
Abstract
Wandering is a potentially dangerous event for individuals living with dementia and is equally as stressful for their caregivers. The purpose of the current study was to examine the validity of the Risk of Wandering (RoW) scale in terms of predicting wandering. We compared the RoW scale’s validity against two widely used scales that assessed dementia as reported by caregivers: Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE; Jorm) and Revised Memory and Behavior Problems Checklist (RMBPC; Roth et al.). The RoW scale predicted wandering events better than the IQCODE and comparably with the RMBPC, which is longer and less specific to wandering.
Wandering is a relatively infrequent event in the general population, but wandering can lead to potentially dangerous consequences for persons living with dementia (PLWD; Barnard-Brak et al., 2018). In the current study, wandering refers to instances in which PLWD abscond or leave the supervision of a caregiver (Monfort et al., 2018). Wandering can lead to potentially dangerous consequences such as individuals going missing and being harmed. Wandering can also serve a potentially therapeutic or meditative purpose via wayfinding through a park or other pedestrian setting (Moser, 2019). However, PLWD who wander can experience injury (Douglas et al., 2011), go missing (Rowe et al., 2012), and there are even reports of death. It is estimated that anywhere from 2% (Furumiya & Hashimoto, 2015) to 8% (Woolford et al., 2017) of wandering events result in death. However, reports of wandering-related deaths may differ based upon certain regions (i.e., international versus United States) or facilities (i.e., institutional versus community settings) and may not be generalizable across settings.
Risks Associated With Wandering
Beyond the possible danger to PLWD who wander and the stress that caregivers experience as a result (Monfort et al., 2018), society also indirectly incurs the costs of wandering. This cost includes Silver Alerts (e.g., Petonito & Muschert, 2015; Yamashita et al., 2013) as well as premature placement in residential facilities (Pope & Kang, 2010). Pope and Kang (2010) found that for about two out of three older persons, relocation from their home was not planned, but a reaction to circumstances such as dementia-related behavior. One explanation for this premature relocation has been, “ . . . fragmented and poorly coordinated care,” (Kolanowski et al., 2018, p. 1050).
Wandering among PLWD has been related to age (Monfort et al., 2018; Rowe et al., 2012) but other variables are also associated with it. Landau et al. (2010) have noted that wandering seems to be “one of the more common behavioral manifestations of dementia,” (p. 409), estimating that approximately 20% to 25% of PLWD will wander at some point in their illness. Barnard-Brak et al. (2018) found that approximately half of caregivers to PLWD reported a wandering event having occurred in the past year. The likelihood of a wandering event increases with symptoms of dementia (Häggström et al., 2010; Monfort et al., 2018). Symptoms of dementia include internalizing, cognitive behaviors such as attention/memory issues (Jorm, 1994) and externalizing problem behaviors such as arguing and threatening to hurt oneself (Roth et al., 2003).
Measuring Wandering Risk
Given the prevalence and potential danger associated with wandering among older adults, an instrument to predict wandering events would be a useful tool. The development of an instrument that specifically predicts wandering can help ensure the well-being of older individuals by alerting professional caregivers to the likelihood of a wandering event. Family caregivers may also desire an objective measure to discern whether their concerns are warranted, especially in view of past wandering events. Caregivers do not want to limit the autonomy of PLWD unnecessarily, via tactics such as restraint or confinement (Landau et al., 2010), but safety is a paramount concern.
Purpose of the Study
Barnard-Brak et al. (2018) developed the Risk of Wandering (RoW) instrument as a quick screening tool. Current evidence indicates that the RoW tool for adults has sufficient psychometric validity in terms of predictive performance (Barnard-Brak et al., 2018). However, given the high correlation between cognitive impairment and wandering (Landau et al., 2010), the question remains whether it improves prediction of wandering over and above a general dementia screening instrument. The purpose of the current study was to examine the validity of the RoW scale in terms of predicting wandering versus two scales for symptoms of dementia: Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE; Jorm, 1994); and Revised Memory and Behavior Problems Checklist (RMBPC; Roth et al., 2003). The IQCODE measures caregiver perceptions of cognitive symptoms of dementia while the RMBPC measures frequency of and stress caused by dementia-related problem behaviors such as arguing and threatening to hurt oneself. Both measures have been widely used to measure symptoms of dementia (Häggström et al., 2010; Kolanowski et al., 2018).
Method
We utilized Receiver Operating Characteristic (ROC) analyses to test the validity of the RoW to predict caregivers’ retrospective reports of wandering events over the past year. One sample completed the IQCODE as a comparison standard; the other sample used the RMBPC. The internal consistency of scores is also reported, along with optimal cutoff scores, determined using ROC analyses, for the RoW scale to best predict wandering events determined using ROC analyses.
Samples
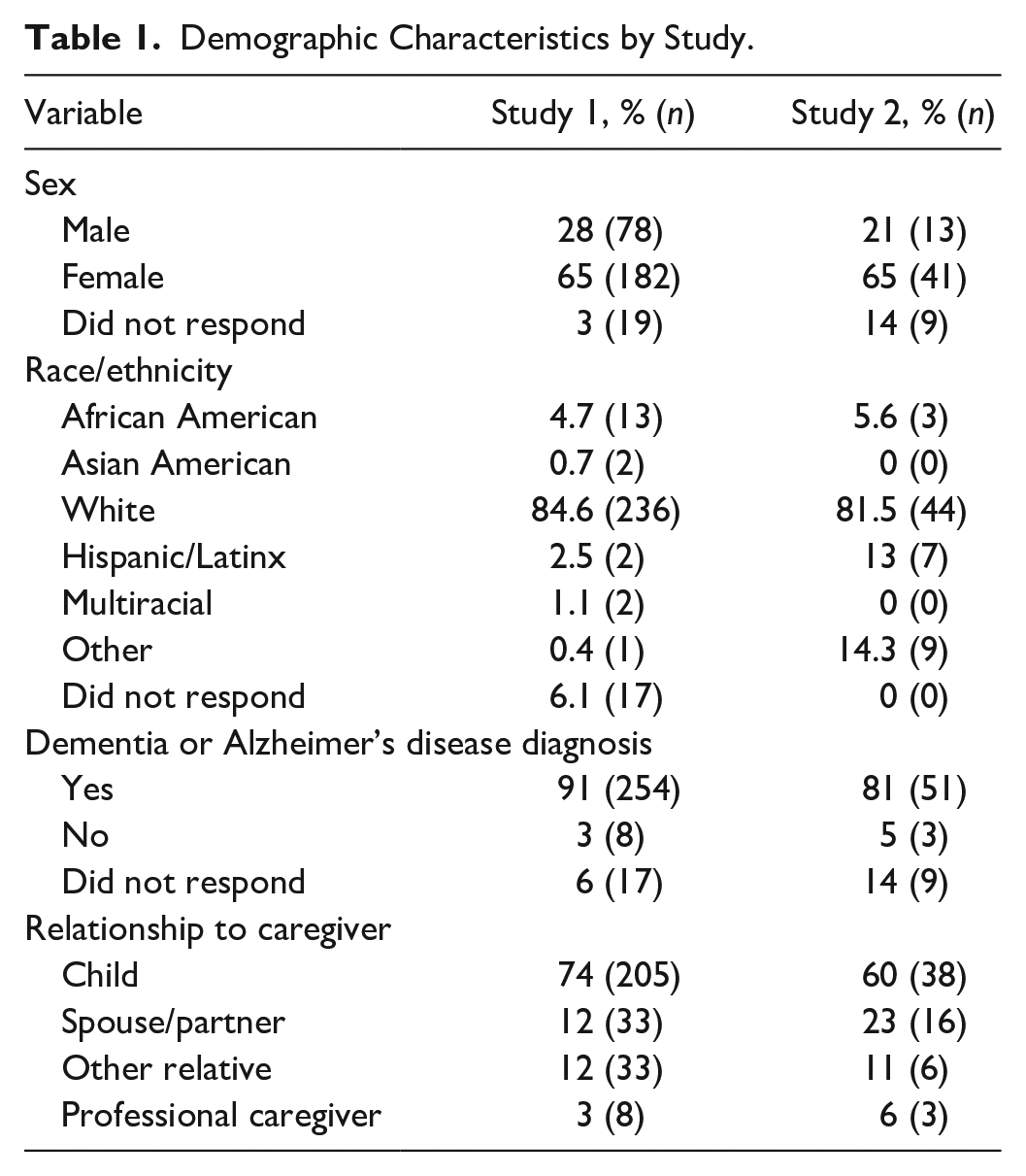
For Study 1, 279 caregivers recruited via the Alzheimer’s Association Trial Match system (Alzheimer’s Association, 2019) completed the RoW and IQCODE scales. The average age of the Study 1 caregivers was 57.52 years (SD = 9.27). Caregivers had known their PLWD on average 52.20 years (SD = 9.27). Average age of PLWD was 81.30 years (SD = 8.33). For Study 2, 63 caregivers were recruited from the same Trial Match system to complete the RoW and RMBPC scales. The average age of Study 2 caregivers was 58.49 years (SD = 14.51). Caregivers had known their PLWD on average 48.00 years (SD = 16.60). Average age of PLWD was 80.91 years (SD = 7.95). Table 1 presents demographic characteristics and relationship to PLWD for caregivers with similar distributions for sex, race, ethnicity, diagnosis, and reported relationship to the caregiver by sample.
Demographic Characteristics by Study.
Measures
The RoW is a 9-item scale completed by caregivers using a 3-point response format (Barnard-Brak et al., 2018). The RoW achieved α = 0.71 for Study 1 and α = 0.90 for Study 2. In Study 1, we measured cognitive status using the short form of the IQCODE (Jorm, 1994). The IQCODE is a 16-item scale using a 5-point response format measuring cognitive function over the past 10 years with α = 0.86. Approximately 42% (n = 109) of caregivers reported one or more wandering events in the past year. For Study 2, caregivers completed the RoW and a 24-item short form of the RMBPC with α = 0.91 (Roth et al., 2003). Caregivers rated frequency of occurrence of problems with memory and disruptive behavior in the RMBPC. Approximately 43% (n = 27) of caregivers reported one or more wandering events in the past year. Table 2 contains the complete items for the RoW scale. The RoW scale should be administered by a caregiver who has known the PLWD for at least 1 year (Barnard-Brak et al., 2018).
RoW Screener Items.
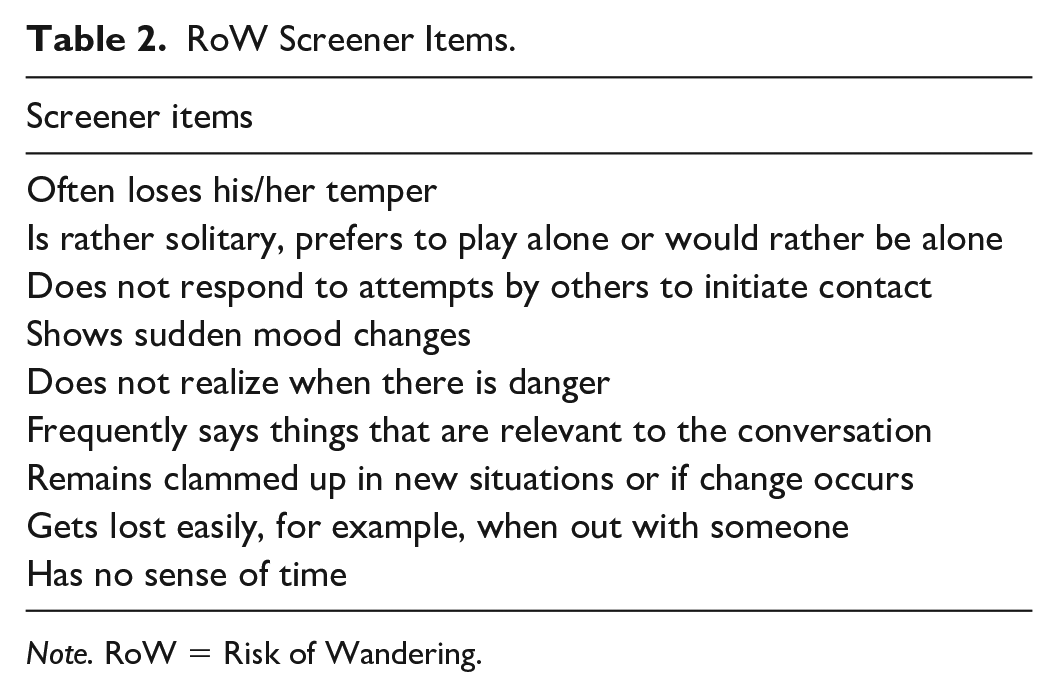
Note. RoW = Risk of Wandering.
Analyses
Bootstrapped ROC curve analyses were conducted separately for each study using the DeLong et al. (1988) method via MedCalc (v.18.9) to predict whether a wandering event occurred in the past year (MedCalc, 2016). Area under curve (AUC) values at or above 0.70 were considered as indicative of acceptable model fit. The optimal cutoff scores for the ROC analyses were determined via Youden J Index calculations (Youden, 1950). We next compared the ROC curves for the RoW, IQCODE, and RMBPC to determine whether these curves were significantly different by respective sample.
Results
Figures 1 and 2 provide the respective ROC curves. From these figures, the false positive rate (1–specificity) is plotted against the true positive rate (sensitivity) for each respective measure score. The optimal cutoff score is the elbow of the curve, which can be calculated via the Youden J index (i.e., sensitivity + specificity –1). The RoW was correlated with the IQCODE, r = 0.39, p < .001 and with the RMBPC, r = 0.41, p = .006. The ROC analyses for the RoW suggested acceptable model fit, AUC = 0.71, z = 6.99, SE = 0.03, p < .001 for Study 1 (IQCODE) and AUC = 0.84, z = 7.03, SE = 0.05, p < .001 for Study 2 (RMBPC). Table 3 displays the cutoff scores for the RoW as well as sensitivity and specificity values.
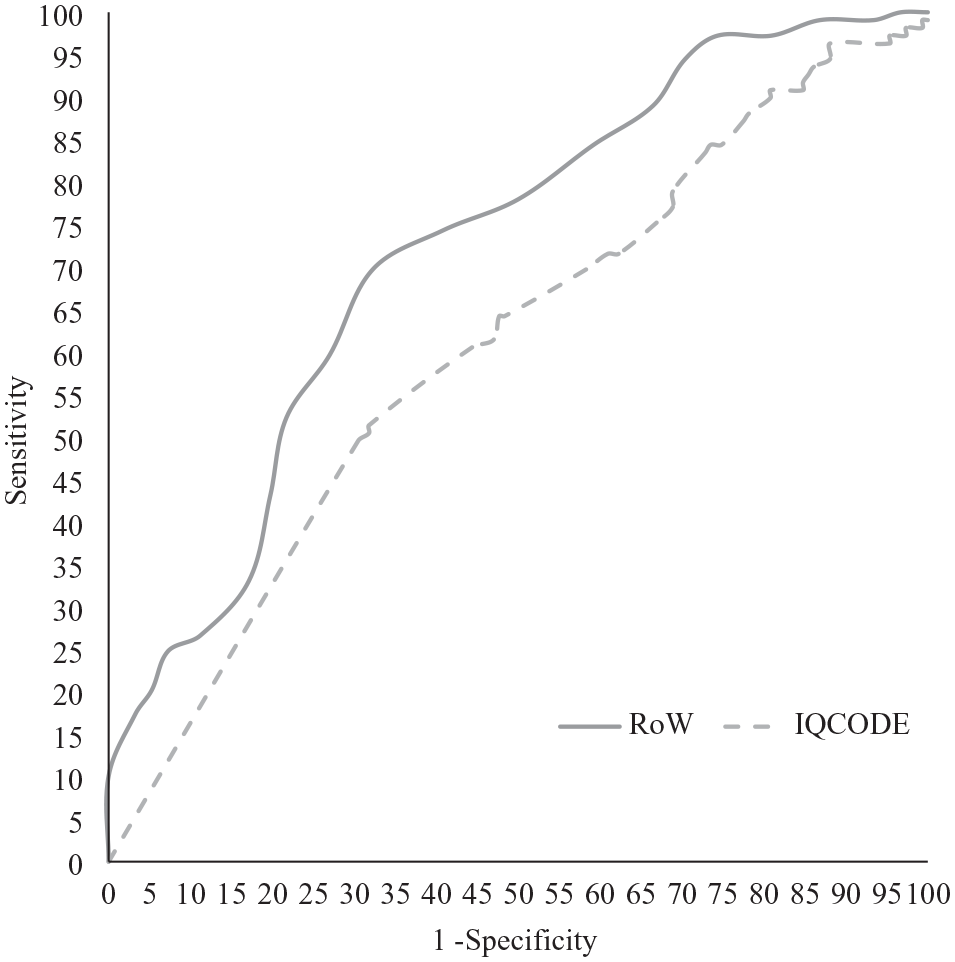
ROC curves comparing RoW with IQCODE.
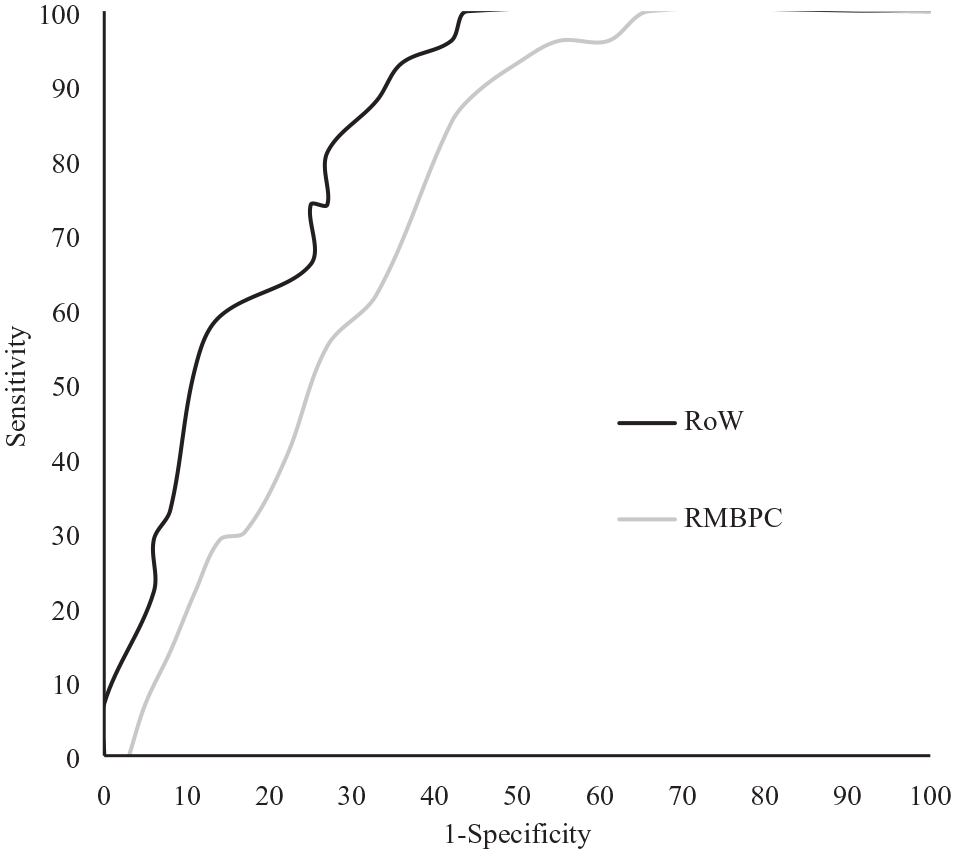
ROC curves comparing RoW with RMBPC.
Summary of RoW Scoring Results.
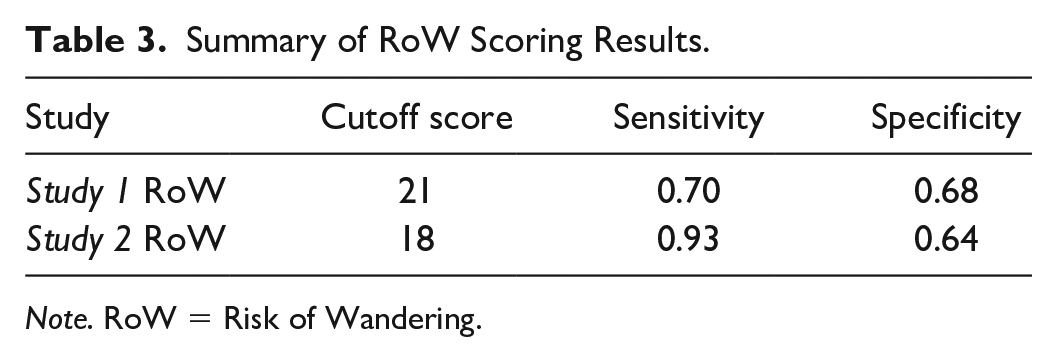
Note. RoW = Risk of Wandering.
The ROC analysis for the IQCODE did not indicate acceptable model fit, AUC = 0.61, SE = 0.03, z = 3.04, p = .002. The RoW had significantly better fit than the IQCODE, ΔAUC = 0.11, SE = 0.04, z = 3.11, p = .002. The RMBPC indicated acceptable model fit, AUC = 0.78, SE = 0.06, z = 4.74, p < .001. The RoW ROC curve was comparable, being no better or worse than the RMBPC, which is a longer instrument, ΔAUC = 0.06, SE = 0.06, z = 1.09, p = .27.
Discussion
The current study provides mixed evidence for the psychometric adequacy of the RoW scale with respect to predicting wandering events. The RoW scale predicted wandering events better than the IQCODE, and performed as well as the longer RMBPC. The IQCODE focuses strictly on cognitive symptoms of dementia (i.e., forgetting names and being inattentive in conversations) but not problem behaviors (i.e., becoming frustrated or impulsive). Thus, the IQCODE results indicate that purely cognitive symptoms of dementia may not be specifically related to wandering. In contrast, the RoW scale includes items that relate to both cognition (five items) and problem behaviors (four items). The RMBPC, however, focuses solely on caregiver-reported problem behaviors related to dementia (e.g., destroying property, arguing, irritability, and complaining). As there is substantive overlap between the RoW and the RMBPC; this may explain their comparability in predicting wandering.
The current study has several limitations. First, the retrospective nature of the survey may result in caregivers’ inaccurately recalling the occurrence and frequency of wandering events in the past year. Thus, our analyses focused on whether the individual had wandered at all rather than the number of wandering events. Second, the sample was predominantly white and, hence, may not reflect the general population. Future research should seek ways to purposefully sample families from non-White backgrounds. Third, we did not request information about comorbid disorders such as depression or anxiety. Future research should examine the role of coexisting disorders in the occurrence of wandering events, including both affective disorders as well as physical impairments that may limit mobility. Fourth, we did not collect information regarding the pre-illness cognitive abilities of the PLWD. The degree of decline in cognitive abilities pre-diagnosis may influence the RoW scores and the frequency of wandering. Future research should incorporate this information in analyses as a covariate whenever possible. Finally, the vast majority of the sample was nonprofessional caregivers at 98%, with only 2% (n = 4) being professional caregivers. The responses of professional caregivers may vary considerably from informal caregivers such as family and friends.
Several strengths have also emerged from the current study. First, a freely available measure to identify when PLWD are mostly likely to wander provides an objective means of assessing RoW among this population for both professional and family caregivers. The scale evidenced acceptable internal consistency and outperformed a standard measure of cognitive function in predicting past-year prevalence of wandering. It also performed equally as well as, but was far shorter than, a widely used measure of problem behaviors in dementia. We should reiterate that wandering can serve a potentially therapeutic purpose for individuals regardless of age. However, our review of the literature provides limited support for wandering as wayfinding and its potential therapeutic benefits at this time. Furthermore, this wandering can become dangerous for PLWD who may not realize that they are lost or able to find their way back (Moser, 2019).
In conclusion, RoW scores better predicted wandering events than the IQCODE and just as well as the RMBPC, a longer measure. The current study provides more evidence as to the psychometric sufficiency of the RoW as developed. Future research will perform additional confirmatory factor analyses to assess evidence of the construct validity of the scale as well as establishing the measurement invariance of the scale across subpopulations according to gender and race/ethnicity as more data are collected.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Statement
The University of Alabama’s Institutional Review Board approved this research study under IRB Protocol # 18-09-1577.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.