
Abstract
Electronic health records (EHRs) can improve quality of care and patient safety, as demonstrated in a variety of health care settings. However, greater use of EHRs in nursing homes (NHs) is needed. To understand which NHs have and have not adopted EHR systems, all federally certified NHs in Arkansas (n = 223) were surveyed, with 27.9% responding. Non-responders were similar to responders on all characteristics except for staffing skill mix, with responders having a higher skill mix than non-responders. Two thirds of responding Arkansas NHs reported having an EHR system in use (69.8%), while only a few reported no plans for an EHR system (4.8%). NHs with greater resources and in competitive markets were more likely to implement EHR systems. Full implementation across all NHs may require intervention, which should be explored in future research. In addition, future investigation should consider the level of interoperability of EHR systems that are in place among NHs.
The quality of U.S. nursing home (NH) care became a national policy concern in the mid-1980s when two federal reports identified shocking deficiencies in the care residents received (General Accounting Office, 1987; Institute of Medicine, 1986). Since that time, federal regulations and national initiatives have been put in place to improve the quality of NH care (Castle & Ferguson, 2010). Although the quality of NH care has improved, care issues persist. The 2014 federal report, Adverse Events in Skilled Nursing Facilities, estimated the cost of adverse events in NHs to be greater than 2.8 billion dollars and that two thirds of the adverse events that resulted in harm were preventable. Examples of adverse events identified by the report include medication errors, poor management of conditions, and preventable infections, among others (Office of the Inspector General, 2014).
Previous research has shown that Health Information Technology (HIT) can improve quality of care and patient safety in a variety of health care settings, including some NHs (Alexander & Madsen, 2017; Kruse et al., 2017; Olsho et al., 2014; Rantz et al., 2010). HIT comprises an “array of computer applications for health care” to be used by health care providers, administrators, and patients for a variety of clinical and administrative functions, such as census management, billing, and maintaining and using electronic health records (EHRs; Richard et al., 2009). Elements of HIT, specifically EHRs with their component capabilities for Computerized Clinical Decision Support (CCDS) and Computerized Physician Order Entry (CPOE), have been shown in clinical practice to assist in chronic care management, transitions of care (Kash et al., 2017; Rau, 2012), clinical decision making (Ben-Assuli, 2015), promoting evidence-based care (Damiani et al., 2010; Garg et al., 2005; McGinn et al., 2013), reducing medical errors (Kaushal et al., 2003; Ranji et al., 2014), and improving the quality of care (Adler-Milstein et al., 2015; Kern et al., 2013).
Although residential NH care faces many of the same issues as clinical practice (e.g., management of chronic conditions, medication administration, and monitoring), the use of EHRs in NHs has lagged behind that of acute and ambulatory care settings. Previous research has estimated that between 18% and 84% of U.S. NHs have EHR systems in place (to some level; Abramson et al., 2014; Kramer et al., 2010; Vest et al., 2018; Wang & Biedermann, 2012; Zhang et al., 2016), whereas 96% of hospitals (Charles et al., 2015) and 87% of private medical practices have implemented an EHR (Jamoom & Yang, 2016). Federal mandates and financial subsidies, primarily made available through the 2009 Health Information Technology for Economic and Clinical Health Act (HITECH), have facilitated the rapid uptake of HIT in other care settings (Gold & McLaughlin, 2016). However, NHs were not eligible to take advantage of the subsidies available through HITECH. As a result, the implementation of HIT in NHs has lagged behind many other health care providers.
There is interest in the role EHRs, and more generally HIT, may play in advancing the value paradigm. It is suggested that expanded EHR use in NHs may provide a mechanism to at least partially address identified NH quality concerns. Expert bodies have stressed the need for greater adoption and use of EHR among NHs (LTPAC HIT Collaborative, 2010; Office of the National Coordinator, 2013). Current research indicates that certain NHs, such as those that are non-profit (Wang & Biedermann, 2012; Zhang et al., 2016), those with more Medicaid residents, and those in more competitive markets (Zhang et al., 2016), are likely to have HIT systems. However, to consider initiatives to facilitate EHR use in NHs beyond the current rates, more information about which NHs have and have not implemented EHR systems is needed. This study addresses this information gap with results that identify and characterize NHs in Arkansas that have implemented EHR systems compared with those who have not.
Method
The study employed a cross-sectional survey research design in which federally certified NHs in Arkansas were surveyed about the extent of their adoption and use of EHRs.
Instrument and Other Data Sources
For this analysis, data on the status of EHR system adoption, and year of adoption for those who have an EHR system in place, were obtained using a survey. The survey instrument used in this study was adapted from a 34-question instrument developed by Stratis Health, a non-profit health care quality organization, to assess HIT use in NHs in Minnesota (Stratis Health, 2008). Minor modifications were made to the original Stratis Health instrument, primarily to shorten the survey’s length (e.g., some questions on NH characteristics were removed as this information was available from existing data sources—see below). All changes were reviewed for appropriate content, clarity, completeness, and format (Wood & Ross-Kerr, 2006) by five local and national experts in survey design, geriatric nursing, long-term care, and NH care who submitted their input and comments via email. The final instrument contained 28 questions (e.g., multiple choice, short answers) and was estimated to take no more than 20 min to complete.
Data to characterize the structure, process, and quality of NHs were obtained from the publicly available 2016 Long-Term Care: Focus on Care in the US (LTCFocus) data set and from the 2017 Certification and Survey Provider Enhanced Reporting (CASPER) data set purchased for the study (see Table 1 for measures that were drawn from the existing data sets). To identify characteristics that predict EHR adoption, data for the year before EHR adoption were used to characterize NHs that had installed an EHR system. Data for the most current year were used to characterize NHs that had not installed an EHR system. Additional information on community characteristics came from other publicly available data sources (e.g., Area Health Resources File, U.S. Census).
Definition of Measures and their Sources, by Type of Characteristics.

Note. LTCFocus data are available from www.ltcfocus.org; CASPER is available for purchase from Cowles Research Group (https://www.longtermcareinfo.com/index.php), the federal data repository. USDA RUCA codes are available at https://www.ers.usda.gov/data-products/rural-urban-commuting-area-codes/. AHRF data are available at https://ahrf.hrsa.gov/download.htm. U.S. Census data are available at www.census.gov. LTCFocus = Long-Term Care: Focus on Care in the US; NH = nursing home; RN = registered nurse; LPN = licensed practical nurse; CNA = certified nursing assistant; FTE = full-time equivalent; RUCA = Rural–Urban Commuting Area; USDA = United States Department of Agriculture; ERS = Economic Research Service; AHRF = Area Health Resource File.
Sample
All federally certified NHs in Arkansas identified through the 2016 LTCFocus data (n = 223) were included in the study. Contact information for those NHs was obtained from the Nursing Home Compare and facility websites.
Survey Procedures
Identification numbers were generated for each NH and were added to the survey instruments to allow characteristics of NHs obtained from existing data sources to be linked to the survey responses. Only study personnel had access to the cross-reference between the identification numbers and the names of the NHs, and all results were reported in aggregate to protect the privacy of the NHs.
A study packet containing a cover letter describing the study’s purpose and procedures, the instrument, and a postage-paid return envelope was mailed to administrators of NHs in Arkansas. The study packet also informed administrators of the voluntary nature of participation, the risks/benefits, and that those who completed the survey would be entered into a drawing for their NH to receive a survey incentive (US$500 for the NH’s resident activity fund). Based on receipt of the information about the study, completion and return of the survey was used to indicate implied consent. Four additional attempts (two postcard reminders and two mailings of full study packets) were made to obtain surveys from non-responding administrators.
Measures
EHR system implementation was assessed by a survey question that asked respondents to describe the extent to which an EHR system was being used in their facility (using in entire facilities, using in part of the facility, have EHR but not using yet, no system but assessing/planning for a system, and no system and not planning). Following Rogers’s Diffusion of Innovation Framework, NHs reporting that they had implemented a system in all or part of their facility were categorized as “implementers” and were asked to report the year in which implementation occurred. NHs that reported having not “gone live” with a system or were planning to implement a system were categorized as “planners.” NHs that reported not having an EHR system and not planning to install a system were categorized as “laggards” (Rogers, 1995).
A series of measures obtained from existing sources, listed and operationally defined in Table 1, were used to characterize the NHs based on their structure (e.g., organizational characteristics such as profit status and size), process of care (e.g., number of nursing staff hours per resident per day), quality of care (e.g., number of state inspection deficiencies), level of market competition (e.g., NHs share of the NH beds available in their county), and community characteristics (e.g., rurality). Structure, process, quality, and community measures for 2016 and for the year prior to the year of EHR system implementation (for those NHs who responded on the survey that they had installed a system) were merged into the data file.
Analysis
Responding and non-responding NHs were compared on a series of structure, process, quality, and community characteristics for the year 2016 to examine potential response bias. Univariate (e.g., means, proportions, standard errors) and bivariate descriptive statistics (e.g., t test, chi-square test) were used to characterize NHs based on the extent of their reported EHR system implementation. For NHs that reported EHR system implementation, data on characteristics were from the year prior to EHR system implementation. For the other NHs, data on characteristics were from 2016. Unadjusted logistic regression models were used to identify individual characteristics that were associated with greater or lesser likelihood of current EHR system implementation. Analyses were conducted using Stata, Version 14 (StataCorp, College Station, TX, USA). The alpha was set at .05.
Results
A total of 63 Arkansas NHs (27.9%) responded to the survey. The NHs that did not respond to the survey were not statistically different from the NHs that did respond to the survey on examined structure, quality, community, and all but one of the process characteristics. The responding and non-responding NHs differed in terms of staffing skill mix, with responding NHs having a significantly higher skill mix on average than non-responding NHs (M = 0.20, SD = 0.12; M = 0.16, SD = 0.10; p = .04; see Table 2).
Characteristics of NHs in Arkansas, Overall and Survey Response Status.

Note. Comparisons were made using chi-square test, t test, and Fisher’s exact test when comparison groups had less than 10 observations. NHs = nursing homes; RN = registered nurse; HRPRD = hours per resident day; LPN = licensed practical nurse; CNA = certified nursing assistant; HHI = Herfindahl–Hirschman Index; RUCA = Rural–Urban Commuting Area.
Of the 63 responding NHs, 44 (69.8%) reported having an EHR system implemented and in use in their entire facility and four (6.4%) reported having implemented a system but it was in use in only part of their facility. With those two groups combined, a total of 48 NHs (76.2%) were classified as implementers. Survey responses indicated that two (3.2%) NHs have a system in place but it has not “gone live,” and another three (4.8%) NHs were currently planning to implement an EHR system. NHs in these two groups were classified as “planners” (n = 5, 7.9%). Ten (15.9%) NHs reported not having an EHR system and not currently planning to implement one. These NHs were classified as “laggards.”
Structure, process, quality, and community characteristics of NHs by their implementation status—implementer (I), planner (P), and laggard (L)—are shown in Table 3. Occupancy rate was the only structure characteristic for which there was a significant difference between the three groups of NHs. Implementers had a significantly higher occupancy rate compared with planners and laggards (I = 75.1%, SD = 17.3%; P = 72.4%, SD = 17.5; L = 52.8%, SD = 14.6%; p = .04). There was no difference between the three groups for the other structural characteristics: chain affiliation, profit/non-profit status, hospital-based, percent Medicare residents, and percent Medicaid residents. There was no difference between implementers, planners, and laggard NHs for the four process characteristics (registered nurse [RN] hours per resident day, licensed practical nurse [LPN] hours per resident day, certified nursing assistant [CNA] hours per resident day, and skill mix) or the two quality characteristics (total health deficiencies and total deficiencies). Among the community characteristics, implementers were located in significantly more competitive markets than planners and laggards (I = 0.3, SD = 0.2; P = .5, SD = 0.3; L = 0.5, SD = 0.3; p = .02). Similarly, implementers were located in counties with significantly fewer available NH beds (I = 26.0%, SD = 6.0%; P = 38.0%, SD = 10.2%; L = 33.6%, SD = 13.8%; p = .001). There was no difference between the three groups of NHs based on the other examined community characteristics of rurality, county per capita income, and percentage of county non-White residents.
Characteristics of Responding Nursing Homes, Overall and by Extent of EHR Implementation.
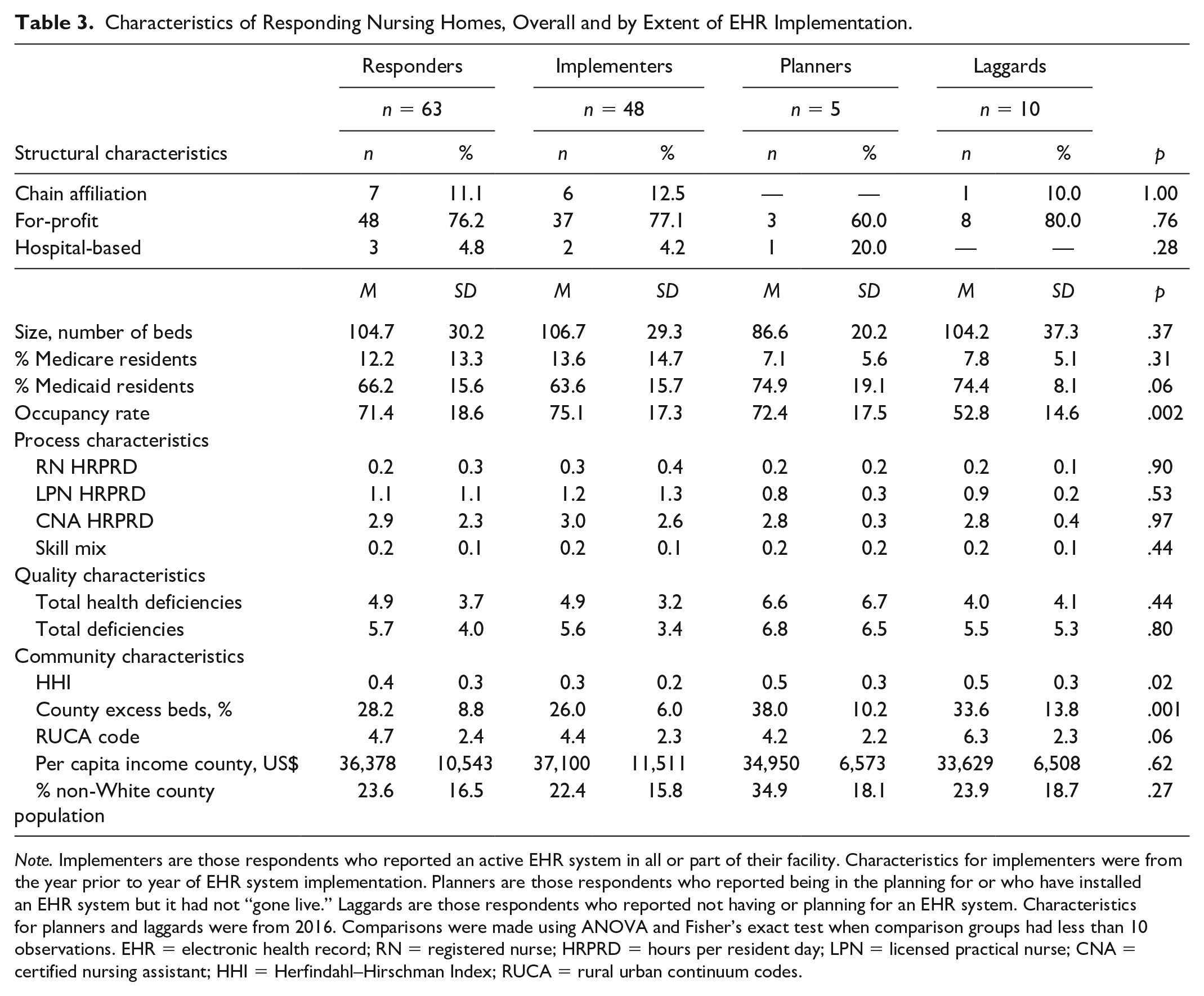
Note. Implementers are those respondents who reported an active EHR system in all or part of their facility. Characteristics for implementers were from the year prior to year of EHR system implementation. Planners are those respondents who reported being in the planning for or who have installed an EHR system but it had not “gone live.” Laggards are those respondents who reported not having or planning for an EHR system. Characteristics for planners and laggards were from 2016. Comparisons were made using ANOVA and Fisher’s exact test when comparison groups had less than 10 observations. EHR = electronic health record; RN = registered nurse; HRPRD = hours per resident day; LPN = licensed practical nurse; CNA = certified nursing assistant; HHI = Herfindahl–Hirschman Index; RUCA = rural urban continuum codes.
Bivariate analyses were conducted to identify structure, process, quality, and community characteristics that were significantly associated with implementers compared with those who currently had not implemented an EHR system (planners and laggards). Two structural characteristics and two community characteristics were significantly associated with implementers: lower percentage of Medicaid residents (63.6% vs. 74.5%, p = .02), higher occupancy rate (75.1% vs. 59.3%, p = .03), more competitive markets (0.30 vs. 0.51, p = .006), and counties with fewer available beds (26.0% vs. 35.0%, p = .0003). None of the other structure, process, quality, and community characteristics were significantly associated with implementing NHs (results not shown).
Discussion
Over the last several decades, a significant body of research has been undertaken to document the quality of care available in U.S. NHs and to identify factors associated with variations in the quality of care, such as staffing levels (Hyer et al., 2011), reimbursement rates (Hackmann, 2019), and leadership styles (Castle & Decker, 2011). That work has been used to inform policy and programmatic efforts to improve the quality of care (Castle & Ferguson, 2010; Institute of Medicine, 1986; Office of the Inspector General, 2014). The use of EHR in health care delivery has been shown to improve quality of health care in acute and ambulatory care settings (Adler-Milstein et al., 2015; Ben-Assuli, 2015; Kash et al., 2017; Kaushal et al., 2003; Kern et al., 2013; Ranji et al., 2014; Rau, 2012). A small but growing body of evidence also indicates that EHRs may provide quality and safety advantages in NH care (Alexander & Madsen, 2017; Kruse et al., 2017; Olsho et al., 2014; Rantz et al., 2010). Finding mechanisms to improve the quality of NH care—such as EHR—is particularly important given the fact that quality-of-care issues persist in the U.S. NH industry (Office of the Inspector General, 2014).
Previous research has shown that NHs have been slow to adopt this technology. Our findings indicate that 69.8% of responding Arkansas NHs have implemented an EHR system across their entire facility and 6.4% reported having an EHR system implemented but in use in only part of the facility. The implementation rate found is consistent with recent national-level estimates of EHR adoption among nursing facilities, such as the 84% adoption rate presented by Vest and colleagues (2018) and the 66% adoption rate presented in the report from the Office of the National Coordinator on skilled nursing facilities (Henry et al., 2018). Findings from this and other recent studies depict a considerably higher rate than has been reported by previous national and state surveys: For example, Abramson et al. (2014) reported that 18% of NHs in New York had fully implemented systems; Stratis Health (2008) reported that 32% of NHs in Minnesota had implemented an EHR system; and Wang and Biedermann (2012) reported that 39% of NHs had fully or partially implemented EHR systems. A national study of HIT in NHs found that HIT was used in resident care among 29.3% of responding NHs and in clinical support among 19.3% of responding NHs (Alexander & Madsen, 2017). The lower rate of EHR system implementation detected in these other studies compared with the present study may have to do with the date of data collection. Data for the present study were collected in 2018, whereas the data for the state-based studies were collected more than 5 years ago and the national study data are 3 years old. These findings may reflect a growth in EHR adoption rates among NHs.
Understanding characteristics of NHs who adopt innovations, such as installing EHR systems, is important to facilitate the diffusion of those innovations (Castle, 2001; Rogers, 1995). To date, however, only limited evidence has been available on the types of NHs that are more likely to be implementers of EHR. NHs in Arkansas with a fully or partially implemented EHR system were more likely to have fewer Medicaid residents and have a higher occupancy rate compared with NHs without currently implemented EHR systems. These findings are consistent with previous research on characteristics associated with EHR adoption (Alexander & Madsen, 2017; Zhang et al., 2016). Both of these structural characteristics suggest that a NH with more resources, as income from non-Medicaid residents is typically higher than from Medicaid residents (Grabowski, 2004), and more residents (higher occupancy rate) is an indicator of more income for the NH. As such, they may have the resources to be able to purchase the relevant technology and software for an EHR system.
It was also found that NHs with EHR systems were located in more competitive markets and counties with fewer available NH beds. Previous research has shown that NHs in highly competitive markets are more likely to innovate (e.g., adopt total quality management, open specialty units) to attract new residents (Banaszak-Holl et al., 1996; Zinn et al., 1998), which likely explains why these types of NHs in Arkansas were more likely to have implemented an EHR system (Zhang et al., 2016).
NHs’ profit status (profit or non-profit) was not found to be associated with adoption of EHR systems. Previous research has found that non-profit NHs were more likely to invest in HIT systems (Wang & Biedermann, 2012; Zhang et al., 2016) as it is presumed that their mission focus will prompt their investment of available resources into facility improvements, whereas for-profit NHs may be more selective in their investments back into the facility (Chesteen et al., 2005). Failure to support the previous research may be due to the makeup of the sample (74.6% of responding NHs were for-profit) and/or that non-profit NHs lack resources to invest in EHR systems even if their mission supports reinvestment in the facility.
Although these results in general—NHs with more resources can install EHR systems—may be intuitive, it is important to confirm them with sound research. If efforts to improve EHR adoption in NHs are initiated, actual evidence is needed to inform them. In this case, results indicate the need for additional resources to facilitate adoption, which suggests that federal mandates and subsidies that were instigated for hospitals and medical practices, may be necessary if nursing homes and their residents are to reap the benefits of EHR systems. Beyond financing, other barriers to adoption have been noted. For example, a systematic review by Kruse et al. (2015) found that user perceptions and issues with implementation were common barriers. Therefore, additional research may be necessary to determine how these other factors may compound the cost issue and to test ways to address them.
Limitations
The response rate for the survey was relatively low (27.9%). However, this examination of the known characteristics of responding and non-responding NHs, which found just one significant difference between the two groups, suggests the results are reasonably representative of NHs in Arkansas. Nevertheless, future research should explore methods for increasing response rate (e.g., different incentive mechanisms) and modes of data collection (e.g., face-to-face interviews or survey data collection at industry conferences). In addition, our results are limited by use of a dichotomous measure of EHR adoption. A measure which assessed the extent of use across the entire NH would provide a more nuanced picture of adoption. Future research should incorporate more specific levels of use and investigate how those levels are associated with facility outcomes (e.g., quality of care).
Conclusion
This study found a relatively high rate of implementation of EHR systems among Arkansas NHs. NHs with more resources and in locations with more competition are most likely to implement EHR systems. Full implementation across all NHs may require intervention, which should be explored in future research. In addition, future investigation should consider the level of interoperability of EHR systems that are in place among NHs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the University of Arkansas for Medical Sciences Medical Research Endowment.
Research Ethics Review
The Institutional Review Board (IRB) of the University of Arkansas for Medical Sciences determined the study did not require IRB review.