
Abstract
Adult day service centers (ADSCs) provide community-based long-term care, including meals, to racially diverse older adults, 47% of whom have dementia and consequently experience elevated nutritional risk. We examine nutritional behaviors for Chinese and Vietnamese persons living with dementia (PLWD) in ADSCs and evaluate the extent to which ADSCs provide person-centered nutritional care. Multi-stakeholder interviews were conducted. Data were coded using Dedoose and analyzed using Braun and Clarke’s six-step method. The Model for the Provision of Good Nutritional Care in Dementia guided analysis. Barriers to food intake included distracting meal environment, rigid mealtimes, and excessively restrictive diets. Conversely, peer relationships, culturally tailored meals and celebrations, and consistent staff assisting with feeding benefited PLWD. ADSCs can support healthy nutritional behaviors and quality of life among PLWD through person-centered nutritional care. To optimize nutritional services, further exploration is needed with respect to the ADSC environment, users’ culture and ethnicity, and liberalized diets for PLWD.
Adult day service centers (ADSCs) are becoming a preferred option for community-based long-term care for ethnically diverse older adults with chronic health conditions (The MetLife National Study of Adult Day Services, 2010). On any given day, ADSCs provide supervised care to more than 286,000 chronically ill individuals in the United States, nearly 60% of whom are racial or ethnic minorities (National Center for Health Statistics, 2019). More than 30% of ADSC clients have a formal diagnosis of Alzheimer’s disease, and it is estimated that 50% of clients experience dementia-related symptoms but lack a formal diagnosis (The MetLife National Study of Adult Day Services, 2010; National Center for Health Statistics, 2019). ADSCs were designed to provide an interactive, safe, and secure environment for older adults who require supervised care during the day (Sadarangani & Murali, 2018). In addition to recreational activities, many ADSCs provide health and therapeutic services, specialized cognitive stimulation, and memory training programs (Sadarangani & Murali, 2018). ADSCs by their nature also provide respite to caregivers of PLWD, reducing hostile behaviors toward caregivers and the caregiving burden they experience (Fields et al., 2012).
All ADSCs provide meals (typically breakfast, lunch, and a snack) to their participants, and most are eligible to receive subsides for these meals from the U.S. Department of Agriculture’s (USDA) Child and Adult Care Food Program (CACFP) (The MetLife National Study of Adult Day Services, 2010). Most centers offer a standard rotating menu or meals. These meals can be prepared on site by kitchen staff or are brought in from an outside vendor. CACFP requires that lunch meals include eight fluid ounces of milk, two ounces of lean protein, half cup of vegetables, half cup of fruits, and one cup of whole grains (USDA, 2017). Access to regular meals through the ADSC has been found to be a critical component to perceived improvements in quality of life and self-rated health among ethnically diverse ADSC clients (Dubus, 2017; Sadarangani & Murali, 2018). Proper nutrition is also an essential part of managing the care of ADSC clients with dementia.
Prevalence of malnutrition in persons living with dementia (PLWD) is higher than those who do not have dementia (Rullier et al., 2013). As many as 50% of PLWD living in the community have been found to be malnourished or at risk of malnutrition (Rullier et al., 2013). Compromised nutritional status in PLWD is associated with declines in physical function, cognition, and behavior (Roqué et al., 2013).
In light of their multi-faceted ability to provide health care, socialization, and healthful meals under the supervision of skilled providers (e.g., registered nurses [RNs], social workers, and, in some instances, dietitians), ADSCs are well-positioned to identify poor nutritional intake and support the nutritional needs of PLWD. However, little is known about current practices in the identification and management of nutritional problems in the ADSC regardless of whether they are living with dementia. Moreover, there is little available research on whether and how ADSCs cater to the culturally based dietary preferences of ethnically diverse PLWD who may be in their care. To address these knowledge gaps and generate an evidence base for future interventions, the purpose of this article is to examine nutritional behaviors for PLWD in ADSCs and evaluate the extent to which ADSCs currently provide person-centered nutritional care (PCNC).
Conceptual Model
In the absence of a framework to inform strategies for sound nutrition and dementia care specific to ADSCs, we looked to comparable models for evidence-based nutrition for PLWD in other long-term care settings. We referred to the Model for the Provision of Good Nutritional Care in Dementia developed by Murphy et al. (2017). At the center of this model is the goal of achieving PCNC, which is defined as prioritizing the nutrition and hydration needs and preferences of people living with dementia. The authors identify six domains that need to be addressed as part of the PCNC: (1) availability of food and drinks, (2) tools, resources, and environment, (3) relationship to others when eating and drinking, (4) participation in activities, (5) consistency of care, and (6) provision of information. Availability of food and drink refers to the need for regular main meals and snacks, recognizing that energy needs may not be satisfied adequately through conventional food intake patterns and adaptations need to be made in response to differences in wandering behaviors, and sleep patterns. Tools, resources, and environment captures the range of resources needed to support the delivery of food and hydration. Relationship to others when eating and drinking references shared mealtimes and also notes that it is important to respect a person’s preferences to eat alone which may evolve in the course of dementia. Participation in activities refers to ways activities can be used to engage adults and stimulate appetite. Consistency of care refers to uniformity in how nutritional care is provided across settings where PLWD live and receive care, including staff members. Finally, provision of information refers to how education, training, and support can guide nutritional care for PLWD by formal and informal caregivers.
Method
In this exploratory descriptive pilot study, we used semi-structured qualitative interviews to support in-depth exploration of current practices around nutrition in ADSCs serving ethnically diverse PLWD. To obtain an interdisciplinary multi-stakeholder perspective, we utilized purposeful sampling. We invited dietitians, RNs, social workers, administrators, and ADSC clients at two sister ADSCs that predominantly service Chinese and Vietnamese older adults in Northern California to participate in one-on-one interviews with the first author.
ADSC clients with mild cognitive impairment were invited to participate if they were deemed capable by their legal proxy and RNs at the center. Capacity was assessed as being able to coherently state preferences or answer questions. The interviewer would exclude anyone who lacked the capacity to answer three consecutive interview questions coherently, although this was ultimately unnecessary. In addition, with the help of center staff, we identified caregivers of older Asian Americans with advanced dementia and invited them to participate in our study, as well.
The interview guide, initially developed by the first author, was informed by Murphy et al.’s (2007) model. The guide was reviewed and edited by the President of the California Association for Adult Day Services, the Principal Investigator of the Center for Study of Asian American Health at New York University School of Medicine, and an ADSC program administrator to ensure the questions were coherent, comprehensive, and relevant to study participants. The questions asked depended on the interviewee’s background.
For professional staff members, interview questions included, but were not limited to, the following:
Describe the foods served at your ADSC. What types of food and meals might you serve in an average week as part of your standard menu?
Describe mealtime at your center. How are clients seated? How are meals served? How long do they have to eat?
What challenges, if any, do clients with dementia encounter at mealtime? How do you help them address these challenges?
How do you handle feeding and meals for clients with dementia who may be limited in their capacity to eat and/or feed themselves?
How do you incorporate clients’ cultural preferences within their diets?
How do you maximize clients’ choice with respect to what and how they eat?
How do Child and Adult Care Food Program guidelines affect what food you serve and how you serve it?
For ADSC clients, interview questions included the following:
What are the biggest barriers you encounter to eating well?
What foods do you enjoy most at the center? Are there any foods you dislike here?
How do your health conditions affect the way you eat?
Do you need any help at home when it comes to cooking, eating, or food shopping? If so, what type of help do you require? Who helps you?
Describe how often you eat during the day and what foods you commonly eat?
For caregivers, interview questions included the following:
Tell me about your loved one’s diet. What do they like to eat? Are there foods they dislike?
How does their eating pattern at home differ from the way they eat at the center?
What challenges do you encounter in helping them eat well?
All interviews were conducted in a closed-door private room at the ADSC. An in-person certified medical interpreter was hired to assist the first author in conducting interviews with clients and caregivers with limited English proficiency. Interviews were recorded and subsequently transcribed verbatim by a professional transcription company after any potential identifiers had been removed from the recording. In addition to transcribing the interviews, the transcription company also translated the original recording into English whenever necessary. This served to cross-check that the initial interpretation was accurate.
Ethical approval for the study was obtained through the institutional review board at the first author’s institution (approval no. IRB-FY2018-1566). Participation in the study was voluntary, and participants provided written consent only after the study was explained to them and all of their questions were answered in their preferred language. Participants received a $25 incentive for participating in the study.
Data Analysis
Coding of interview data was completed using Dedoose, a qualitative software program. Analysis was guided by Braun et al.’s (2019) “six-phase” approach inclusive of (1) familiarization, (2) generating codes, (3) constructing themes, (4) defining themes, (5) revising themes, and (6) producing the report. In Phase 1, the first and second authors read through all transcripts to familiarize themselves with the data. In Phase 2, codes were initially generated deductively based on findings from published research focused on nutritional care of PLWD. The first and second authors worked collaboratively to generate an initial codebook which evolved as the coding process went on. The first and second authors met weekly to review and discuss disagreements on coding and come up with new or revised code when necessary. In Phase 3, the codes were grouped together into themes, based on the study’s framework, and in Phase 4, the themes were initially defined in relation to this study by the first author. These themes were cross-checked by the second author and collaboratively revised in Phase 5. Stage 6 was comprised of the written manuscript.
Results
In total, we conducted 13 interviews. Study subjects included two full-time RNs, one full-time social worker, one part-time registered dietitian, one community health worker, five ADSC clients, and three family caregivers of ADSC clients with advanced dementia. Participant characteristics are provided in Table 1.
Breakdown of Participant by Characteristics.

Note. ADSC = adult day service center.
Data were organized within Murphy’s Model for the Good Provision of Nutritional Care in Dementia and validated the seven main themes within that model, which are presented in Table 2. Certain subthemes were unique to the ethnicities within the sample studied.
Themes Affecting Person-Centered Nutritional Care in Dementia Users.
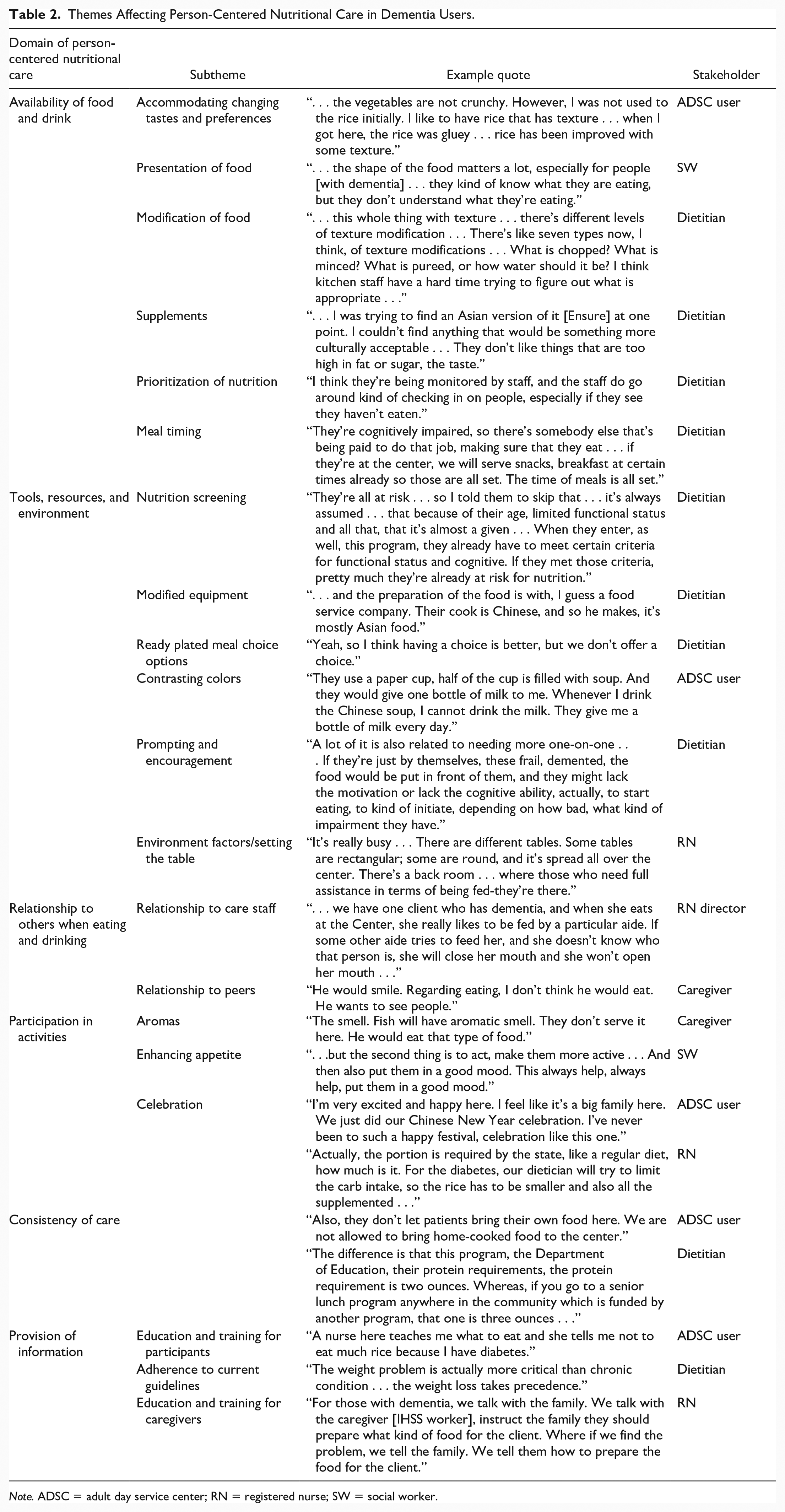
Note. ADSC = adult day service center; RN = registered nurse; SW = social worker.
Availability of Food and Drink
The meal was viewed as a fundamental part of the ADSC experience, and creating and serving healthy, tasteful meals was a priority to ADSC staff. Nutritional status was viewed by staff as a key health indicator, and observing mealtime was a routine part of the ADSC nurse’s clinical assessment: “. . . so we have to check on the client how they eat and ask how—is there any problem . . . with swallowing? Is the client agitated or refusing food?”
Meal timing
Food and drink were provided at designated meal and snack times only. For example, lunch was served over a period of 30 to 40 min. Those with special diets or those who required additional time to complete their meals received their plates first allowing them more time to finish. Emphasis was mostly on food and less so on drink. Meal and snack time were the only opportunities for hydration. Established mealtimes, centered around one large meal, were inconsistent with how ADSC clients ate outside of the center. At home, for example, clients had several small meals per day, which did not occur at regular times. One client described his daily eating pattern: In the morning, I have breakfast on my own . . . Then I come here, where I get the supply of the second breakfast . . . So I come here for the second meal. Then the third meal is the lunch. After lunch I take the afternoon nap, and another meal after that. That’s the time I will need to eat. In a day, I have a dinner, and another meal before I go to bed. Five meals a day, then I would have enough nutrients.
Presentation
Plated meals were served on plastic trays with plastic utensils. Most of the time, portions and quantities were described as excessive leading to significant waste. However, the dietician felt that meals did not contain sufficient amounts of protein. The dietitian elaborated that CACFP guidelines were not consistent with those of other nutrition programs that serve older adults, such as the Older Americans Act (OAA) Congregate Meal Program, which serves functionally independent older adults in senior centers (as opposed to those, described here, who have functional limitations and require supervised care in an ADSC). For example, older adults in the ADSC were potentially getting smaller portions of protein than healthier older adults attending a senior center whose meals are subsidized by the OAA: The difference is that this program, the Department of Education [which administers CACFP], their protein requirements, the protein requirement is two ounces . . . I think it could be higher. I think if it went up to three ounces, it would be better because protein is really essential.
Pureed food, while very common because of the pervasiveness of oral health issues, was seen as less visually appealing. Peers regularly compared what was served to them with what was served to others at their tables. This led to frustration among those who relied on pureed foods and found their meal to be unappetizing. The on-site social worker spoke to the appearance of foods, particularly purees, and how altering the appearance of purees could potentially enhance the food’s appeal to PLWD: . . .[they] can make some pureed food in the shape of a steak, right . . . the shape of the food matters a lot, especially for people—they kind of know . . . they kind of know what they are eating, but they don’t understand what they’re eating.
Supplements
Nutritional supplements commonly used in the United States, such as Ensure, were not available at the ADSC and generally hard for clients to come by for those who needed them. Clients who benefited from nutritional supplementation relied on family members to purchase them because they were expensive and not covered by insurance. In addition to being prohibitively expensive, the taste and the milk-base also made these supplements unappealing. The RN explained, . . . most of them do not like to drink the supplements because even though there is still sweetener . . . it’s too sweet for them. For the culture, the Asian culture, they just don’t like the flavors—in the strong sweetness it has to it. They try to mix it with full milk or water or put it into their oatmeal.
Tools, Resources, and Environment
The environment in the ADSC, which catered to many of the client’s functional impairments (e.g., raised toilet seats, hand grab bars), was less conducive to PCNC for PLWD. Meals were prepared off site, plated, and served to clients on plastic tray. This meant that clients had limited choice in what they ate, and aromas associated with cooking and mealtimes that stimulate hunger were absent. Modified equipment for feeding and eating was also not readily available. Meals were eaten on paper plates with plastic utensils. Mealtime was not a focused activity. A TV was on in the background and clients played cards or other games as they ate.
Staff members, did however, provide prompting and encouragement to support individuals with advanced dementia while eating. This was essential to supporting nutritional intake: They might be distracted mentally or whatever, and they can’t get them to focus on the food and start eating. I think having a staff member to just come around, maybe to encourage them to eat or take a bite, or actually help them to start. Helping them to start that first bite might initiate the mental, something clicks, and they start eating, or they got refocused.
Clients with dementia or feeding difficulties were kept in a separate dining area at lunchtime, the RN described: “. . . we try to get a room, especially for those dementia patients. We have a feeding . . . put in a more quiet environment inside a room.”
Caregivers reiterated the importance of aroma to the mealtime process for ADSC clients: “. . . roasted meat, roasted duck . . . he likes flavorful food. Fish has to be pan-fried and aromatic. He smells the aroma, he can smell the aroma.”
Relationship to Others When Eating or Drinking
The presence of others, including staff and peers at mealtime, affected PLWD positively. However, in advanced dementia, crowded dining rooms, with upward of 100 clients, often became overwhelming and confusing.
Relationship to peers
Peer relationships and support were essential to mealtime at the ADSC. Friends encouraged one another to eat more. When a person with dementia was not consuming their lunch at the center, peers might call or send a text message to the caregiver informing them they had not eaten. Excessive peer stimulation was also problematic, however. Integrating persons living with advanced dementia into the social milieu of the mealtime environment was challenging, and often it was easier to isolate them to get them to eat, as the ADSC RN described: “I’ll bring her to our nursing office. It’s more quiet and I try to feed her.”
Relationship to care staff
For PLWD, it was imperative that they had access to a consistent staff member to support their needs at mealtime. Caregivers and staff remarked that clients’ food intake, and mood deteriorated when there was a change in staffing. The community health worker said, . . . another patient with dementia, she stopped eating for a while, and she was dropping weight as well, and we didn’t know why . . . we just discovered that the aid who usually serves her food was out. She was on vacation . . . just because she didn’t have someone familiar to feed her that’s why she just did not want to eat.
Participation in Activities
Daily therapeutic activities were a fundamental part of the ADSC experience, but they were rarely linked to nutrition. The meal in and of itself was an activity that allowed social interaction. One class of activities, however, was centered around food: cultural celebrations. Important holidays, such as the Chinese New Year, were celebrated with large meals featuring traditional foods including dumplings and fish. Exercise, which was one of the most widely enjoyed activities, also provided the added benefit of stimulating appetite. The social worker emphasized the exercise time spent at the ADSC as being beneficial to proper nutrition: I want to kind of arouse them in a way that put them in a good mood and then put them in—physically, they’re more active. They’re throwing ball, they’re kicking ball, so naturally use more energy and you’re more hungry.
Consistency of Care
Nutritional care of PLWD at the ADSC was often inconsistent with the care they received at home and the instructions they received from health care providers around what they should eat. The dietician referenced Academy of Nutrition and Dietetics (AND) guidelines surrounding diet in dementia and emphasized that diets were not being sufficiently liberalized. The dietitian, however, was clear that those living with dementia would benefit from a liberalized diet: I think with that [dementia] population, they should really not be on any restricted diet. They should really just have a regular diet that may have more salt and fat in it, actually. That’s actually what the position is, the current position of AND.
ADSCs were unable to provide the flexibility needed to honor participants’ preferences because of strict regulations set forth by the CACFP that challenged their ability to provide a sufficiently liberalized diet. The dietitian also lamented the fact that physician orders for a liberalized diet, which were needed to work around CACFP regulations, were rarely provided. However, one caregiver reported that the physician had specified a liberalized diet at home for his father, but at the ADSC, he was subjected to whatever was being served.
More continuity between food served in settings might have been achieved if clients with dementia were allowed to bring food in from home that they preferred. However, this practice was strongly discouraged and said to be a violation of the ADSC’s formal policy. One client wanted to bring in food from home, but was not allowed to per protocol. A caregiver described, how, as a result of this, his father, who suffers from dementia, will simply not eat when at the ADSC: “He doesn’t eat here . . . He doesn’t like it . . . He said it’s tasteless.” Observations of clients at mealtime, however, revealed that policies around bringing outside food were not fully enforced, and many clients brought seasonings, such as onion and salt, from home to enhance the flavor of the meal.
Provision of Information
Information and training for caregivers and staff around nutritional support for PLWD were provided, although mostly on an “as needed” basis and not in a routine or standardized manner. Clients were referred to the part-time dietitian by the RN only if they were prescribed a special diet by a physician. RNs were primarily responsible for providing nutritional education to clients, and, sometimes, family members. RNs did recognize the important role home health aides and other caregivers played with respect to what and how food was consumed outside the center. They described working with and educating caregivers and family members. Generally, however, education was focused on diabetes and cardiovascular disease risk reduction as opposed to management of nutrition in dementia. RNs also provided individualized trainings for home health aides on a case-by-case basis: If it’s a regular diet, we just instruct them how they should eat because many of the clients’ hypertension—the main part is we instruct them to eat less sodium, less fat, less cholesterol food. I teach according to their diagnosis. If they have high cholesterol, then I have to tell them how to restrict your diet on the fat, all this. If the client has diabetes, of course, I have to teach them the carb control part. Yeah if the client has high potassium or renal diet, of course, we have to be more strict.
Discussion
The purpose of this article was to examine nutritional behaviors for PLWD in ADSCs and to evaluate to what extent ADSCs currently provide PCNC for this population. To our knowledge, this is the first study to examine nutrition in Asian American users of ADSCs. We utilized the Model for the Provision of Good Nutritional Care in Dementia as our standard of care to assess whether nutritional services within ADSCs are meeting the needs of a culturally diverse group of PLWD. We identified strengths and weaknesses within the ADSC nutrition programs and identified both challenges and opportunities that exist for ADSCs in providing PCNC.
Delivering person-centered care to PLWD involves creating a positive social environment that allows PLWD to experience well-being through care that fosters the development of meaningful relationships (Fazio et al., 2018). In our study, we found that all team members acted based on a mutual understanding of the clients’ nutritional needs and preferences. Essential to this was the fact that the relationships between the interdisciplinary staff and Chinese and Vietnamese clients were grounded in cultural understanding. Not only do culturally informed relationships support the provision of appropriate meals, in our study, they also allowed staff, clients, and caregivers to more easily negotiate mutually satisfactory treatment goals around nutritional care (Epner & Baile, 2012).
Based on the six domains of PCNC within the Model for the Provision of Good Nutritional Care in Dementia, the ADSC excelled in two, in particular, consistent staffing and collaborative relationships between staff, caregivers, and clients. The ADSC lends itself to a collaborative environment in which interdisciplinary staff members develop relationships with PLWD over time and can work as a team to support optimal nutrition in PLWD. For example, in our study, the registered dietitian assessed and managed nutritional intake, RNs provided education to clients and caregivers and assessed weight and other relevant clinical measures, and social workers connected clients to nutritional resources outside the ADSC. Since nursing assistants played a critical role with respect to supporting eating and feeding (Liu et al., 2018), we recommend additional training and greater involvement for them within the collaborating team to further optimize mealtime care. We also recommend including their perspectives in future qualitative inquiries of ADSCs.
There were also domains of the Model for the Provision of Good Nutritional Care in Dementia that could be strengthened to enhance the ADSC’s ability to deliver a wide range of flexible dietary recommendations and culturally sensitive food and nutrition services. These include the tools, resources, and environment for PLWD at mealtime, as well as the availability of food and drink. In our study, food was described as being bland, clients reported they lacked choice in what they ate and when they ate it, and the environment at mealtime was distracting and overstimulating for PLWD.
Although ADSCs are community-based centers, barriers to PCNC parallel to those that commonly occur within more institutional environments, such as nursing homes (Milte et al., 2018). Literature on optimizing nutritional support for PLWD in nursing homes supports, among other things, flexible mealtimes, liberalized diets, adapted utensils, and enhancing the presentation of food to make it more appetizing (Anderson et al., 2016; Aselage, 2010; Slaughter et al., 2011).
Using the Provision of Good Nutritional Care in Dementia as a guide, we recommend the following as suggestions for improvement based on our findings: creating “hydration” stations where participants can have ready access to water and other drinks and providing meals throughout the day as opposed to fixed mealtime (Popejoy et al., 2017). In addition, PLWD are stimulated to eat when food and drink are visually appetizing and when flexible open access to food and drink is given (Johansson et al., 2015). We suggest working with outside vendors to alter the presentation of meals and incorporating the opinions of clients in the design of monthly menus. For PLWD with physical impairments, having foods accessible by hand (i.e., finger food) and contrasting crockery to define plates and utensils while eating may support independent eating (Brook, 2014). Removing possible distractions at mealtime, such as television and replacing it with soothing music, may reduce confusion and anxiety for PLWD (Hicks-Moore, 2005). Not having to separate PLWD from the social milieu of mealtime would also facilitate more integration for PLWD with other cognitively intact ADSC clients. We also recommend conducting a detailed social history on clients to learn about their favorite foods and cultural preferences to incorporate them into their meals. As the aging population diversifies, it is critical that person-centered nutritional care accounts for ethnic food preference.
ADSCs may, in particular, benefit from adopting models of “culture change” that have been implemented in skilled nursing facilities to make them less institutional and more person-centered (Petriwskyj et al., 2016). This includes the creation of a more home-like environment. RNs can work with other staff members to reduce possible distractions, especially noise from televisions, that might interfere with meals. Food and drink would be available at all times; clients’ favorite foods, ethnic foods, and recipes would be prepared to create more individualized menus; and clients would have greater choice and autonomy with respect to when, where, what, and with whom to eat. In addition, making the dining area less of a multi-purpose room may help PLWD remember its use and cue appropriate mealtime behaviors.
It is important to note that the ADSC’s capacity to offer flexible and liberalized diet is hindered by strict regulations associated with the CACFP, which is a federally sponsored program that provides ADSCs with subsides for meals provided. CACFP regulations require that participating ADSCs serve meals that are consistent with the USDA’s Dietary Guidelines for Americans (DGA; Hartle & Jensen, 2011). The ADSC studied here exclusively provided meals that were low in salt, sugar, and fat to adhere to DGA. Any deviation from this had to be justified using a physician’s order (Hartle & Jensen, 2011). We strongly recommend that, where appropriate, ADSC staff members advocate with physicians, on behalf of their clients with poor nutritional intake, for a liberalized diet. We also recommend that ADSC operators advocate for changes to the CACFP, including clearer guidance on appropriate use of pureed food for older adults. Currently, the only guidelines on pureed food within the CACFP are for infants (USDA, 2017).
Limitations
This study had a number of limitations. The small sample reflects two sister Northern California ADSCs that participate in the CACFP thus limiting generalizability. Centers that do not participate in the CACFP may have different nutritional offerings and be more likely to achieve PCNC. In addition, not all ADSCs have consulting dietitians. The two centers studied primarily served Chinese and Vietnamese clients. Providing PCNC in ADSCs serving more heterogeneous clientele may present different challenges. Finally, these centers were located in California, a unique policy environment, that differs considerably with respect to services and supports available for older adults. Thus, findings may not be generalizable to ADSCs in other states. In addition, the sample was limited to Asian Americans, who make up just 4% of the overall aging population (Administration for Community Living, 2019). Thus, the findings may not be generalizable to the elderly dementia population as a whole.
Conclusion
As the population ages and diversifies, there will be a growing demand for culturally appropriate long-term care services for older adults, particularly in light of the looming dementia epidemic. ADSCs are well-positioned within communities and can leverage their culturally and socially congruent relationships with clients to address the unique nutritional needs of diverse PLWD. However, ADSCs and their interdisciplinary staff would benefit from additional clinical guidance on eating and feeding practices in PLWD. In addition, providers should advocate for changes in CACFP policies for PLWD and remove unnecessary barriers in achieving PCNC.
Footnotes
Authors’ Note
The study was approved by the institutional review board, University Committee on Activities Involving Human Subjects (UCAIHS), New York University (Approval No. IRB-2018-1566).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this presentation was supported in part by the National Institute on Minority Health and Health Disparities of the National Institutes of Health under Award Numbers U54MD000538 and P60MD000538. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.