
Abstract
This study evaluated a 12-week, home-based combined aerobic exercise (walking) and computerized cognitive training (EX/CCT) program on heart failure (HF) self-care behaviors (Self-care of HF Index [SCHFI]), disease specific quality of life (Kansas City Cardiomyopathy Questionnaire [KCCQ]), and functional capacity (6-minute walk distance) compared to exercise only (EX) or a usual care attention control (AC) stretching and flexibility program. Participants (N = 69) were older, predominately female (54%) and African American (55%). There was significant improvement in self-care management, F(2, 13) = 5.7, p < .016; KCCQ physical limitation subscale, F(2, 52) = 3.4, p < .039; and functional capacity (336 ± 18 vs 388 ± 20 m, p < .05) among the EX/CCT participants. The underlying mechanisms that EX and CCT targets and the optimal dose that leads to improved outcomes are needed to design effective interventions for this rapidly growing population.
Heart failure (HF) is increasing by epidemic proportions in the United States with over 6.5 million individuals currently diagnosed, and approximately 960,000 new cases identified yearly (Benjamin et al., 2017). Among older adults, HF is the most common reason for readmission within 30 days of hospital discharge and the most costly Medicare expenditure (Heidenreich et al., 2013). Cognitive impairment (CI) is a prevalent comorbidity in HF which can have devastating effects on the ability to carry out HF self-care behaviors (Lovell et al., 2019). The cognitive decline observed in HF is more pronounced than with normal aging, but lacks the symptoms of dementia, such as impaired judgment, reasoning or difficulties performing activities of daily living. CI is established to contribute to adverse clinical outcomes, increased rehospitalizations, and higher mortality rates in persons with HF (Gelow et al., 2015).
Self-care is a naturalistic decision-making process used by individuals to make behavior choices about symptom monitoring and treatment adherence that preserve physiological stability (self-care maintenance) and responding to symptoms when they occur (self-care management). These self-care behaviors are influenced by the confidence or self-efficacy an individual has to perform them (self-care confidence) (Riegel et al., 2004, 2007, 2011, 2016). Participation in effective self-care, along with providers following the recommended HF guidelines, are essential for successful disease management and optimal quality of life (QOL; Yancy et al., 2017).
Few studies have evaluated interventions to improve self-care in patients with HF and co-existing CI. Davis and Colleagues (2012) evaluated a targeted self-care teaching intervention on HF self-care and knowledge in 125 patients with HF and myocardial infarction (MCI). They reported improved knowledge among the intervention participants, but self-care remained poor as indicated by Self-care in Heart Failure Index (SCHFI) subscale scores below <70%; hospital readmission rates were unchanged (Davis et al., 2012).
Other studies evaluating interventions to improve cognitive function have used aerobic exercise (Alosco et al., 2014; Gary et al., 2019; Stanek et al., 2011; Tanne et al., 2005) or computerized cognitive training (Pressler et al., 2011, 2015). The cognitive benefits of aerobic exercise in older adults are well-established. Only recently have the benefits of exercise to improve cognitive function in HF been investigated. Three of the 4 previous exercise studies conducted in HF that included a cognitive outcome were conducted in cardiac rehabilitation settings using 36 aerobic exercise sessions over 12 to 18 weeks but none of these included computerized cognitive training (CCT) or self-care measures (Alosco et al., 2014; Stanek et al., 2011; Tanne et al., 2005). Our work is the only home-based aerobic exercise and CCT program reporting cognitive outcomes in HF which showed improved verbal memory (Gary et al., 2019).
The efficacy of CCT was reviewed in a recent meta-analysis, which reported cognitive benefits in both cognitively healthy older adults and in those with mild CI (Hill et al., 2017). Among persons with HF, improved delayed recall and working memory (Pressler et al., 2011, 2015), and verbal memory (Gary et al., 2019) have been reported. While CCT has been found to be beneficial for enhancing cognitive function in older adults, its benefit in HF remains inconclusive due to the small, under powered samples in previous studies and the lack of standardized cognitive testing (Kua et al., 2019).
Evidence suggests that the combination of exercise and CCT may act synergistically for greater cognitive benefit than either strategy alone (Theill et al., 2013; Barcelos et al., 2015). General cognitive function (Shatil, 2013), executive function (Barcelos et al., 2015; Heill et al., 2013), processing speed (León et al., 2015), and memory performance (Zhu et al., 2016) have been shown to benefit more from a combined approach. In a recent meta-analysis (Zhu et al., 2016), the effects of CCT and physical activity interventions on cognitive function were evaluated in healthy older adults. The analysis included 20 randomized controlled trials (RCTs) and 2,667 participants which showed a significant effect for combined cognitive and physical activity versus (active or passive) control groups. Interventions reporting the use of combined exercise and CCT are sparse and none to our knowledge except our preliminary work have been conducted in HF.
The primary aim of the study (previously published) was to evaluate the efficacy of a 12-week aerobic exercise and CCT intervention on neurocognitive outcomes compared to exercise alone or an attention control usual care group receiving a stretching and flexibility program (Gary et al., 2019). We reported improved verbal memory among participants in the combined aerobic exercise and cognitive training group, with no significant changes observed in the exercise only or attention control groups from baseline to 3 months. In the current study, we hypothesized that participants in the combined aerobic and cognitive training program would also have the greatest improvement in HF self-care behaviors, disease specific QOL, and functional capacity compared to an exercise only (EX) and stretching and flexibility attention control groups (AC) from baseline to 3 months.
Method
Study Design
A three-group, pre–post randomized controlled design was used to evaluate intervention efficacy with data collected at baseline and 3 months. The protocol was approved by the Institutional Review Board, and all participants provided written informed consent before participation. Recruitment and data occurred from December 2014 to October 2016 in the southeastern United States at three large HF clinics affiliated with an academic health science center. After baseline measurements, participants were randomized using a table of random numbers prepared by a statistician. Participants were assigned to receive a Usual Care Attention Control Stretch and Flexibility Program (UCAC, n = 19), an exercise only intervention (EX, n=29), or exercise + cognitive training (EX/CCT, n = 21) for 3 months. Data collection was conducted by trained research assistants (RAs) blinded to group assignment.
Participant Eligibility
Participants were screened for eligibility using an electronic medical record. To be eligible, participants had to be ambulatory, between 40 and 75 years of age, have a left ventricular ejection fraction (LVEF) ≥ 10% documented within the last year by echocardiogram, cardiac catheterization ventriculography, or radionuclide ventriculography, stable New York Heart Association (NYHA) class II-III HF, receiving medication therapy for HF according to the American College of Cardiology/American Heart Association recommendation guidelines (Yancy et al., 2017) for at least 3 months prior to study enrollment. Participants also had to be English speaking and live independently. In addition, participants had to score ≤ 26 on the Montreal Cognitive Assessment (MoCA) (Nasreddine et al., 2005) and have access to a computerized device for cognitive training. Exclusions included those with unstable angina or hypertension, end-stage organ failure, and any identified or diagnosed neurological or psychological disorder that would interfere with the ability to walk or cognitive function.
Intervention
Exercise only program
A home-based aerobic exercise program was used; participants were instructed to walk 3 times per week for 12-weeks at moderate intensity. Dose-specific exercise was based on maximum heart rate (HR) obtained during a maximal effort treadmill test. Each participant was provided a target heart rate (THR) of 60% to 70% of maximum HR achieved on the cardiopulmonary exercise test (CPET) for the exercise prescription using the HR reserve (HR maximum—resting HR) x % intensity) + resting HR (Karvonen et al., 1957) calculation. A home-visit by the research team after baseline testing was conducted to provide instructions on the Polar HR monitor and pedometer (Polar HR monitor [Polar, USA; https://www.polarusa.com]; Omron pedometer) for tracking THR and steps, respectively. In addition, the participant received instructions on how to evaluate their exertion level using the Borg 60-20 scale (Borg, 1982) and complete a written walking log to document adherence to the intervention. Under weekly telephone supervision by a member of the research team, participants began the walking sessions at 60% of THR for 30 min, increasing to 70% intensity and 45 min duration over the next 4 weeks. Participants were followed by telephone for the remainder of the 12 interventions.
Combined exercise and computerized cognitive training (EX/CCT) program
The same aerobic exercise walking instruction was provided to the combined EX/CCT group as discussed above in one home-based session. The Intensive Auditory Training program (formally Brain Fitness) (Posit, San Francisco, CA detailed below) computerized program was used for the cognitive training component (Posit Science). The program is based on the principles of neuroplasticity and is designed to enhance sensory integration and strengthens capability for encoding information. The Intensive Auditory program is designed to be completed over 8 weeks in 40 one-hour sessions (Pressler et al., 2011, 2015). In a second home visit, research staff provided training and demonstrated how to use the CCT program with a return demonstration provided by the participant. In the current study, all participants were provided free access to the CCT program and completed the computerized program at home at a time convenient for them.
Usual Care Attention Control
Stretching and flexibility movements
Education, flexibility, and stretching protocols were provided to controls as a time-equivalent, placebo exercise condition. Participants received a home visit to review the standardized HF educational materials. The flexibility and stretching movements were also demonstrated by the research staff during the home visits with a return demonstration by the participant. In pilot evaluations, the stretching and flexibility movements had high satisfaction and were well received but were not strong enough to influence study outcomes (Gary et al., 2018). The attention control stretching and flexibility program was delivered within 2 weeks after baseline measures were completed and participants were instructed to complete the program 2 to 3 times per week over the next 12 weeks. Weekly telephone calls were made for 12 weeks to discuss educational materials and to answer questions about the stretching and flexibility movements.
Adherence
To be 100% adherent for the exercise sessions, participants in the EX groups were required to document walking three times per week at the prescribed intensity/duration on the exercise log. Polar HR monitors and pedometers were also used to objectively document exercise intensity (i.e., maximum HR) and rate of perceived exertion [RPE] achieved using the Borg Scale, walking duration, adherence and progression. Participants completed walking logs and received telephone calls weekly to discuss their walking progression.
Adherence for the Brain Fitness intervention was evaluated by the number and duration of sessions automatically logged when the participant accessed the program. Time to complete the entire program was pre-established by Posit Science to be 2,310 min (Posit Science). Participants were considered adherent if they completed 80% or 1,848 min of the program during the 12-week intervention period which was approximately three times per week for 180 min total.
Measures
Socio-demographic and clinical characteristics were validated using the electronic medical record (Table 1). The Charlson Comorbidity Index (Charlson et al., 1987) was used to assess the number and severity of comorbid diseases. HF etiology and type were validated in the participant’s medical record.
Baseline Sociodemographic and Clinical Characteristics.

Note. BDI = Beck Depression Inventory; UCAC = usual care attention control; EX only = exercise only; EX/CT = exercise and cognitive training; NYHA = New York Heart Association functional class; LVEF = left ventricular ejection fraction; ICD = implantable cardiac device; BMI = body mass index; ACEI = angiotensin converting enzyme inhibitor; ARB = angiotensin receptor blocker; MoCA = Montreal Cognitive Assessment; Peak VO2 = peak oxygen consumption; 6MWT = 6-minute walk test.
Cognitive screening assessment
Prior to enrollment, participants were screened for global cognitive function using the MoCA (Nasreddine et al., 2005). Validity of the MoCA has been previously reported in HF patients (Pressler et al., 2015). Scores range between 0 and 30, with a score of 26 to 30 considered normal or no MCI present. In the current study, participants were enrolled if they had a MoCA score of ≤ 26 and met other eligibility criteria.
Aerobic and functional capacity
A maximal symptom-limited modified Balke Treadmill Test was used to determine aerobic capacity. The modified Balke is a well-tolerated exercise test that maintains treadmill speed at 3.0 mph while advancing incline to increase workload and employed with no adverse events in our work with hf participants (Balke & Ware, 1959). Peak oxygen consumption (VO2peak) was obtained using continuous gas exchange according to the American Heart Association guidelines (Gibbons et al., 2002). The 6-minute walk test (6MWT) a measure of functional capacity was administered using a standardized protocol where participants walked back and forth on a 100-foot flat, level hall-way, a change of 50 m is considered clinically significant (Rasekaba et al., 2009).
HF self-care
Self-care was measured using the SCHFI v.6.2 which is a 22-item self-report instrument that includes three sub-scales that measure the three components of HF self-care: maintenance, management, and confidence (Riegel et al., 2009; Vellone et al., 2013). The self-care maintenance subscale is composed of 10 items that assesses the ability to monitor symptoms and adherence behaviors utilized to avoid worsening symptoms or a HF exacerbation (i.e., dietary salt intake and medications). The self-care management subscale evaluates the ability to recognize symptoms and the initiation and evaluation of treatment in response to symptoms (i.e., take an additional diuretic, consult provider, and reduce fluid intake). The self-care confidence subscale has six items to evaluate patients’ perceived ability to engage in each phase of the self-care process (e.g., preventing symptom onset, and recognizing symptom changes). Raw scores are standardized from 0 to 100 with higher scores reflecting better self-care. A score of ≥70 on each subscale is recommended as the minimum level of self-care adequacy. The SCHFI is widely used and has undergone extensive psychometric testing and revision with excellent validity and reliability reported (Riegel et al., 2009; Vellone et al., 2013). A change in a subscale score of more than one-half of a standard deviation is considered clinically relevant.
Disease specific QOL
The Kansas City Cardiomyopathy Questionnaire (KCCQ) is a 23-item, self-report outcome measure that quantifies physical function, symptoms (frequency, severity, and recent change), social function, self-efficacy, and knowledge for individuals with HF. Scores range from 0 to 100, with higher scores reflecting less disease burden, symptom severity, and better QOL. The KCCQ overall summary score includes the scales for physical limitations, symptom summary, social limitations, and QOL (Green et al., 2000). The KCCQ also provides an evaluation of the magnitude of clinical change (KCCQ overall summary scores: small clinically important change, 5 points; moderate change, 10 points; and large change, 20 points or greater) (Spertus et al., 2005).
Data Analysis
Baseline descriptive statistics were computed for the socio-demographic, clinical, and study variables and compared across study groups. Analysis of variance (ANOVA) and chi-square tests were used to examine differences between the three study groups on all demographic, clinical, and outcome variables. Linear mixed-effects models were used for testing preliminary efficacy of the intervention on the outcomes of interest over time. Separate models were fitted for individual outcomes to assess group, time, and group by time interaction effects, where a significant group by time interaction is indicative of a differential effect of the intervention across groups. Analyses were first unadjusted for any baseline characteristics and then adjusted for comorbidity due to baseline differences between groups. Pairwise differences between time points were used to evaluate within group changes from baseline to 3 months and Bonferroni correction was used for multiple comparisons. Missing data patterns were assessed at each time point. An intent to treat analysis was used for all data analysis. Analyses were performed using version 24 of SPSS software.
Results
The sample comprised 69 participants who completed baseline assessments. A total of 952 individuals were screened for study participation, 807 were deemed ineligible, 76 declined, and 69 were enrolled (Figure 1). Participant flow from baseline to 3 months is illustrated in Figure 1. Baseline sociodemographic and clinical characteristics are presented in Table 2. The groups were comparable at baseline with the exception of higher comorbidity in the EX only group which was controlled as a covariate in the analysis. The mean age of the sample was 61 ± 10, the majority were female (N = 37, 54%), African American (N = 38, 55%), and most had some college education; mean 14 ± 3 years of education (range = 8–22 years). Clinically, the majority were NYHA class II (N = 38, 55%), LVEF% mean was 35 ± 15 with a range of 10%–65%. LVEF, and peak V02peak (r = -0.42, p = .002) were significantly correlated at baseline.
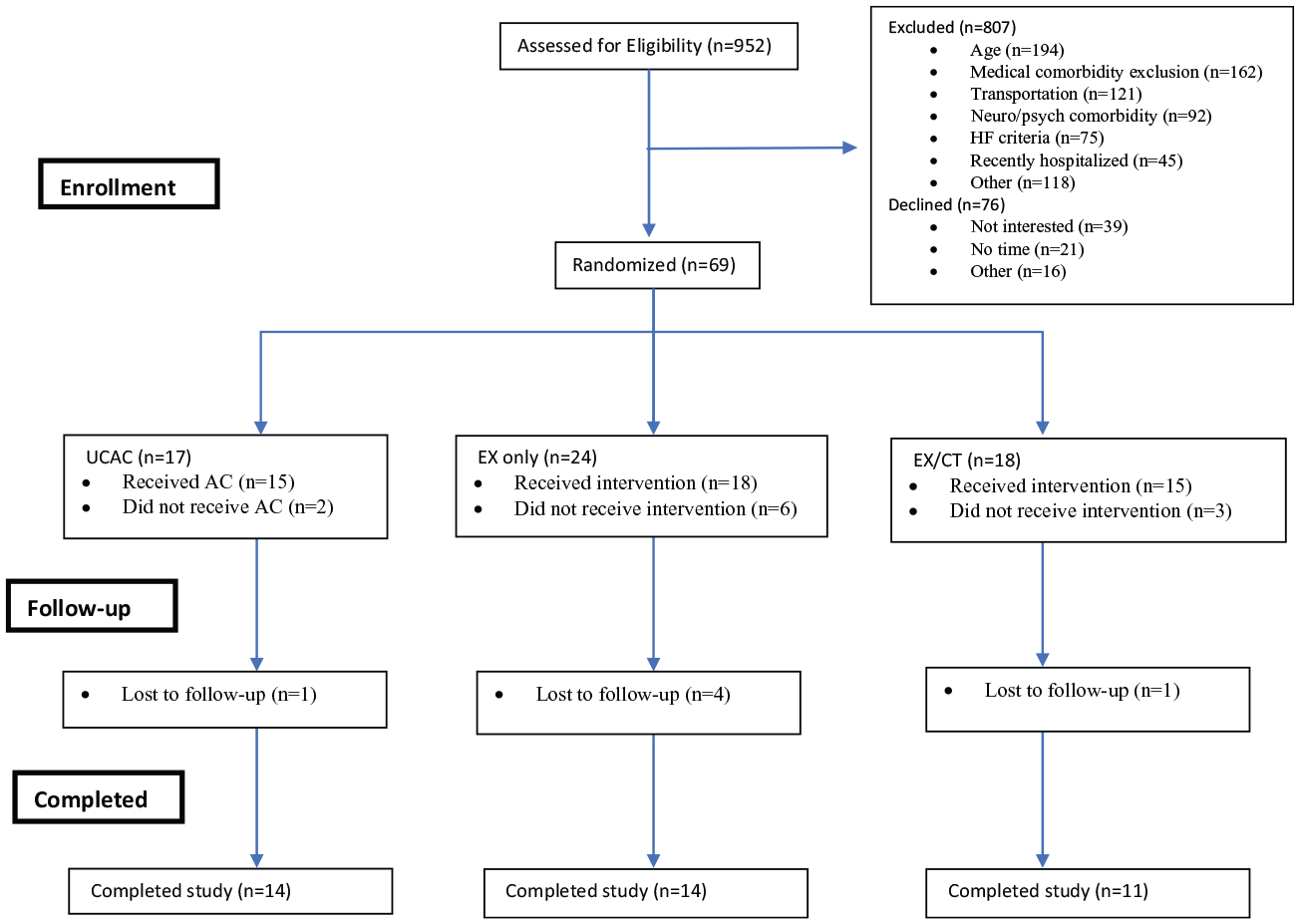
CONSORT flow diagram.
Quality of Life, Heart Failure Self-Care, Aerobic and Functional Capacity Outcomes From Baseline to 3-Months.

Note. RM ANOVA = analysis of variance with repeated measures; BL = baseline; UCAC = usual care attention control; EX only = exercise only; EX/CT = exercise and cognitive training; KCCQ = Kansas City Cardiomyopathy Questionnaire; SCHFI = Self Care Heart Failure Index; Peak V02 = peak oxygen consumption; 6MWT = 6-minute walk test.
A mean MoCA score of 21 ± 3 (range = 13–26) indicated that many participants were experiencing mild to moderate CI at baseline with scores ≤16 indicating the presence of possible dementia. In the current sample, 29 (42%) participants scored ≤ 20 on the MoCA.
HF Self-Care
There was a significant effect of the EX/CCT intervention at 3 months on the SCHFI self-management subscale, F(2, 13) = 5.7, p < .016; improvement also occurred in the EX only group (+4-points) but was not statistically significant. Self-care management scores significantly declined in the AC group from 87 to 70 (p < .009). There was a clinically meaningful increase of 5-points on the self-care maintenance subscale in the EX/CCT participants compared to no change in the EX only group and scores slightly increasing in the AC (+2 points) group. Overall, the two intervention groups showed greater improvement in self-care management and maintenance compared to the AC participants.
Disease Specific QOL
There was a significant 13-point increase in the KCCQ physical limitation subscale, F(2, 52) = 3.4, p < .039, and a 5-point increase in the overall summary scores among the EX/CCT participants. There was also a loss of 12-points on the KCCQ physical limitation subscale among the AC group which suggests they perceived their physical function to worsen over 3 months and was associated with a decline in the 6MWT distance. In addition, although not statistically significant, there was a nine-point increase on the physical limitation scale among the EX only participants. Both intervention groups had greater improvement in QOL compared to the AC group.
The mean V02peak was 16.8 ± 5 kg/mL/min with no significant group differences occurring from baseline to 3 months, F(2, 42) = 0.13, p = .877. The intervention had a positive effect on 6MWT distance at 3 months, F(2, 52) = 3.3, p =.036, as indicated by larger increase in the intervention groups compared to the UCAC group over time.
Exercise Adherence Rates
There were no significant differences in adherence rates for both exercise groups. Participants 100% adherent or walked a minimum of three or more days per week was 60% in the EX/CCT group and 27% were moderately adherent walking a minimum of two times per week. In the EX only group, the adherence rate was slightly higher with 64% walking a minimum of three or more days per week and 24% were moderately adherent walking a minimum of two days per week.
CCT Adherence Rates
Seventeen out of 22 participants participated in the Brain Fitness exercises. Of this number, 9 (41%) were 80% adherent completing an average of 3 days and 80 min total per week. Three participants were less than 80% adherent and 5 did not complete any of the Brain Fitness games.
Discussion
The current study examined the effect of a combined aerobic exercise and computerized cognitive training intervention on self-care behaviors, functional capacity, and disease-specific QOL in 69 participants with stable NYHA class II and III HF over a 3-month period. At baseline, all study participants had inadequate self-care management (<70). There was significant improvement among the combined EX/CCT group in self-care management with clinically meaningful improvements among those in the EX only group. The EX/CCT group also showed greater improvement in self-care maintenance. These findings have important clinical implications since self-care management activities such as identifying and appropriately responding to worsening HF symptoms are critically important to avoid acute exacerbations and subsequent hospitalization.
Neurogenesis and neuroplasticity are means for the brain to recover from poor perfusion and oxygen deprivation such as that occurring in HF (Vogels et al., 2007). It is plausible that exercise and cognitive training target different mechanisms in the brain and in part explain why combination therapy may be more effective. Future research to test different exercise modalities and intensity are also warranted to identify which types of training programs are superior and may lead to better cognitive outcomes. Routine evaluation of cognitive function using simple screening tools such as the MoCA (Nasreddine et al., 2005) may assist providers to identify cognitive changes that may signal a person’s difficulty in practicing effective self-care.
Patient reported outcomes are important and have been shown to predict hospitalization and death in HF (Kelkar et al., 2016). The KCCQ includes a subscale for physical limitations, which quantifies from the patient’s perspective the extent to which HF symptoms influence functional capacity such as walking one-block or climbing stairs. In the current study, EX/CCT participants perceived these functional limitations to be substantially declining at 12-weeks which was supported by a significant increase in 6MW distance. A 5-point change in KCCQ overall score and 13-point increase on the physical limitation subscale was associated with a 52-meter improvement in 6MW distance in the EX/CCT group which is considered clinically significant (Myers et al., 2006). Disease-specific measures such as the KCCQ are more sensitive to clinical changes and are particularly applicable when used in clinical practice settings (Yee et al., 2019). Most practice settings have limited time and resources so questionnaires that are brief, easy to administer, and interpret are appealing. The 23-item KCCQ requires less than 10 min to complete and the more recent, 12-item short version, takes only 2 to 3 min without losing its validity, reliability, or prognostic capabilities (Spertus & Jones, 2015). Studies support that clinicians often underestimate functional capacity among patients (Kelkar et al., 2016). Health status changes can be quantified, monitored over time, and interpreted using the KCCQ. For instance, a change in score may indicate a medication adjustment is needed, identify if symptoms have worsened or if other therapies should be initiated.
The prognostic ability of the 6MW distance in HF is well established with 300 m or less associated with higher disease burden, higher rates hospitalizations, and mortality (Flynn et al., 2012). In the current study, 43% of the participants had a 6MW distance of 300 m or less which is lower than previously reported (Forman et al., 2012). The reason for the lower 6MW distance may reflect demographic differences from previous studies that are predominately White males with fewer comorbidities. Our population included a higher proportion of African Americans who were female, obese who had 3 or more comorbidities which may have negatively influenced their functional capacity. The 6MWT is a simple, inexpensive, and objective test that is safe in stable persons with HF in outpatient settings and may be useful for risk stratification.
An interesting finding was that all three-study groups had adequate self-care confidence at baseline, which did not significantly change over the study duration. This is consistent with Freedland et al., (2015) who also showed no increase in self-care self-confidence among participants with HF exhibiting adequate confidence at baseline. Self-care confidence or self-efficacy was first thought to be a central component of self-care but is now thought to mediate and/or moderate self-care outcomes (Riegel & Dickson, 2008). Several recent secondary analyses by Vellone et al. (2016) have shown that self-care confidence mediates the relationship between cognition and self-care behaviors (Vellone et al., 2015). Future studies are warranted to examine longitudinal relationships between cognitive function, high and low levels of self-efficacy on performance of self-care activities and their influence on clinical outcomes.
Strengths and Limitations
Findings from the current study extends research in HF to a broader population of African American females with lower global cognition and functional capacity than previously reported. Previous studies have included greater numbers of Caucasian males with higher global cognition and functional capacity (Pressler et al., 2011, 2015; Tanne et al., 2005). Importantly, none of the participants had been previously screened for cognitive decline prior to enrolling in the study but joined the study because they perceived their memory and ability to recall information had substantially declined.
The sample size was small and not adequately powered to determine group differences; larger trials are needed to determine whether these intervention strategies are clinically beneficial. Among individuals with low global function and low literacy, cognitive reserve may have been too limited to successfully engage in the Intensive Auditory Training program. Some of our participants had limited use of computers which also may have influenced their ability and motivation to engage in this type of intervention. Although we used a placebo exercise condition that included stretching and flexibility movements, a sham computer program would have better equalized the intervention groups in relation to the CCT intervention. MoCA scores have been shown to be lower among African Americans and may not have been as reliable to measure global cognitive function in the current sample (Rossetti et al., 2017).
In conclusion, our findings indicate that a combined EX/CCT may improve self-care management, QOL, and functional capacity in persons with HF. Because there was no significant change in the EX only group, computerized cognitive training may be a more effective intervention strategy and needs further testing with and without an exercise component in an adequately powered sample. The reasons for higher self-care management and QOL scores in the EX/CCT group are unclear but may reflect improvement in functional capacity. The prevalence of HF is anticipated to rise as the population ages, which necessitates that the management of HF includes other comorbid geriatric conditions such as CI and dementia (Heidenreich et al., 2013).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported in part by the National Institutes of Health National Institute of Nursing Research grant no. 1P30NR014134-01 (PI-D. Waldrop), Advancing Translational Sciences of the National Institutes of Health under award no. UL1TR000454 (D. Stephens). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.