
Abstract
Background:
Interventions supporting older adults’ transition from hospital to home can address geriatric needs. Yet this evidence base is fragmented. This review describes transitional interventions that provide pre- and post-discharge support for older adults and evaluates their implementation and effectiveness in improving health and well-being.
Method:
Articles were included if they examined the extent to which transitional interventions were effective in improving health and well-being outcomes and reducing hospital readmission rates among older adults.
Results:
Twenty studies met the inclusion criteria. Four types of interventions were identified: education-based (10/20); goal-oriented (4/20); exercise (4/20); and social support interventions (2/20). Education and goal-oriented interventions were effective in improving health and well-being outcomes. The impact of interventions on mitigating hospital readmissions was inconclusive. Only five studies examined implementation.
Discussion:
Older adults transitioning from hospital to home would benefit from tailored education and goal-oriented interventions that promote their capacity for self-care.
Background
As the average age of the population, worldwide, continues to rise, so does the use of and need for acute hospital services (United Nations, 2017). The rate of people being admitted and readmitted into hospital is increasing (i.e., patients who have been discharged from hospital are admitted again within a specified timeframe, Lowthian et al., 2012). Older adults (i.e., aged over 60 years) are a high-risk group that are more likely to experience hospital readmissions, as they are vulnerable to increased health needs and social isolation (Coyle & Dugan, 2012). At least one in five older individuals are at risk of hospital readmission within 30 days of discharge (Andreasen et al., 2015). Yet, a large proportion of these readmissions are considered preventable and are often viewed as a result of inadequate coordination of care between hospital and community services, and ineffective post-discharge follow-up support (Leigh, 2016).
High rates of hospital readmissions among older adults significantly impact the acute care system and the individual. Readmissions place a strain on hospitals, resulting in excess health care expenditure and limited resources, such as reduced bed capacity and provision of care (Scott, 2010). Hospital readmission can also have a significant impact upon the patient post-discharge, including significant decline in overall functioning, increased expenses (i.e., hospital bills), stress, risk of hospital acquired adverse events, such as falls, pressure injuries, or infection (Madeira et al., 2007) and subsequent difficulty integrating back into the community (Andreasen et al., 2015).
Governments across the world are investing in models of care to keep older adults at home rather than hospital (Powers et al., 2016). A model of care that has been trialed is “transitional care,” which encompasses interventions that promote the safe and timely transfer of patients from hospital to home (Allen et al., 2014). These models are effective in supporting older adults in their transition home when they are at their most vulnerable through the delivery of educational, social, and medical support (Feltner et al., 2014; Van Spall et al., 2019). Braet and colleagues (2016) provide an earlier meta-analysis of randomized controlled trials that examined the impact of transition interventions on hospital readmissions. Their review synthesized studies delivering transitional support pre-discharge, post-discharge, or pre- and post-discharge. They found that interventions mitigated hospital readmission rates, particularly those that included pre- and post-discharge support. These findings are also supported by earlier reviews (e.g., Feltner et al., 2014; Scott, 2010).
Despite prior research, gaps exist. First, past reviews have focused on evaluating the impact of transition interventions for one specific diagnosis, such as dementia (Hirschman & Hodgson, 2018), heart failure (Feltner et al., 2014), or chronic obstructive pulmonary disease (Sharma et al., 2010). This limits our understanding and applicability of transition programs as these individuals experience high rates of comorbidity (Murad & Kitzman, 2012). Second, no review has focused specifically on interventions that provide both in-hospital and post-discharge support, rather the focus has been on either hospital or post-discharge support (e.g., Braet et al., 2016). Finally, research has not evaluated the effect of such interventions on health and well-being outcomes, often focusing solely on hospital readmission rates instead (Hansen et al., 2011). It is clear that the fragmented evidence-base needs to be updated to inform the development and implementation of transition interventions for older adults.
The aim of this review was threefold: (a) describe the different types of transition interventions for older adults that provide both in-hospital and post-discharge support; (b) evaluate how effective these interventions are in improving health and well-being outcomes and hospital readmission rates; and (c) evaluate the implementation of these interventions.
Method
Design
A systematic scoping review was conducted, following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement guidelines.
Search Strategy
Four electronic databases (PsycINFO, PubMed, MEDLINE Complete, and CINAHL) were searched from January 2000 to January 2020. A search strategy was developed using medical subject heading (MESH) search terms and keywords (refer to the supplementary materials) and was customized to each database as needed. Reference lists of included articles were also searched.
Inclusion and Exclusion Criteria
Study inclusion criteria: (a) Randomized controlled trials (RCT) published in English from January 2000 to January 2020 inclusive; (b) effectiveness of the intervention supporting patients’ transition from hospital to home was assessed; (c) intervention delivered to patients in hospital and once they were discharged home; (d) study participants aged 60 years and over with any diagnosis; (e) study outcomes included hospital readmissions and overall health and well-being outcomes for patients (e.g., physical health, quality of life). Study designs were restricted to RCTs to obtain a synthesis of the most rigorous and robust research. Studies from the past 20 years were included to provide an overview of the recent evidence regarding the impact of interventions to inform current practice. Studies where the intervention was delivered in the hospital only or the home only were excluded, as well as studies that did not assess patient outcomes.
Study Selection and Data Extraction
Two researchers (R.O. and M.S.) independently screened and excluded studies based on title and abstract. For articles not excluded, the full-text versions were sourced and assessed for inclusion by the same two researchers. The interrater agreement, calculated by the proportion of studies that were given the same rating, was 0.97. Disagreements were resolved by a third researcher (D.A.). Summary tables were created to extract data from the included studies (see Table 1 and Table 2 in the supplementary materials). One researcher extracted data from all studies (M.S.), with 30% cross-checked by a second researcher (R.O.). Data extracted included country of study; sample size; participant diagnosis, age, and gender; intervention and comparison group description, duration, frequency, and adherence; assessment time points and methods; outcomes; and effectiveness findings.
Study Synthesis
Given the heterogeneity across the studies (i.e., differences in the types of interventions employed, measures used, and the outcomes assessed), and the lack of reporting of effect sizes, meta-analysis was neither possible nor feasible. Instead, the findings were categorized according to intervention type, which was determined by the predominant form of support provided to participants (e.g., education, social support, etc.).
Quality Assessment
The methodological quality assessment of included studies was conducted independently by two researchers using the National Institute of Health (NIH) Quality Assessment Tool for Controlled Studies. This scale rates 14 aspects (see Table 3 in the supplementary material) of methodological quality of RCTs as “yes,” “no,” or “not reported” (NR). Studies that scored “yes” for at least 80% of their assessment criteria were categorized as “high” quality, studies that fulfilled 50% to 79% of the criteria were classified as “medium” quality, and studies that scored “yes” for less than 50% of the criteria were considered “low” quality. Consensus was achieved through a cooperative discussion between the two researchers, where the interrater agreement (proportion of agreed ratings) was 0.94. A third researcher was consulted to resolve any disagreements.
Results
Search Yield
The stages of study selection are summarized in the PRISMA flowchart presented in Figure 1 and Table 4 (refer to the supplementary materials). The search of four electronic databases identified a total of 7,483 studies. After the removal of 892 duplicates, 6,591 studies were screened at the title and abstract stage, followed by 193 studies assessed at full text. Nineteen studies were deemed eligible for inclusion, and an additional study was identified from the reference list of these included studies. Therefore, a total of 20 studies were included in this review.
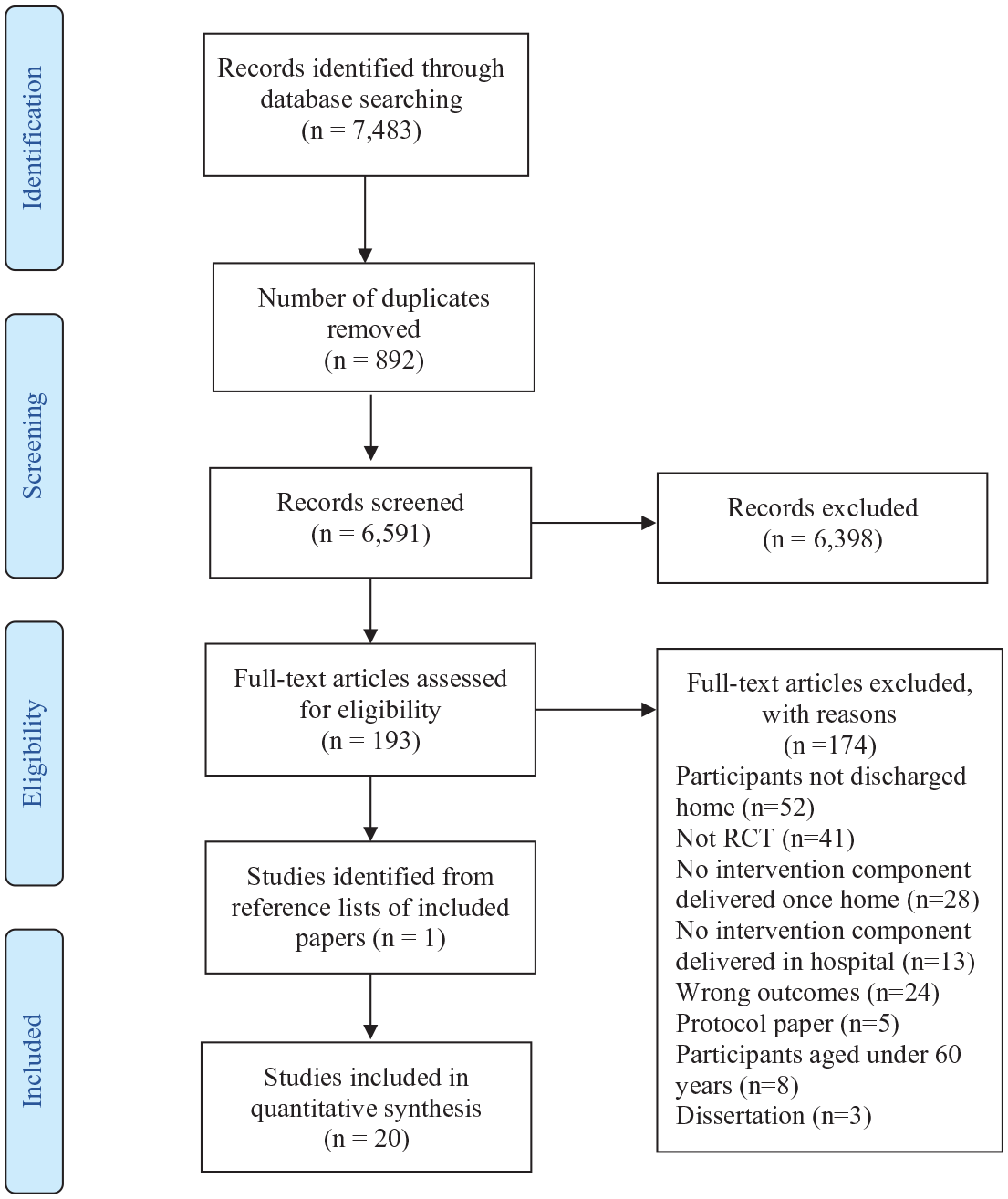
Flow diagram illustrating the selection process for the systematic review of the literature.
Study Characteristics
Six of the 20 studies were conducted in China, three in the United States (Burns et al., 2014; Goldman et al., 2014; Naylor et al., 2004), three in Taiwan (Huang & Liang, 2005; Lin et al., 2009; Shyu et al., 2016), and two in the United Kingdom (Johnson-Warrington et al., 2016; Thompson et al., 2005), Canada (Harrison et al., 2002; Van Spall et al., 2019), and Australia (Courtney et al., 2009; Finlayson et al., 2018). The remaining two studies were conducted in Denmark (Lindhardt et al., 2019) and Switzerland (Lindpaintner et al., 2013).
The studies varied considerably in sample size, ranging from 50 to 2,494 (M = 317, SD = 536). The average age of participants was 73.50 years (SD = 5.17 years) and men and women were equally represented (47% male). Diagnoses of participants varied significantly. The majority of the studies (7/20) included participants admitted to the general medicine wards with a diagnosis of a cardiac, respiratory, or endocrine disease. The remaining 13 studies assessed participants with the same single diagnosis, including individuals with chronic heart failure (n = 6), hip fracture (n = 3), coronary artery disease (n = 2), chronic obstructive pulmonary disease (n = 1), and stroke (n = 1). All studies excluded individuals with cognitive deficits (e.g., dementia), primarily due to challenges obtaining informed consent.
Quality of Evidence
The quality assessment summary for the 20 studies is presented in Table 3 of the supplementary material. Eleven studies (55%) were high quality, while nine studies (45%) were medium quality. Randomization was adequate in all studies, and groups were similar at baseline in 16 studies (80%). Only two studies (10%) were blinded to both participants and providers of the intervention (Chow & Wong, 2014; Shyu et al., 2016). Outcome assessors were blinded in 16 of 20 studies (80%). Four studies (20%) reported rates of attrition more than 20% at the endpoint of the study, but the differential dropout rates between groups was less than 15% (Courtney et al., 2009; Harrison et al., 2002; Naylor et al., 2004; Shyu et al., 2016). Limitations were a lack of reporting of adherence to the intervention in 15 of 20 studies (75%), and small sample sizes which were not large enough to detect differences with 80% power (50%). Outcomes were assessed using valid and reliable measures.
Control Groups
All control groups received usual or standard care. This included routine in-hospital care, discharge, and follow-up protocol, which remained relatively consistent across studies regardless of participants’ diagnoses. Routine in-hospital care included appropriate medical tests, procedures, medication, and care provided by a multidisciplinary team (e.g., physician, nurses, physiotherapists). Usual discharge care comprised a final multidisciplinary team round to discuss discharge planning and patients’ needs. Nurses reconciled medication changes, reviewed the written discharge instructions with the patient in hospital, and provided them with their medication prescriptions. The discharge summary was sent to the patient’s physician in the community. Routine post-discharge follow-up included an outpatient appointment with the patient’s primary physician. Care coordination of additional post-discharge services was performed as necessary before discharge.
Intervention Characteristics
The intervention groups received routine care in addition to the transitional intervention. Interventions were delivered by nurses in 18 of 20 studies (90%). In the remaining two studies, community health workers and exercise physiologists delivered the interventions. Interventions were delivered for 3 months (M = 12 weeks, SD = 12 weeks). The frequency of contact was minimal in hospital, with more than one contact provided to participants in nine studies (45%) followed by weekly contact in the home in 14 of 20 studies (70%). The type of contact (delivery mode) once home was generally in-person and included home visits (n = 7), phone calls (n = 4), or a combination of both (n = 9). Interventions were disease specific, providing targeted support according to the patients’ diagnoses and needs.
Intervention Content
The tabulated findings (see supplementary materials) are qualitatively described according to four types of interventions: education-based (10/20), goal-oriented (4/20), exercise (4/20), and social support (2/20).
Education interventions
Ten of the 20 studies implemented an educational intervention, which provided patients with information, education, strategies, and/or skills that were tailored to manage the patient’s specific diagnosis and overall health. Disease-specific information, including symptom recognition, symptom management, or advice about the importance of medication adherence and how to achieve it, was delivered in 6/10 studies to individuals with heart failure (Harrison et al., 2002; Thompson et al., 2005; Van Spall et al., 2019), hip fracture (Huang & Liang, 2005; Lin et al., 2009), and stroke survivors (Wong & Yeung, 2015). Three education interventions delivered general health and stress management information to individuals with varying general medical conditions, such as respiratory, cardiac, or endocrine disease (Goldman et al., 2014; Lindpaintner et al., 2013; Wong et al., 2008). Zhang and colleagues (2017) delivered a multicomponent education intervention for patients with coronary artery disease, including stress management tips, medication adherence, and self-care skill development.
Goal-oriented interventions
Four of the 20 studies implemented goal-oriented interventions (Chow & Wong, 2014; Lindhardt et al., 2019; Naylor et al., 2004; Zhao & Wong, 2009). Three of these studies worked with patients with a range of medical diagnoses (e.g., heart failure, coronary artery disease) to identify and achieve general health-based goals, such as enhanced nutrition, increased physical activity, or cessation of unhealthy habits (Chow & Wong, 2014; Lindhardt et al., 2019; Zhao & Wong, 2009). For example, in Chow and Wong (2014) study, nurses supported patients in hospital to identify health goals and barriers to achieving those goals. Once home, nurses conducted phone calls and home visits to motivate and provide ongoing advice around goal attainment. Naylor and colleagues (2004) helped patients with heart failure set goals pre-discharge to specifically manage their symptomology (e.g., medication adherence) followed by home visits to implement ongoing strategies for goal attainment.
Exercise interventions
Four of the 20 studies implemented an exercise intervention, which supported patients to achieve basic physical exercise to improve their general fitness and well-being (Courtney et al., 2009; Finlayson et al., 2018; Johnson-Warrington et al., 2016; Shyu et al., 2016). Individuals with a general medical condition (e.g., cardiovascular or respiratory disease) received a tailored exercise program in hospital, based on a comprehensive assessment, and regular home visits by an exercise physiologist (Finlayson et al., 2018) or telephone follow-up from nurses (Courtney et al., 2009). In Johnson-Warrington and colleagues’ (2016) study, patients with chronic obstructive pulmonary disease received a healthy lifestyle manual and exercise demonstration while in hospital followed by phone calls post-discharge to reinforce exercise adherence, motivation, and skills. Finally, Shyu and colleagues (2016) employed a physical therapist to deliver rehabilitation pre- and post-discharge among individuals with hip fracture.
Social support interventions
Two of the 20 studies adopted a social support model of care (Burns et al., 2014; Kwok et al., 2008) to provide companionship, encouragement, and informal counseling to participants. In Kwok and colleagues’ (2008) study, patients with chronic heart failure received in-person visits both pre- and post-discharge from a community nurse who provided social support through health counseling and dietary advice and encouraged participants to contact them if they developed symptoms. Similarly, in Burns and colleagues’ (2014) study, a community health worker visited patients with chronic obstructive pulmonary disease in hospital to identify and address patients’ concerns about transitioning home, followed by weekly phone calls post-discharge to provide ongoing support and address concerns.
Effectiveness of Interventions
As the reporting of effect sizes was absent for the majority of these studies, the effectiveness of these interventions has been detailed descriptively. All studies assessed hospital readmissions and at least one outcome associated with health and well-being, which was often measured using the self-reported Short Form Survey. Outcomes included overall quality of life, mental health, physical health, and independent functioning (i.e., which encompassed self-care ability/knowledge, and completing activities of daily living).
Education interventions
The efficacy of education interventions was evaluated using the following outcomes: hospital readmission rates (assessed in 10/10 studies), quality of life (5/10; Harrison et al., 2002; Lindpaintner et al., 2013; Thompson et al., 2005; Wong & Yeung, 2015; Zhang et al., 2017), mental health (5/10; Harrison et al., 2002; Huang & Liang, 2005; Lin et al., 2009; Thompson et al., 2005; Wong & Yeung, 2015), physical health (6/10), and independent functioning (4/10; Huang & Liang, 2005; Lin et al., 2009; Wong et al., 2008; Zhang et al., 2017). Only one education intervention found a significant difference in hospital readmission rates at follow-up between treatment groups (Huang & Liang, 2005). The majority of studies found significant improvements among patients’ quality of life (3/5; Harrison et al., 2002; Wong & Yeung, 2015; Zhang et al., 2017) and independent functioning (3/4; Huang & Liang, 2005; Lin et al., 2009; Zhang et al., 2017). Only two studies found a significant improvement in mental and physical health (2/5; 2/6; Huang & Liang, 2005; Wong & Yeung, 2015).
Goal-oriented interventions
The efficacy of goal-oriented interventions was evaluated using the following outcomes: hospital readmission rates (4/4), mental health (3/4; Chow & Wong, 2014; Lindhardt et al., 2019; Naylor et al., 2004), physical health (2/4; Chow & Wong, 2014; Naylor et al., 2004), independent functioning (2/4; Chow & Wong, 2014; Zhao & Wong, 2009), and quality of life (2/4; (Lindhardt et al., 2019; Naylor et al., 2004). Two of the four studies observed lower hospital readmissions rates among intervention participants compared to controls 84 days (Chow & Wong, 2014) and 52 weeks post-discharge (Naylor et al., 2004). For physical health, both Chow and Wong (2014) and Naylor and colleagues (2004) found significant improvements in the intervention group at follow-up. Chow and Wong (2014) and Zhao and Wong (2009) found significant improvements in intervention participants’ capacity for independent functioning and adherence to daily activities. One study found a significant improvement in mental health outcomes (1/3; Chow & Wong, 2014) and no study found improvements in quality of life.
Exercise interventions
The efficacy of exercise interventions was evaluated using hospital readmission rates (4/4), independent functioning (2/3; Johnson-Warrington et al., 2016; Shyu et al., 2016), and physical and mental health (1/4; Courtney et al., 2009). Two exercise interventions (e.g., Courtney et al., 2009; Finlayson et al., 2018) demonstrated a significant difference in readmission rates between groups, with participants in the intervention group reporting less unplanned hospital admissions within 28 days and 12 weeks post-discharge compared with control participants. Only one study found significant improvements in intervention participants’ ability to function independently (Shyu et al., 2016) and in their physical and mental health (Courtney et al., 2009).
Social support interventions
The efficacy of social support interventions was evaluated using hospital readmission rates (2/2; Burns et al., 2014; Kwok et al., 2008), and independent functioning (1/2; Kwok et al., 2008). Neither study found a significant difference in hospital readmissions between the groups at follow-up. Kwok and colleagues (2008) found a significant improvement in independent functioning among intervention participants who received social support from a community nurse, in comparison to control participants.
Implementation of Interventions
Five of 20 studies (25%) assessed and reported on implementation outcomes (Burns et al., 2014; Courtney et al., 2009; Finlayson et al., 2018; Goldman et al., 2014; Thompson et al., 2005). Burns and colleagues (2014) found that for their social support intervention, 40% of patients had no contact with the community health worker in hospital, and only 38% received the intended four follow-up calls once home. The authors maintained that the community health worker was often unaware of discharge times, outpatient appointments, or readmissions, so could not provide phone calls at the most welcome or effective time. Similarly, there was low adherence to the exercise interventions, with only 42% to 68% (Finlayson et al., 2018) and 53% (Courtney et al., 2009) of participants adhering to the exercises, as intended. Contrastingly, the two education interventions demonstrated high fidelity, with 83% of participants receiving two follow-up phone calls from nurses (Goldman et al., 2014) and 98% receiving a home visit post-discharge (Thompson et al., 2005) as intended.
Discussion
The aim of this review was to synthesize the evidence base of interventions that provide both pre- and post-discharge support to facilitate older adults’ transition from hospital to home. Specifically, this review aimed to (a) describe the different types of transition interventions; (b) evaluate their effectiveness in improving health and well-being outcomes and hospital readmission rates; and (c) evaluate their implementation. Four types of transition interventions were identified: education-based, goal-oriented, exercise, and social support interventions. The interventions were delivered for an average of 3 months, by nurses. This is consistent with Hirschman and Hodgson’s (2018) systematic review, which found that psychoeducation and goal-based interventions were most commonly delivered by nurses.
Goal-based and educational interventions were most effective in improving the self-reported physical health, independent functioning, and overall quality of life of older adults transitioning from hospital to home. The goal-based interventions significantly improved physical health and independent functioning, while education interventions were effective in improving quality of life and independent functioning. The common ingredients to both interventions was the comprehensive assessment of patients’ individual needs, problem identification, decision support, and participatory goal setting and attainment. These components help the patient to build their self-efficacy and promote self-management (Carvalho et al., 2018).
The exercise interventions were not significant in generating consistent change in physical health or independent functioning. Adherence rates were either not reported or low (i.e., 42% to 68% of participants who adhered; Finlayson et al., 2018). Prior research shows that exercise interventions work best when there is a self-monitoring component attached to the intervention (Chase, 2013). None of the exercise interventions incorporated a self-monitoring feature within the intervention so patients may have struggled to adopt the exercise behavior into their routine. Moreover, previous exercise behaviors are highly predictive of future exercise behaviors (Rhodes & Kates, 2015). Given that older adults are often categorized as having sedentary behaviors, this would be a difficult behavior to change. More work is needed to assess whether exercise interventions with high adherence generate change. Incorporating self-monitoring elements within such interventions is recommended.
Similarly, social support interventions were not shown to significantly improve physical or mental health outcomes. One reason that may explain this is that the interventions did not embed themselves within the patient’s preexisting care team. Indeed, there was no description in either study about how providing nurse-support and guidance was offered to enhance the already active care team. Social support programs for older adults need to not only acknowledge and involve the wider care team in their planning but also work in tandem with these supports, to achieve better outcomes (Ray et al., 2015). More work is needed to establish whether the inclusion of the care team in the delivery of social support generates improvements in older adults’ health and well-being.
Finally, the majority of interventions were not shown to mitigate hospital readmission rates. This could be due to the characteristics of the patients. Indeed, the majority of studies reviewed herein included patients who had chronic health issues (e.g., heart failure). It may be the case that for some of these patient groups, close medical supervision was in fact warranted and not easily prevented via transitional interventions. It is recommended that further research examines the degree to which transitional interventions can mitigate hospital readmission rates for particular groups of patients (i.e., no chronic health issues vs. chronic health issues).
The studies included in this review were conducted in eight different countries with varying health care systems, including different models of primary care, hospital services, home-based care, and rehabilitative care, which may have contributed to variability in the findings. Overall, transitional interventions implemented in China (n = 6) and Taiwan (n = 3) were most effective in improving health and psychosocial functioning, while studies from Europe (n = 4) were less effective. This could be due to the type of interventions evaluated, as five of the six studies from China implemented either an education or goal-oriented intervention. Alternatively, the findings may be more reflective of characteristics inherent to each country’s health system and the context within which the intervention was delivered. Therefore, deeper exploration and analysis of transitional care for older adults among individual countries is warranted.
Limitations
There are key limitations worth noting. First, the lack of reporting on implementation findings reflects a significant limitation of this literature and impacts the quality of evidence presented. Intervention implementation was assessed in only five studies, with two studies delivering the intervention with good adherence. For the remaining studies, there was no way to extrapolate whether the intervention was implemented as intended. This shows that not only is the notion of implementation overlooked within this area of literature, but also within the intervention delivery itself. It is well established that if participants do not receive an intervention as intended, it can significantly impact the effectiveness of said intervention (Handley et al., 2018). Future research needs to be dedicated to assessing implementation of transitional care interventions to ensure their delivery as close to as intended as possible.
Second, the majority of reviewed studies included active control groups that delivered some type of care, ranging from minimal to intensive, and often included separate components from what was delivered in the intervention itself. These different control conditions may create different effect measurements. Pooling the different control conditions together may obscure the effectiveness of the interventions. In light of the ethical issue in randomizing patients to an organic control group wherein no care is delivered, it is recommended that more consideration is applied to the delivery of the control group. Ensuring the control and intervention groups are as matched as possible may help to separate the individual contribution that the intervention is making, above and beyond the control group.
Third, the majority of studies consistently excluded individuals with cognitive deficits, such as dementia, from participation, often due to difficulties in obtaining their consent to participate in research. This has implications for the design and implementation of transition interventions that meet the needs of this high-risk population who often experience hospital care and face difficulties transitioning into the community. Systematic reviews have focused on examining transition interventions for patients with dementia when they are transitioning to an aged care facility rather than their home (Hirschman & Hodgson, 2018). Further research is needed to examine how persons with specific cognitive deficits are able to most effectively transition from hospital to home. Similarly, there was no discussion or assessment of frailty among participants in the included studies, which could have influenced the effectiveness of interventions. The extent of frailty among older adults impacts their health and can be a significant predictor of health status following a serious medical diagnosis or exacerbation of existing physical illness (Albert, 2019). Therefore, it is necessary that future studies explore the relationship between frailty and the transition from hospital to home among this population.
Implications
The findings of this review show that goal-based and educational interventions were most effective in improving the physical health, independent functioning, and overall quality of life of older adults transitioning from hospital to home. It is recommended that transition interventions that are tailored to meet the person’s unique needs, support patient empowerment, and promote their knowledge and capacity for self-care are delivered to this population. The findings also provide a useful framework within which health professionals, researchers, policy makers, and other stakeholders across health and social care settings can be guided. Specifically, these findings may inform the development (and redevelopment) of transition interventions for older adults, as well as training for care providers that focuses on improving patient empowerment through knowledge sharing, goal setting, and self-care management. Implementing transitional care models more broadly may require additional resources, such as financial systems and staffing, to support and facilitate the collaboration between hospital and home care.
The transition from hospital to home represents a key opportunity for interventions to improve the physical health and independent functioning of older adults. Future efforts need to be directed toward mitigating hospital readmissions and improving mental health. Best practice recommendations for successful outcomes among older adults transitioning from hospital to home include tailored education and goal-oriented interventions that meet the person’s needs and promote their capacity for self-care.
Supplemental Material
sj-pdf-1-jag-10.1177_0733464820968712 – Supplemental material for The Effectiveness of Transition Interventions to Support Older Patients From Hospital to Home: A Systematic Scoping Review
Supplemental material, sj-pdf-1-jag-10.1177_0733464820968712 for The Effectiveness of Transition Interventions to Support Older Patients From Hospital to Home: A Systematic Scoping Review by Renee O’Donnell, Melissa Savaglio, Helen Skouteris, Jane Banaszak-Holl, Chris Moran, Heather Morris, Dave Vicary and Darshini Ayton in Journal of Applied Gerontology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.