
Abstract
Replications of evidence-based dementia care receiver–caregiver dyad interventions in the community are scarce. We aimed to assess the effectiveness of the Kansas City implementation of Reducing Disability in Alzheimer’s Disease (RDAD) among a convenience sample of dyads with moderate dementia, which addressed needs identified by nine participating community agencies. We hypothesized that dyads’ mental health and physical activity outcomes would improve from baseline to end-of-treatment. The final analytic sample included 66 dyads. Outcomes improved (p < .01) from pre- to post-intervention: behavioral symptom severity (range 0–36) decreased from 11.3 to 8.6, physical activity increased from 125.0 to 190.0 min/week, caregiver unmet needs (range 0–34) decreased from 10.6 to 5.6, caregiver behavioral symptom distress (0–60) decreased from 15.5 to 10.4, and caregiver strain (0–26) decreased from 11.1 to 9.7. This adapted implementation of RDAD leads to clinically meaningful improvements and might inform scaling-up.
Introduction
It is well-known that the U.S. population is getting older. By 2034, there will be more adults of age above 65 years than children (Vespa, 2018). Older adults and aging policies have emphasized “aging in place” in their own homes and communities (Altshuler & Schimmel, 2010; Oberlink, 2014). With this shift in living situations, the U.S.’s current support infrastructure will face unprecedented challenges providing the in-home services and infrastructure that the aging population demands. These challenges especially apply to the growing population of persons with dementia (PWDs), which doubles every 5 years beyond the age of 65 years (Alzheimer’s Association, 2015). Dementia presents additional barriers to providing in-home services due to the increased need for behavioral management and functional support for activities of daily living such as cooking, dressing, and hygiene (Riley et al., 2014).
As outlined in the National Plan to Address Alzheimer’s “enabling family caregivers to continue to provide care while maintaining their own health and well-being” is a primary need for communities and the nation. Achieving this support requires identifying unmet needs and matching these needs with best practices and evidence-based interventions through a broad dementia-capable system. Specifically, the plan calls for caregivers to be “linked to interventions shown to decrease burden and depression among caregivers and enhance the care received by PWDs.”
Behavioral challenges and the caregivers’ own health are two of the primary reasons for nursing home placement (Buhr et al., 2006). It has been well established that behavioral challenges are most often associated with care recipient and caregiver dyad factors such as lack of activity, depression, and anxiety (Okura et al., 2010; Ornstein & Gaugler, 2012). Compounding the problem, the caregiver/recipient dyad tends to become increasingly isolated through the course of the illness (Buhr et al., 2006; Moyle et al., 2011). Fatigue, depression, and an unwillingness to expose deficits to a wider community separate them from vital social support (Moyle et al., 2011).
Numerous interventions to improve quality of life have been tested in the home setting for dyads (Dawson et al., 2015; Gitlin et al., 2012, 2015). However, despite the strong evidence base for interventions to improve the quality of life of PWDs and their caregivers, few interventions have been implemented in the community (Gitlin et al., 2012, 2015). This limitation hinders the translation from research to practice. In fact, according to the National Institutes of Health Intervention Development Model, the intervention development process is incomplete until it is optimally efficacious and implementable with fidelity by practitioners in the community (Onken et al., 2014).
Among the most successful has been the Reducing Disability in Alzheimer’s disease (RDAD; Teri et al., 1998). RDAD is a dyad home-based multicomponent intervention that focuses on exercise for PWDs and coping with behavioral symptoms for caregivers. The original goal of RDAD was to decrease behavioral and physical outcomes among PWDs and delay their institutionalization. RDAD includes 12 modules on behavior management training and exercise instruction. Behavior management instruction focuses on the “ABCs” of problem behaviors, Antecedents, Behaviors, Consequences, as well as communication skills, pleasurable events and realistic expectations. Exercises include strength, balance, endurance, and flexibility. The original dose was comprised of 1-hr sessions over 3 months, weekly or biweekly, depending on the stage of the intervention. Caregivers are instructed to keep a log with the exercise sessions completed without the instructor and to keep a behavior diary. Caregivers are also asked to complete other information that is useful for the sessions, including a problem-solving form, the Pleasant Events Schedule and a home safety checklist. The RDAD program initially demonstrated benefits among PWDs for depression and increased physical activity and function. Subsequent replication at the state-wide level yielded evidence of the scalability of the program in a less research-controlled, more diverse, community environment, and effectiveness in reducing caregiver strain and unmet needs (Menne et al., 2014).
In 2016, two research centers organized a meeting with leaders in aging and disability in the Kansas City community (“the Collaborative”) to discuss potential collaborations. The Collaborative was comprised of the two research centers plus nine community-serving agencies including a medical hospital, a dementia organization, two Area Agencies on Aging, two organizations serving individuals with disabilities, two social services organizations, and a community clinic. The research centers administered the Community-Based Organizations Dementia Capable Quality Assurance Assessment Tool (National Alzheimer’s and Dementia Resource Center, 2020) to each leader individually. Those answers were later shared with the broader group during a second meeting for further discussion. The survey identified that while most community partners reported providing specialized services for PWDs and their caregivers, there was an additional desire for evidence-informed care programs that could be deployed across organizations to leverage training efficiency. The Collaborative identified the RDAD as a potential intervention. However, despite the existence of a previous community translation of RDAD, the group identified three major changes to implement RDAD in Kansas City. Changes included (a) not having to rely solely on licensed clinicians given the agencies’ shortages, (b) need for greater flexibility in delivery of the content to increase efficiency, and (c) not having to depend on interventionists to deliver exercise education, since previous work shows they do not feel comfortable doing so (Menne et al., 2014). We aimed to assess the effectiveness of the Kansas City RDAD implementation (RDAD-KC), which addressed these changes. We hypothesized that dyads’ mental health and physical activity outcomes would improve from baseline to end-of-treatment. We also aimed to assess potential mechanisms by which RDAD-KC improved behavioral outcomes among dyads, including physical activity change, length of the intervention and number of completed sessions and modules.
Method
Study Design and Sample
This pre–post intervention assessment is a secondary analysis of an in-home dementia support services quality improvement project conducted among a collaborative of nine community agencies. Agencies administered RDAD-KC to a convenience sample of dyads they recruited in their service areas. De-identified data were obtained from the partner agencies who agreed to enroll dyads. Dyads’ eligibility criteria included: living in the community, having moderate severity of Alzheimer’s disease and other dementias (Stage 5 and 6 on the Global Deterioration Scale) (Reisberg et al., 1982), not having activity restrictions by a physician, being able to walk across a room in their home with or without an assistive device and having a 2.4 m2 space free of obstacles in which to exercise. Caregivers who did not meet the physical requirements could recruit an “Exercise Buddy” to assist with that component of the program. The final analytic sample included those eligible for the intervention, who had a family caregiver, had no intellectual disability and completed nine of 12 modules (>75%) of the intervention. Among the 157 screened dyads, 47 were excluded from the final analytic sample due to intellectual or developmental disability (an alternative diagnosis for the program). The analysis also excluded three dyads that included formal caregivers and other three in which the relationship between the caregiver and PWD was not defined. Among the remaining 104 dyads, 38 did not complete at least nine RDAD modules and were excluded from the analysis. Therefore, the final analytic sample included 66 dyads.
Data Source
The Collaborative created a shared data collection workbook that included the necessary pre-and post-intervention outcome measures, basic demographics, compliance work forms from the original RDAD, and agency-modifiable consent, physician notification, and technology agreement. Each agency was encouraged to adapt these documents to their own needs and agency policies. Once client dyads completed their participation in the RDAD-KC program, de-identified data were transmitted to the designated Project Evaluator. The project was determined to be secondary data analysis by the Institutional Review Board of the Project Evaluator site, because no identifiable information linked to the outcomes was transmitted outside of the agencies that delivered the intervention, and the outcomes were collected as part of the service provided to the community under the cooperative funding agreement.
Intervention Translation
Changes needed to implement RDAD in Kansas City were addressed in the following way. First, to address the need for greater flexibility in content delivery, the Collaborative elected to deploy the modules in the order that best fit the dyadic situation, needs, and time available. For example, all 12 modules could be delivered in two or 20 different sessions. Second, to address the dependence on the interventionist to deliver the exercise education, an academic team with exercise delivery experience was recruited to create prerecorded exercise educational videos specific to the original RDAD program that could be viewed via tablet devices (Kindle Fire™; Amazon.com, Inc., Seattle, WA, USA) provided to each dyad during the intervention. Four prerecorded instructional videos that covered the first four behavioral modules (introduction to the program, strengthening exercises, balance exercises, and endurance and flexibility) were created for dyads to view and repeat on their own. Dyads were encouraged to call the exercise interventionist each week during the first 4 weeks of the intervention to receive support, problem solve any barriers to the exercises, and review possible exercise modifications. The team was also available for phone consultation throughout the remainder of the dyads’ time in the program, up to 12 weeks. The team was composed of two individuals with a Bachelor’s in Exercise Science or equivalent, a clinical license in Occupational Therapy, or an American College of Sports Medicine certification related to exercise prescription or adaptive physical activity. Third, to address the dependence on licensed clinicians to deliver the intervention, community health workers and other experienced individuals were trained to deliver the intervention as long as they had a bachelor’s degree, at least 100 hr in geriatric experience and dementia training via the Alzheimer’s Association, Health Resources and Services Administration (HRSA) Dementia Training Curriculum, or National Task Group (NTG) Dementia Capable Care Training. On average, each agency employed 0.75 Full-Time Equivalent (FTE) RDAD-KC interventionists per year.
The content of the modules was consistent with prior implementations. The original RDAD manual was employed, including interventionist materials and caregiver handouts. To incorporate current dementia care and research, the original RDAD education workbook was replaced with the Alzheimer’s Association publication “Basics of Dementia Care.” Each of the 12 modules included both behavior management training and exercise instruction. Behavior management instruction focused on the “ABCs” of problem behaviors: Antecedents, Behaviors, Consequences, as well as pleasurable events: identifying activities the PWDs would like to do and simplifying them so that they can enjoy them. Exercise training encouraged dyads to independently engage in 30 min of exercise most days of the week.
Outcome Measures
The Collaborative collectively worked with the funding agency to identify outcomes that were specific to caregivers but were broadly implementable among the various workflows of the partners. Six caregiver-administered outcomes (three caregivers and three PWD-related) were identified as consensus measures that were already being implemented by the partner agencies or could be easily integrated into their workflow. Instruments were selected to measure relevant PWD or caregiver outcomes, be brief, not require extensive staff training or clinical expertise to use and be freely available. All except the physical activity and sedentary behavior instruments have been validated previously through research.
Caregiver-related outcomes
Unmet needs (Measure of Unmet Needs)
The Measure of Unmet Needs (Gaugler et al., 2004) is a validated 24-item survey for caregivers (Thornton & Travis, 2003) that requires “Yes” = 1 or “No” = 0 answers regarding additional assistance with categories such as activities of daily living, dementia symptoms, and social support. Outcomes include a summary score of the 24 items and summary scores of each subscale. Psychometric properties include good to excellent internal consistency in all subscales (α =0.77–0.85), and associations with subjective stress in a variety of contexts (Gaugler et al., 2004).
Caregiver strain (Modified Caregiver Strain Index)
The Modified Caregiver Strain Index (Thornton & Travis, 2003) is a validated 13-item screener for caregiver strain after the hospital discharge of an older adult family member. For each of the items, the caregiver can respond either no (0), yes sometimes (1), or yes on a regular basis (2). Outcomes include an overall summary score as well as four factors informed by a previous factor analysis: Inconvenience, Adjustment, Upsetting and Work adjustments (Rubio et al., 1999). Psychometric properties of the overall score include an internal consistency of α = 0.90, a 2-week test–retest reliability is 0.88 and correlations with cognitive and physical functioning among other variables (Thornton & Travis, 2003).
Behavioral symptom–related distress (Neuropsychiatric Inventory Questionnaire [NPI-Q])
NPI-Q (Kaufer et al., 2000) is a validated clinical instrument for evaluating psychopathology in dementia. If any of the 12 neuropsychiatric symptoms is present, caregivers rate their own distress on a 6-point scale (not distressing at all-extreme or very severe distress). For example, if the caregiver responds yes to “Does the PWD seem sad or say that s/he is depressed?,” the following question would be: “Rate the distress you experience due to that symptom.” An overall distress summary score is calculated by adding the distress scores of all items. Psychometric properties include a 7-hr test–retest correlation of 0.94, an inter-scale correlation of 0.92 with the original longer version of the instrument, inter-item correlations of 0.71–0.97, and correlations with cognitive function (Kaufer et al., 2000).
PWD-related outcomes
Behavioral symptom–related severity (NPI-Q)
If any of the 12 neuropsychiatric symptoms is present, caregivers rate the level of severity for the PWDs on a 3-point scale (mild–severe) (Kaufer et al., 2000). For example, if the caregiver responds yes to “Is the PWD resistive to help from others at times, or hard to handle?,” the following question would follow: “Rate the severity of the symptom.” An overall severity summary score is calculated by adding the severity scores of all items. Outcomes also include summary scores of two factors informed by a previous factor analysis: Negative/oppositional and Anxiety/restlessness (Travis Seidl & Massman, 2016). Psychometric properties include a 7-hr test–retest correlation of 0.80, an inter-scale correlation of 0.91 with the original longer version of the instrument, inter-item correlations of 0.71–0.93, and correlations with cognitive function (Kaufer et al., 2000).
Sedentary behavior
Interventionists asked about the number of days the PWDs spent either sitting or lying down in the last week. This rating was developed by the study team and consisted of subjective caregiver responses.
Physical activity
Interventionists asked about the number of minutes the PWDs were physically active (including walking and cycling but excluding wandering or pacing) during the previous week. This rating was developed by the study team.
Statistical Analyses
Descriptive statistics were calculated for baseline charac-teristics.
Preliminary analysis
The sedentary behavior and physical activity outcomes were developed by the study team. For this reason, to provide evidence of their validity, we assessed their baseline correlations with each other and with the other outcomes in our current sample of 104 participants who enrolled in RDAD-KC (whether they completed it or not).
Effectiveness analysis
Since the distribution of overall scores of all caregiver outcomes, behavioral symptom distress subscales and behavioral symptom severity of the PWDs was normal, we used paired-samples t tests to assess their pre-post-intervention change. The distribution of unmet needs subscales and caregiver strain subscales as well as physical activity and sedentary behavior was not normal. Therefore, we analyzed the change in these variables using paired samples Wilcoxon for all variables except for the “Work adjustments” subscale of the Caregiver Strain Index, for which we used a McNemar test due to its binary distribution.
Mechanistic analysis
Given the normal distribution of the change in all overall outcome scores, we calculated Pearson correlations to analyze between-outcome associations. The number of completed RDAD sessions, modules and length of the intervention in days were all positively skewed. For this reason, we analyzed their association with change in overall outcome scores using Spearman correlations. All the change in overall outcome scores were calculated by subtracting raw scores at follow-up minus baseline.
We used SPSS v20.0 (IBM Corporation, Armonk, NY, USA) for all data analyses and a significance of p < 0.05 (IBM Corporation, 2013).
Results
There was some evidence of the validity of the outcomes developed by the study team, sedentary behavior and physical activity. Sedentary behavior was negatively correlated with minutes of physical activity at baseline (r = −0.338) and positively correlated with baseline levels of unmet needs (r = 0.268) and caregiver distress (r = 0.221; p < 0.05). Table 1 shows the participants’ characteristics at baseline. PWDs who completed at least nine modules were more likely to be women than noncompleters (66.6% vs. 36.8%, p < 0.05) and were less likely to live alone (7.0% vs. 24.3%, p < 0.05). Caregivers who completed at least nine modules were less likely to be women than noncompleters (58.5% vs. 78.4%, p < 0.05). Baseline clinical variables did not differ between completers and noncompleters (p > 0.05).
Participant Characteristics at Baseline.
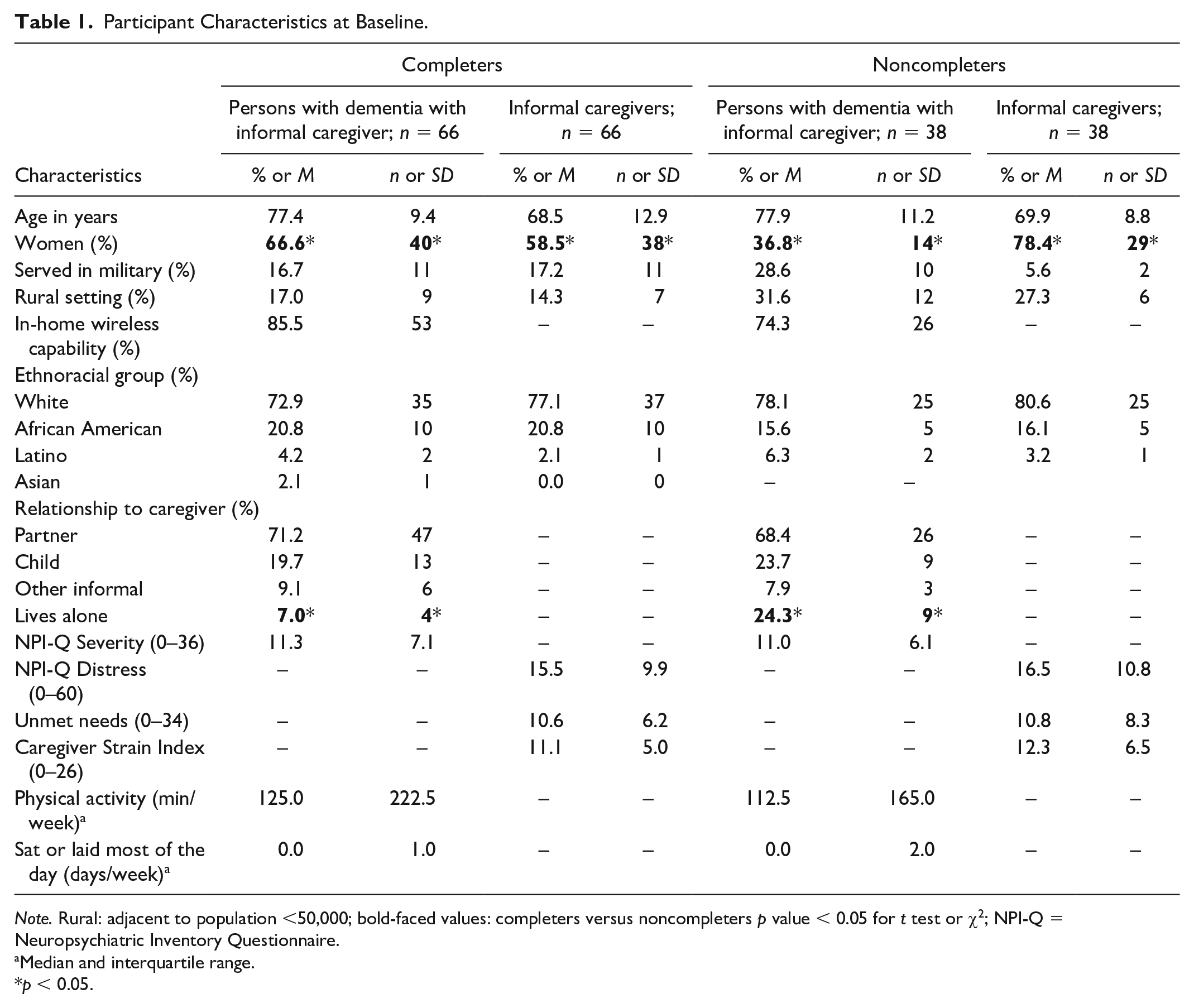
Note. Rural: adjacent to population <50,000; bold-faced values: completers versus noncompleters p value < 0.05 for t test or χ2; NPI-Q = Neuropsychiatric Inventory Questionnaire.
Median and interquartile range.
p < 0.05.
The final analytic sample included 66 dyads. PWDs’ mean age was 77.4 years and ranged from 52 to 95. Among the PWDs, 16.7% were veterans, 17.0% lived in rural areas, and 85.5% had in-home Wi-Fi. PWDs mostly identified as non-Latino White (72.9%) or non-Latino African American (19.7%), and their caregiver was usually their partner (71.2%) or their child (19.7%). Caregivers’ mean age was 68.5 years and ranged from 33 to 90. Among the caregivers, 17.2% were veterans and 14.7% lived in rural areas. Caregivers mostly identified as non-Latino White (77.1%) or non-Latino African American (20.8%). Dyads completed a median of six sessions (minimum 3, maximum 20), 49.9% completed the 12 modules and the median number of days from the first to the last RDAD session was 70 (minimum 28, maximum 219). As a reminder, dyads in the final analytic sample had to complete nine of 12 modules, but the number of sessions needed to complete these modules was flexible.
Table 2 shows the effectiveness of RDAD-KC on PWDs’ behavioral symptom severity, physical activity, and sedentary behavior. The overall mean of PWDs’ behavioral symptom severity, as rated by the caregiver in the NPI-Q, decreased from 11.3 to 8.6 (p < 0.001) as did the NPI-Q negative/oppositional behavior (6.0–4.7, p < 0.01) and anxiety/restlessness subscales (4.1–3.0, p < 0.001). The median number of minutes per week of physical activity increased from 125.0 to 190.0 (p < 0.01) but the median number of days per week spent sitting or lying was zero at baseline and did not change significantly at follow-up.
Effectiveness: Change in Means From Baseline to Follow-Up for Persons With Dementia Outcomes Among Completers.
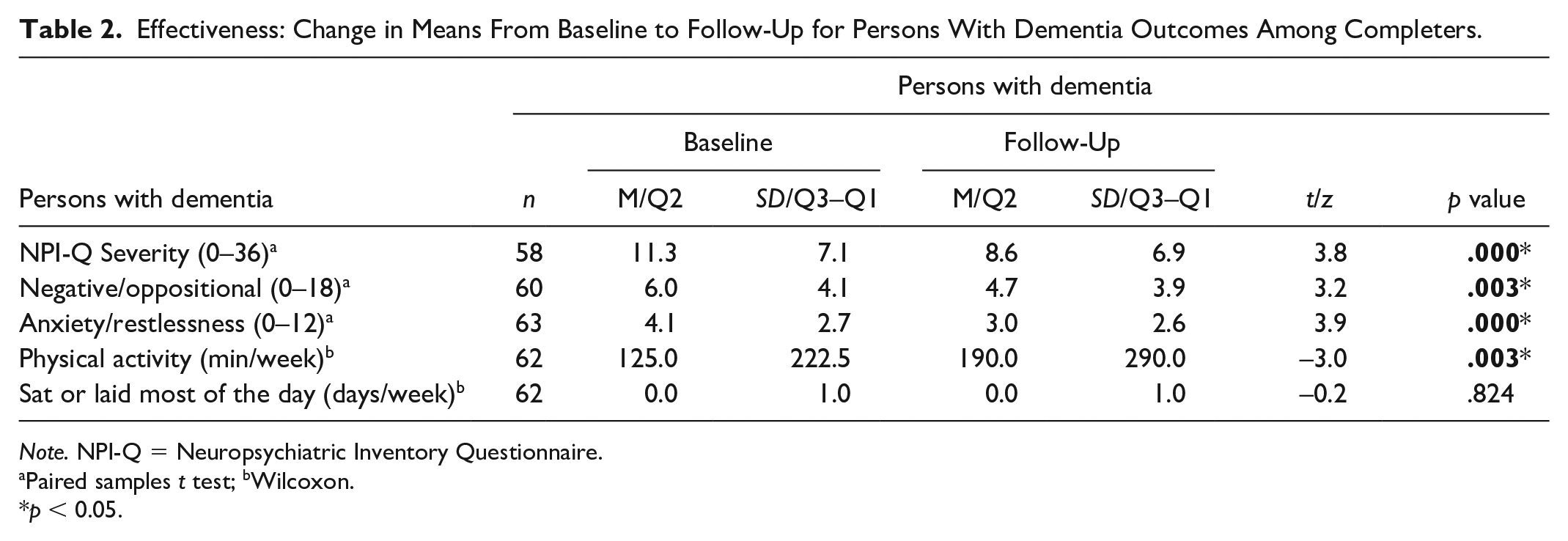
Note. NPI-Q = Neuropsychiatric Inventory Questionnaire.
Paired samples t test; bWilcoxon.
p < 0.05.
Table 3 shows the effectiveness of RDAD-KC on caregiver unmet needs, behavioral symptom–related distress and strain. The mean number of unmet needs decreased from 10.6 at baseline to 5.6 at follow-up (p < 0.001). The median number of all unmet need subscales also decreased statistically from baseline to follow-up (p < 0.05). The overall mean of caregiver distress associated with behavioral symptoms, as rated in the NPI-Q, decreased from 15.5 to 10.4 (p < 0.001) as did the overall caregiver strain, which decreased from 11.1 to 9.7 (p < 0.010). The “upsetting” subscale was the only caregiver strain subscale that decreased statistically (p < 0.01). No correlation between change in physical activity of the PWDs and overall outcomes (behavioral symptom severity and distress, unmet needs or caregiver strain) was statistically significant (Table 4). Change in unmet needs was the only outcome that was correlated with change in sedentary behavior (r = 0.469; p < 0.05). Change in caregiver strain was statistically correlated with change in caregiver unmet needs (r = 0.450), change in distress related to behavioral symptoms (r = 0.425), and change in severity of behavioral symptoms (r = 0.438; p < 0.05 for all mentioned correlations). Change in caregiver distress related to behavioral symptoms was also correlated with change in severity of behavioral symptoms (r = 0.851; p < 0.05). The number of days from baseline to end-of-treatment was correlated with the number of sessions (r = 0.634) and number of modules completed (r = 0.490; p < 0.05). The only outcome statistically significantly associated with any of these process variables was the number of RDAD sessions, which was correlated with the change in unmet needs (r = -0.325; p < 0.05).
Effectiveness: Change in Mean Scores From Baseline to Follow-Up for Caregiver Outcomes Among Completers.
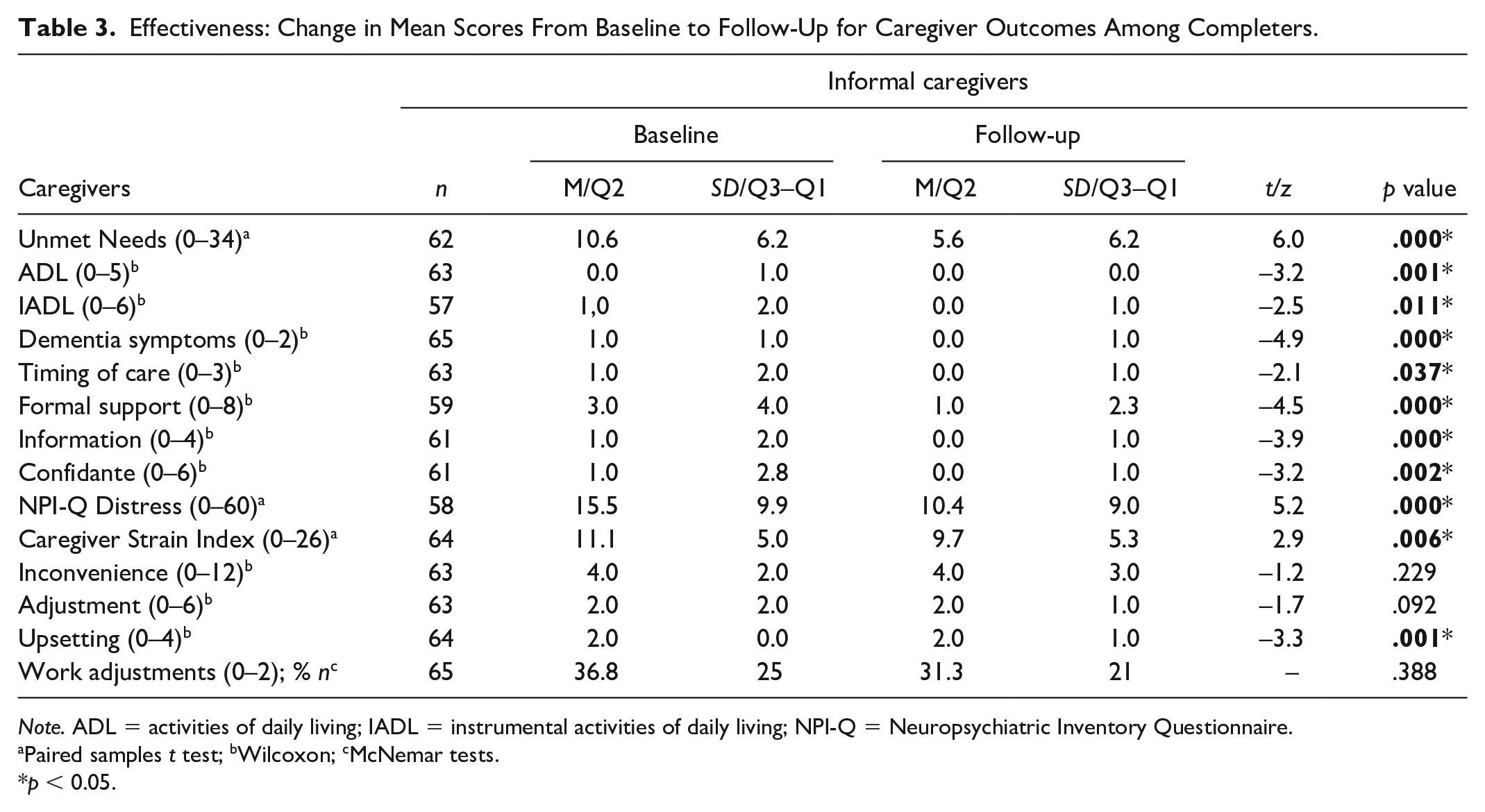
Note. ADL = activities of daily living; IADL = instrumental activities of daily living; NPI-Q = Neuropsychiatric Inventory Questionnaire.
Paired samples t test; bWilcoxon; cMcNemar tests.
p < 0.05.
Mechanistic Analysis: Between-Outcome Correlations and Correlations Between Intervention Implementation Outcomes and Effectiveness Outcomes.
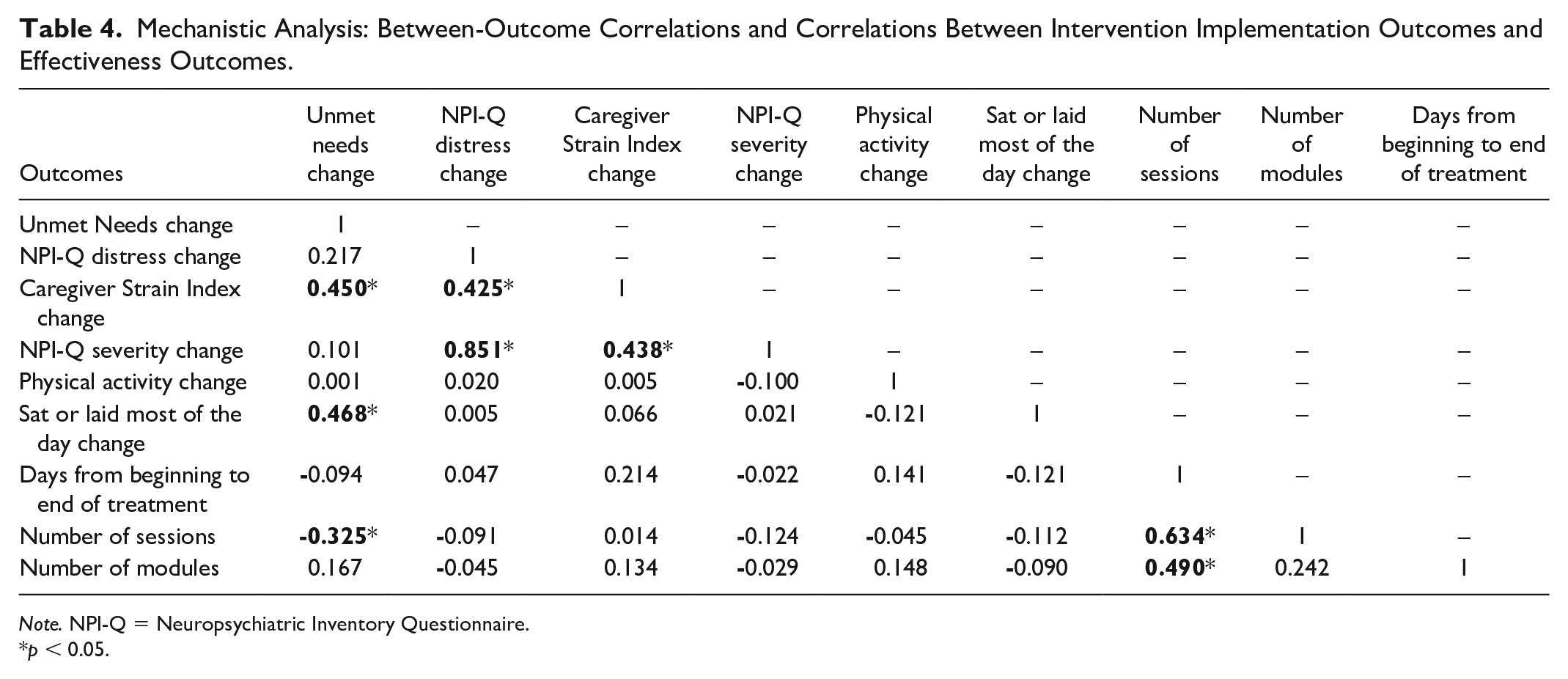
Note. NPI-Q = Neuropsychiatric Inventory Questionnaire.
p < 0.05.
Discussion
The U.S. government has identified caregiver support and dementia-capable care among service-providing agencies as critical needs (U.S. Department of Health & Human Services, 2015). To address these needs in Kansas City, a Collaborative of nine community agencies with expertise in aging and disability selected and modified the proven RDAD intervention for semi-standardized training and implementation across its agencies. The agencies found that the RDAD-KC improved caregiver unmet needs, behavioral symptom distress and strain as well as the PWDs’ behavioral symptom severity and their level of physical activity. It is important to note that these improvements are taking place in the moderate stage of dementia, a time when behavioral symptoms and challenges faced by caregivers, usually begin to escalate. In addition, this implementation showed that the more RDAD-KC sessions that were attended, the more caregiver unmet needs were addressed. These results, overall, demonstrate the effectiveness of scaling up the RDAD intervention for targeting outcomes in care for persons with moderate dementia and their caregivers in the Collaborative service region.
To our knowledge meaningful clinical differences in the “Measure of Unmet Needs” and the “Modified Caregiver Strain Index” have not been established. However, our analyses showed a 47% decrease in the number of unmet caregiver needs, suggesting that the RDAD-KC program, interaction with supports in the home and tele-exercise counseling improved access to resources. Similarly, caregivers reported a 12.6% reduction in feelings of strain. These results are in line with a previous community implementation of RDAD, which led to comparable improvement in unmet needs and strain (Menne et al., 2014). Differences in neuropsychiatric symptom severity and distress scales suggest that RDAD-KC meaningfully reduced behavioral symptoms. NPI-Q severity was reduced by 2.7, close to the 2.77 points reported to be a minimal clinically significant difference (Mao et al., 2015). The NPI-Q distress score, related to the amount of distress the caregiver experiences, was reduced by 5.1 points, exceeding the reported minimal clinically significant difference of 3.1 (Mao et al., 2015). To our knowledge, this is the first RDAD community implementation to assess behavioral symptoms and PWD outcomes in general. RDAD-KC has led to comparable improvements in similar outcomes than the original study, providing evidence that the community translation maintains the intervention’s effect (Teri et al., 2003).
RDAD-KC PWDs increased their average number of minutes of physical activity from baseline to follow-up, reaching levels recommended by the World Health Organization for older adults (World Health Organization, 2020). These findings are important because physical activity has shown to be effective in both the treatment and prevention of a variety of chronic conditions and disability (Thompson et al., 2020). In our study, physical activity was not associated with any other caregiver or PWD mental health outcome. The lack of association between physical activity and caregiver outcomes is inconsistent with findings from the previous RDAD implementation that found that the more exercise sessions the lower the caregiver strain related to their relationship and physical health. The lack of association between physical activity and PWD outcomes in our study is in line with a recent meta-analysis that concluded that the evidence for beneficial effects of exercise on quality of life in PWDs is inconclusive (Ojagbemi & Akin-Ojagbemi, 2019).
Sedentary behavior has been linked to mental and physical health (de Rezende et al., 2014). RDAD-KC participants did not decrease their sedentary behavior. However, it is important to note that this lack of change might be due to a floor effect of the measurement. PWDs were already spending an average of zero days mostly sitting or lying at baseline, leaving no room for improvement. More rigorous sedentary behavior assessments such as accelerometers or validated scales might help capture the change in sedentary behavior. Alternatively, agencies might need to make additional efforts to recruit more sedentary PWDs, as they might further benefit from RDAD-KC physical activity component.
This study highlights the need to tailor interventions to the community. RDAD-KC, a less stringent version of RDAD led to clinically significant benefits that are comparable with original RDAD results. The association between number of RDAD-KC sessions and unmet needs suggests that while a degree of flexibility in the implementation of RDAD-KC is important, interventionists should encourage dyads to complete as many sessions as feasible. RDAD-KC participants did not improve their levels of sedentary behavior.
Caution is warranted when considering these results, as limitations of this project include a pre–post design with no control group, which prevents from causation inference. The outcomes were not collected as part of a prospective research study. Rather, the outcomes and data collection were part of a mutually agreed upon standard set in a collaborative service provision project in Kansas City. Significant flexibility was afforded to the agencies in the delivery of the intervention and the integration of the outcomes into workflows. Thus, these results reflect “real world” realities, essential to our goals. The results do provide support that several independent agencies can mutually deliver a semi-standardized dementia support program in the home and identify meaningful improvements for the caregiver and PWD. The number of dyads who could not complete the intervention is problematic, though perhaps not unexpected. The requirements of the project and the cooperative funding agreement necessitated the inclusion of PWDs who were at moderate stage dementia. Moderate stage dementia is typically a transitional time, when caregivers begin to consider placement. Unfortunately, the service providing agencies did not collect information on reasons for ending participation in the intervention. Post hoc interviews with the agencies suggest that caregiver burden, medical crisis, and residential care placement were the primary reasons for ending program participation. This was a quality improvement project and research was not its primary goal. For this reason, results are specific to the partnering organizations and are not necessarily generalizable to other communities or collaborative groups.
Conclusion
Despite their strong evidence, replications of evidence-based dementia care receiver–caregiver dyad interventions in the community are scarce. This limitation prevents from understanding whether the benefits of these interventions can be translated into real life. This implementation of RDAD-KC leads to clinically meaningful improvement of behavioral symptom distress among caregivers and severity among PWDs. RDAD-KC also leads to improvements in other outcomes including caregiver strain and unmet needs and physical activity of PWDs. Findings from this study address key needs identified in the National Plan to Address Alzheimer’s. These findings provide useful information to implement a real-life intervention that enables family caregivers to continue to provide care while maintaining their own health and well-being. Despite the uniqueness of every community, the RDAD-KC implementation experience may contribute to informing the scaling-up of RDAD in other communities.
Footnotes
Acknowledgements
The corresponding author affirms that he has listed everyone who contributed significantly to the work and has obtained written consent from all contributors who are not authors and are named in this section. The authors thank all community agencies who participated in the RDAD-KC project, the ACL officers for their input during the project and all individuals who participated in RDAD-KC.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Findings reported in this project were supported by the Administration for Community Living under Cooperative Agreement Award Number 90KSALGG0009. The sponsors defined the dementia severity required for individuals to participate in the project. The work reported in this publication was partly supported by the National Institute on Aging of the National Institutes of Health under Award Number P30AG035982.
Human Subjects
The project was determined to be secondary data analysis by the University of Missouri at Kansas City Institutional Review Board of the Project Evaluator site, because no identifiable information linked to the outcomes was transmitted outside of the agencies that delivered the intervention, and the outcomes were collected as part of service provided to the community under the cooperative funding agreement (Protocol #17-281).