
Abstract
Older adults’ preference to age in place and health systems’ commitment to cost-effective quality care has set the stage for a growing interest in home-based primary care (HBPC). The objective of this study was to explore what patients and caregivers value about HBPC and what modifications could improve its value. Semi-structured individual interviews (n = 20) were audio-recorded, transcribed, and coded for themes. Four themes emerged: (a) HBPC offers peace of mind because patients can access care without leaving the home and can reach the primary care team at all hours, (b) HBPC supports aging in place by providing in-home care, (c) HBPC supports provider rapport building because of the intimate setting and continuity of care, (d) HBPC patients and caregivers have significant nonmedical needs. Findings suggest that teams developing or expanding on HBPC programs should prioritize access to providers, rapport building with patients and families, and supporting patients’ and caregivers’ nonmedical needs.
Introduction
Approximately two million older adults in the United States are homebound, primarily as a result of functional limitations (Ornstein et al., 2015). These functional limitations make traveling to a medical office almost impossible, limiting access to primary medical care (Ornstein et al., 2015; Qiu et al., 2011; Simonsick et al., 1998) and commonly resulting in fragmented and costly medical care (Congressional Budget Office, 2005; Komisar & Feder, 2011). Home-based primary care (HBPC) provides dependable access to primary care for people who are homebound by bringing medical care to patients’ homes. HBPC programs are heterogenous in their design and services, but share a comprehensive, multidisciplinary approach to care (Leff et al., 2015). Prominent health care systems have started to create new HBPC programs or expand on existing HBPC programs, in part a reaction to older adult preference to age in place, and in part a result of studies demonstrating HBPC cost-effectiveness (de Jonge et al., 2014; Edes et al., 2014; Figueroa et al., 2017; Kinosian et al., 2016; Schuchman et al., 2018).
Prior research suggests that homebound individuals are satisfied with care received through HBPC programs (Shafir et al., 2016; Smith-carrier et al., 2017). In previous studies, HBPC patients reported strong bonds with the HBPC interdisciplinary care team, reported that HBPC was their only source of accessible care, and reported valuing timely, skillful, and affordable care provided by the HBPC team (Edes et al., 2014; Shafir et al., 2016). Although existing studies have demonstrated that HBPC provides a patient-centered care experience, there is scant research on the specific program elements and characteristics of HBPC that patients most value, and on service elements that would provide additional value to patients and caregivers if added to HBPC programs. The objective of this study was to explore what patients and caregivers value about HBPC and what modifications to HBPC could improve its value.
Method
Study Design, Setting, and Participants
We recruited older adult patients and their informal caregivers from the Johns Hopkins Home-Based Medicine (JHOME) program. JHOME provides primary care in the home to homebound older adults in urban and suburban neighborhoods in and surrounding Baltimore city. The JHOME care team consists of a physician medical director, two nurse practitioners, a registered nurse, a social worker, and two patient services coordinators. The JHOME team served 359 patients in 2019.
JHOME patients and caregivers of patients who received care in the past year were eligible for inclusion in the study. Any family member or friend identified as a regular caregiver of a patient, either by a patient or a member of the care team, was eligible to participate. We excluded individuals who did not speak English, and those who lacked capacity to participate in interviews due to cognitive or medical limitations. The Johns Hopkins Medicine institutional review board approved the study.
Enrollment
A research assistant mailed study information to patient households with an option to opt out of the study. A research assistant then called patients and caregivers who had received letters and who had not opted out, and invited them to participate. Participants completed a written consent prior to enrollment. Each participant who completed an interview received a US$25 gift card. A research assistant unaffiliated with the program managed recruitment and conducted all interviews. The research assistant is a registered nurse and a doctoral student who has worked with older adults in home and community-based settings for more than a decade. She has had formal training in interview facilitation and qualitative methods, including taking three graduate-level qualitative research courses. We used purposive sampling to enroll approximately an equal number of patients and caregivers. We enrolled participants until we reached data saturation based on redundant findings in initial data analysis.
Data Collection and Analysis
We developed a semi-structured interview guide (see Supplemental Table 1) that focused on understanding patient and caregiver values and preferences related to HBPC care. Questions and probes in the interview guide were grouped into domains including access, scheduling, medical services, nonmedical services, priorities, technology, care coordination, additional input, and demographics. The interview guide included questions about the person’s current experience and about the person’s ideal-state experience with HBPC. For example, in the medical services domain, we asked both about what medical services the patient currently receives from the HBPC program and about what additional or different medical services they would receive in an ideal HBPC program.
One study team member completed all the interviews from October to December 2018. Interviews lasted an average of 42 min (ranging from 26 to 90 min). All interviews took place in patients’ homes. Most interviews were completed with only the interviewer and interviewee in the room, but in a few cases, that was not possible due to the layout of the home or due to a caregiver’s responsibilities for monitoring a patient’s safety. All interviews were audio-recorded and transcribed verbatim.
We used both inductive and deductive coding techniques. First, three of our study team members reviewed two of the study transcripts, and each coded the transcripts independently without a codebook. Then, each of the three study team members developed a draft codebook based on their findings from those two transcripts. The study team met and compared draft codebooks and collaborated to combine them into an initial codebook. The agreed-upon codebook included codes, subcodes, and exemplar quotes/explanation for each code and subcode. A fourth study team member reviewed and revised the codebook for clarity. Next, two study team members used the codebook to code an additional study transcript. The study team reviewed their coding and made minor revisions to the codebook at that time, including adding a new code that had not been included based on the content of the first two transcripts. Then, two study team members each coded half of the remaining transcripts using the revised codebook.
During the coding process, the two study team members who coded the transcripts met weekly to discuss memos taken during coding, decide if new codes were required, discuss data saturation, and conduct reflexive dialogue regarding each researcher’s beliefs and experiences. The codebook was sufficient for all the remaining transcripts and no further edits were required. After all transcripts had been coded, the study team met to review coded transcripts and the distribution of codes. The team utilized graphical displays and group dialogue to conceptualize connections between codes. The team synthesized the codes into categories and the categories into themes. In keeping with qualitative research best practices, themes were identified based on the research team’s reflections on participants’ shared experiences, rather than on a quantification of the qualitative transcripts (Merriam & Tisdell, 2016).
Results
Table 1 depicts demographic characteristics of the study participants. Two thirds of patients interviewed were female. Just more than half of caregivers interviewed were male. The majority of both patients and caregivers self-identified as non-Hispanic White. Most of the caregivers interviewed were the adult children of patients receiving HBPC services. None of the caregivers who participated in the study were caregivers of patients who participated in the study. We identified four major themes related to the participants’ perspectives on the value of HBPC services.
Demographic Characteristics of Patients and Caregivers.
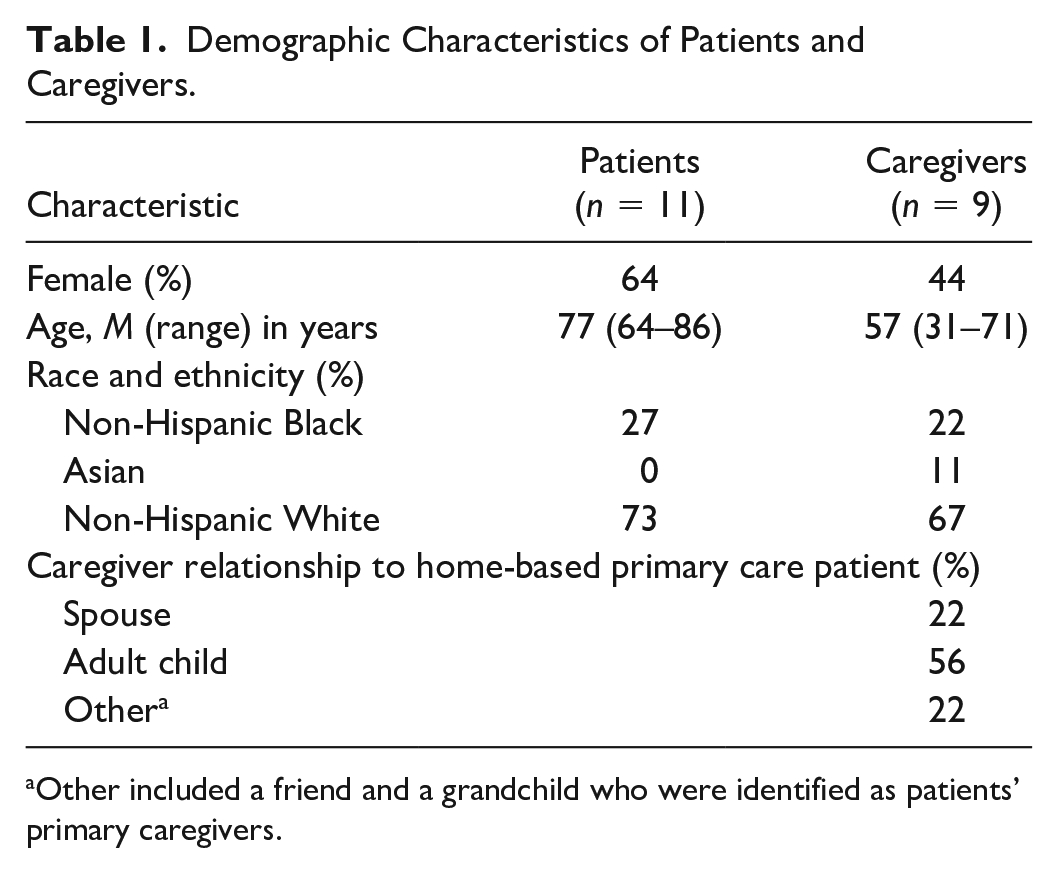
Other included a friend and a grandchild who were identified as patients’ primary caregivers.
Theme 1: HBPC Offers Peace of Mind
Both patients and caregivers consistently reported that HBPC provides relief and peace of mind. Having clinicians come to their homes relieved participants of the major challenge of accessing primary care services. Caregivers described the stress of helping their loved ones navigate stairs and get in and out of vehicles and medical offices, before enrollment in HBPC. One caregiver (CG12) said, Getting her to the car, getting her in and out of the car, into the doctor’s office– oh, it’s just so convenient that they come here . . . I mean, every time they come out, that means I don’t have to get Mom in a car. I don’t have to—it’s hard. It got really hard.
A patient (PT08) shared, The program’s great. It’s been a blessing that I don’t have to try to get out of here and get my husband to take me down the steps in a wheelchair to get me out to get me to a doctor. That’s been a blessing.
Participants also described the relief that comes from being able to reach someone in the HBPC practice any time of day, any day of the week, with questions and concerns. A caregiver (CG10) shared, “. . . I’m able to call them, like, any time, you know, after hours or on the weekends. In case I had a question or something, and she’s sick and I don’t know what to do . . .” Participants often described their “before and after” experiences: before enrollment in HBPC, they had trouble reaching health care providers, getting responses to questions, and resolving issues without going to the emergency department or a provider’s office. HBPC resolved those issues and brought them peace of mind. One participant remarked (PT15), But after I got in the program with them they gave me the number to call them, you know, to keep from dialing 911 and going to the hospital. Because if she didn’t give me that number . . . I would’ve dialed 911 and went to the hospital.
Participants expressed mixed opinions on the potential use of video-based visit technology to enhance access. They generally felt that access to the team by telephone was an important contributor to peace of mind and that “phone visits” were acceptable if used in addition to in-person visits.
Theme 2: HBPC Supports Aging in Place
Participants explained that a primary reason they value HBPC is because it helps them to be able to stay at home and age in place rather than have to relocate to a nursing home. All participants expressed a desire to age in place (or to support their loved one to age in place). Participants described negative experiences associated with short-term rehabilitation stays or long-term stays in skilled nursing facilities. Said one caregiver (CG11), . . . If she were to transition into a nursing home, it would be negative for her. She would kind of give up on life at that point. So more services that can help keep her in the home and kind of thriving until she’s really called to end of life, that would be helpful.
Participants expressed that HBPC was valuable in large part because it supported their goals related to aging in place. Said one caregiver (PT09), “No, I don’t want to send her in there. We can much better take care [of her] at home.”
Theme 3: HBPC Supports Provider Rapport Building With Patients
Participants explained that HBPC is uniquely able to support patients to build rapport with providers because of the intimate setting of care and the consistency in team members who provide care. Said one caregiver (CG16), “I think being home she feels more comfortable. She feels, you know, at peace with everything, and I think she’s able to share, you know, what’s going on with her feelings and everything.” Participants described interactions with HBPC providers that demonstrate that the provider was familiar to them, remembered them, made nonmedical conversation with them, and seemed to care about them. Participants consistently expressed value associated with seeing the same provider on a regular basis and developing a relationship with that provider. For example, one caregiver described her father’s relationship with his provider and how much he looked forward to visits with that familiar provider. A patient explained that she would never want to switch to a different primary care program because she likes the particular people who visit her from the HBPC team. Participants consistently reported that rapport with the team was a primary reason they valued the program. In the words of one patient (PT17), “They’re nice. They ask you good questions . . . As a matter of fact, they’re really interested in you. That’s good enough for me.”
Theme 4: HBPC Patients and Caregivers Have Significant Nonmedical Needs
Patients and caregivers described significant nonmedical needs, that is, long-term services and supports, including needing support with personal care, household assistance, caregiver respite, transportation, home modifications and equipment, and addressing social isolation. Participants were appreciative of nonmedical services that the HBPC team was able to connect them to, such as describing how staff helped them identify useful community resources. One patient (PT03) said of the team’s social worker, “She is the type that she’ll get right in and if she has to go to social services for you whatever it takes she’ll do it . . . Well, she got me my food stamps.” Participants described “before and after” scenarios of not having support with nonmedical needs prior to enrollment in HBPC and satisfaction after enrollment with HBPC support through referral to nonmedical services.
Participants often said that they did not expect HBPC to assist with nonmedical needs, but that it would add value to the program if nonmedical services were available. Caregivers consistently reported a desire for HBPC to provide nonmedical respite services. One caregiver (CG09) shared, Two years I don’t sleep in my room, because I have to watch her . . . I know it’s her disease and everything . . . but . . . if one or two days I can get somebody in the nighttime, I can take a good sleep. Like, at least, relax and sleep in my own [bed]—that’s the only thing.
Participants also expressed a desire to have additional support with personal care. A patient (PT03) reported, “I haven’t been able to wash my hair for over a month because it’s not the right kind of outfit in the bathroom. And I cannot stand up and bend over for my daughter to do it.” A caregiver (CG19) described his frustration with not having assistance finding and paying for personal care and medical supplies for his wife, So this is something very important for the organization who will take care of the ill people at home. You have to tell me how I will get the supplies.—how are we going to, you know, pay for these supplies?
Both caregivers and patients described substantial nonmedical needs and identified this as a potential service element that could add value to HBPC programs.
Discussion
In this study, we explored what patients and their caregivers value about HBPC and what modifications to HBPC could improve its value for them. Participants valued not having to leave the home for care and being able to reach providers at all hours to obtain guidance about their care. Participants also valued the opportunities to age in place, the provision of continuity in primary care, and rapport building with providers. Participants valued the HBPC team’s support with navigating nonmedical resources, and expressed additional unmet nonmedical needs that, if addressed by the HBPC, could add to its value.
Lack of access to medical care can be particularly stressful for homebound individuals and their caregivers because of difficulty leaving the home and the complexity of care needed to manage frailty and multiple chronic conditions. Participants in our study expressed relief at being able to access clinicians, including after hours, and being able to request a home visit or a provider phone call whenever they were concerned about a medical issue. This report of an overall highly positive experience and valuing of access is consistent with previous studies of the experiences of HBPC patients (Shafir et al., 2016). Patients and caregivers described building rapport with HBPC team members as an element of the program that added value for them. This connection may be more important in the home environment than in an ambulatory setting due to the deeply personal nature of a home visit and the fact that homebound older adults may not have many choices of medical providers who can provide care in their homes (Yao et al., 2016). When asked what they liked most about the care they receive through HBPC, participants most consistently discussed the relief of receiving care at home and the caring personalities of the providers. These findings were consistent with past research in which HBPC patients have reported relief and satisfaction as a result of receiving home-based services (Shafir et al., 2016). Making efforts to limit providers’ panel sizes, developing team-based and medical home approaches that emphasize continuity of care, and providing after-hours support could improve the value of primary care programs for homebound people and their caregivers.
Participants reported that the HBPC program has supported their (or their loved one’s) ability to age in place, which was a major contributor to the value of the program. Given that the majority of older Americans hope to age in place, HBPC will likely increase in popularity with patients and their families (Schuchman et al., 2018). Consistent with past studies (Wool et al., 2019), participants in this study reported that they had significant nonmedical needs, including caregiver respite care and personal care. Caregivers, including spouses, adult children, grandchildren, and friends, described adjusting their routines, employment, living situation, and finances to accommodate their caregiving responsibilities. Despite their many responsibilities and stressors, the caregivers we interviewed reported wanting to continue providing care to the HBPC patient at home to support their loved one’s ability to age in place. In addition to the need for caregiver respite, participants described several nonmedical needs with which they could use additional support as they age in place. Examples included help with cleaning, transportation to nonmedical appointments, companionship, and personal care. The findings from our interviews support expansion of HBPC models, as HBPC seems to be uniquely positioned to support aging in place for people who are homebound. The findings also support the potential importance of addressing nonmedical needs in HBPC models. Potential strategies include incorporating social workers, community health workers, or home health aides into the HBPC model, or formally partnering with community-based organizations to address HBPC patients’ and caregivers’ personal care and social needs. Past studies support the incorporation of long-term services and supports in HBPC, both as a patient-centered and cost-effective innovation (Leff et al., 2019; Valluru et al., 2019). The addition of long-term services and supports to HBPC models has the potential to reduce institutionalization and to increase opportunity for homebound older adults to age in place (Valluru et al., 2019). For example, research demonstrates that homebound older adults are at heightened risk for falls, as compared with nonhomebound older adults (Casteel et al., 2018). HBPC coupled with enhanced long-term services and supports could mitigate this disparity by addressing both intrinsic fall risks (e.g., medication-related risks) and extrinsic fall risks (e.g., fall hazards in the home).
There are some limitations to this study. All participants in this study were affiliated with one academic HBPC care program that serves a community bordering an urban area so results may not be directly generalizable to other programs. Of all JHOME patients, 63% are non-Hispanic White, 32% are non-Hispanic Black, and <2% are of any Other race. Compared with the national Medicare population, a higher percentage of this study sample was non-Hispanic Black, a slightly lower percentage was non-Hispanic White, and Other races and ethnicities were underrepresented (Kaiser Family Foundation, 2018). The findings from this study may not be representative of the perspectives of patients and caregivers from all racial and ethnic backgrounds. In addition, nationwide, about 40% of family caregivers are male and, in this study, about 60% of caregivers were male. Because male caregivers are often underrepresented in research and services, it may be a strength of this study that male caregivers were overrepresented in the study sample (Accius, 2017). However, caregiver perspectives reported here may not be representative of the national caregiving population. Although the average age of participants in this study (77 years old) is similar to that of the overall JHOME patient population (79 years old), findings may not be representative of homebound people of all ages. In addition, as is true of all research studies, patients and caregivers who agreed to participate may have been different in important ways compared with those who did not agree to participate. Also, participants may have shared less openly because interviews were audio-recorded. To mitigate potential bias due to recording, the research assistant informed each participant prior to the interview that responses would not affect their participation in HBPC services and that only deidentified comments would be shared with the HBPC team. In addition, the research assistant emphasized that the HBPC team was interested in constructive feedback and that critical comments were welcome. Still, some participants may have felt uncomfortable openly sharing their opinions about the program. However, results were generally consistent with other studies of HBPC programs.
Despite limitations, this study offers additional insight into an important issue for older adults, caregivers, and primary care providers. HBPC programs offer critical access to services for a population that would otherwise be unable to receive routine medical care, would need to relocate to a skilled nursing facility, or would undergo significant stress in an effort to access care. Participant experiences in this study reinforce the importance of offering home-based care to older adults aging in place and suggest that HBPC may be an important contributor to preventing unnecessary relocation to skilled nursing facilities.
Themes from this study highlight important considerations for HBPC programs. HBPC programs should prioritize their availability for urgent home visits or telephone communications, and ensure that staff and providers are trained and have the resources to provide consistent, personalized services. HBPC practices may consider other strategies to meet participants’ needs in the home such as collaborating with community organizations to provide nonmedical services. HBPC programs and other programs that support homebound individuals and their caregivers can use this knowledge to incorporate more meaningfully the patient and caregiver perspective in the design and implementation of home-based health care programs.
Supplemental Material
Unblinded_Supplementary_Table_1_9-28-20 – Supplemental material for The Value of Home-Based Primary Care: Qualitative Exploration of Homebound Participant Perspectives
Supplemental material, Unblinded_Supplementary_Table_1_9-28-20 for The Value of Home-Based Primary Care: Qualitative Exploration of Homebound Participant Perspectives by Sarah LaFave, Brittany Drazich, Orla C. Sheehan, Bruce Leff, Sarah L. Szanton and Mattan Schuchman in Journal of Applied Gerontology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Johns Hopkins Center for Innovative Care in Aging.
Ethics Approval
The Johns Hopkins Medicine institutional review board approved the study (IRB00163140).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.