
Abstract
A focus of community-based elder abuse response programs (EARP), such as Adult Protective Services, is to reduce the risk of revictimization among substantiated victims. While elder abuse (EA) risk factor research has predominantly focused on understanding the risk of initial EA onset among the general older adult population, understanding of revictimization risk among substantiated victims is weak. This study sought to identify conditions that perpetuate EA among substantiated victims. Data were collected from multiple sources: focus groups with multidisciplinary teams (n = 35), multidisciplinary team case revictimization risk evaluations (n = 10), and reviewing a random sample of case records (n = 250) from a large EARP in New York City. Sixty-two indicators of EA revictimization risk were identified across several ecosystemic levels: individual victim or perpetrator, victim–perpetrator relationship, and surrounding family, home, community, and sociocultural contexts. Findings carry implications for EARP practices to reduce EA recurrence and the development of measures to evaluate EARP intervention.
Background and Objectives
Elder abuse (EA) is a pervasive problem associated with major individual consequences, including shortened survival, and societal costs (Yunus et al., 2019). Approximately 10% of older adults living in the community experience some form of EA each year. EA encompasses emotional/physical/sexual/financial abuse or neglect toward an older adult by a person in a relationship involving an expectation of trust (Pillemer et al., 2016).
Community-based EA is addressed by different types of EA response programs (EARPs), including centralized state/county-administered Adult Protective Services (APS; Administration for Community Living, 2016), decentralized programs embedded within community-based organizations (Rizzo et al., 2015), and multidisciplinary teams (MDTs; Navarro et al., 2015). In epidemiological terms, EARPs would be considered secondary or tertiary prevention—reducing the risk of EA revictimization among older adults who have already been victimized—as opposed to primary prevention that focuses on forestalling the initial onset of EA among the general population of older adults (Porta, 2014).
To date, EA risk factor research has focused largely on risk of initial EA onset (with direct implications for primary prevention), such as general population-based studies aiming to identify factors that predispose EA among older adults (Pillemer et al., 2016). Little research has been conducted to understand the risk of EA revictimization—conditions that maintain or perpetuate EA among victims of substantiated cases. EA revictimization risk factors are central to EARP secondary/tertiary prevention efforts and may diverge from risk factors of initial EA onset. Understanding the nature of revictimization risk would inform EARP practice aimed at reducing EA recurrence. It would also inform efforts to measure the impact of EARP interventions (e.g., to what extent risk of revictimization changes over the intervention).
EA research has used an ecological-systems perspective to understand risk factors. According to the seminal EA Theoretical Risk Framework (National Research Council, 2003), indicators of EA risk are attached to several ecosystemic levels, including the individual older adult and trusted other, older adult–trusted other relationship, social network, and surrounding sociocultural context. The Abuse Intervention Model (AIM) focuses on EA risks related to the vulnerable older adult, the trusted other, and the surrounding context to inform interventions (Mosqueda et al., 2016). Guided by these existing models, this study explored indicators from different levels of ecosystemic influence underlying the risk of EA revictimization.
Method
This study integrated data from three sources to explore indicators of EA revictimization risk.
Data and Analysis
MDT focus groups
Focus groups provide an exploratory mechanism to understand complex phenomena, such as revictimization risk, through collaborative participant synergy (Green & Thorogood, 2004). We conducted focus groups with professionals from two EA MDTs in Manhattan and Brooklyn, NY, respectively. MDTs consisted of EA professionals/specialists from numerous disciplines, including physicians, nurses, social workers, psychiatrists, neuropsychologists, civil attorneys, forensic accountants, and law enforcement. MDTs represented a valuable source of information to inform our understanding about EA revictimization risk from several perspectives. Although MDTs as a form of intervention focus on complex cases, the professionals comprising the MDTs provide frontline work with cases on a daily basis outside of their specific MDT role that represent a wide spectrum of EA complexity. We used a semi-structured, open-ended format to direct the focus group conversation and allow unanticipated themes to emerge (see Supplemental Material for interview questions). Each MDT focus group consisted of 15 to 20 interdisciplinary participants. Focus groups were audio-recorded and transcribed verbatim. Data analysis followed an iterative, constant comparison process that allowed themes to emerge and become reorganized as new information arose (Padgett, 1998). NVivo qualitative analysis software was used to organize the analytic process of identifying, sorting, and clustering key transcript statements into themes related to risk of revictimization. Data coding/analysis was completed by two independent raters (D.B., B.M.F.).
MDT risk evaluation cards
One of the MDTs that participated in focus groups used a process to evaluate the overall level of EA revictimization risk for cases at intake and case closure. For this evaluation process, each MDT member anonymously filled out a card to identify their assessment of the overall level of risk of revictimization (none, low, moderate, high) and documented specific reasons underlying their appraisal of risk. Thus, for each case, 15 to 20 MDT members documented specific indicators of risk of revictimization. At the time of data collection for this study, we accessed risk evaluation cards for 10 cases. Two raters (D.B., B.M.F.) independently analyzed risk evaluation data to identify the risk of revictimization indicators.
EARP case review
The Jewish Association Serving the Aging Legal/Social Work Elder Abuse Program (JASA-LEAP) is the largest EARP in New York City for cognitively intact older adults living in the community. As part of a previous study, 250 random case files from three JASA-LEAP sites were reviewed by two independent raters (D.B., E.C.) to assign each case into a level of revictimization risk (low, moderate, high) at case closure (Burnes et al., 2014). The reasons used to adjudicate cases into varying levels of revictimization risk status were used in this study as a basis to identify indicators of EA revictimization risk. Detailed information on case sample characteristics, study design, and the JASA-LEAP EARP intervention model is available elsewhere (Rizzo et al., 2015).
Drawing from these three data sources, indicators of revictimization risk were identified in an iterative and accumulative manner and integrated into an overall ecosystemic framework using domains adapted from existing models. This study received ethics approval from the University of Toronto.
Results
The ecosystemic framework of indicators of risk of EA revictimization is presented in Figure 1. We identified 62 indicators across four domains (victim, perpetrator, victim–perpetrator relationship, and context). Notably, previous models have described risk of EA onset in relation to a “vulnerable older adult” and “trusted other.” We chose, instead, to use the terms “victim” and “perpetrator,” given that, in revictimization risk, EA has already occurred.
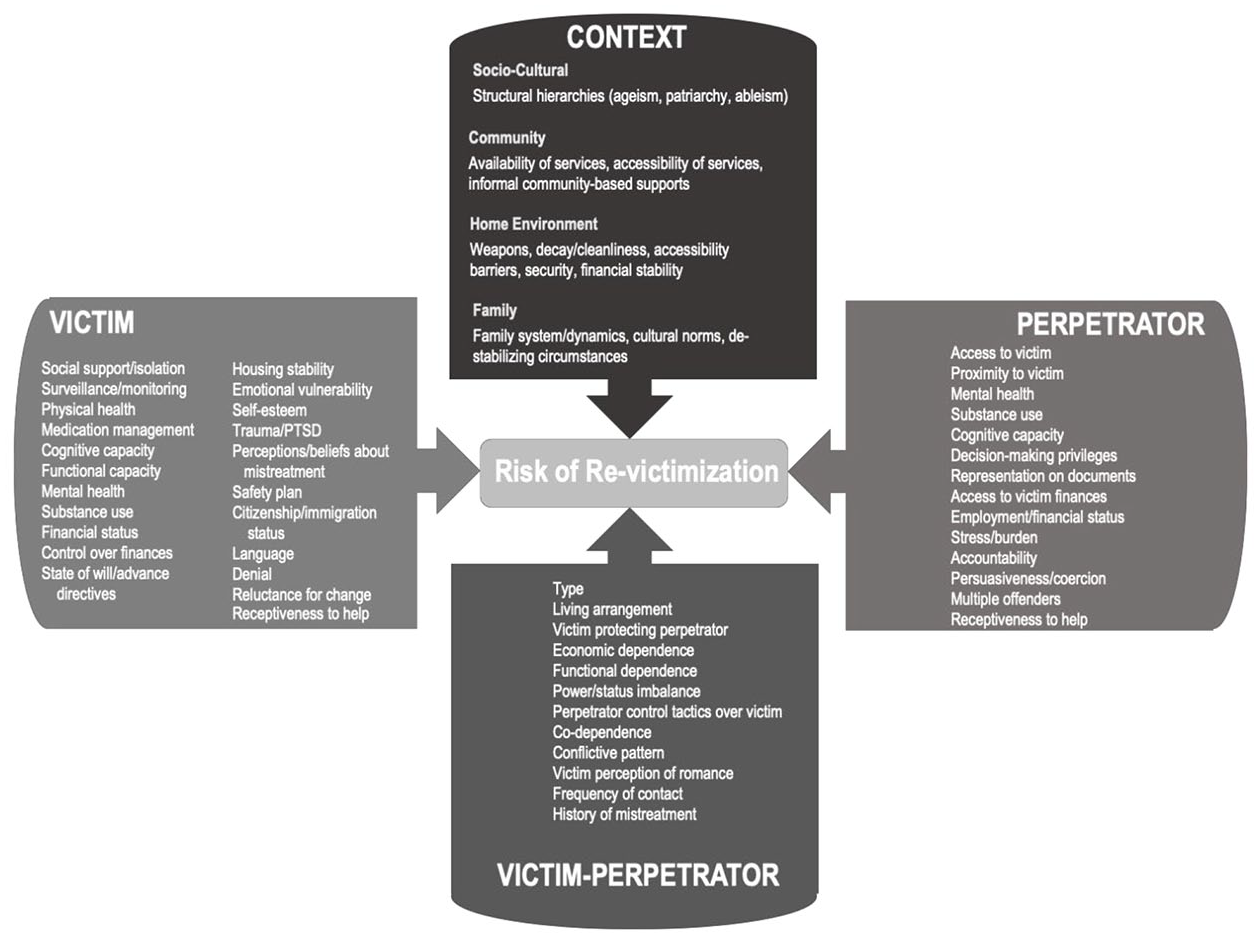
An ecosystemic framework of elder abuse revictimization risk indicators.
Individual-Level Indicators (Victim)
Indicators of revictimization risk attached to the individual victim included low social support; low surveillance/monitoring by others; poor physical health; medication mismanagement; cognitive incapacity; functional incapacity; mental/psychiatric illness; substance use; low control over finances; precarious state of will (e.g., whether will is absent/outdated/comprised); emotional vulnerability related to abuse, such as helplessness, shame, and guilt; low self-esteem; trauma/post-traumatic stress disorder (PTSD); minimizing or denial about the abuse; lack of safety plan; help-seeking barriers (e.g., undocumented citizenship status, language barriers); reluctance/ambivalence about change; and low receptivity to help.
Individual-Level Indicators (Perpetrator)
Perpetrator-oriented indicators of risk of revictimization included access and proximity to victim; mental/psychiatric illness; substance use; cognitive incapacity; having health care proxy, power of attorney, or other decision-making privileges; representation on legal documents; access to victim finances, credit cards, or assets; employment/financial instability; stress/burden; low accountability; persuasiveness/coercion; presence of multiple offenders; and low receptivity to help.
Victim–Perpetrator Relationship
At the level of the victim–perpetrator relationship, indicators of revictimization risk included relationship type (e.g., offspring, spouse); shared living; frequency of contact; victim protecting perpetrator (e.g., excusing or minimizing perpetrator actions); economic/resource dependence (in either relational direction); functional dependence (in either relational direction); perpetrator power/status advantage over victim (e.g., age, ability, gender); perpetrator control tactics over victim (e.g., blocking support services or social contact, instilling a fear of retaliation); and victim perceptions of romantic relationship with perpetrator.
Context
We identified contextual factors in four categories (sociocultural, community, home environment, family) as indicators of EA revictimization risk. At a sociocultural level, unequal social arrangements (e.g., ageism, patriarchy, able-body centeredness) were seen as reinforcing or facilitating revictimization risk. At the level of community, risk indicators included the absence of EA-related support services or lack of accessibility/connectedness to services (e.g., distance, transportation). Revictimization risk indicators attached to the home environment included presence of weapons; decay or uncleanliness; accessibility barriers (e.g., no escape route); and security status (e.g., locks, security system). At the family level, indicators of revictimization risk were related to family system dynamics (e.g., mistreatment normalization, implicit hierarchies, intergenerational patterns of violence, enablers) and the presence of destabilizing family circumstances (e.g., death, job loss, incarceration/release).
Discussion and Implications
This study explored indicators EA revictimization risk and proposed an ecosystemic model to assist EAPRs. Some indicators of revictimization risk found in this study were similar to “primary” EA risk factors previously identified as predisposing initial EA onset among older adults in the general population (e.g., older adult cognitive/health/functional impairments and social support/embeddedness; perpetrator mental illness, substance abuse, and dependency; and a shared living arrangement) (Pillemer et al., 2016). Overlap between revictimization and initial onset victimization risk factors is unsurprising, as the circumstances that predispose EA onset may remain active after the problem has begun. However, using a different and highly relevant conceptual lens for EARP clinical practice, risk of revictimization is also driven by perpetuating factors—those factors that maintain the problem and exist once the problem has started (Regehr & Glancy, 2010). These perpetuating EA factors include the victim’s perception of the mistreatment problem (e.g., denial, minimizing), extent to which the victim protects/excuses the perpetrator, victim and perpetrator receptiveness to help or readiness for change, barriers to utilization of EARP services (e.g., language, citizenship status, transportation), and control tactics used by the perpetrator to silence the victim or discourage them from seeking help (Acierno et al., 2020). Perpetuating factors are critical to our understanding of revictimization risk. EARP intervention practices and evaluation strategies should consider risk factors that both predispose and perpetuate the problem.
Findings from this study carry implications for secondary/tertiary EA prevention interventions, such as APS, MDTs, or other community-based programs that respond to substantiated EA cases, as well as EA resource centers that respond to allegations (Weissberger et al., 2019). Adding to existing practice tools, such as “TRIO” or “EARAE,” which link EA risk factors to interventions (Dauenhauer et al., 2019; Sommerfeld et al., 2014), the model presented in this study could help guide EARP practitioners to ensure that interventions are targeting all relevant aspects of revictimization risk. Supports can be implemented to mitigate risk attached to nonmodifiable or deteriorating factors. Alternatively, direct interventions may be necessary to alter risk attached to improvable/modifiable factors.
Study findings also carry implications for measuring the impact of EARP interventions. A central EARP intervention objective is to reduce the risk of revictimization (Administration for Community Living, 2016), yet a measure of revictimization risk status does not exist. EARP evaluation research has typically used subjective measurement processes to measure revictimization risk status (Burnes et al., 2014). Risk indicators found in this study could be used as a basis to construct a tool that measures revictimization risk status. We included a broad range of factors in this initial study so that future research may use systematic methods to identify the most important ones and help define or specify specific items. Psychometric analysis, including factor analysis, would be a critical preliminary step in tool development to help reduce the total number of items. Such a tool could be administered at intake and case closure to assess the extent to which revictimization risk has been alleviated (or not) over the course of EARP intervention. It could also be used to guide decisions about case closure.
This study contains limitations. Although appropriate for an exploratory study, our findings are based on qualitative and case review data from an urban context. Therefore, our results may not be generalizable beyond an urban context and are subject to the limitations of extracting data from preexisting records. As initial exploratory research on the topic, this study presents a model of EA revictimization based on EA as a global phenomenon. However, given the clinical and substantive differences across EA subtypes, it is likely that revictimization risk profiles vary across them, and further research is required to differentiate which factors are most relevant to specific subtypes. Despite these limitations, this study highlights the importance of distinguishing between risk of initial EA onset and risk of revictimization and provides the first systematic exploration of revictimization risk indicators to help inform practice and evaluation in EARP settings.
Supplemental Material
Supplemental_Material – Supplemental material for Exploring Risk of Elder Abuse Revictimization: Development of a Model to Inform Community Response Interventions
Supplemental material, Supplemental_Material for Exploring Risk of Elder Abuse Revictimization: Development of a Model to Inform Community Response Interventions by David Burnes, Alyssa Elman, Beatrice Marie Feir, Victoria Rizzo, Amy Chalfy, Erin Courtney, Risa Breckman, Mark S. Lachs and Tony Rosen in Journal of Applied Gerontology
Footnotes
Acknowledgements
The authors thank the following organizations and partners for their involvement in this study: New York City Elder Abuse Center Manhattan and Brooklyn Multidisciplinary Teams and Jewish Association Serving the Aging (JASA) Legal Social Work Elder Abuse Program (LEAP).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research Ethics
The Health Sciences Research Ethics Board at the University of Toronto provided approval for this study (Protocol ID 30559).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.