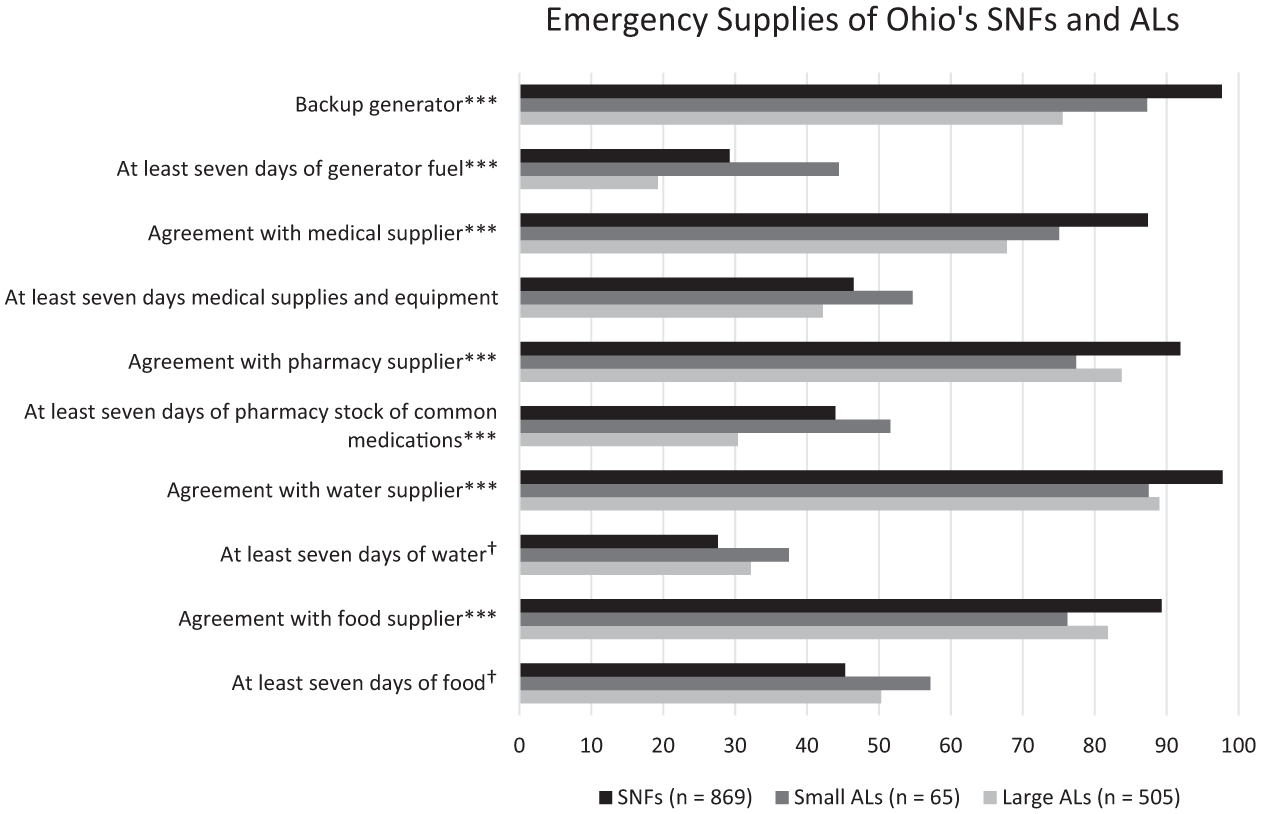
Emergency supplies of Ohio’s SNFs and ALs in 2015 (%).
Settings were asked to provide the number of days of different types of supplies they had on hand. We compared the percentage of facilities that had at least a week’s worth of supplies with those that did not; we chose this cut point because the CMS checklist indicated that facilities must have adequate supplies to shelter in place for at least 1 week (CMS, 2016a). Small ALs were the most likely to report having 7 or more days of generator fuel (44%) followed by 29% of SNFs and 19% of large ALs (p < .001). Approximately 44% of SNFs had at least 7 days of pharmacy stocks of common medications compared with approximately 30% of large ALs and 52% of small ALs (p < .001). Approximately 55% of small ALs had extra stocks of medical supplies and equipment; 46% of SNFs and 42% of large ALs had this amount. This difference was not statistically significant. In addition, SNFs were the most likely of the three settings to have contracts with food, water, medical, and pharmacy suppliers (p < .001). Approximately 98% of SNFs compared with 88% of small and 89% of large ALs had an agreement with a water supplier (p < .001). Compared with 87% of SNFs, 75% of small ALs and 68% of large ALs had an agreement with a medical supplier (p < .001). In addition, 92% of SNFs compared with 77% of small ALs and 84% of large ALs had an agreement with a pharmacy supplier (p < .001).
Table 4 describes collaboration with emergency partners and the completion of emergency drills by SNFs and ALs. Large ALs appeared to be the least likely to have contact with regional HCCs; approximately 11% of large ALs compared with 21% of small ALs and 16% of SNFs had contact with an HCC (p < .05). Only 18% of SNFs, 23% of small ALs, and 14% of large ALs reported discussing emergency plans with their area’s representative of the State Long-Term Care Ombudsman Program (p < .05).
Emergency Drills and Partners of Ohio’s SNFs and ALs (%).

Note. SNFs = skilled nursing facilities; ALs = assisted living settings.
p < .05. **p < .01. ***p < .001.
Table 5 indicates the percentage of facilities that have planned for each hazard. SNFs were more likely to plan for a loss of power; approximately 93% of SNFs compared with 89% of small ALs and 86% of large ALs were prepared for this emergency (p < .05). Large ALs were the least likely to prepare for extreme heat or loss of air conditioning (p < .01). Approximately 56% of SNFs, 62% of small ALs, and 52% of large ALs reported having plans for indirect hazards (p < .001).
Specific Hazards Prepared for by Ohio’s SNFs and ALs (%).
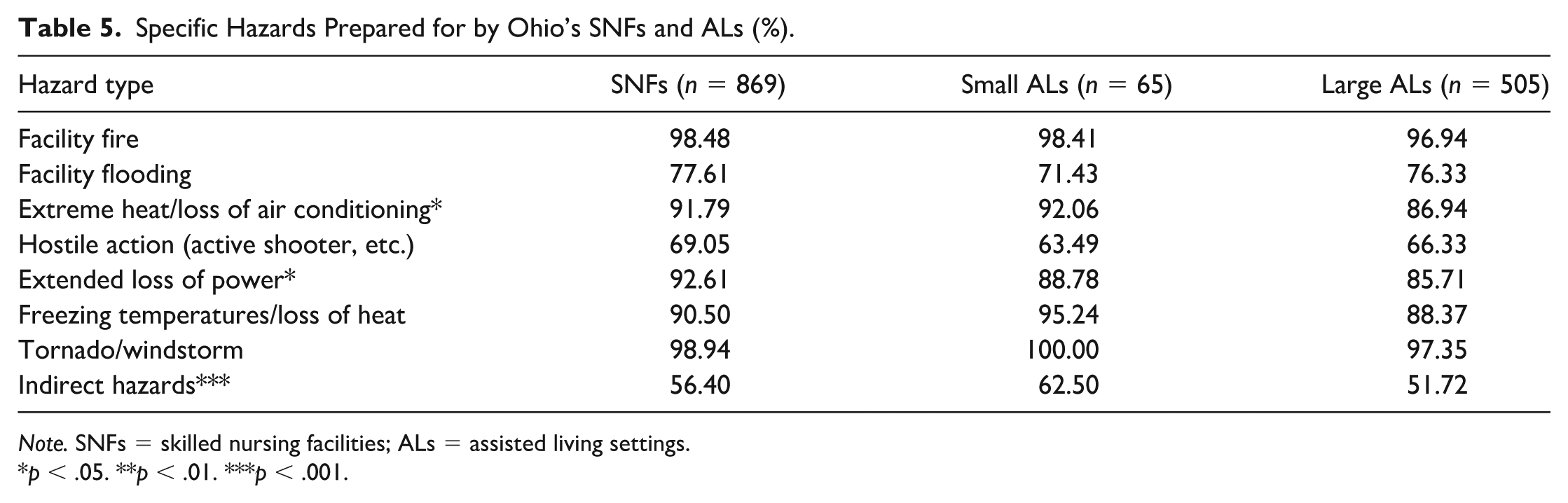
Note. SNFs = skilled nursing facilities; ALs = assisted living settings.
p < .05. **p < .01. ***p < .001.
Discussion
Our study found that ALs and SNFs are preparing for emergencies at similar levels on many plan elements. Most survey items evinced no statistically significant differences between setting types when it came to having a written plan or specifying critical elements of plans for evacuation (e.g., staff deployment, resident tracking, transportation of water, medication, resident information) or for sheltering in place (e.g., having sufficient staffing, triggers for evacuation). No significant differences emerged concerning reviewing the emergency plan, conducting drills, having communication procedures, or reviewing a plan with local ombudsmen. As expected, Ohio’s LTC facilities were well prepared for fires, tornados, and windstorms. Overall, these similarities were not surprising, given the overlap in state policies emphasizing having a written plan, preparing for adequate staffing during emergencies, and conducting annual drills for fires and tornados.
However, our study found some significant differences in emergency preparedness between SNFs and ALs, especially large ALs, which partially supported our hypothesis, especially concerning supplies. The 22-percentage point difference in the proportion of facilities with a backup generator between SNFs and large ALs was striking; yet when one considers that ALs lack a policy requiring backup generators, it shows that ALs are taking steps to prepare anyway, perhaps because they realize the vulnerabilities of their resident population (Barney & Roush, 2009).
We also found large ALs were least likely to have 7 days of generator fuel. SNFs were most likely to report that loss of power and extreme heat/loss of AC were included in their plans. These results could be interpreted as a reflection of the policy differences that require SNFs that have life support systems to maintain an emergency generator, whereas ALs are not required to do so. These results also align with those of Brown et al. (2015) in that Florida AL administrators reported deficient generator support.
Another result related to supplies was that large ALs were significantly less likely than SNFs to have a 7-day pharmacy stock of common medications. However, this measure of pharmacy stock was not a test of state policy and could have been misinterpreted by AL administrators because the question is tailored more for SNFs. ALs that are part of CCRCs partially explain why some ALs report having a week-long pharmacy stock (supplementary analysis available on request) because CCRCs include SNFs as the highest level of care (Groger & Kinney, 2006) that require an emergency drug supply. Adding specifications about the amount of emergency medications (and water) would also serve to protect residents and staff in disaster situations.
Interruptions in medication regimes can lead to an exacerbation of chronic conditions (Spurlock et al., 2019). In one study following households across Puerto Rico before and after Hurricane Maria, researchers found that disruptions to medical regimes were associated with increased risk of mortality (Kishore et al., 2018). Continuity of medication is important in the AL setting. Diabetes, for example, affects nearly 28% of AL residents (Thomas et al., 2018); hyperglycemic incidents are important to prevent with continued access to insulin (Munshi et al., 2016). Thus, Ohio policymakers should be aware of the current limitations on emergency medications in ALs, given the increased frailty of residents.
Furthermore, SNF administrators were also more likely to report including hospitals and transportation providers in their evacuation plans than ALs. Similarly, SNFs were more likely than ALs to specify communicating with local agencies about sheltering in place. When it came to drills and partners, we found that large ALs were least likely to engage with a regional HCC and local ombudsmen. These differences illustrate that SNFs are leveraging their community resources according to the principle that “all disasters are local,” (Hyer et al., 2007, p. 29) more so than large ALs, and in accordance with recommendations from the CMS Emergency Checklist (CMS, 2014). Large ALs reported less preparedness in these areas concerning localized communications and collaborations on plans, a potential problem when the next emergency occurs because large ALs may not have all the resources they need.
Earlier research on Texas SNFs and ALs that experienced Hurricanes Katrina and Rita demonstrated the need for policy change (Castro et al., 2008). Motivations for policy change for both SNFs and ALs were to improve resident and facility outcomes, such as mortality, and act as protection against financial losses due to evacuation and sheltering in place (e.g., staff overtime, transportation). Moreover, Castro and colleagues (2008) pointed to the need for better education of nurses regarding disaster management, not only in SNFs but also in ALs because residents who need feeding tubes or oxygen reside in both settings. An overarching theme from that study echoed the importance of better communication and coordination between LTC settings (regardless of type) and local and regulatory organizations involved with disaster response and public health (Hyer et al., 2007). Communication plans are necessary for evacuation; the emergency communications of the Florida SNF that experienced a loss of AC were focused entirely on state officials and agencies. Administrators delayed contacting local emergency management agencies (EMAs) (U.S. Senate Committee on Finance, 2018).
Like SNFs, ALs should be a focus of policy development for disaster preparedness at the local, state, and federal levels (Hyer et al., 2007). The current study provides evidence to suggest that the CMS Emergency Checklist should be broader in its application, including ALs, because SNF-eligible residents are increasingly AL residents using the Medicaid Waiver. Furthermore, our data support the consideration of a state policy for ALs that require an emergency generator (Castro et al., 2008). Generators are important for maintaining life-sustaining equipment such as ventilators; they are also critical for maintaining heating and cooling systems, necessary to shelter in place during a storm (Hyer et al., 2007). Having a generator shows concrete action has been taken and is different from having a plan to prepare for loss of power, which is interpreted uniquely by every setting. In 2017, 14 residents in a Florida SNF died as a result of Hurricane Irma disabling the AC system (Spurlock et al., 2019); as a result, Florida enacted a new policy for NHs and ALs to have emergency generators “capable of maintaining comfortable temperatures for at least 96 hr in the event of a power loss” (Fink & Stevens, 2017). This rule underscores that SNFs and ALs are responsible for resident safety and well-being through investment in essential supplies and the coordination of local resources (Barney & Roush, 2009).
Another area to develop among both setting types is contact with the local representative from the ombudsman program. In the event of an actual emergency, ombudsmen can help contact family members, track and visit residents, and transport resident belongings (Nelson et al., 2012). As shown in our results, this resource is underutilized among Ohio LTC settings. This finding parallels the results of a study by Nelson and colleagues (2012); although the role of the ombudsmen encompasses disaster preparedness, even disaster-experienced professionals perceive this role to be filled with challenges such as how to determine when to shelter in place or evacuate. Furthermore, their study identified gaps in ombudsmen’s training and ability to assess facility disaster readiness. Thus, there is much work to be done in providing resources and training to ombudsmen, as well as education to SNFs and ALs about what kind of partnership they should expect and work to cultivate.
Interestingly, we found in many cases that small ALs were more prepared than large ALs. This is problematic and important for policy, as large ALs house a greater share of the total number of AL residents (Harris-Kojetin et al., 2016). In addition, evacuation may be especially difficult in buildings of larger size, especially for ALs with multiple stories.
Limitations of this study are worth mention. Data were self-reported; therefore, there may be some inaccuracies. Data were from 2015, which may not reflect the most updated level of preparedness. In addition, the proportion of AL communities that reported having a plan for an extended loss of power was higher than the proportion that reported having a generator. To explain this discrepancy, we spoke to a previous director of the Ohio Assisted Living Association to obtain her response; she explained that ALs likely interpreted the question as whether they took any steps toward preparedness, such as battery-powered lights. The interview guide and specific responses are included in Supplementary Material.
However, there were a variety of strengths to the current analysis. Primarily, there was a very high response rate for Ohio SNFs and ALs achieved through stakeholder support, advance letters, and reminders, as well as the industry’s familiarity with the state-required survey (Berish et al., 2018). In addition, this study uses the only data available that could compare ALs with SNFs on their preparedness. While the data refer back to calendar year 2015, this provides a good baseline for measuring future differences or changes in preparedness after the Mega Rule has been in effect. Future research can assess the postrule state of emergency preparedness among LTC facilities, with an expectation that even greater differences between SNFs and ALs may be observed.
Conclusion
Although not as functionally impaired as SNF residents, AL residents have become frailer and more dependent on assistance with activities of daily living than in the past. This trend means that, in emergency or disaster situations, AL residents are vulnerable and special care is needed to ensure their safety and well-being. It may not be in the best interest of the AL resident population to treat assisted living as merely a social model of care, when, in fact, personal care, medication administration, intermittent skilled care, memory care, and hospice care are provided. This study illustrated that Ohio ALs are preparing in similar ways as Ohio SNFs, including major components of plans to evacuate, reviews of plans and drills, and preparations for expected hazards. However, some aspects were significantly different between ALs and SNFs. Furthermore, these differences were aligned with differing policies at the state and federal levels (e.g., backup generator and its fuel, communication with local agencies, emergency supplies of drugs). Future research can examine the sufficiency of AL emergency policies for each state, given increased frailty of AL residents.
Supplemental Material
Supplementary_material_-_interview_guide-_JAG-19-0226.R2 – Supplemental material for A Comparison of Emergency Preparedness Policies by Long-Term Care Setting Type in Ohio: Assisted Living Settings Lag Behind Nursing Homes in Key Areas
Supplemental material, Supplementary_material_-_interview_guide-_JAG-19-0226.R2 for A Comparison of Emergency Preparedness Policies by Long-Term Care Setting Type in Ohio: Assisted Living Settings Lag Behind Nursing Homes in Key Areas by Katherine A. Kennedy, Cassandra L. Hua and Ian Nelson in Journal of Applied Gerontology
Supplemental Material
Supplementary_material_-_Missing_analysis_in_tables_-_JAG-19-0226.R2 – Supplemental material for A Comparison of Emergency Preparedness Policies by Long-Term Care Setting Type in Ohio: Assisted Living Settings Lag Behind Nursing Homes in Key Areas
Supplemental material, Supplementary_material_-_Missing_analysis_in_tables_-_JAG-19-0226.R2 for A Comparison of Emergency Preparedness Policies by Long-Term Care Setting Type in Ohio: Assisted Living Settings Lag Behind Nursing Homes in Key Areas by Katherine A. Kennedy, Cassandra L. Hua and Ian Nelson in Journal of Applied Gerontology
Footnotes
Acknowledgements
We would like to thank Dr. Bob Applebaum for providing feedback on an initial draft and Malinda Deacon for providing industry-based insights to contextualize our findings.
Authors’ Note
This research consisted of a secondary data analysis at the facility level, and no humans were involved.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported, in part, by the Agency for Healthcare Research and Quality (AHRQ) T32 Training Grant (No. T32HS000011).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.