
Abstract
It is widely recognized that the engagement of older adults with multimorbidity and their caregivers as partners in health care research is important and invaluable. The objective of this study was to examine how researchers can best engage and support older adults with multimorbidity and informal friend or family caregivers of older adults with multimorbidity as research partners in health care research teams. The persona-scenario method was used for participants to create fictional stories. These stories were analyzed to shed light on specific strategies that can support older adults and caregivers as partners on health care research teams, such as a patient-centered approach, identifying and addressing barriers to engagement, and clarifying roles and responsibilities on the research team. The results from this study can be used to inform research, policy, and education on supporting older adults with multimorbidity and caregivers of older adults with multimorbidity as research partners.
Keywords
Introduction
A compelling base of expert opinions and experiences suggest that engagement of older adults and caregivers in health care research can improve the relevance, acceptability, and usability of research findings (Domecq et al., 2014; Duffett, 2016; Vat et al., 2017). Yet little is known about strategies to optimize the engagement of older adults with multimorbidity (two or more chronic conditions; Roberts et al., 2015; Van den Akker et al., 1996), Canada’s fastest growing segment of the health care population and the highest users of the health care system (McNeil et al., 2016).
In 2018, Statistics Canada estimated greater than one in six Canadians are older adults (Statistics Canada, 2019). By 2037, the proportion of older adults is expected to increase to over one in four Canadians (Government of Canada, 2014). Older adults with multimorbidity are high service-users, compared with older adults with no or single chronic conditions (Canadian Institute for Health Information [CIHI], 2011). Community-dwelling older adults with multimorbidity make up 24% of the older adult population in Ontario, but account for 40% of health care use among older adults (CIHI, 2011). The prevalence of chronic conditions among older adults in Canada continues to increase, along with their impact on the health care system (World Health Organization, 2005). The cost of addressing multimorbidity among older adults is further complicated by the way health care services are currently delivered, which applies a single-illness approach rather than a coordinated approach to address multimorbidity (CIHI, 2011; Holroyd-Leduc et al., 2016).
However, older adults with multimorbidity, as health care service-users, have had limited involvement as research partners (Holroyd-Leduc et al., 2016). In instances where older adults with multimorbidity and their caregivers have been involved, many expressed their engagement (as participants, advisors, or consultants) in research to be disingenuous, especially when they perceived that their ideas and concerns were not validated or acknowledged in the research (Alzheimer Society, 2015; Marlett & Emes, 2010). This feedback cues researchers to consider more meaningful ways that they can optimize patient engagement in research to avoid tokenism. Engaging older adult patients with multimorbidity and their caregivers with opportunities to share their experiences and interactions with the health care system can provide researchers with insight into this population’s patient experience with health care services, particularly in relation to inequity and accessibility (Age UK, 2011; Holroyd-Leduc et al., 2016; Pizzo et al., 2015).
The limited meaningful involvement of older adults with multimorbidity may be attributed to research engagement strategies that are insensitive to their visible and invisible disabilities, as well as social inequities such as gender, level of education, income, and other life experiences that limit opportunities for individuals of this vulnerable population (Invisible Disabilities Association, 2018; Snow et al., 2013). Being aware of potential barriers to patient engagement and tailoring engagement strategies to the population of interest are crucial considerations when planning for meaningful and sustained patient engagement across the research timeline (Snow et al., 2013). Known barriers to the meaningful engagement of older adults with multimorbidity and their caregivers include overlooking individual engagement needs, disregarding power imbalances with researchers, research funding constraints, and limited time for their recruitment (Holroyd-Leduc et al., 2016). Additional barriers may include the fact that many experience health challenges or may find it difficult to participate given their caregiving responsibilities (Holroyd-Leduc et al., 2016; Marlett & Emes, 2010).
Existing literature on patient engagement in research has mostly developed within the last 10 years, but largely reflects experiences from the researchers’ perspectives (Brett et al., 2014; Domecq et al., 2014; Holmes et al., 2018; Wilson et al., 2015). In addition, the literature suggests that patient engagement at different points in the research process is feasible, but more research is needed to identify methods for achieving optimal engagement. Moreover, the relevance of this literature to older adults with multimorbidity and caregivers of older adults with multimorbidity is undetermined.
There is limited understanding from the perspective of older adults with multimorbidity and their caregivers on how to meaningfully engage them as research partners. Furthermore, the specific actions (what activities or processes need to happen for the event to occur) and products (what product or items are needed to support the action) researchers can employ to operationalize meaningful engagement of patients as research partners in different phases of the research process are unknown. The published literature presents strategies that lack detail and provide limited direction to best engage older adults in health care research, while unpublished documents present actionable strategies but lack credibility, dependability, and confirmability. The objective of this study was to examine how to optimize meaningful engagement of older adults with multimorbidity, and informal friend and/or family caregivers of older adults with multimorbidity as partners in health care research from the perspective of those individuals. We believe this to be the first work to understand how to best and meaningfully engage this population as partners in health care research.
Design and Methods
Persona-Scenario Method
The research objective was addressed using the persona-scenario method, a user-centered approach. A key aspect of the persona-scenario method is the active engagement of participants through the use of the persona-scenario exercise (Mao et al., 2005). Unlike traditional qualitative data collection methods, persona-scenarios have the capacity to capture “multiple views of an interaction with diverse kinds and amounts of detailing” (Valaitis et al., 2014) to produce design specifications for a patient engagement strategy to be understood. Persona-scenarios have been shown to be an effective method for co-designing and implementing interventions, such as eHealth interventions, co-writing clinical study protocols, as well as in the early engagement of key stakeholders to promote the uptake of a primary care health service intervention (Reeder & Turner, 2011; Valaitis et al., 2014; Weng et al., 2007). Further description is provided under Data Collection.
Setting and Participants
This study was supported and coordinated from the Aging, Community and Health Research Unit (ACHRU) at McMaster University. ACHRU is a patient-oriented program of research at McMaster University supported by the CIHR Signature Initiative in Community-Based Primary Health Care and the Ontario Ministry of Health and Long-Term Care, Health System Research Fund Program (Markle-Reid et al., 2018). The aim of this pan-Canadian program is to promote optimal aging at home for older adults with multimorbidity and to support their family caregivers (Aging Community and Health Research Unit [ACHRU], 2016).
Study participants were older adults ≥65 years of age, mentally competent to give informed consent, competent in English, able to travel to McMaster University to participate in a persona-scenario session, and had previous experiences as either a research participant or research partner. To validate their ability to provide informed consent to enroll in the study, participants needed to score ≤4 on the Short Portable Mental Status Questionnaire (Pfeiffer, 1975). There was a preference to recruit older adults with caregiving experiences (e.g., as an informal family or friend caregiver for persons with multimorbidity), to achieve a better understanding of their unique perspectives; however, this was not a requirement for participation. For these individuals, the presence of chronic conditions (two or more physical and/or mental chronic conditions) was preferred, but not required.
Recruitment Strategies
Participants were recruited into the study using a purposive snowball sampling strategy. The principal investigator (PI) recruited participants from the ACHRU’s studies, its patient and caregiver stakeholder group, and a community network, the Circle of Friends (a peer-based program for isolated seniors). The ACHRU’s administrator identified potential participants who met the study’s eligibility criteria, and the PI followed up with potential participants by phone to obtain their verbal consent to participate. After participants provided verbal informed consent, baseline data were obtained using a sociodemographic questionnaire developed by the PI. A date and time for the 2-hr persona-scenario session was then arranged. Study participants were informed that they would receive a study information package and a reminder by phone, email, or mail within 1 week of the scheduled appointment time.
Data Collection and Analysis
Persona-scenario exercise
The PI led the persona-scenario exercises. The first session was attended by one of the co-investigators who had experience with the method (R.V.) for peer debriefing and to provide feedback on data collection, which increased the rigor of the research process. The PI received support from staff and students affiliated with the ACHRU to coordinate and conduct the research, which included note-taking during the persona-scenario session. Prior to the first session, the PI provided the research assistants with an orientation to the persona-scenario exercise.
Study participants were paired and organized into sessions based on whether they most identified themselves as having experience as a patient or as a caregiver for an older adult with multimorbidity. At the beginning of each persona-scenario session, participants were provided with an agenda followed by a 15-min introductory presentation, which included examples from the literature on ways to meaningfully engage older adults and caregivers in health care research to provide context for the creation of personas and scenarios. Participants then worked in pairs through the guiding prompts (e.g., name, age, gender) to create a fictitious but authentic persona that represented them, or people like themselves (older adults with multimorbidity, or caregiving experiences). They were then asked to use their persona and follow the guiding questions to create a story about their involvement in research as a research partner. Examples of guiding questions included: How does your character find out about the health care research and obtain the invitation to be a partner (co-researcher) on the health care research team? What happens at research team meetings? How is your character involved in making decisions within the research team, if at all? Lay language was used to improve the readability of the introductory presentation and the guiding questions. For example, the terms “persona” and “scenario” were replaced by “character” and “story,” respectively.
During the creation of the persona-scenarios, the note-taker captured the key points of the participants’ descriptions. This summary was projected onto a screen for the participants to view in real time. After participants created their persona and at least one scenario, the PI verbally summarized the details of their character(s) and story. This allowed the participants to verify the accuracy of the notes captured in real time, rather than returning transcripts to participants to provide feedback. The creation of person-scenarios was audio-recorded to capture the dialogue that occurred between participants.
The first persona-scenario session was a trial-run with two participants to determine the timing of the agenda, the flow of the persona-scenario exercise and discussion, and the readability of the guiding questions. The data collected from the trial-run session were included in the analysis. The trial-run confirmed the value of the 15-min introductory presentation and helped to more accurately estimate the length of time required to conduct the persona-scenario exercise. Data collection occurred until “data saturation” was reached. That is, no new ideas emerged from the data.
Data Analysis
Audio-recordings and notes were transcribed verbatim and checked by the PI for accuracy prior to analysis. Personas were summarized from the notes. The PI listened to the audio-recordings and read the transcribed content several times to identify common themes. While the personas’ descriptions provided necessary context for the design choices made in the scenarios, the scenarios provided the data for analysis (coding). The analysis was conducted in two phases: (a) identification of codes, subthemes, and themes using a qualitative descriptive approach and (b) interpretation of themes and subthemes into design specifications (actions and products).
First Phase: Identification of Codes, Subthemes, and Themes Using a Qualitative Descriptive Approach
In keeping with a qualitative descriptive approach, the transcripts describing the scenarios were coded into descriptive qualitative codes staying as close to the data as possible (Sandelowski, 2010). Using NVivo, version 11.3.2, the PI created codes from phrases within the content of the transcripts, summary notes, and field notes. These codes were then collapsed into subthemes and broader themes (Neergaard et al., 2009). The coding and development of themes was completed by the PI and checked by the co-investigators in an iterative process, which further supports the rigor of the analysis process.
Second Phase: Interpreting Codes and Subthemes Into Design Specifications
The next phase of analysis involved interpretation of codes and subthemes into design specifications. Design specifications include actions required to achieve the theme or idea, and products required to actualize the action (Valaitis et al., 2014). Examples of actions and products are provided in Tables 2 to 4. The co-investigators audited a sample of the codes, actions, and products to ensure that they fit. Afterward, the design specifications, subthemes, and major themes were confirmed in meetings with the PI and co-investigators, contributing to the rigor of this phase of the analysis.
Results
Participant Characteristics
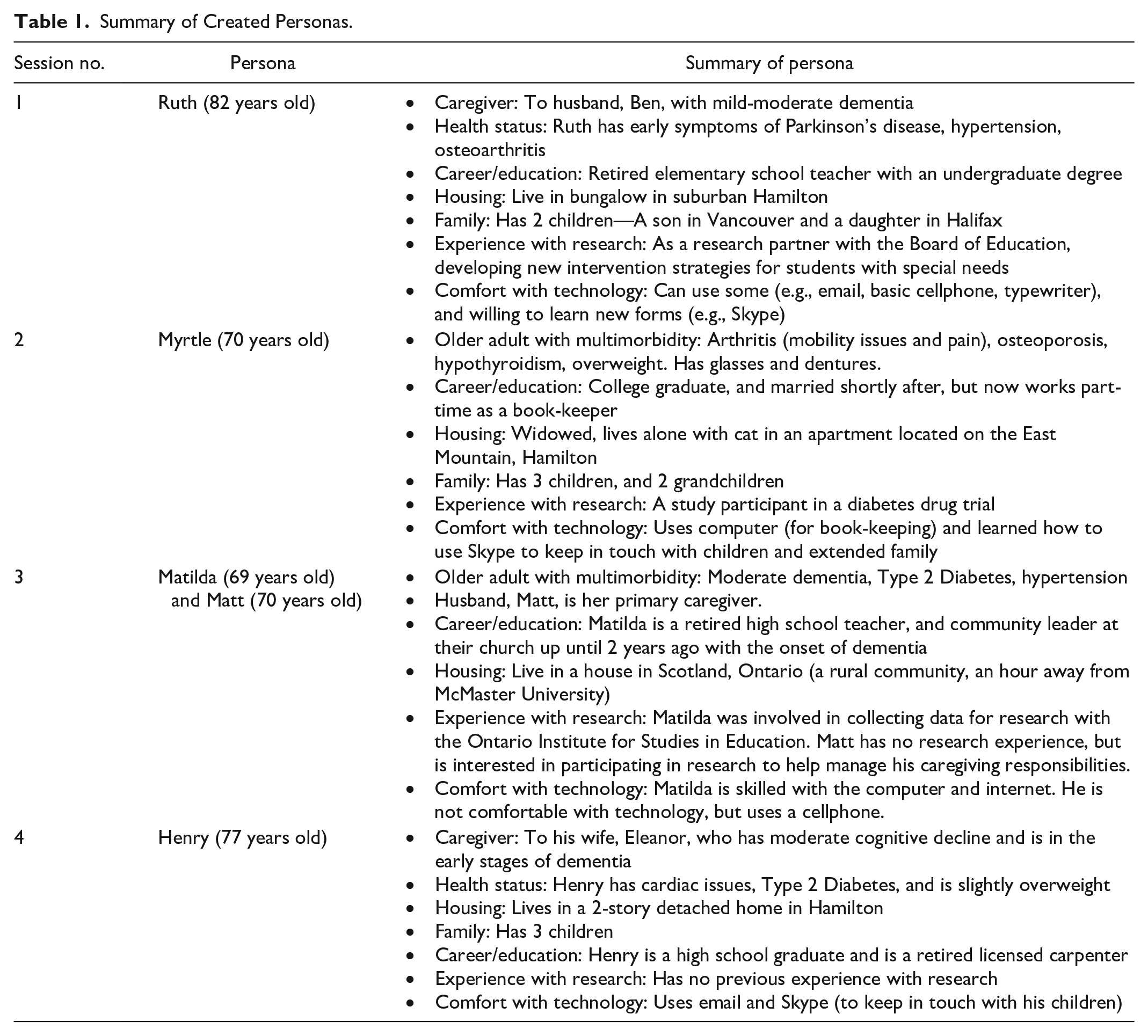
Four persona-scenario sessions were held over 4 months with eight older adult participants. Six of the eight participants had experience as research partners, and two had experience as a study participant. All participants reported experiences as a patient, and seven reported experiences as an informal caregiver. Informal caregivers reported a mean of 14 years of caregiving experience; four informal caregivers were caregiving at the time of the study. Two thirds (n = 5, 63%) of the older adult participants were women, three quarters (n = 6, 75%) were ≥75 years of age, and similar proportions were married (n = 3, 38%) and widowed/divorced (n = 3, 38%). Participants had a mean of five chronic conditions, and almost all (n = 7, 88%) of the participants had multimorbidity. A little more than one third (n = 3, 38%) of participants had annual incomes of less than US$50,000. Most (n = 7, 87.5%) had completed post-secondary education. All participants were Caucasian and spoke English as their primary language. Five personas were created during the four persona-scenario sessions: three caregiver-personas and two patient-personas. A summary of these rich and detailed personas and their characteristics (e.g., health status, career/education, housing, family, experience with research, comfort with technology) are provided in Table 1.
Summary of Created Personas.
First Phase of Analysis: Identification of Codes, Subthemes, and Themes
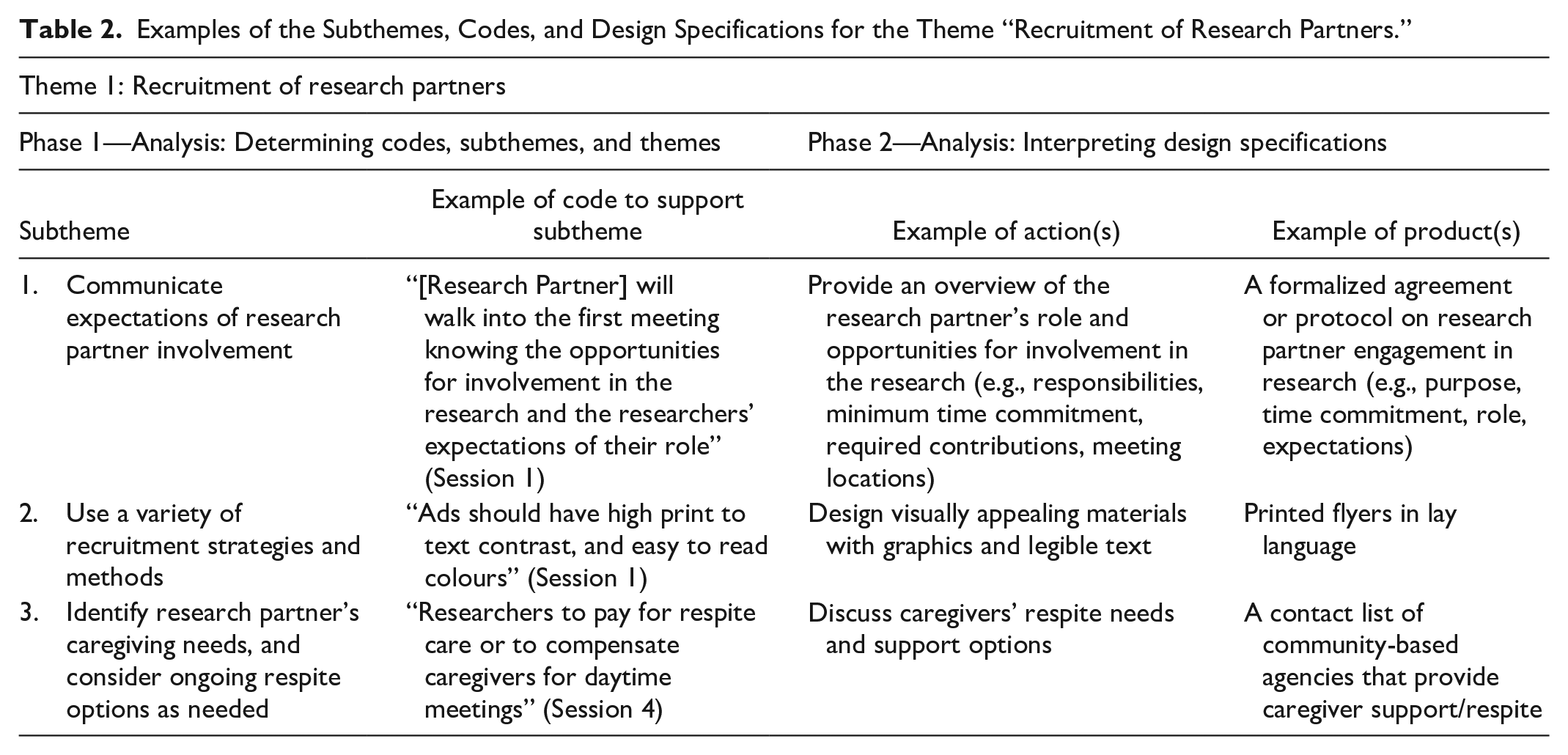
Three major themes emerged from the data: (a) Recruitment of research partners, (b) Planning for meaningful engagement, and (c) Establishing collaborative relationships. The relationships between these themes and subthemes are interrelated and not listed in order of priority. For example, the recruitment of research partners does not need to occur before researchers can plan for their meaningful engagement in health care research. Tables 2 to 4 illustrate the two-phase data analysis process and present a summary of the subthemes of each major theme with selected examples of a code for each subtheme and their related design specifications (actions and products). These examples demonstrate how subthemes emerged from ideas that frequently occurred in the data.
Examples of the Subthemes, Codes, and Design Specifications for the Theme “Recruitment of Research Partners.”
Examples of the Subthemes, Codes, and Design Specifications for the Theme “Planning for Meaningful Engagement.”
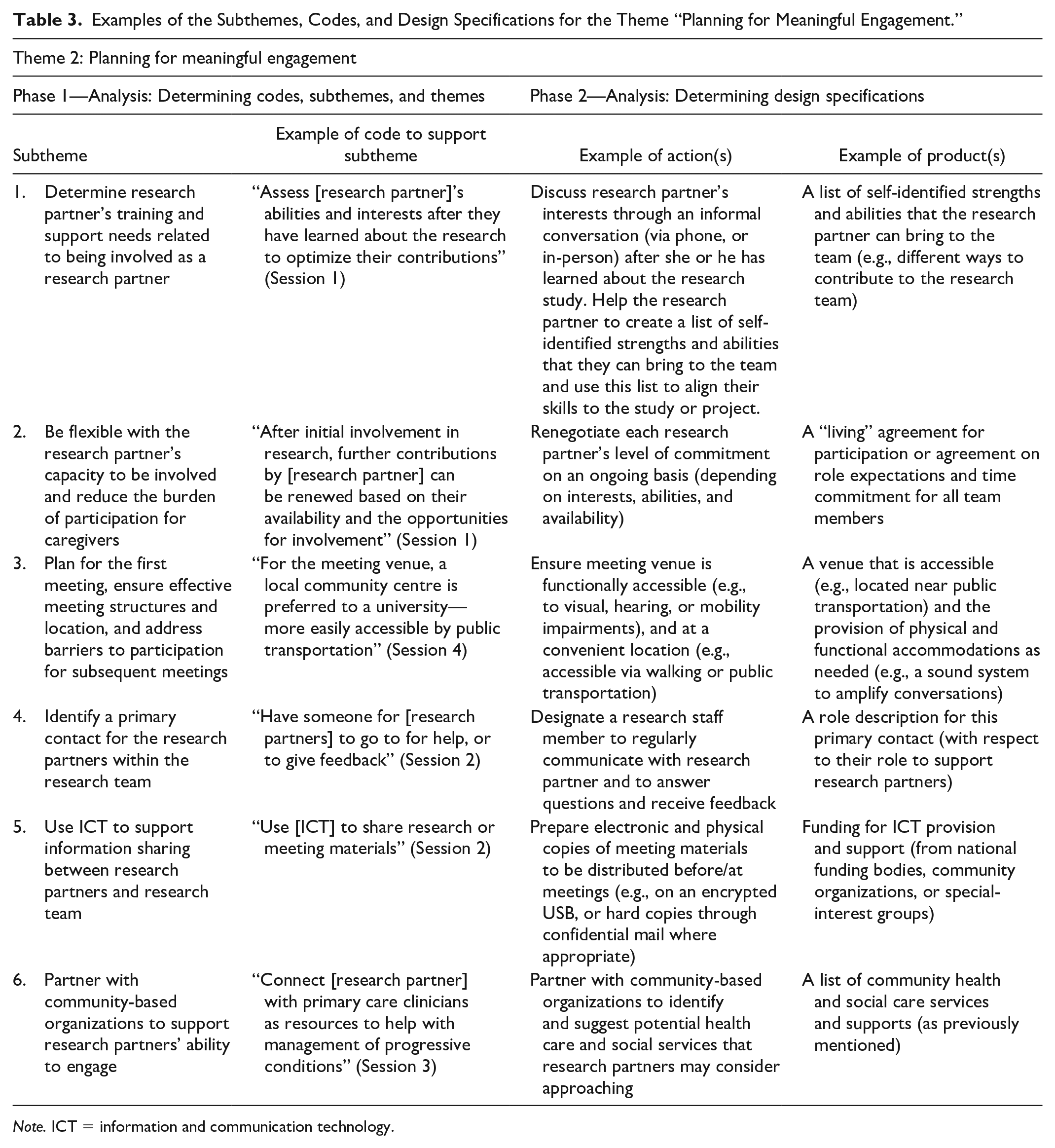
Note. ICT = information and communication technology.
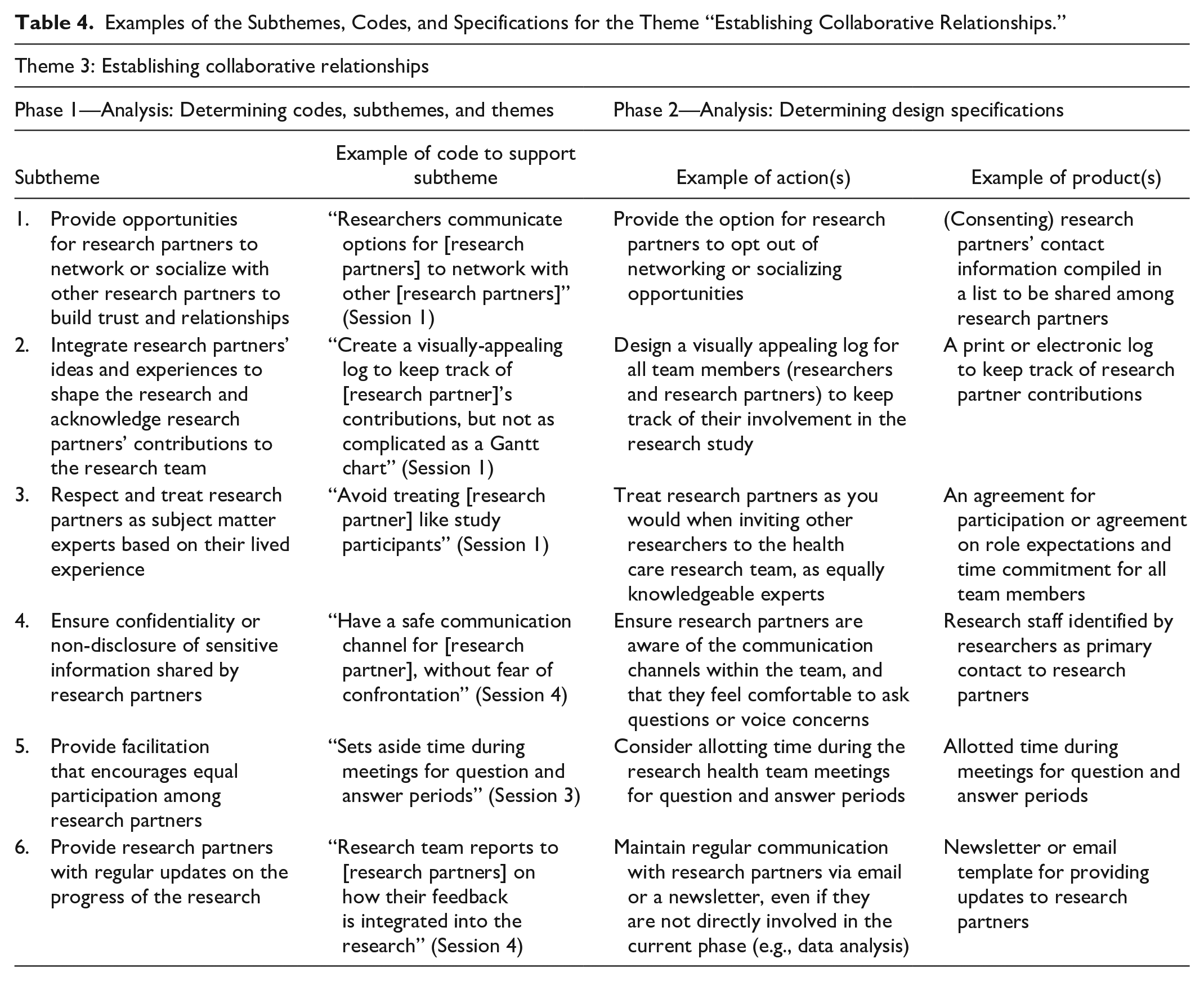
Examples of the Subthemes, Codes, and Specifications for the Theme “Establishing Collaborative Relationships.”
Theme 1: Recruitment of Research Partners
The first main theme that emerged was the “recruitment of research partners.” This included the older adult personas’ first point of contact with the researchers prior to agreeing to participate as a partner in the research. Three main subthemes were identified as influencing their recruitment, including (a) communicate expectations of research partner’s involvement, (b) use a variety of recruitment strategies and methods, and (c) identify research partner’s caregiving needs and consider ongoing respite options as needed.
Theme 2: Planning for Meaningful Engagement
“Planning for meaningful engagement” involved planning for the first health care research team meeting and sustaining research partner engagement in subsequent meetings for the duration of the research (e.g., sharing research findings). Six subthemes were identified related to planning for meaningful engagement: (a) determine research partner’s training and support needs related to their role; (b) be flexible with their capacity to be involved and reduce the burden of participation for caregivers; (c) plan for the first meeting, ensure effective meeting structures and location, and address barriers to participation for subsequent meetings; (d) identify a primary contact for research partners within the research team; (e) use information and communication technology (ICT) to support information sharing between research partners and researchers; and (f) partner with community-based organizations to support research partners’ ability to engage.
Theme 3: Establishing Collaborative Relationships
The third main theme “establishing collaborative relationships” included considerations for researchers to develop mutually respectful, trusting, professional, and communicative relationships with research partners. The six subthemes that relate to this theme included the following: (a) provide opportunities for research partners to network or socialize with other research partners to build trust and for relationship building, (b) integrate research partners’ ideas and experiences to shape the research and acknowledge their contributions to the research team, (c) respect and treat research partners as subject matter experts based on their lived experience, (d) ensure confidentiality or non-disclosure of sensitive information shared by research partners, (e) provide facilitation that encourages equal participation among research partners, and (f) provide research partners with regular updates on the progress of the research.
Second Phase: Interpreting Subthemes and Codes Into Design Specifications
In total, 52 unique actions were identified, and 37 products were interpreted under the three major themes. These design specifications highlighted novel actions and products that were not identified in the existing literature for researchers to consider, which included applying patient-centered approaches to planning meaningful engagement, such as the most appropriate meeting structures for research partners, identifying and addressing barriers to their engagement, and enhancing their ability to engage in the research. For example, research team meetings should include opportunities for socialization, and researchers should partner with community-based organizations to expand their knowledge of health care and social services. Tables 2 to 4 provide examples of how the actions and products were interpreted to bring about the ideas described in the codes.
Discussion
The objective of this study was to examine how to optimize the meaningful engagement of older adults with multimorbidity, and caregivers of older adults with multimorbidity as partners in health care research from the perspective of older adults, and their caregivers. To the author’s knowledge, this is the first study to explore strategies for optimizing the meaningful engagement of older adults with multimorbidity as partners in health care research. Previous studies have focused primarily on researchers’ experience with patient engagement (Carroll et al., 2017; Tran et al., 2016). This study highlighted the importance of examining engagement from a patient perspective.
The importance of engaging patients and caregivers as partners in health care research has been widely recognized. However, a paucity of knowledge exists on how to optimize the meaningful engagement of vulnerable populations (Bardach et al., 2020), specifically older adults with multimorbidity, and their caregivers (Bowen et al., 2011). For example, in a systematic review which included 10 studies, Smith et al. (2012) examined the effectiveness of health care interventions for older adult patients with multimorbidity, but none of them addressed interventions that were co-designed with the patients and caregivers.
The persona-scenario method produced detailed user-centered design specifications (actions and products), which operationalized this study’s themes and subthemes in practice. Many of the subthemes could fit under more than one theme, suggesting that they are interrelated. Moreover, as patient engagement strategies for this population are often discussed in terms of ideas or concepts (Boivin et al., 2014), these design specifications have the potential to address gaps in inequity related to research partner engagement in research and to serve the needs of older adults with multimorbidity and their caregivers.
The findings from this study will contribute to a foundational understanding of how to engage and build strong collaborative relationships in the early phases of the research, which may enhance how researchers can sustain a meaningful level of research partner engagement over an extended period of time (Duffett, 2016; Manafo et al., 2018). Noteworthy of these findings is that the three major themes related primarily to the early stages of engagement in research (e.g., recruitment, planning for meaningful engagement, and establishing relationships). There are two possible explanations for this finding. This may reflect the importance of this phase of engagement. Alternatively, this could reflect the fact that participants had more experiences as research partners in the early phases of research, and thus, could not comment on their involvement in other aspects of the research, such as co-design, implementation, or evaluation of interventions. The three major themes and the finding that there was greater emphasis on the early phases of the research are consistent with existing literature. For example, the core elements of the BC SUPPORT Unit’s patient engagement framework, as described by Holmes et al. (2018, p. 42), included recruitment of patient research partners, initial and ongoing training, and “support for administrative, logistical, financial, and psychosocial” concerns, rather than issues that can arise later in the conduct of research (data collection, analysis, dissemination, etc.). Nevertheless, future research is warranted that involves older adult patient, and caregiver participants who have and can speak to experiences in all aspects of the research process (Ganann et al., 2018).
The findings suggest a number of factors that influence the engagement of older adults with multimorbidity, and their caregivers as partners in health care research, which researchers should consider. These factors include engaging research partners early in the research; clarifying the their roles and responsibilities; adopting a flexible patient-centered approach to their involvement; respecting research partners as colleagues and acknowledging their contributions; identifying and addressing barriers to their engagement (e.g., caregiving support, transportation); providing initial and ongoing training about research; and facilitating continued dialogue and feedback to clarify roles and manage expectations. Regarding the latter, ICT can be a useful tool to support ongoing communication and sharing information between researchers and research partners. In addition, researchers should adopt a variety of recruitment strategies and methods to improve the likelihood of reaching potential research partners with diverse life experiences. Moreover, the findings highlighted that research team meetings that included opportunities for socialization play a key factor in enhancing trust and research partner engagement in the research. Furthermore, researchers need to consider the most appropriate meeting structures (e.g., meeting formats, locations and venues, meeting materials and equipment, human resources) to accommodate their research partners’ physical and learning needs and enhance their ability to engage in the research. In addition, researchers should consider partnering with community-based organizations to expand their knowledge of services that can support a research partner’s ability to engage in research.
Existing literature suggests that training should be tailored to the needs of learners; however, there is no consensus on the training required to prepare researchers for older adult and caregiver engagement in research, nor is there a consensus on recommended training for research partners (Holroyd-Leduc et al., 2016; NIHR-INVOLVE, 2015). The findings from this study identify potential areas for interprofessional training of researchers and clinicians on patient and family engagement in research. Researchers may benefit from attending workshops on patient-centered research to discuss processes, methods, and strategies of engagement. In addition, researchers and research staff could benefit from topics such as strategies to promote optimal engagement of older adults (with multimorbidity) and caregivers; how to facilitate communication and team meetings; and how to improve accessibility and dismantle barriers to access (e.g., Accessibility for Ontarians with Disabilities Act). It would also be advantageous to include patient and caregiver engagement in research as a seminar or unit topic in the education of health professional researchers.
Design Specifications
Many of the design specifications were consistent with existing literature, including the actions and products to address recruitment of research partners on health care research teams (Nkimbeng et al., 2020). Participants recommended the use of a variety of recruitment strategies, such as word of mouth, flyers and newsletters, radio advertisements, personal invitations from former research partners, and reaching out to community organizations. This finding was consistent with the Alzheimer Society (2015, p. 8), which suggested recruiting potential participants through “clinics, websites, consumer mail-outs, support groups, and local action groups.”
Novel actions and products that were not previously identified in the existing literature also emerged from the rich and detailed scenarios created by participants. An example of a novel action to address recruitment of research partners involved researchers connecting with potential research partners over coffee, where afterward, interested individuals could then decide to contact the researchers by phone using the contact information provided on the research team’s business card. The accompanying product for this strategy was business cards with the research team’s contact information.
Some of the ideas discussed by participants regarding the provision of respite or caregiving support may not be feasible for all research teams, due to insufficient funding, or if they fall outside of the researchers’ scope of practice. For example, participants from Session 3 created a scenario where the researchers were to ensure that their personas were transitioned from the health research intervention (e.g., regular interactions with a social worker) to community health and social care support services after the study was completed. However, to address funding constraints, participants also discussed the potential of partnering with existing community-based organizations to access funding opportunities, or health and social care services to support the research partners (e.g., transportation or respite care). The accompanying action and product for this subtheme were to build partnerships and compile a list of community health and social care services. This finding was consistent with Nkimbeng et al. (2020), who found leveraging partnerships with community-based organizations or established social programs were a cost-effective strategy for recruiting older adult participants.
The novel design specifications identified from this study can be compiled into a list for further discussion among key stakeholders (e.g., health care researchers, research partners, health care professionals, community health care service providers) to determine the applicability and pragmatism of these actions and products within their own research and partnerships. This would culminate in the development of a knowledge translation and exchange product (e.g., a toolkit, or resource guide) for use by health care researchers to promote meaningful engagement of patients and caregivers as research partners. In this sense, as Valaitis et al. (2019) explained, the persona-scenario method is a knowledge translation and exchange strategy as it facilitates the advancement of a product by involving the users and individuals implementing the strategy.
Study Limitations and Strengths
Overall, the older adult participants enjoyed the persona-scenario method and found it to be stimulating and innovative compared to interviews or focus groups. The benefit of the persona-scenario method over other qualitative methods is participants developing detailed scenarios within one session, which led to an abundance of rich and descriptive design specifications to operationalize the codes, subthemes, and themes that emerged from the data. However, there is no consensus on the best way to apply this method. Little is known about the human and ICT resources required to effectively conduct the persona-scenario exercise, and it is important to note that the persona-scenario method, including the two-phase data analysis, is resource-intensive. Further research is warranted to explore how best to use this method in co-designing health care research interventions with older adults with multimorbidity and their caregivers.
A limitation of the study was that the sociodemographic characteristics and experiences of the study participants were homogeneous due to the convenience and snowball sampling recruitment strategies. A purposive snowball sampling strategy has the potential to recruit like-minded individuals. Future research is warranted that involves a more diverse population in terms of characteristics such as race, income, and education. A future study on this topic could incorporate sampling strategies including maximum variation to see if more varied and textured experiences with research can be explored in scenarios. Participants’ lack of experience in research limited the discussions to the early phases of the research process. Future research is needed that involves participants who have experience designing, implementing, or evaluating health care research interventions, and the development and implementation of knowledge translation and exchange plans. The lack of older adult/caregiver dyads recruited to the study is also a limitation.
Conclusion
Meaningful engagement of patients and caregivers as research partners is a key component of patient-centered research. This study’s findings expand our understanding of the factors influencing the optimal engagement of older adults with multimorbidity as research partners. The implications of these findings are that to optimize meaningful patient engagement among this population, considerations must be made to support the needs and perspectives of research partners during their recruitment, to plan for meaningful engagement, and to establish collaborative relationships. In addition, the persona-scenario method is a promising design that encourages the active engagement of patients and caregivers as research partners in the co-design, implementation, evaluation of health care research, and the dissemination of research findings.
Footnotes
Authors’ Note
This study was approved by the Hamilton Integrated Research Ethics Board (HiREB #2513).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded in part by support from the Ontario Nursing Informatics Group with the Registered Nurses’ Foundation of Ontario, McMaster University, and Dr. Markle-Reid’s Canada Research Chairs Program.