
Abstract
Aged care services have the potential to support social participation for the growing number of adults aging at home, but little is known about the types of social activities older adults in community care are engaged in. We used cluster analysis to examine the current profiles of social participation across seven domains in 1,114 older Australians, and chi-square analyses to explore between-group differences in social participation and sociodemographic and community care service use. Two distinct participation profiles were identified: (a) connected, capable, older rural women and (b) isolated, high-needs, urban-dwelling men. The first group had higher levels of engagement across six social participation domains compared with the second group. Social participation among older adults receiving community care services varies by gender, age, individual care needs, and geographical location. More targeted service provision at both the individual and community levels may assist older adults to access social participation opportunities.
Introduction
The world’s population is aging and health care systems are under increased pressure to care for older people (Ministerial Advisory Council on Ageing, 2003). Accordingly, demand for policies that promote “active aging” via optimizing opportunities and connections with community, friends, and family is increasing (World Health Organization [WHO], 2015). In addition to the societal value proffered by older adults’ continued engagement in areas of social participation such as community involvement (Martinson & Minkler, 2006), a growing body of research has shown that such participation can also contribute to better individual health outcomes. Indeed, engagement in social activities can have positive impacts on mental health (Croezen et al., 2015), quality of life (Levasseur et al., 2008), cognitive function (Tomioka et al., 2016), mortality (Glass et al., 1999), and older adults’ perceptions of their community age-friendliness (Cao et al., 2020).
Given the multiple benefits associated with social participation, it is critical to identify individuals who may be at risk of unwanted social isolation and to improve their outcomes (Douglas, Georgiou, & Westbrook, 2017). Previous studies have shown men (Department of Social Services, 2015), younger age (Cherry et al., 2013), immigrants, and individuals with disabilities (Mendes de Leon et al., 2003) engage in social participation activities less frequently than their peers. However, these studies have focused on older adults in the general population or those residing in long-term aged care facilities. Consequently, little is known about participation activities among community-dwelling adults receiving community-based care. A recent study exploring participation of more than 2,800 older adults in home care in six European countries (Garms-Homolová et al., 2017) found that 40% of older adults have limited social interactions. However, that study only examined general social participation and did not describe the multiple forms of social participation that older adults may engage in.
Measures of social participation typically focus on specific social networks (e.g., contact with friends) (Fiorillo & Sabatini, 2015), activities (e.g., voluntary engagement) (Sirven & Debrand, 2012), or the total time engaged in social activities (Baker et al., 2005). Most commonly, studies use an index of the number of social participation activities someone engages in (Liu et al., 2016). Few studies derive or construct a social participation profile. Describing the multitude and degree of activity engagement in older adults will better capture their activity profiles.
Recent studies characterizing social activity profiles of older adults in the community have been conducted in Japan (Amagasa et al., 2017), Korea (Katagiri & Kim, 2018), Switzerland (Dawson-Townsend, 2019), and among partnered-older adults in Australia (Lam & Bolano, 2019). These studies have shown some individuals engage more in formal activities (e.g., club memberships, volunteering) and others in informal ones (e.g., family networks). Social participation profiles were found to differ mostly by gender, age, and socioeconomic status (Dawson-Townsend, 2019). However, a social participation profile of older adults receiving community-based care services remains largely unexplored.
Community Care Service in Australia: Enduring Gaps Between Policy and Practice
Current aged care reforms in Australia include a focus on providing home and community-based care services to support older people to remain in their own homes (Jorgensen & Haddock, 2018). The provision of these services recognizes the importance of maintaining social engagement for older adults and supporting socially isolated individuals through a range of social care services (Cherry et al., 2013; Jorgensen, Siette, Georgiou, Warland & Westbrook, 2018). Despite efforts to increase social engagement, aged care providers have found that 41% of older adults initially accessing services are lonely (The Benevolent Society & Social Policy Research Centre, 2009).
Measuring levels of social participation has multiple benefits for different stakeholders. At the individual level, the process of considering these questions can be used to open a conversation about social needs (Cardona, 2018). For care coordinators, results can assist in designing new and appropriate programs for the individual client (Siette et al., 2018). At an organization service provider level, results can inform where to direct resources and measure impact of policy and practice change. While current aged care policy supports the assessment and documentation of social needs, (e.g., adequacy of social support [Department of Health, 2018]), there is no mandatory nationwide assessment form or procedure to assess individual social needs. Some organizations are now targeting a more social approach, with a diversity of tools used across providers to measure psychosocial needs and health outcomes (Cardona et al., 2017). Nevertheless, this information remains patchy and, consequently, little is known about the social needs of older Australians in community care.
In this study, we investigated how social participation activities vary among older adults receiving community care services across seven forms of participation: social participation with members of the household, extended family, neighbors, friends, community, current affairs, and religion. The aim of this article was to examine (a) current levels of social participation, (b) sociodemographic, and (c) service use patterns associated with social participation among a large sample of older Australians receiving community care services.
Method
Setting
This cross-sectional study forms part of a larger program of research evaluating the implementation process of psychosocial tools for community care clients by a large aged care provider (Uniting) (Brett et al., 2019). Uniting provides aged care services across New South Wales (NSW) and the Australian Capital Territory (ACT) to more than 7,500 individuals annually. This study was conducted primarily across three Uniting community aged care regions (Northern Sydney Region, Hunter Region, and Blacktown Region) in NSW.
Participants
Participants consisted of those aged ≥60 years (n = 1,141) who completed the social participation tool with their care coordinator at Uniting as part of routine assessments during the period March 1, 2016 to December 30, 2018. All community aged care clients that were living in NSW and the ACT during the study period and have completed the assessment tools as part of a routine needs assessment were included. During this assessment period, 49% of the total client base receiving Commonwealth Home Support Program (CHSP) services (see definition below) in the three regions was interviewed as part of clients’ annual care needs assessment. Prior to interview, each person was invited to participate in the present study. All (100%) agreed to do so and went on to complete their participation. Clients in these regions who did and did not complete the tools were similar in terms of age and country of birth, but a greater proportion of women (77% vs. 64%) and those receiving a pension (86% vs. 79%) completed the tools.
Data Source
Nonidentifiable data on service provision, demographic characteristics, and social participation were extracted from Carelink+, Uniting’s centralized client management system. Further information about the implementation of Carelink+ is available at Brett et al. (2019). The data extracted are described below.
Social participation measurement
Social participation was measured using the 15-item short form of the Australian Community Participation Questionnaire (ACPQ-SF15), a validated instrument with good construct validity and reasonable concurrent validity for assessing social participation in the Australian general population (Berry et al., 2007). The ACPQ-SF15 measures diversity of social participation both in a formal (e.g., political participation) and informal (e.g., active social life, organized aspects of community life) context, based on definitions of social participation by Australians (Berry, 2008a, 2008b; Berry et al., 2007). This instrument is a systematically developed, theory-based, comprehensive measure of volitional community participation (Berry et al., 2007).
The ACPQ-SF15 was integrated into the client management system prior to study commencement and was embedded into community care coordinators’ routine assessment procedures (Siette et al., 2018).
The ACPQ-SF15 contains 15 items assessing seven domains of participation: contact with immediate household, extended family, friends, neighbors, participating in organized community activities, taking an active interest in current affairs, and religious observance. On average, there are two items per domain. See Supplementary Material for a copy of the questionnaire. There are three measures of participation that can be derived from the ACPQ-SF15:
Individual item scores. Each of the 15 items was scored from 1 “never or almost never” to 7 “always or almost always” using a 7-point Likert-type response format (see Supplementary Material).
Domain scores. Mean scores for each of the seven domains were calculated using weightings derived from one-factor congeneric models, as previously described (Berry et al., 2008).
Breadth of overall participation scores. An overall score that ranges from 0 (respondent did not participate at above-average levels in any domain of social activity) to 7 (respondent participated at above-average levels in all domains of social activity). This overall breadth of participation was calculated by initially (a) dichotomizing participants’ scores about the sample mean for each domain, then (b) assigning values of 0 to those whose scores fell below the sample mean and 1 to those at or above the mean and finally (c) summing these values to calculate a final score. Thus, higher scores denote greater breadth of social participation. Further information on this approach can be obtained from Berry et al. (2008).
Community care service factors
In Australia, there are two major types of government-subsidized community aged care: the “CHSP” and “Home Care Packages” (HCPs). The CHSP provides entry-level, low-care support (e.g., respite centers, social support), whereas HCPs provide coordinated services for older adults with ongoing higher level complex care needs (e.g., personal services, clinical services) (Department of Social Services, 2015). Service factors obtained from Carelink+ included type of aged care funding, service hours, and service types. The type of aged care funding was determined at the time of administration of the ACPQ-SF15.
The start time, end time, date, and service type were available for each occasion of service. Service hours per week were calculated as the median number of service hours per week for up to 91 days before the assessment. The number of different service types and the most common service type that made up the largest proportion of service hours delivered to the client over this period were also calculated.
Demographic factors
Demographic data such as age, gender, relationship status, carer status, country of birth, language spoken, pension status, suburb, and postcode were extracted. The client’s suburb of residence (or postcode, where there was no matched suburb) was used to classify remoteness based on the Accessibility/Remoteness Index of Australia (Australian Bureau of Statistics, 2018a). The Index of Relative Socioeconomic Advantage and Disadvantage was used to classify socioeconomic status based on the client’s suburb or postcode (Australian Bureau of Statistics, 2018b). Carer status refers to whether the client had a family or other person with responsibility for caring for them.
Statistical Analyses
Descriptive statistics were produced for all measures, with one-way analysis of variance used to compare mean social participation scores by gender and age group. For all tests, a Bonferroni correction was made to adjust for the large number of tests and comparisons by dividing the alpha level by the total number of calculations made for each dependent measure (n = 12), thereby reducing alpha to .004 (.05/12) (Althouse, 2016).
Individuals had multiple unique patterns and combinations of the 16 service types used by the study population (88 service types). To account for the interplay between services provided and to identify the major service use patterns, each client was assigned a “service group” based on similar patterns of types of services used over the study period. Factor analyses using principal axis factoring and a varimax (orthogonal) rotation procedure were applied to produce uncorrelated, easily interpreted factors of the services used (Yong & Pearce, 2013) (see Supplementary Material for the factor loadings).
Social participation profiles were generated using two-step cluster analysis, an analytic method in which ordinal and continuous variables are used together to identify distinctive and unique subgroupings of individuals within a heterogeneous sample (Berry, 2008b).
Two-step clustering with a log-likelihood distance measure was used because our data set was large and contained a mixture of continuous and ordinal and variables. Variables entered in the analysis included individual responses to the 15 statements of the ACPQ-SF15 questionnaire. Schwarz’s Bayesian criterion and Akaike’s information criterion were calculated to measure the distance between clusters for different cluster solutions to determine its appropriateness, a statistic commonly used in social and health care clustering studies (Finch et al., 2016; Vuik et al., 2016).
To evaluate the stability of the cluster solution, the original data were randomly split into two data sets and the two-step cluster analysis repeated separately on each data set. Multivariate analysis of variance (MANOVAs) were then conducted to evaluate whether there was significant or substantively important variation within clusters between each data set for each social participation type.
Chi-square tests were used to assess between-cluster differences in distributions of demographic variables and service use. All statistical analyses were performed with IBM SPSS Statistics version 22 (IBM Corporation, Armonk, NY, USA).
Ethics
Ethical approval was granted by the Macquarie University Human Research Ethics Committee.
Results
Client Characteristics
Most clients were aged ≥75 years (M = 81.1; SD = 8.4), female (75.5%), living alone (56.6%), residing in a major city (79.1%), born in a country where the main language is English (59.9%), and receiving a government pension (92.6%) (Table 1). The majority of clients (81.9%) received entry-level home support services. Clients received 5.2 hr of care per week on average (SD = 4.1). Clients most frequently belonged to the center-based respite service group (75.2%), with social support services a distant second (14.5%).
Sociodemographic Characteristics of Older Adults in Home Aged Care by Social Participation Cluster Type (N = 1,141).
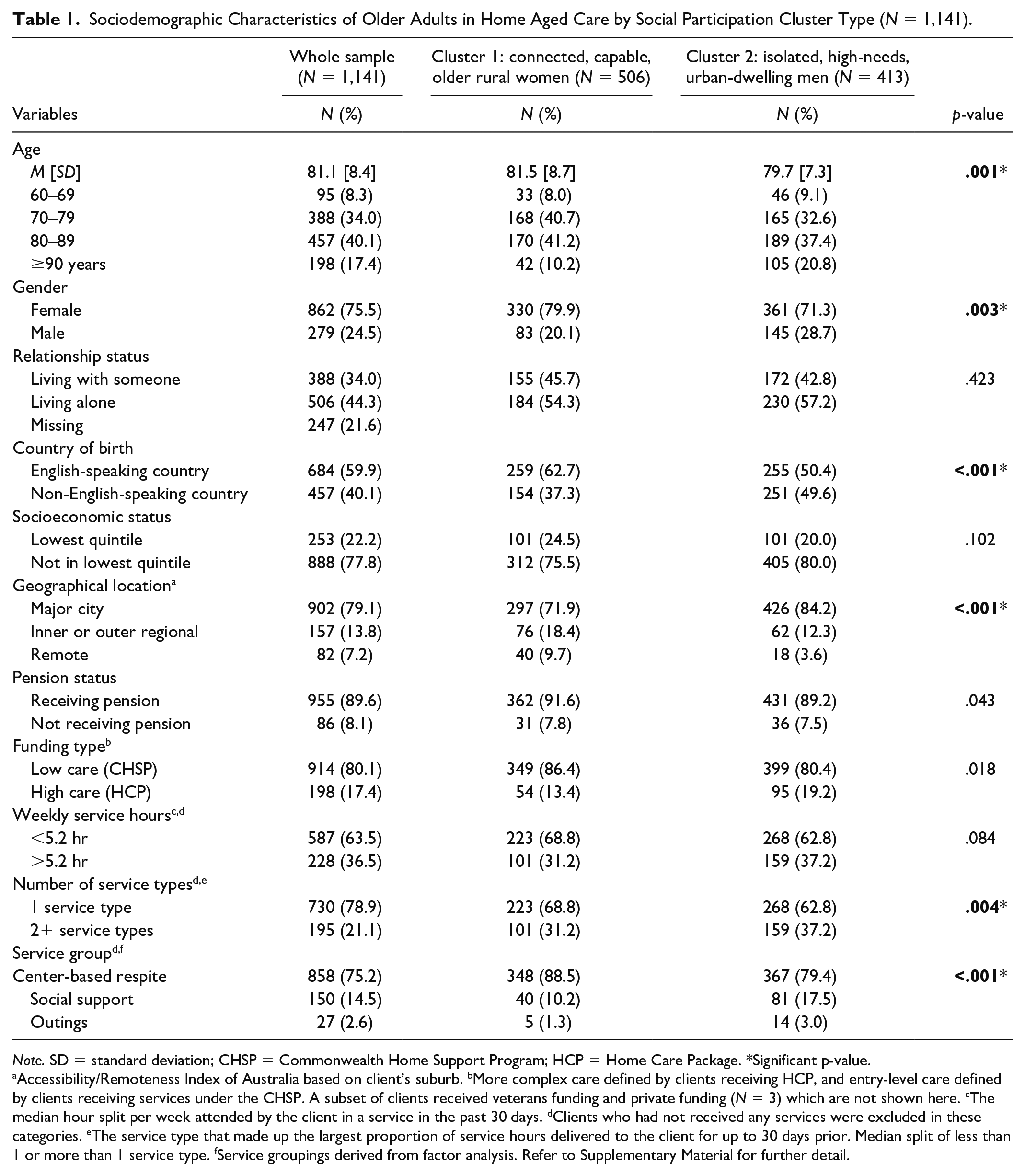
Note. SD = standard deviation; CHSP = Commonwealth Home Support Program; HCP = Home Care Package. *Significant p-value.
Accessibility/Remoteness Index of Australia based on client’s suburb. bMore complex care defined by clients receiving HCP, and entry-level care defined by clients receiving services under the CHSP. A subset of clients received veterans funding and private funding (N = 3) which are not shown here. cThe median hour split per week attended by the client in a service in the past 30 days. dClients who had not received any services were excluded in these categories. eThe service type that made up the largest proportion of service hours delivered to the client for up to 30 days prior. Median split of less than 1 or more than 1 service type. fService groupings derived from factor analysis. Refer to Supplementary Material for further detail.
Social Participation
Responses to each ACPQ-SF15 item are shown in Figure 1. Although 53% of clients often saw people in their immediate household (n = 591), one third of clients did not. Clients generally participated in current affairs, with almost half the sample often talking about current affairs (48%, n = 534) and reading articles about current affairs (43%, n = 479). In comparison, there was a high percentage of clients who reported never or rarely engaging in the following activities: seeing their friends (31%, n = 345), discussing news with their neighbors (33%, n = 368), chatting with their neighbors (26%, n = 280), attending religious services (54%, n = 601), going to prayer meetings (69%, n = 771), and attending community events (36%, n = 401).
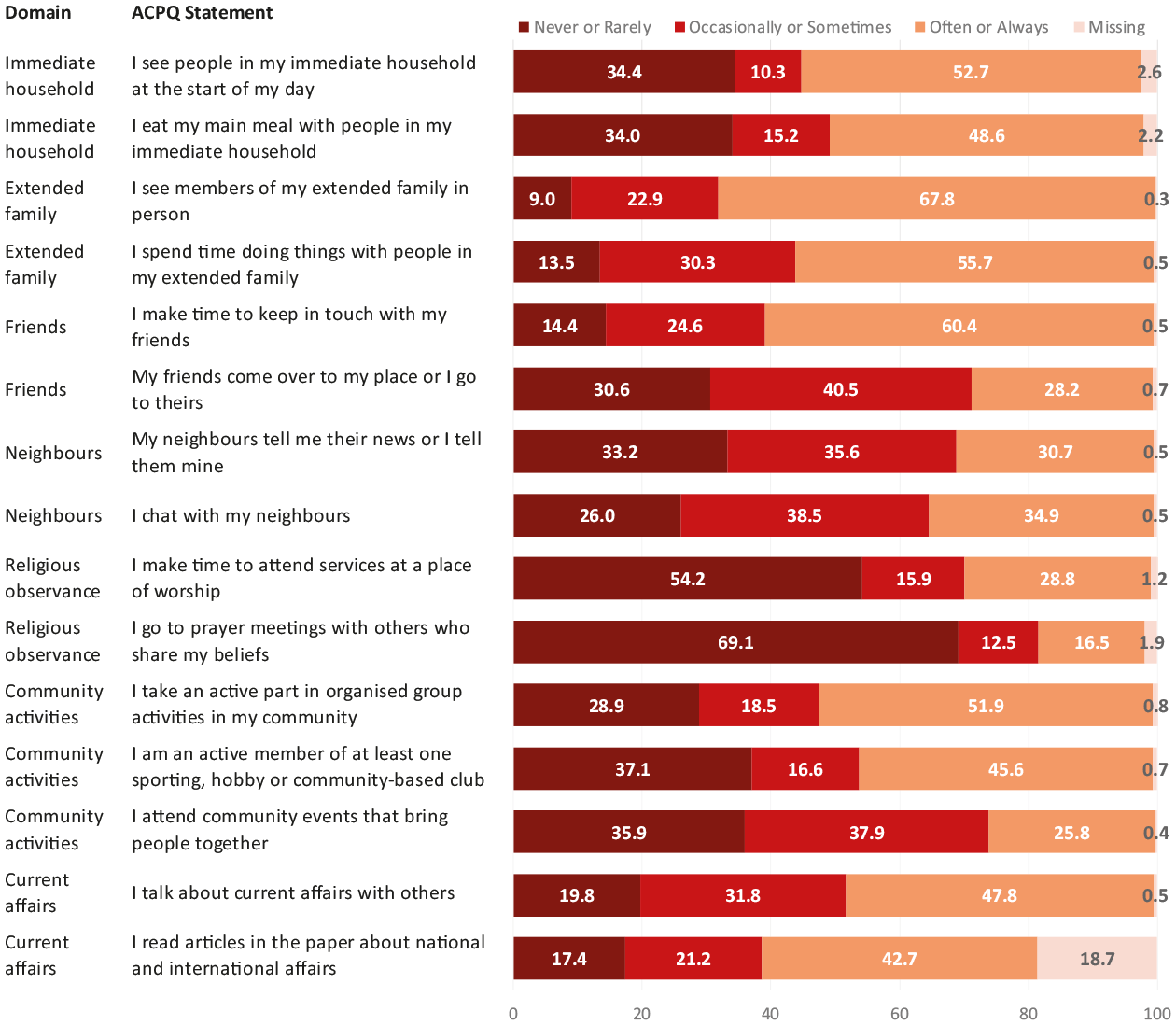
Distribution of responses to each ACPQ-SF15 statement (N = 1,141).
The most frequent domains of social participation were, in order, having contact with extended family, with household members and with friends (Table 2). Religious observance was the least frequently reported type of participation.
Mean Scores and Standard Deviations for Social Participatory Domains by Cluster.

Note. SD = standard deviation; CI = confidence interval.
Cluster 1 is significantly different to Cluster 2.
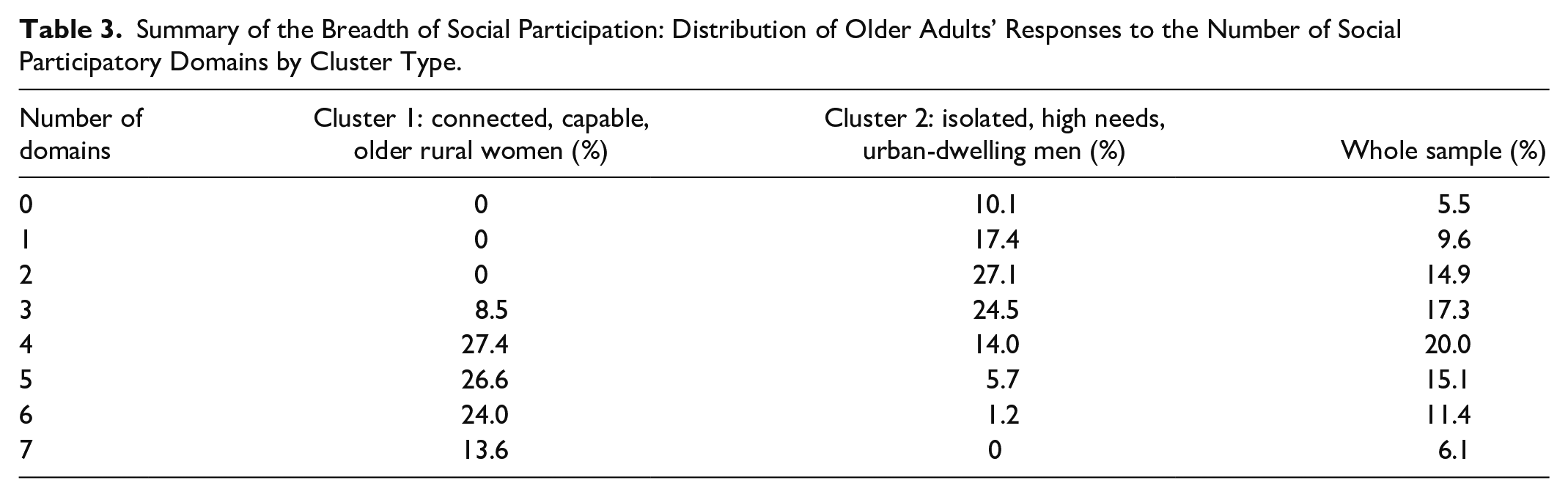
On average, clients participated in at least three of the seven domains (breadth score = 3.61, SD = 1.90). Most people participated in at least one domain (94.5%), and 6.1% were participators in all seven domains (Table 3).
Summary of the Breadth of Social Participation: Distribution of Older Adults’ Responses to the Number of Social Participatory Domains by Cluster Type.
Types of participation varied by gender and age (Table 4). Individuals aged 85 years and older participated significantly less often in the friends and community domains compared with individuals aged 84 years and younger. Overall, individuals aged 85 years and more had significantly lower breadth of participation when compared with individuals aged between 76 and 84 years. Women reported participating more often in the friends and community domains than did men, whereas men participated more often in the immediate household domain (Table 4).
Mean Participation Scores Across Seven Social Participatory Domains by Age and Gender.
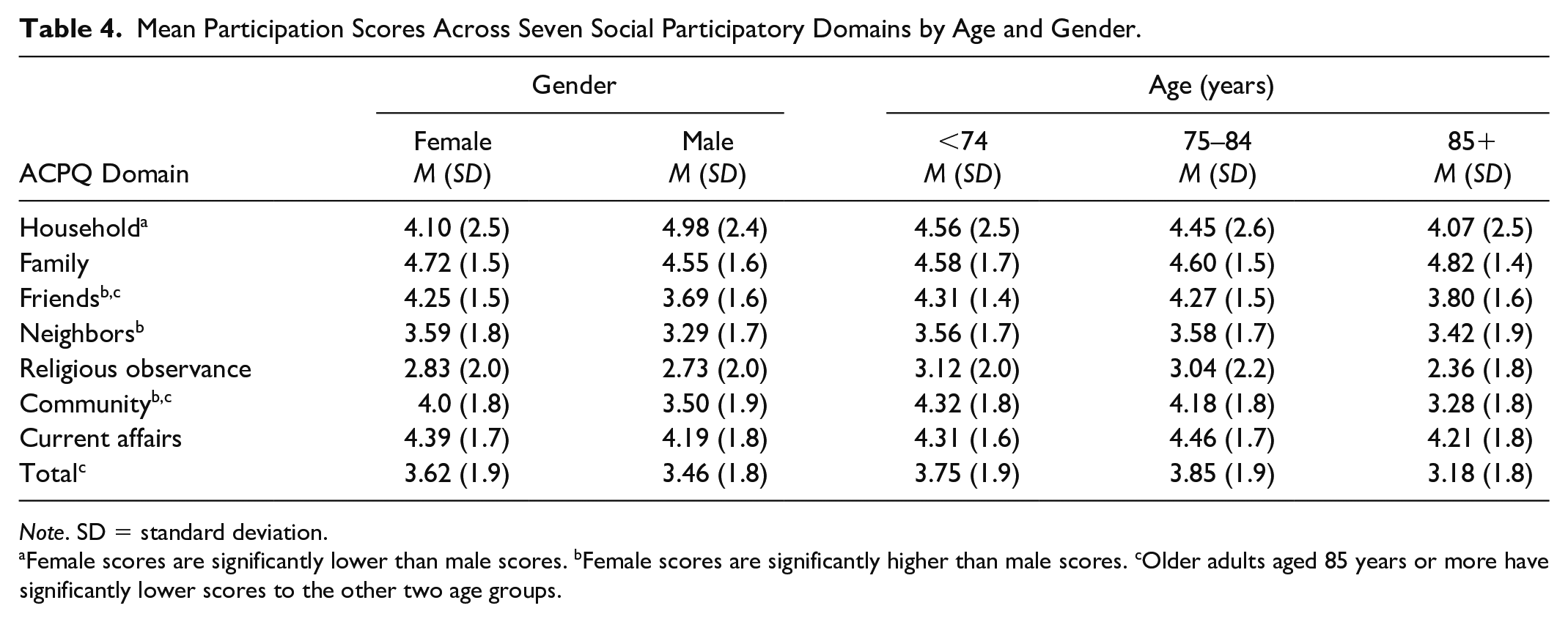
Note. SD = standard deviation.
Female scores are significantly lower than male scores. bFemale scores are significantly higher than male scores. cOlder adults aged 85 years or more have significantly lower scores to the other two age groups.
Social Participation Profiles
Supplementary Material presents the criterion statistics for the agglomeration schedules and the ratios of change for both criteria indicated cut-offs at two clusters. The same number of groupings emerged when the analysis was repeated on two data sets created by randomly splitting the original sample. Mean scores and standard deviations for measures of social participation domains by cluster are presented in Table 2.
Cluster 1 (“Connected, capable, older rural women”) consisted predominantly of clients reporting high levels of most types of participation across family, friends, neighbors, religious observance, community engagement, and current affairs domains. They also reported by far the highest breadth of participation in social activities and participated in between three and seven different social participatory domains. Members of Cluster 1 were older women, not living alone, living in a regional area, born in an English-speaking country, receiving less than one service type and mostly attending a center-based respite group.
Cluster 2 (“Isolated, high needs, urban-dwelling men”) comprised clients with the lowest levels of involvement across most participatory domains. Compared with Cluster 1, clients in Cluster 2 reported similar levels of social engagement with immediate members of their household but significantly lower levels of engagement with the other six domains (family, friends, neighbors, religious observance, community engagement, and current affairs). They also reported a narrower breadth of participation across all social activities. A small but important minority (10.1%) of these clients were not participators in any social participatory domain. Compared with Cluster 1, those in Cluster 2 were more likely to be younger, male, living alone, living in a major city, and from a non-English speaking country. The vast majority of members of Cluster 2 were receiving more than one service type, with attendance at center-based respite groups and social support groups.
Discussion
There have been few empirical studies exploring social participation patterns among older adults receiving community care services (Garms-Homolová et al., 2017). Our study offers insights into the types of social activities in which this population is engaged, including contact with household, family, friends, neighbors and participation in community, current affairs, and religious activities. The majority of aged care clients in our study participated in at least one of the seven domains. However, close to one third did not see their friends, discuss news with their neighbors or attend community events and around one in 20 did not participate in any domain. This is a concern as older adults with low levels of community participation are at high risk of ongoing social marginalization, and the isolation and poor physical and mental health outcomes that typically accompany it (Berry et al., 2008).
Our study participants fell into two groups of clients with distinct patterns of social participation and associated sociodemographic characteristics. The connected, capable, older rural women group accessed fewer services, had high levels of participation and were older women living in a regional area with someone; and the isolated, high needs, urban-dwelling men, who participated little, were younger men living alone in a major city from a non-English speaking country, and had more complex and intensive service use. It is this group that is particularly at risk of marginalization.
Detailed comparison with other study findings is difficult due to the relative absence of similar studies. However, a cluster analysis of patterns of community participation, social cohesion, and mental health in an Australian regional community identified a group of older adults, “aging, participating less,” with compromised community participation and poor mental health (Berry, 2008b). Other than high levels of contact with neighbors, these older adults had generally lower levels of participation than did other groups, although they enjoyed their participation and would have liked more. Compromised participation, alongside barriers to participation (such as financial constraints and declining health), contributed to participants’ poor sense of belonging and elevated psychological distress.
We found major differences between our findings and those reported in previous general population studies in Australia (Australian Bureau of Statistics, 2016; Berry, 2008a, 2008b). Compared with a national Australian study surveying more than 18,000 adults (Australian Bureau of Statistics, 2016), our sample of older adults in community care participated in fewer activities away from home in the community. Furthermore, compared with retired community-dwelling adults aged 45 years and older (Berry, 2008a, 2008b; Cruwys et al., 2013), our sample engaged more often with family members, religious observance and community activities but less with current affairs. These distinctions are consistent with an older, frailer sample more likely to require care from family members, formal home care support and services tailored toward community engagement (e.g., respite centers and day trips). The fact that these older care recipients do still participate in their communities highlights that community care services are able to promote community and personal participation and are supporting the social needs of older adults.
Consistent with other studies, we found that men had more contact with family while women were more engaged in social and community-based activities (Berry et al., 2008). Also, women tend to innovate more than men in later life by being more receptive to new leisure activities, actively participating in social activities and engaging at a greater frequency (Jaumot-Pascual et al., 2016). To boost older men’s engagement in social activities beyond the family, aged care providers could make social programs and services more appealing to men by increasing male representation, such as, program advertisements featuring men as well as adapting program content to suit their interests (Department of Health, 2014).
Our findings add to the evidence base by identifying groups where low social participation is prevalent and describing their service use and sociodemographic profiles. High levels of social engagement were significantly greater for people who were older, female, living remotely, and receiving less than one type of aged care service. This suggests that having fewer care needs and better health status facilitates social participation. In comparison, there was less social involvement among younger males living alone in a major city and receiving more services, suggesting that gender and a higher level of need may hinder participation.
Our results provide further information for people aged 85 years and older. This group varies substantially in how often they see friends and participate in religious activities and community events compared with people aged less than 85 years. However, this does not mean that older adults no longer wish to participate socially. Indeed, older adults aged 80 years and over report that having satisfying social relationships facilitated by gatherings is critical to their wellbeing (Halaweh et al., 2018), however participating in group recreation activities often decline with age (Australian Bureau of Statistics, 2016; Black & Hyer, 2020).
Social participation also differed by geographical location. It was expected that, as remote and rural areas have fewer accessible social and community resources than are available in urban areas (Eckert et al., 2004), this would reduce opportunities for social participation for older people living in more rural locations. However, we found older adults living in regional areas reported significantly greater involvement in five types of social participation, reporting more contact with family, friends, and neighbors, and more engagement community activities and current affairs. It could be argued that lower population density as well as lower levels of public services, as are often found in rural areas, better facilitate community activities, cooperation, and exchange and contribute to a greater sense of belonging (Duppen et al., 2019; Pretty et al., 2007).
Implications
There is increasing emphasis from governments on enabling older adults to stay at home for longer, yet there are significant gaps in knowledge about the social needs of older adults in community care. Our findings confirm that individuals with greater care needs participate less than those with fewer needs and highlight other factors that affect older adults’ participation. Despite wanting to continue engaging in their communities, we show that older adults aged 85 years or more were less likely to attend community events, suggesting that current aged care services may need to be adapted to use more creative ways to support engagement. Providing services to individuals in their own homes through technological means may be one effective strategy to facilitate some forms of social participation (Pinto-Bruno et al., 2017). Having flexible home service sessions and targeting personal interests can also assist with developing community connections (The Benevolent Society & Social Policy Research Centre, 2009). Furthermore, clients who are unable to leave their homes could benefit from the delivery of innovative social support services, such as bringing an outing to the client either through a befriending service (Kharicha et al., 2017).
The accessibility and adequacy of public transport are particularly important elements of creating an aging-friendly living environment (WHO, 2007). When older adults lose the ability to drive a car, aged care providers and local and state governments should improve public transport options, such as group transportation by coach, to allow older people to reach social gathering places and maintain a high level of social participation. Moreover, providers could consider offering informal meeting places in the nearby neighborhood to foster opportunities for social participation. Such offerings would also address older peoples’ tendency to reject activities with rigid schedules (WHO, 2007) and their preference for casual, spontaneous, and voluntary encounters rather than regular and mandatory commitments (Rainer, 2014).
Limitations
The use of self-report data alone means that we could not corroborate participants’ perceptions with observational data. Older adults may have different goals relating to social participation or may value particular social participation domains more than others, and this was not captured in our study. Future studies should address this and consider adding measures of the quality, quantity, and nature of participation obtained from structured observations as well as using other methodologies (e.g., field experiments). These would provide the additional detailed information to better understand and respond to older adults’ social participation preferences (Sampson & Raudenbush, 1999).
The goal of this study was to develop an understanding of older community-dwelling adults’ social participation and potential areas to target. While our cross-sectional design was appropriate for this goal, it could only provide a snapshot of participation patterns at one point in time. Examining changes in patterns of social participation in a longitudinal study would be valuable in identifying the determinants of community engagement and outcomes such as time to residential care admission.
Conclusion
Our findings provide a better understanding older adults’ social needs and preferences and provide information to facilitate targeting and adaptation of services to improve older adults’ social engagement. Directing services to older adults that most need them and tailoring these services to individual preferences is an enduring public policy challenge. Services and systems that can identify and address gaps and variations in older adults’ social participation should be explored for their potential to reduce isolation and loneliness and their harmful consequences. Our findings describe two distinct subgroupings of community-dwelling older adults with very different service needs. We provide information for policymakers and service providers to see the value of incorporating individual- and population-based social participation profiles into planning more innovative resources, such as bringing a social service to the individual that may support our aging population to live at home for longer. Ultimately, this could substantially improve well-being among this vulnerable group.
Supplemental Material
JAG_Resubmission_Supplementary_Material_Unblinded – Supplemental material for Social Participation Among Older Adults Receiving Community Care Services
Supplemental material, JAG_Resubmission_Supplementary_Material_Unblinded for Social Participation Among Older Adults Receiving Community Care Services by Joyce Siette, Helen Berry, Mikaela Jorgensen, Lindsey Brett, Andrew Georgiou, Tom McClean and Johanna Westbrook in Journal of Applied Gerontology
Footnotes
Author Contributions
J.S., M.J., L.B., A.G., and J.W. planned the study. M.J. prepared the data for analysis, J.S. performed all statistical analyses and H.B. supervised the data analysis. T.M. helped to plan the study, including the instrumentation. J.S. wrote the first draft of the manuscript, and all authors contributed to revising the paper. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an Australian Research Council Linkage Grant (LP120200814) and a Dementia and Aged Care Services, Australian Government Department of Health Grant (Agreement ID:4-4ZO9T5A, Schedule ID:4-4ZO9T62) in partnership with Uniting. The funding body did not have an input in any part of the research process including the design of the study, data collection, analysis and interpretation of data, and in writing the manuscript.
IRB Protocol/Human Ethics Approval Numbers
Ethical approval was granted by the Human Research Ethics Committee at Macquarie University, Australia, protocol number 5201401031.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.