
Abstract
Keywords
Introduction
The U.S. population is aging rapidly. By 2050, 88.5 million individuals will be aged ≥65 years, and the population requiring long-term care services is projected to double from 13 million in 2000 to 27 million (Family Caregiver Alliance, 2015; Vincent & Velkof, 2010). Many older adults are choosing to age-in-place in their homes and communities and to maintain their independence (Ewen et al., 2017). Oral diseases (particularly dental caries and periodontal disease) are common noncommunicable diseases (NCDs) that can negatively influence health and wellbeing of older adults and reduce their quality of life (Abrao et al., 2010; FDI World Dental Federation, 2015; Shaw & Cummings, 2012). The number of healthy teeth, and oral health more broadly, is associated with masticatory ability, dietary intake, and proper nutrition, which can affect a person’s immune system, diabetes management, and other NCDs (Touger-Decker et al., 2014).
The U.S. Department of Health and Human Services administers programs for the elderly population through the Administration for Community Living (ACL)/Administration on Aging (AOA), authorized under Title III of the Older Americans Act (OAA), federal legislation that first passed in 1965 (Beasley et al., 2018). Through the “Aging Services Network,” a wide array of home- and community-based services (HCBS) are provided to assist families and caregivers to support the health and well-being of individuals aged ≥60 years or those with disabilities and to help them live independently in their homes and communities (Barrett & Schimmel, 2010; Colello & Angela, 2016). Participants can receive one or multiple HCBS as follows:
Case management (coordinated health care): evaluates, develops, and integrates health care plans based on patient and family/caregiver needs and arranges services to promote patient safety, quality of care, and cost-effective outcomes;
Congregate meals (group meals away from home): provides nutritious meals in a group setting;
Family caregiver support (resources): provides physical and/or emotional care services and resources to informal caregivers and families that provide care;
Home-delivered meals (nutritious meals delivered at home): provides adequate and nutritious meals to homebound individuals or those who are unable to obtain or prepare their own meals;
Homemaker (activities of daily living [ADLs] assistance): provides assistance with household tasks to older adults unable to perform critical ADLs or instrumental activities of daily living (IADLs); and
Transportation (access enabling service): provides travel arrangements to facilitate access to essential medical services, stores, pharmacies, and so on (ACL Organization, 2017; AoA, n.d.; Indiana Health Coverage Programs, 2017).
HCBS are an option to delay institutionalization or allow institutionalized older adults who have regained sufficient functional capacity to return home and be sustained in their communities (Thomas, 2014; Thomas & Mor, 2013). However, lack of awareness, social isolation, functional impairment, and scarcity of services often become a barrier to utilization increasing the risk of disability and mortality (Ewen et al., 2017).
Oral health is an important aspect of health that can affect general well-being and quality of life and vice versa (Dolan et al., 2005). Dental caries, periodontal disease, and tooth loss are key indicators of oral health in older adults. Among U.S. adults aged ≥65’years in 2011–2012, approximately 96% had experienced caries in their permanent teeth during their lifetime, 19% had untreated dental caries, and 19% were edentulous (Dye et al., 2015). About 60% of dentate adults aged 65’years and older have periodontitis (Eke et al., 2018), a chronic inflammatory disease that may include systemic health effects.
Regular dental visits are necessary for early detection and timely treatment of oral diseases, particularly life-threatening conditions such as oral cancers as adults above the age of 65 years account for 60% of oral cancer–related deaths (Maramaldi et al., 2019). The delay or failure to seek dental care can compromise an individual’s health status and lead to late diagnosis or treatment of oral diseases, which generally worsen over time if left untreated (Wall et al., 2012). Poor oral health can also exacerbate chronic health conditions such as diabetes (Mark, 2018) and affect proper nutrition, which is essential for physical and mental health and well-being of older adults (Razak et al., 2014).
Maintaining nutrition, personal oral hygiene, and access to dental services remain significant challenges for many older adults, especially for those with disabilities (Dolan et al., 2005; Evashwick et al., 1982; Razak et al., 2014; Tilly, 2016). Research has shown that older adults receiving HCBS under the OAA are more vulnerable individuals who are older, food insecure, and who reported more co-morbidities and functional limitations (Sonnega et al., 2017; Vieira et al., 2017).
A national survey of OAA program recipients found that more than 85% of individuals receiving HCBS were able to remain at home, and without the relatively basic and inexpensive assistance from the HCBS to meet their needs, many would have been institutionalized (Arora et al., 2019). Remaining at home and aging-in-place significantly reduce nursing home, hospital admissions, and health care expenditures (Ferris et al., 2016).
A study from the 2008 Nationwide Emergency Department Sample of the Health care Cost and Utilization Project showed that health care expenditures related to oral diseases among older adults are costly as they have more complex medical needs, which utilize more hospital resources to manage their cases. The same study reported that in 2008, among individuals aged ≥60 years, a total of 50,881 emergency department (ED) visits were related to dental conditions, and the mean hospital charge per ED visit was US$1,114 (Nalliah et al., 2013). This re-emphasizes the importance of regular dental visits and screening for older adults. Nevertheless, in 2015, less than half of adults (46%) aged 65 years and older in the United States had a dental visit or accessed the oral health care system in the preceding 12 months (Healthy People 2020, 2016). As a result, additional coordinated efforts are needed to strengthen health care services and improve service utilization for older adults to meet their psychosocial, physical, nutritional, and oral health needs (Dolan et al., 2005; Joostepn, 2015; Yellowitz & Schneiderman, 2014).
In April 2016, the U.S. Congress reauthorized the OAA amending the definition of disease prevention to include oral health screenings as part of routine services for older adults (144th Congress, 2015–2016; American Dental Association, 2015; Tilly, 2016). To date, no study has assessed the influence of HCBS in relationship to elders’ oral health. Therefore, our objective was to assess HCBS participants and their utilization of oral health services by exploring selected factors potentially associated with infrequent dental use among community-dwelling older adults by the main HCBS groups.
Method
Study Design and Participants
This cross-sectional study used existing de-identified secondary data from the 2014 National Survey of Older Americans Act Participants (NSOAAP), a nationally representative survey of the OAA population. The NSOAAP is a telephone interview survey focusing on consumer quality valuation of services and self-reported outcomes to assess special needs and other health-related characteristics such as physical and social functioning among the older population (AoA, n.d.). Participants received a letter explaining the survey and could decline their participation; consent was given by agreeing to continue with the phone survey. Some NSOAAP participants received and responded to multiple HCBS questionnaires. Consequently, each HCBS data set was analyzed independently because of multiple responses from the same individual across surveys.
The 2014 NSOAAP included data from recipients of six HCBS with a total sample of 5,923. As the HCBS-Family Caregiver Support had caregivers as its target population (questionnaire respondents) rather than HCBS users, this group was excluded from the analysis. Our final analytical sample comprised 3,995 participants aged ≥65 years who received any of the following HCBS: case management (539), congregate meals (985), home-delivered meals (1,018), homemaker services (464), and transportation (989).
Measures
The outcome variable for this study was “infrequent dental use” defined as “not having a dental visit in the past 12 months” (Thomson et al., 2010). It was derived from the NSOAPP question “About how long has it been since you last visited a dentist?” with seven valid responses: (1) 6 months or less; (2) more than 6 months, not more than 1 year; (3) more than 1 year, not more than 2 years; (4) more than 2 years, not more than 3 years; (5) more than 3 years, not more than 5 years; (6) more than 5 years ago; (7) never have been to dentist. Responses of “Don’t know” and “Refused to answer” were excluded, and the remaining responses were dichotomized as “routine dental users” defined as “those who had a dental visit in the past 12 months” (6 months or less; more than 6 months, but not more than 1 year ago) or “infrequent dental users” (more than 1–5 years; never been to a dentist). The modified Andersen’s Behavioral Model was utilized to propose factors related to service utilization. This model incorporates predisposing, enabling, and need factors that can influence health services utilization (Babitsch et al., 2012; Joostepn, 2015). In this study, it was used to identify independent variables of interest with potential influence on dental services utilization among community-dwelling older adults.
Predisposing factors included sociodemographic characteristics such as age (65–74 years, 75–84 years, ≥85 years); sex; race/ethnicity (Hispanic, Non-Hispanic White, Non-Hispanic Black, Other); marital status (married, widowed, divorced/separated/never married); and educational attainment (less than high school diploma, high school diploma or GED, higher education). Enabling factors included residence location (urban, suburban, rural) and income (less than US$20,000, more than US$20,000). Need factors (health status) included total number (≤3, 4–6, ≥7) of medical conditions (i.e., hypertension, heart disease/other heart problems/stroke, high cholesterol, diabetes, cancer); having three or more ADLs limitations; and satisfaction with general health status, which was dichotomized as “Yes” (Excellent, Very Good, Good) and “No” (Fair, Poor).
Statistical Analyses
All analyses were weighted to account for the NSOAAP multistage sampling scheme to ensure nationally representative findings. Analyses were performed with SAS version 9.3. Weighted univariate analysis was conducted to describe the participants in each HCBS group in terms of the independent variables listed above. Weighted bivariate and multivariate logistic regression analyses were performed to explore the associations between infrequent dental use and independent variables and to calculate unadjusted odds ratios (OR), adjusted odds ratios (AOR), and 95% confidence intervals (CI95). A controlled manual entry for backwards selection multivariate logistic regression analysis was employed to produce the parsimonious model. Each HCBS group was analyzed individually due to the possibility of participants receiving more than one service.
Results
Home- and community-based service participants were predominantly female, non-Hispanic White, widowed, belongs to low-income group (<US$20,000), lived in urban areas, and had attained high-school education or higher (Table 1). Among the congregate-meals group, about one in five participants were ≥85 years (19%), whereas nearly one in three participated in case management (34%), home-delivered-meals (35%), and homemaker (39%) services were in this age group. More than half of participants in case management (55%) and homemaker (54%) services had ≥7 medical conditions. Rural residency ranged from 21% (case management) to 29% (congregate meals). The proportion of infrequent dental use was highest among participants of case management and home-delivered meals (63%) and the lowest among those participating in congregate meals (41%).
General Distribution of People Using Home and Community-Based Services.
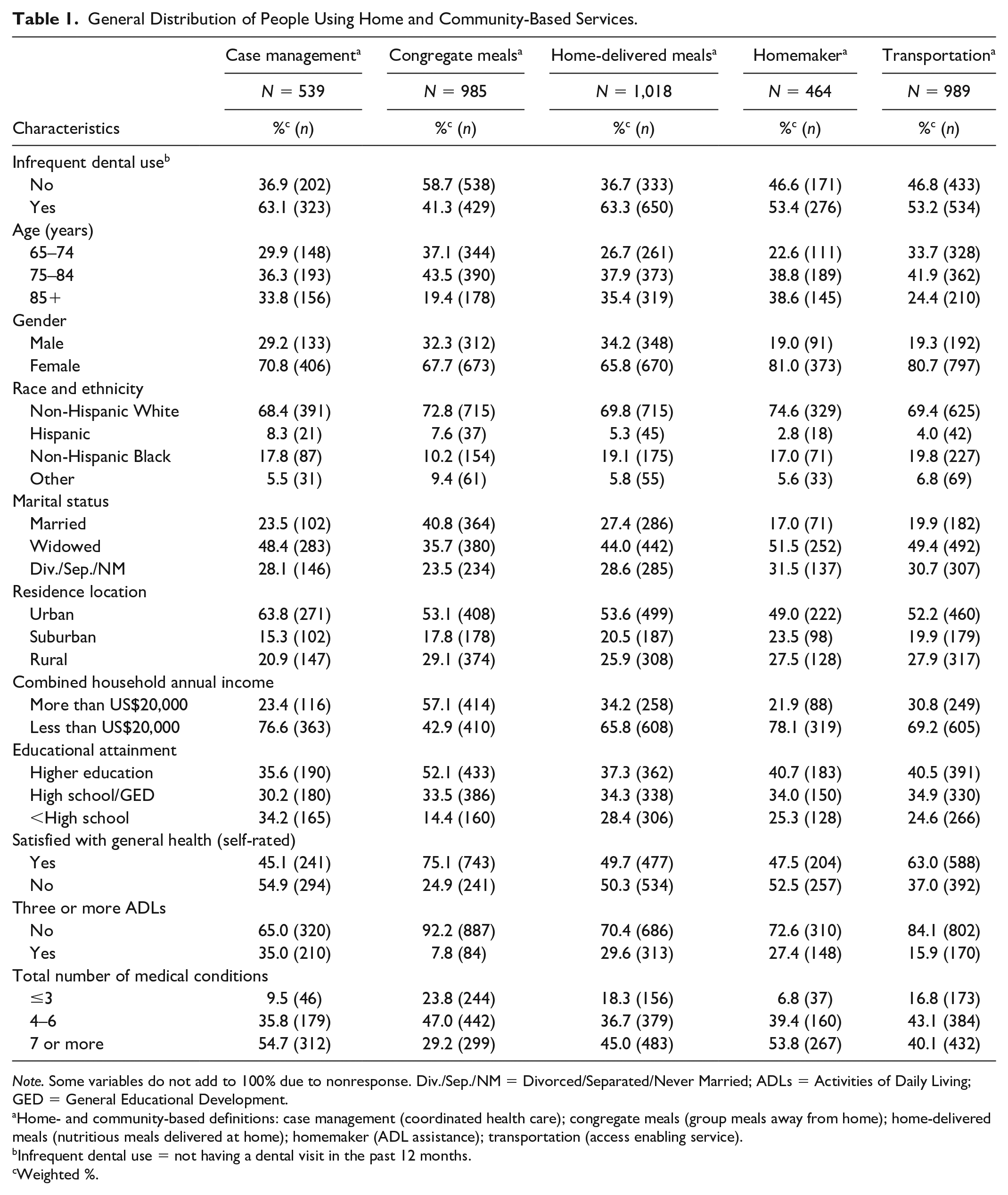
Note. Some variables do not add to 100% due to nonresponse. Div./Sep./NM = Divorced/Separated/Never Married; ADLs = Activities of Daily Living; GED = General Educational Development.
Home- and community-based definitions: case management (coordinated health care); congregate meals (group meals away from home); home-delivered meals (nutritious meals delivered at home); homemaker (ADL assistance); transportation (access enabling service).
Infrequent dental use = not having a dental visit in the past 12 months.
Weighted %.
Table 2 shows the unadjusted association between infrequent dental use and selected characteristics for each of the five HCBS groups. For adults receiving case-management services, those living in rural areas (OR = 0.42, CI95 = [0.20, 0.86]) were less likely to be infrequent dental users compared to those living in urban areas. Individuals ≥85 years receiving home-delivered meals (OR = 0.62, CI95 = [0.39, 0.99]) or transportation services (OR = 0.43, CI95 = [0.25, 0.74]) were less likely to be infrequent dental users compared to younger participants. Overall, low educational attainment (i.e., less than high school diploma) was the strongest indicator for being an infrequent dental user among participants receiving congregate meals, home-delivered meals, and homemaker and transportation services.
Association Between Infrequent Dental Use and Select Characteristics of People Using Home and Community-Based Services in the United States, 2014 (Unadjusted Models).
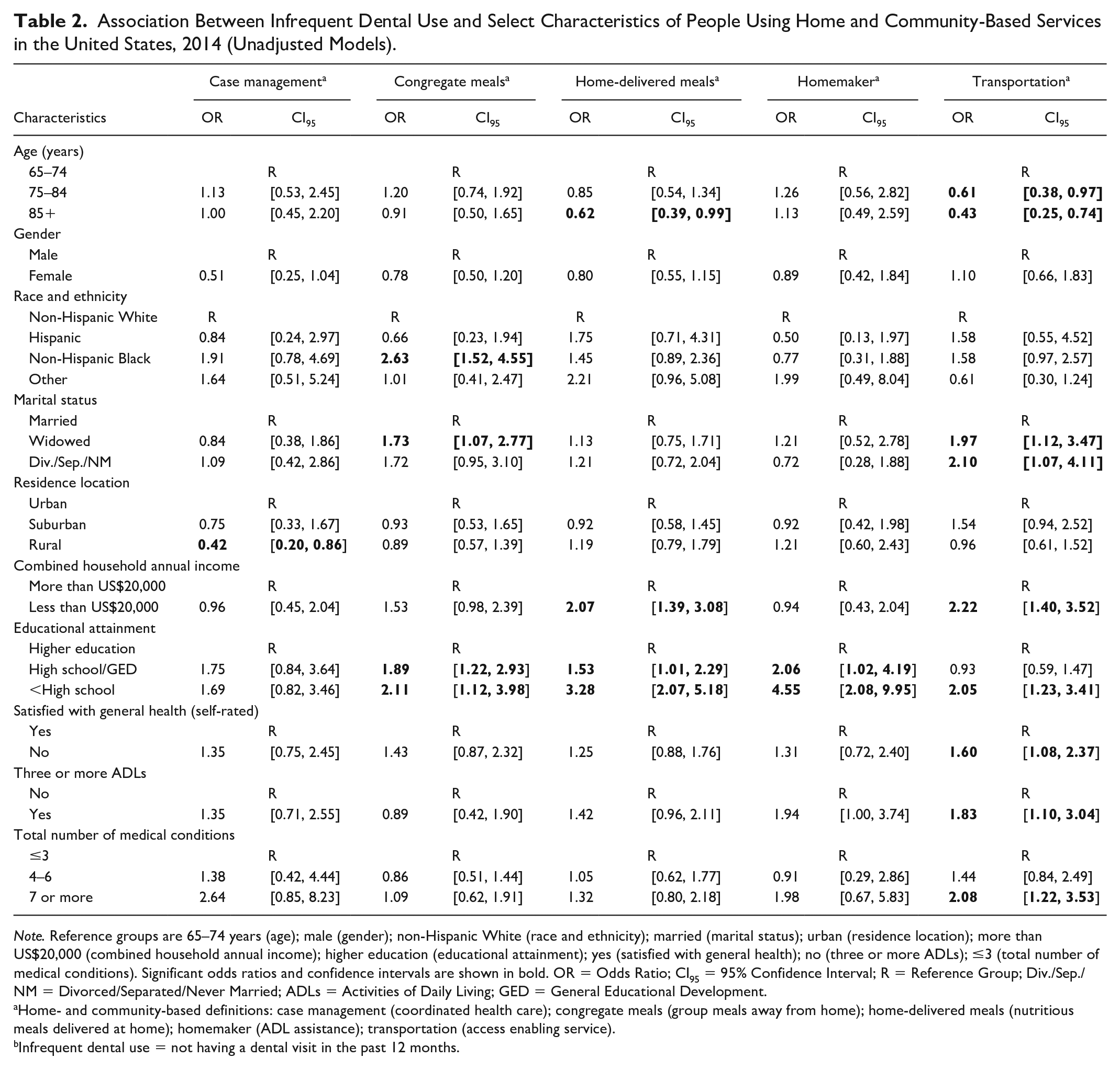
Note. Reference groups are 65–74 years (age); male (gender); non-Hispanic White (race and ethnicity); married (marital status); urban (residence location); more than US$20,000 (combined household annual income); higher education (educational attainment); yes (satisfied with general health); no (three or more ADLs); ≤3 (total number of medical conditions). Significant odds ratios and confidence intervals are shown in bold. OR = Odds Ratio; CI95 = 95% Confidence Interval; R = Reference Group; Div./Sep./NM = Divorced/Separated/Never Married; ADLs = Activities of Daily Living; GED = General Educational Development.
Home- and community-based definitions: case management (coordinated health care); congregate meals (group meals away from home); home-delivered meals (nutritious meals delivered at home); homemaker (ADL assistance); transportation (access enabling service).
Infrequent dental use = not having a dental visit in the past 12 months.
Table 3 shows multivariate modeling results for each of the five HCBS assessed. After controlling for potential confounders, low educational attainment remained significantly associated with infrequent dental use across all HCBS except for case management (AOR = 1.31, CI95 = [0.47, 3.70]). The association between infrequent dental use and low educational attainment ranged from an AOR = 2.03 (CI95 = [1.02, 4.02]) for transportation to AOR = 4.74 (CI95 = [1.75, 12.8]) for homemaker services. Among older adults receiving transportation services, those who were widowed or divorced/separated/never married were more likely to be infrequent dental users compared to the married group (AOR = 3.06, CI95 = [1.45, 6.46] and AOR = 2.31, CI95 = [1.04, 5.10], respectively). Reporting having ≥7 medical conditions was associated with infrequent dental use compared to having ≤3 medical conditions (AOR = 2.95, CI95 = [1.39, 6.25]) among transportation participants. In the same group, persons aged 75 to 84 and 85 years and older were less likely to be infrequent dental users compared to those aged 65 to 74 years (AOR = 0.43, CI95 = [0.24, 0.76] and AOR = 0.23, CI95 = [0.11, 0.47], respectively). Having difficulty with three or more ADLs was associated with infrequent dental use only for persons receiving home-delivered-meals services (AOR = 1.89, CI95 = [1.14, 3.13]).
Association Between Infrequent Dental Use and Select Characteristics of People Using Home and Community-Based Services in the United States, 2014 (Adjusted Full Models).
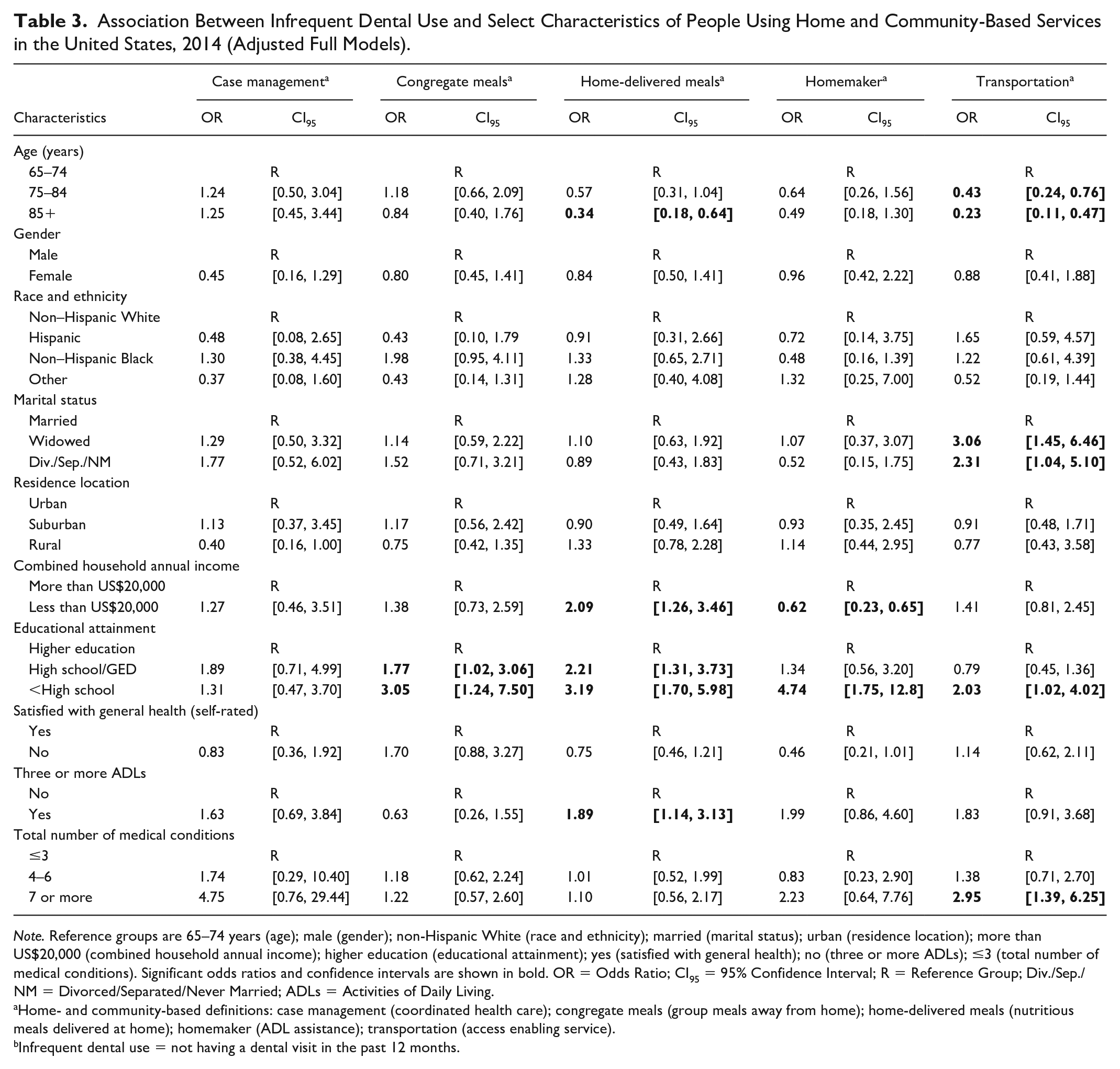
Note. Reference groups are 65–74 years (age); male (gender); non-Hispanic White (race and ethnicity); married (marital status); urban (residence location); more than US$20,000 (combined household annual income); higher education (educational attainment); yes (satisfied with general health); no (three or more ADLs); ≤3 (total number of medical conditions). Significant odds ratios and confidence intervals are shown in bold. OR = Odds Ratio; CI95 = 95% Confidence Interval; R = Reference Group; Div./Sep./NM = Divorced/Separated/Never Married; ADLs = Activities of Daily Living.
Home- and community-based definitions: case management (coordinated health care); congregate meals (group meals away from home); home-delivered meals (nutritious meals delivered at home); homemaker (ADL assistance); transportation (access enabling service).
Infrequent dental use = not having a dental visit in the past 12 months.
Results from multivariate regression modeling producing parsimonious models for the five HCBS are shown in Table 4. Low educational attainment remained associated with infrequent dental use for four of the HCBS (congregate meals, home-delivered meals, homemaker, and transportation). Among persons using case-management services, females (AOR = 0.39, CI95 = [0.18, 0.84]) and those living in rural areas (AOR = 0.38, CI95 = [0.18, 0.79]) were less likely to be infrequent dental users compared to males and participants living in urban areas. However, those with ≥7 medical conditions were more likely to be infrequent dental users compared to those with ≤3 medical conditions (AOR = 3.62, CI95 = [1.24, 10.61]). Persons with ≥7 medical conditions were also more likely to be infrequent dental users if they receive transportation services (AOR = 2.64, CI95 = [1.51, 4.61]). For having difficulty with ≥3 ADLs, those receiving homemaker services were more likely to be infrequent dental users compared to those not having difficulty with ≥3 ADLs (AOR = 2.0, CI95 = [1.06, 3.77]). Among those receiving home-delivered meals, persons with an annual income below US$20,000 were more likely to be infrequent dental users compared to those with an income above US$20,000 (AOR = 1.62, CI95 = [1.04, 2.51]). Again, among home-delivered-meals and transportation participants, people 85 years and older were less likely to be infrequent dental users compared to those 65–74 years old (AOR = 0.43, CI95 = [0.25, 0.74] and AOR = 0.42, CI95 = [0.23, 0.76], respectively). Finally, among congregate-meals group, non-Hispanic Black were more likely to be infrequent dental users compared to non-Hispanic White (AOR = 2.5, CI95 = [1.41, 4.44]).
Association Between Infrequent Dental Use and Select Characteristics of People Using Home and Community-Based Services in the United States, 2014 (Adjusted-Parsimonious Models).
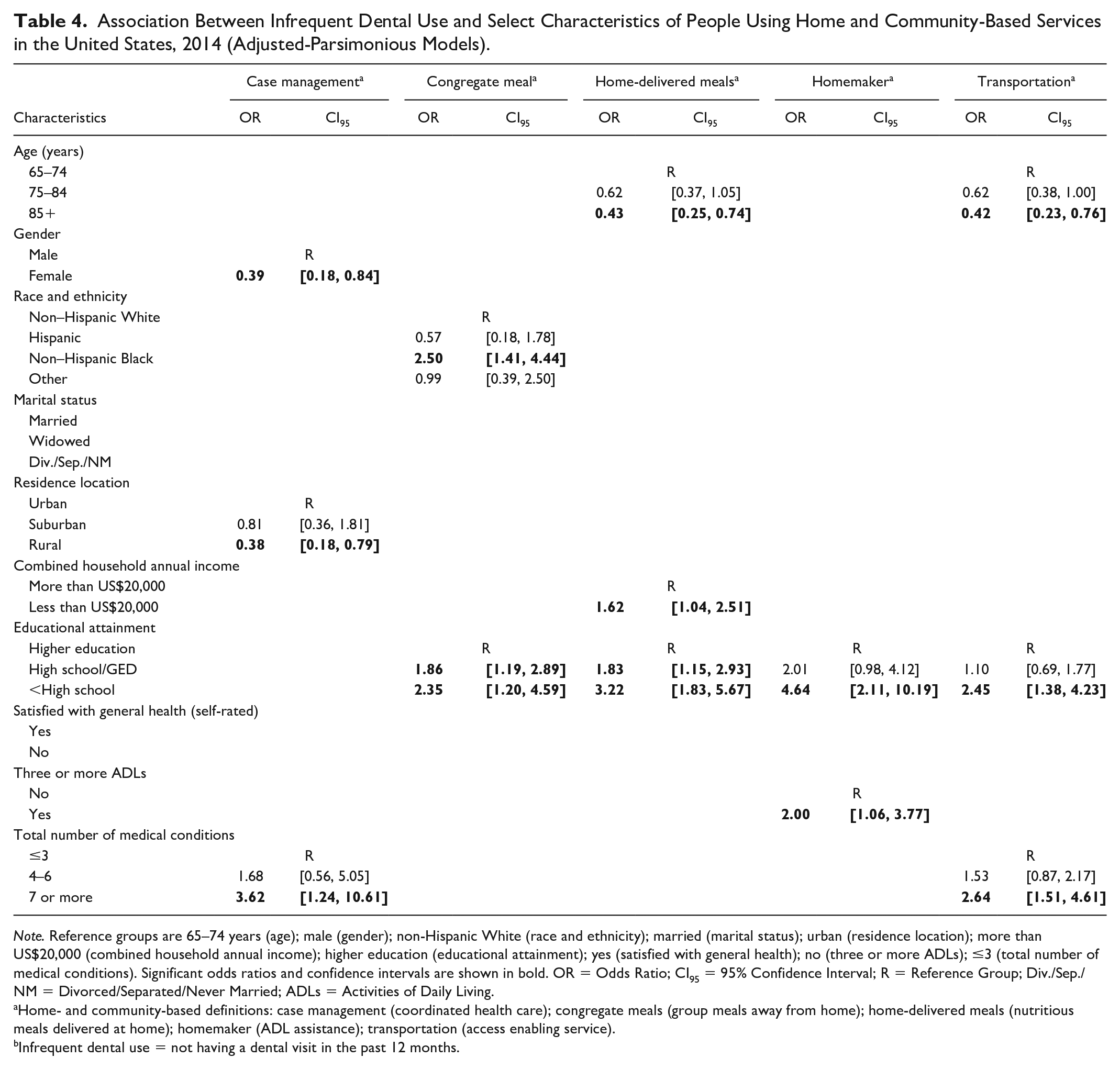
Note. Reference groups are 65–74 years (age); male (gender); non-Hispanic White (race and ethnicity); married (marital status); urban (residence location); more than US$20,000 (combined household annual income); higher education (educational attainment); yes (satisfied with general health); no (three or more ADLs); ≤3 (total number of medical conditions). Significant odds ratios and confidence intervals are shown in bold. OR = Odds Ratio; CI95 = 95% Confidence Interval; R = Reference Group; Div./Sep./NM = Divorced/Separated/Never Married; ADLs = Activities of Daily Living.
Home- and community-based definitions: case management (coordinated health care); congregate meals (group meals away from home); home-delivered meals (nutritious meals delivered at home); homemaker (ADL assistance); transportation (access enabling service).
Infrequent dental use = not having a dental visit in the past 12 months.
Discussion
This study reports the results of the 2014 National Survey of Older Americans Act (NSOAPP), administered to almost 4,000 participants who received HCBS. The analysis describes factors associated with infrequent use of dental services among community-dwelling (i.e., noninstitutionalized) elders participating in ACL-/AOA-funded home and community-based services. Oral conditions and diseases are largely preventable, and regular dental visits at any age have been shown to aid in the prevention of oral and overall health problems (Silva et al., 2013). Dental visits also provide an opportunity for referral and treatment of general health conditions including diabetes and hypertension. Numerous factors can either facilitate or act as barriers to access to care (Dolan et al., 2005). Therefore, it is important to recognize that having a regular source of care such as HCBS can assist older adults to achieve better health outcomes. As each service has a different purpose and focus, ACL/AOA participants often rely on more than one HCBS (Low et al., 2011).
We found that infrequent dental use varied from 41% to 63% based on the type of HCBS used. Alternatively, having a dental visit in the past 12 months differed among the five HCBS studied (37% in case management and home-delivered-meals; 47% among homemaker and transportation services; and 59% among congregate-meals participants). For some groups, this falls short of the Healthy People 2020 goal for the total U.S. population (49%). Having an annual dental visit has been identified as a Leading Health Indicator for Healthy People 2020 due to the importance of regular dental care utilization to maintain oral health and overall wellbeing. Improving access to oral health care for many older adults receiving HCBS is important to support their independence, delay institutionalization, and reduce the burden of health care cost.
Across four of the five HCBS studied, low educational attainment, particularly those not completing high school, was associated with higher likelihood of being an infrequent dental user, a finding in line with previous studies showing that socioeconomic factors such as education level and income are associated with dental visit frequency (Kiyak & Reichmuth, 2005; Silva et al., 2013). Davis et al. found that a lack of education reduced people’s knowledge of the importance of oral self-care and dental visits, and their ability to consistently engage in healthy behaviors and to coordinate health care visits, transportation, and payment for services (Davis & Reisine, 2015). In a white paper published by the Gerontological Society of America, insufficient oral health literacy of older adults and their caregivers was cited as a barrier to improving and maintaining oral health. One of the six solutions discussed for improvement of oral health among older adults was to increase awareness of the economic and humanistic value of better oral health for this population through health promotions and public relations campaigns (The Gerontological Society of America, 2017). Griffin et al. identified that one way to prevent poor oral health among older adults is to promote effective educational interventions to improve oral health knowledge regarding self-care (Griffin et al., 2012).
Recipients of HCBS are a vulnerable population for whom access to oral health services is a challenge. The Institute of Medicine, the National Research Council, and the U.S. Health Resources and Services Administration (HRSA) have issued reports discussing basic approaches to expanding oral health services for vulnerable, underserved, and individuals with disabilities. The reports’ recommendations provide a roadmap supporting the integration of oral health within primary health care and expanding the scope of practice among health professionals to prevent oral disease, increase access to services, and develop and disseminate oral health information (Institute of Medicine & National Research Council, 2011; Tilly, 2016; U.S. Department of Health and Human Services Oral Health Coordinating Committee, 2016). Offering referrals and/or providing preventive services by health professionals is important, but lack of oral health literacy has been identified as a barrier. Many providers, HCBS participants, and people caring for older adults have limited knowledge about oral health. Consequently, additional efforts to disseminate oral health information leading to improve provider, caregiver, and HCBS participants’ oral health literacy are warranted.
Some studies have reported that fewer than half of older adults receive annual dental care (Kakatkar et al., 2011) and that some seek dental care only when pain is present and do not return for follow-up appointments (Gambhir et al., 2013). The 2014 National Health Interview Survey reported that nearly 58% of people aged ≥75 years had a dental visit in the past year (National Center for Health Statistics, 2014). Our study found that participants aged 85 years and older in home-delivered-meals and transportation groups were more likely to have a dental visit in the past year compared to younger participants. Although the reason is not clear, it is possible that these individuals, due to the increasing frailty and older age, are more likely to get help from a family member, caregiver, or case manager to coordinate their health care and more likely to use transportation services provided by a program. According to Ewen et al., given the HCBS instrumental support, individuals who are older or in worse physical health tend to rely more on utilization of HCBS to meet their needs (Ewen et al., 2017).
Congregate-meals participants had the highest prevalence of routine dental users (59%), and as a group, they reported higher income, educational background, and likelihood of general health satisfaction. In addition, participants in the congregate-meals group reported a lower likelihood of having multiple medical conditions or difficulty with ADLs. An Illinois State University report also found that congregate-meals participants tend to have higher education and annual income but rely on this service as a venue to socialize and because illness or frailty prevents them from cooking for themselves (Myers, 2013). Receiving meals in a social group setting could provide a positive motivation that leads congregate-meals participants to seek healthier behaviors including dental visits. Although the reasons for the association between social relationships and health are not completely understood, studies have demonstrated that the association exists even if the social participation is minimal (Myers, 2013).
In contrast to congregate meals, individuals receiving homemaker and case-management services reported the highest rates of having income below US$20,000, general health dissatisfaction, and having difficulty with three or more ADLs. Participants receiving homemaker services tend to be either medically compromised, face physical disabilities and limitations with fewer resources, or need personal care and assistance with ADLs/IADLs (Area Agency on Aging, 2013; North Dakota Department of Human Services, n.d.). Homemaker services allow frail older adults or those with concomitant medical conditions to stay at home and remain more independent by providing necessary personal care. However, homemaker visits could also include additional services that facilitate oral hygiene care and opportunities to improve dental utilization. Effective homemaker services could be part of a strategy to help older adults maintain good oral and general health, prevent emergencies, and delay institutionalization or hospitalization, resulting in improved quality of life and monetary savings to families, government, and health systems (Area Agency on Aging, 2013).
Individuals who receive support through case management must have a needs evaluation, an identified care plan, and a service arrangement (Hammond et al., 2012; Missouri Department of Health and Senior Services, n.d.; Silva et al., 2013). For instance, case management may include a plan for rehabilitation and services necessary to transition from a hospital or assisted living institution to home placement (Hammond et al., 2012; Missouri Department of Health and Senior Services, n.d.). In our study, older adults living in rural areas and receiving case-management services were more likely to be routine dental users by having a dental visit in the last 12 months. This suggests that case management might have a positive effect on dental visit utilization when access to health care is limited. Case managers with knowledge of oral health and preventive measures can assist community-dwelling older adults and caregivers to take preventive actions that could enhance oral and general health (Silva et al., 2013).
Dolan et al. reported that besides education, lack of transportation is a frequent barrier to access dental services (Dolan et al., 2005). Transportation services are designed to enhance opportunities to access medical/dental appointments and other needed social services for those too frail or ill to drive. However, in our study, more than half of participants who received transportation services were infrequent dental users, which indicates that access to transportation services is not enough to improve dental services utilization. A number of studies showed that medical conditions, frailty, limited mobility, and/or the use of a special adaptive device (i.e., wheelchair, scooter) often add a layer of complexity to the existing barriers and restrict the utilization of the available transportation services to access a dental clinic (Davis & Reisine, 2015; Griffin et al., 2012). Furthermore, Rashid-Kandvani et al. (2015) and an issue brief published by the ACL advised states to encourage their public health networks, stakeholders, government entities, and dental professional bodies to improve coordination aimed at expanding the delivery of preventive, educational, and oral health services for older adults, individuals with disabilities, and those who present challenges toward the dental care pathway (i.e., finding a dentist, transportation, building mobility, transfer from van to places) (Rashid-Kandvani et al., 2015; Tilly, 2016).
Finally, 30% of home-delivered meal participants reported having difficulty with 3 or more ADLs, 50% reported not being satisfied with their general health, and 63% reported being an infrequent dental user. These results align with the findings of Thomas and Dosa (2015) as these participants are frequently frail, homebound, or isolated and therefore less likely to prepare their own meals and provide self-care (North Dakota Department of Human Services, n.d.). Home-delivered meal services have shown positive nutritional outcomes among participants (Thomas & Dosa, 2015).
In summary, our results demonstrate that among all HCBS groups, congregate-meals participants had the highest prevalence of routine dental users (59%), which could be due to their better overall health and socioeconomic outcomes. On the other hand, participants of case management and home-delivered meals had the lowest prevalence of routine dental users (37%), possibly because people receiving these services were more likely to be more frail, homebound (Frongillo et al., 2010), or undergoing rehabilitation (Hammond et al., 2012). Even with transportation assistance, mobility restrictions could be a barrier to accessing oral health care.
There are limitations to our study. The NSOAAP is a cross-sectional survey, which does not permit evaluation of causality. In addition, our analysis was constrained due to the limited nature of the demographics, insurance, dentition status, and other data provided by NSOAAP’s questionnaire. Due to participation overlap, we were not able to test for significant differences among HCBS groups. Although self-reported responses offer valuable information regarding health outcomes, these measures are subject to bias based on the respondent’s level of knowledge, perception, and understanding. Finally, our findings describe the characteristics of older adults receiving ACL/AOA HCBS in the United States and cannot be generalized to other populations. Nonetheless, our analysis covers a gap in the literature regarding the factors that influence dental visits among people receiving HCBS.
Conclusion
This study presents the first national estimates of dental visit utilization among NSOAP ACL/AoA HCBS recipients. Among older adults receiving four out of five HCBS services, there was a large disparity in dental visits (routine vs infrequent dental users) between those who did not complete high school compared to those with educational attainment beyond high school. HCBS have been shown to be successful in assisting older adults and people with disabilities to remain at home and age in place; but as the older adult population continues to grow, so will be the demand for health care services. In recognition of the significant changes in the U.S. aging population, promoting collaborative practices among HCBS presents opportunities for integrating oral health into their existing focus and increases dental service utilization toward better patient-centered outcomes. Facilitating oral health care, including oral health education, within AoA programs may be an effective means for improving the oral health of HCBS participants, which can lead to improvements in overall wellbeing of older adults.
Footnotes
Acknowledgements
The authors would like to thank Gabriela Lopez-Mitnik, MS, MPhil (NIH/NIDCR), Alicia Livinski, MPH, MA (NIH/NIH Library), and Karen Sokal-Gutierrez MD, MPH (UC Berkeley-UCSF Clinical Professor) for their statistical, library, and editorial support, respectively.
Author Note
At the time of the study, Dr. Steffany Chamut was a fellow at the National Institute of Dental and Craniofacial Research, National Institutes of Health in Bethesda, MD, and Dr. Elena Fazio was with the Administration for Community Living/Administration on Aging, Department of Health and Human Services in Washington, DC, USA. Margo Adesanya is currently retired from Federal Government (NIH/NIDCR).
Authors’ Contributions
Steffany Chamut, DDS, MPH, made a substantial contribution to the concept and design of the work, analysis and interpretation of data, as well as the drafting of the manuscript.
Shahdokht Boroumand, DMD, MPH, assisted with the concept and design of the work, analysis and interpretation of data, as well as the drafting of the manuscript.
Timothy J. Iafolla, DMD, MPH, assisted with the concept and design of the work, analysis and interpretation of data, as well as the drafting of the manuscript.
Margo Adesanya, DDS, MPH, assisted with the concept and design of the work, interpretation of data, and the review of the manuscript.
Elena M. Fazio, PhD, assisted with the concept and design of the work, as well as the interpretation of data.
Bruce A. Dye, DDS, MPH, assisted with the concept and design of the work, analysis and interpretation of data, as well as the drafting of the manuscript. He supervised the project as well.
Disclaimers
The views stated in this article are those of the authors and do not reflect the policies and beliefs of the U.S. Department of Health and Human Services (HHS), the National Institutes of Health (NIH), the National Institute of Dental and Craniofacial Research (NIDCR), the Administration for Community Living (ACL)/Administration on Aging (AOA), or the U.S. Federal Government.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Fellowship Program in Dental Public Health at the National Institute of Dental and Craniofacial Research, National Institutes of Health, Bethesda, MD, USA. Some authors were paid a salary by their institutions. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. The survey was funded by U.S. Administration for Community Living/Administration on Aging. The Westat Institutional Review Board (IRB) reviewed the materials submitted for Ninth AoA National Survey, Project Number 6198.01. The secondary analysis of data for this manuscript received exemption from the NIH IRB.