
Abstract
Depression symptoms are key risk factors for suicide; however, older adults differ from younger adults in types of depression symptoms experienced and thus their risk factors for suicide. The present brief report investigated relations between different symptoms of depression and suicide risk and whether these relations are moderated by age. Participants were 944 community-dwelling adults (N = 512, M = 39) and older adults (N = 432, M = 66) from the United States recruited through Mechanical Turk. Participants completed self-report measures on depression symptoms and suicide risk. Age was found to moderate the relation between cognitive-affective and somatic symptoms and suicide risk. Younger age exacerbated the negative effects of these symptoms on suicide risk. The study is the first to investigate whether older adults differed from younger adults in the association between types of depression symptoms and suicide risk and found that the risk posed by cognitive-affective and somatic symptoms was greater for younger adults.
Suicide rates in the United States have increased 35% between 1999 and 2018, from 10.5 to 14.2 deaths per 100,000 (Hedegaard et al., 2020). Middle-aged and older adults are at high risk for suicide, with older adult white males having the highest risk (Conwell et al., 2011). The prevention of suicide is especially challenging among older adults due to their determination, careful planning, and unwillingness to seek help (Conwell et al., 2011). Identification of age-specific risk factors may lead to more effective interventions to prevent suicide for different age groups. Depression is a well-established and prevalent risk factor for suicide with a 12-month prevalence rate of 10.4% and lifetime prevalence of 20.6% among U.S. adults (Hasin et al., 2018). Meta-analysis found that depression was associated with suicidal ideation, attempts, and death (Ribeiro et al., 2018). Given the importance of depression in identifying at-risk individuals, the accurate assessment of depression is essential, especially among older adults whose suicides are particularly difficult to prevent.
Numerous studies suggest that depression may have a more somatic presentation among older adults, for example, sleep, appetite, fatigue problems, as compared to younger adults who may have more affective presentations, for example, dysphoria (Fiske et al., 2009). Greater age is associated with decreases in mood symptoms as well as increases in somatic symptoms (Schaakxs et al., 2017; Yu et al., 2012). Depression severity is a key suicide risk factor (Hawton et al., 2013) and is typically established through a simple count of depression symptoms (e.g., Cukrowicz et al., 2011). However, a sum of all symptoms may not be the most accurate measure of severity, and thus suicide risk, among older adults as depression may have a predominantly somatic presentation among these individuals (Fiske et al., 2009).
Depression is associated with suicide risk; however, research suggests that phenotypical presentations of depression differ by age (Fiske et al., 2009). Thus, cognitive-affective and somatic symptoms of depression may differ in utility in predicting suicide risk depending on the age of the individual. The present brief report investigated the association between cognitive-affective and somatic symptoms of depression and suicide risk among adults and older adults and whether age moderated these relations.
Methods
Procedures
All participants were recruited from Amazon’s Mechanical Turk (Smith et al., 2016). Participants were limited to adults (18+) residing in the U.S. as research indicates that non-U.S. participants provide less reliable data (Smith et al., 2016). Three exclusion criteria were used: (a) failed four of six attention checks or deviated by more than one year on two questions assessing age, (b) multiple survey attempts, and (c) non-U.S. participants. Demographic make-up and attention check success rates of Mechanical Turk studies are comparable to samples recruited through traditional survey methods (Berinsky et al., 2012). The study was approved by the university’s Institutional Review Board and participants provided written informed consent.
Measures
Demographics of age, gender, race, education, marital status, number of children, and employment were assessed at end of survey.
Suicidal Behaviors Questionnaire-Revised (SBQ-R; Osman et al., 2001) is a four-item self-report questionnaire assessing suicide risk. Questions inquired about suicidal ideation and behaviors. Total score ranges from 3 to 18 with higher scores indicating greater risk. Cut-off scores of seven and eight have been used for community adult and older adult samples, respectively (Osman et al., 2001). Cronbach’s alpha was .83. Both skew and kurtosis were abnormal, 1.86 and 3.37, respectively, and thus a logarithmic transformation was applied, reducing the skew to .93 and kurtosis to -.21.
Patient Health Questionnaire-9 (PHQ-9; Kroenke et al., 2001) is a 9-item self-report measure of depression symptoms experienced during the past 2-week period. Each item was rated on a 0 (not at all) to 3 (nearly every day) scale. The PHQ-8 scoring excluding item 9, assessing suicidal ideation, was used in analyses predicting suicide risk. The PHQ-9 and PHQ-8 both demonstrated an internal consistency reliability of .91. Skew and kurtosis were 1.08 and 0.38 for the full scale and 1.01 and 0.14 with item 9 excluded. The cognitive-affective subscale consisted of items one, two, six, and seven and the somatic subscale consisted of items three, four, five, and eight.
Center for Epidemiological Studies Depression Scale 11 item version (CES-D11; Kohout et al., 1993) is a self-report measure of depression symptoms experienced over the past week. Each item is rated on a scale from 0 (rarely or none of the time) to 3 (most or all of the time). Internal consistency reliability was .92 with a skew and kurtosis of .62 and -.52, respectively. The cognitive-affective subscale consisted of items 2, 6, 9, and Reverse-Coded Items 5 and 8 and the somatic subscale consisted of items 1, 3, 4, and 11.
Data Analytic Plan
Separate multiple linear regressions were conducted to investigate the relation between depression subscales and suicide risk, as well as whether age moderated these relations, by entering age (dichotomized at 60) and depression subscale into Step 1 and their interaction into Step 2 of the model to predict risk. Analyses were repeated with age as a continuous variable. Two separate regression models, one with younger adults and the other with older adults, investigated the predictive utility of all individual depression symptoms entered into the model simultaneously. Age and gender were controlled for in all analyses. Analyses were conducted using SPSS Version 21 with two-tailed significance set at α = .05.
Results
A total of 944 participants met criteria and were included in the final analyses. Participants were excluded due to survey incompletion (51 participants), multiple survey attempts (6 participants/12 entrees), and failing attention checks (2 participants). The majority of participants were Caucasian (86.4%), partnered (51.6%), and female (53.3%). The average age of participants was 51.8 (SD = 16.2, range = 18–88) with most having some college education (86.8%), and current employment (68.9%). Age distribution is as follows: 18 to 39 = 31% (N = 296, M = 31), 40 to 59 = 23% (N = 216, M = 52), 60 to 69 = 35% (N = 335, M = 65), 70+ = 11% (N = 97, M = 73).
Older adults age 60+ had lower overall symptoms of depression, PHQ-8 M = 4.17, SD = 4.90; CES-D11 M = 8.07, SD = 6.28, as compared to younger adults; PHQ-8 M = 6.74, SD = 5.90; and CES-D11 M = 10.56, SD = 7.31, p < .05 for all. With respect to subscales, older adults had lower cognitive-affective symptoms, PHQ-8, M = 1.75, SD =2.64; CES-D11 M = 4.04, SD = 3.32; as compared to younger adults, PHQ-8 M = 3.28, SD = 3.38; CES-D11 M = 5.08, SD = 3.76; p < .01 for all. Older adults also had lower somatic symptoms, PHQ-8 M = 2.41, SD = 2.57; CES-D11 M = 3.25, SD = 2.66, relative to their younger counterparts, PHQ-8 M = 3.46, SD = 2.84; CES-D11 M = 4.13, SD = 2.94; p < .01 for all. Finally, younger adults had higher suicide risk scores, SBQ-R = 6.11, SD = 4.09, than older adults, SBQ-R = 4.66, SD = 2.51, p < .01.
Age, measured dichotomously, significantly moderated the relation between the cognitive-affective subscale of the PHQ-8 and suicide risk (p < .05). Age, both measured dichotomously and continuously, also significantly moderated the relation between the somatic subscale of the PHQ-8 and suicide risk (p < .05 for all). Finally, age, measured dichotomously as well as continuously, significantly moderated the relation between suicide risk and both the CES-D11 cognitive-affective and somatic subscales (p < .05 for all). Additional statistics are presented in Table 1.
Age by Depression Moderation Predicting Suicide Risk.
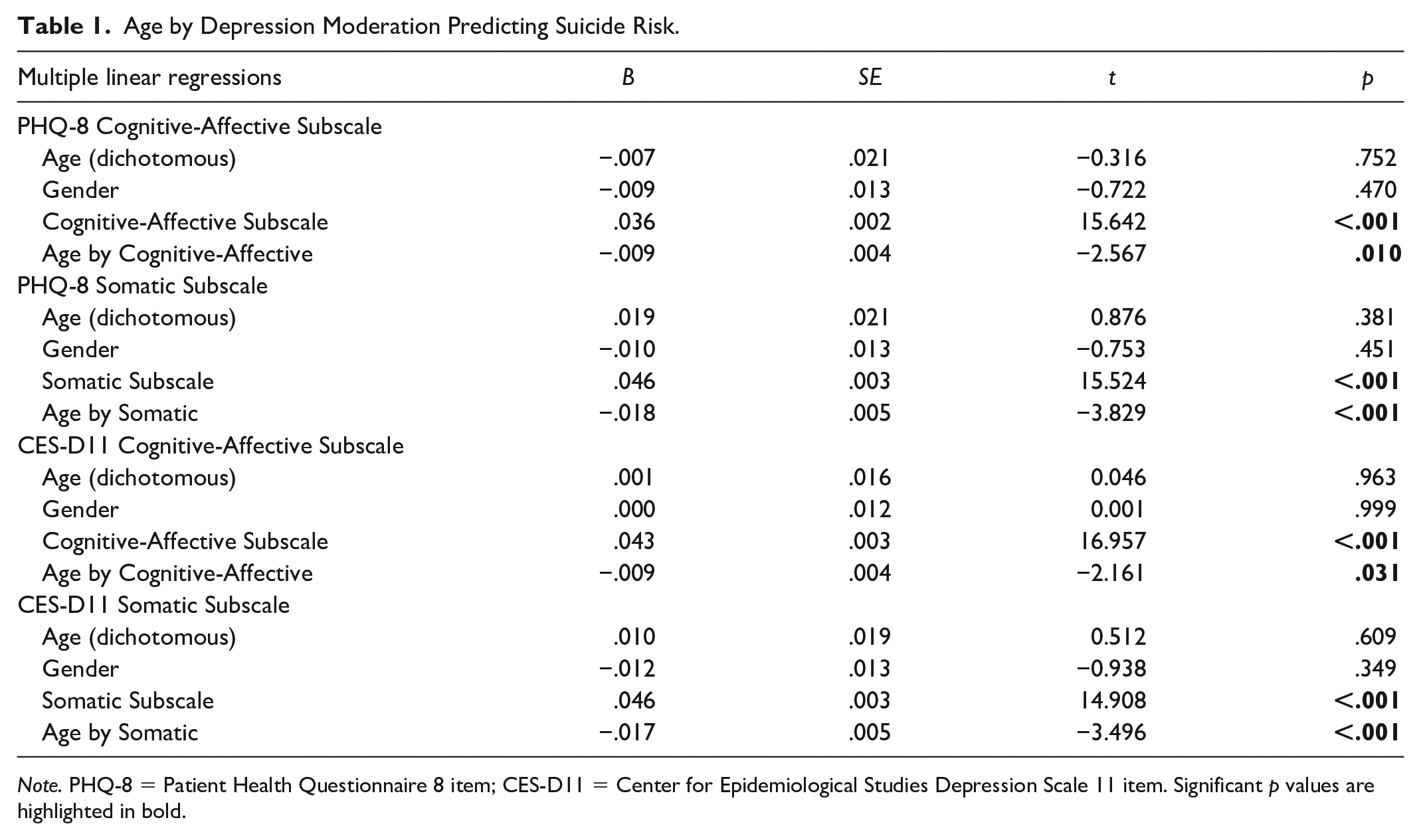
Note. PHQ-8 = Patient Health Questionnaire 8 item; CES-D11 = Center for Epidemiological Studies Depression Scale 11 item. Significant p values are highlighted in bold.
Follow-up graphical depictions of the moderation effect for the PHQ-8 subscales indicated that at higher levels of cognitive-affective and somatic depression symptom severity, younger adults had higher suicide risk scores than older adults with similar levels of depression severity (Figure 1). Patterns were similar for the CES-D11.
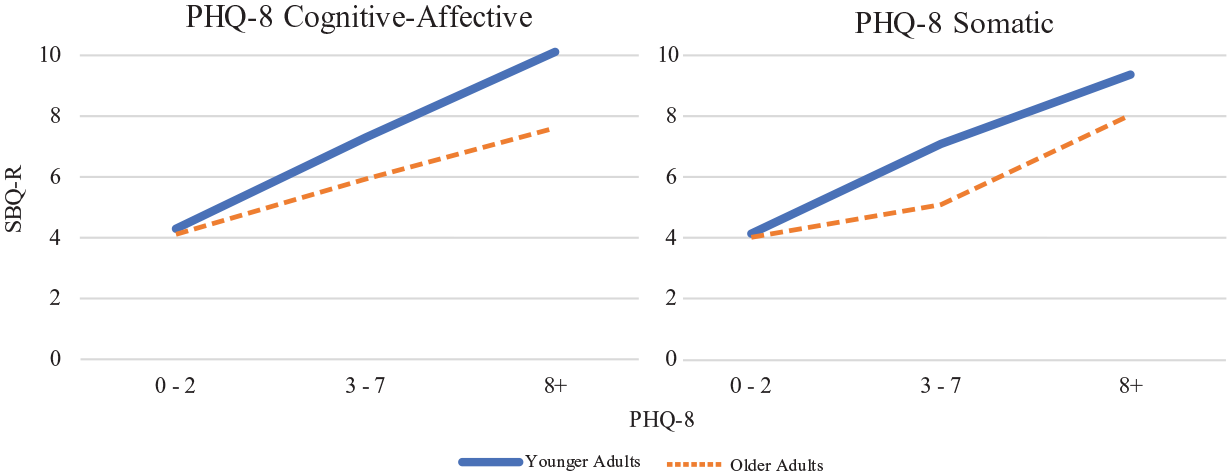
Suicide risk by age group and depression symptom severity.
When all PHQ-8 symptoms were entered into a multiple linear regression model simultaneously to predict suicide risk among younger adults, negative affect, sleep problems, poor self-esteem, and psychomotor problems were significantly associated with risk. Only negative affect and poor self-esteem significantly predicted risk among older adults (Table 2).
Individual Depression Symptoms Predicting Suicide Risk by Age.

Note. PHQ-8 = Patient Health Questionnaire 8 item; CES-D11 = Center for Epidemiological Studies Depression Scale 11 item. Significant p values are highlighted in bold.
In the CES-D11 model predicting risk among younger adults with all items entered simultaneously, negative affect, sleep problems, poor self-esteem, positive affect, and psychomotor problems were significant. Only negative affect, hedonia, and psychomotor problems were significantly associated with risk among older adults (Table 2).
Discussion
The present study investigated whether younger adults and older adults differed in the types of depression symptoms associated with suicide risk. Compared to older adults, younger adults had higher levels of cognitive-affective and somatic symptoms of depression as well as suicide risk. The relations between both types of depression symptoms and suicide risk were moderated by age. Cognitive-affective and somatic symptoms were both associated with suicide risk, though the risks posed by these symptoms were greater for younger adults as compared to older adults with similar levels of depression. The interpersonal theory of suicide states that suicide risk arises from feelings of perceived burdensomeness and thwarted belongingness (Van Orden et al., 2010). The socio-emotional selectivity theory posits that older adults have greater interpersonal and emotional wellbeing because they prioritize maximizing positive close relationships with others (Carstensen, 1995). Across one’s lifespan, individuals shift from maintaining large social networks for pursuit of information and opportunities into maintaining small close-knit groups of friends and family for emotional fulfillment and support (Carstensen, 1995). These behaviors may serve as a protective barrier against experiencing depression (Blazer & Hybels, 2005) as well as the negative impact of depression on feelings of thwarted belongingness and perceived burdensomeness (Kleiman et al., 2014), thus leading to lower suicide risk as compared to younger adults.
Fewer individual depression symptoms predicted suicide risk for older adults. Depressed mood, sleep problems, self-esteem issues, and psychomotor problems consistently predicted suicide risk across both the PHQ-8 and CES-D11 for younger adults. In older adults, however, only depressed mood consistently predicted suicide risk across the two depression measures. Older adults may be less likely to present with mood symptoms (Schaakxs et al., 2017); however, these findings highlight the importance of assessing for suicide risk among those who do endorse depressed mood. Although fewer individual depression symptoms consistently predicted suicide risk among older adults, the present findings indicate that when taken together, both cognitive-affective and somatic symptom severity remain important predictors of risk in this age group.
Several important limitations should be considered when interpreting the relevance of findings. The study used a non-clinical sample comprised of primarily Caucasians with low depression symptoms and suicide risk. Findings will benefit from replication in more heterogeneous and clinically severe samples. Limited number of adults age 70+ were recruited and thus findings will also benefit from replication in larger samples of middle-old and oldest-old adults. Finally, the study utilized a cross-sectional correlational design and thus inferences cannot be made regarding temporal precedence or causality among variables.
These limitations notwithstanding, the present study adds to the literature by being the first to investigate differences among younger versus older adults in the types of depression symptoms associated with suicide risk. Cognitive-affective and somatic symptoms are predictors of suicide risk for both younger and older adults; however, younger age accentuates the negative impact of these symptoms on suicide risk. Adults and older adults presenting with elevated somatic and/or cognitive affective symptoms of depression, particularly depressed mood, would benefit from screening for suicide risk.
Footnotes
Authors’ Note
West Virginia University Institutional Review Board Protocol: 1808231837.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.