
Abstract
This study examined sleep concerns among direct-care workers in long-term care and their perceived need for a sleep intervention. Thirty-five participants reported their sleep concerns and willingness to participate in a sleep intervention with preferred delivery forms/content. Multiple sleep characteristics were assessed via ecological momentary assessment and actigraphy for 2 weeks. Eighty percent reported at least one sleep concern with insomnia-related concerns being most prevalent. Those with insomnia-related concerns tended to have long sleep onset latency, frequent awakenings, suboptimal (long) sleep duration, and long naps. Most participants (66%) expressed interest in participating in a sleep intervention either online or in group sessions; interest was higher in those with insomnia-related concerns. Mindfulness strategies were most preferred, followed by cognitive-behavioral therapy and sleep hygiene education. The high prevalence of insomnia-related concerns in direct-care workers needs to be addressed for the well-being of these workers and for the quality of geriatric care delivery.
Keywords
Introduction
Nursing homes, adult day care centers, hospices, home care agencies, and residential care communities provide long-term care (Harris-Kojetin et al., 2019). Direct-care workers (e.g., nursing assistants, personal care aides, and home health aides) assist older adults with activities of daily living and play important roles in the well-being of older adults (Scales, 2006). Across the multiple settings, their roles require good interpersonal skills to build relationships with older adults and their families, and mental sharpness to notice residents’ physical or cognitive changes and report concerns or safety issues to other members of the care team. Many of these skills and abilities are dependent on good sleep recovery (Gordon & Chen, 2013; Lee et al., 2019); yet direct-care workers face challenging work conditions (e.g., work shift, caregiving stress) that do not support good sleep. In turn, sleep concerns and poor sleep in direct-care workers may result in the high rates of burnout and turnover often observed in this occupational sector (Bamonti et al., 2019; Choi et al., 2020; Konetzka et al., 2005; Rosen et al., 2011).
The most frequently reported sleep concern in general populations is insomnia. Because insomnia is a complaint or a symptom reported by a subject rather than a disease with a particular etiology (Buysse, 2016), it has been underdiagnosed and undertreated (Drake et al., 2003). However, many health care workers experience insomnia symptoms. For example, 13% of Japanese hospital workers have clinical insomnia (Koyama et al., 2017). Since the COVID-19 outbreak, insomnia prevalence in Chinese health care workers has been estimated at 39% across five studies (Pappa et al., 2020). The overall prevalence of insomnia in U.S. health care workers before the onset of COVID-19 is also similarly high at 39% (Jacobsen et al., 2014). Among nursing staff who work extended shifts, the prevalence of insomnia is higher at 54% to 58% (Eldevik et al., 2013).
The stress-diathesis model of insomnia (Drake et al., 2014) guides us to expect a high prevalence of insomnia concerns in direct-care workers due to exposure to stressors. Direct-care workers face many work-related stressors, such as caregiving demands, proximity to chronic disease, and bereavement; all these may be sources of insomnia-related concerns (Jansson & Linton, 2006). Because the majority of direct-care workers are women, many of them are also primary caregivers for their aging parents as well as for their own children (DePasquale et al., 2017). Moreover, direct-care workers have nonstandard shifts that may vary across weeks or months and interfere with their circadian rhythms (Kecklund & Axelsson, 2016), which may increase their vulnerability to insomnia (Booker et al., 2018). For example, in long-term care it is common that a team of direct-care workers is assigned to a group of residents, and the team rotates by use of a predetermined schedule (Burgio et al., 2004). Direct-care workers are also likely to have lower socioeconomic status (Potter et al., 2006), which may indicate a lack of resources to cope with stress. All these factors relate to a high level of burnout in direct-care workers (Bamonti et al., 2019) and may contribute to prevalent insomnia concerns.
To test the stress-diathesis model of insomnia (Drake et al., 2014), this study takes a descriptive approach to examine the prevalence of insomnia-related concerns in direct-care workers. The vulnerability to stress of direct-care workers likely increase insomnia-related concerns, such as indicating difficulty falling or maintaining sleep and not restorative sleep as their sleep concerns (Ohayon & Roth, 2001). To verify their concerns, this study also examines multiple sleep characteristics assessed by self-report and actigraphy over multiple days. For example, those with insomnia-related concerns may have poorer sleep quality, longer sleep onset latency, and more frequent awakenings than those without insomnia concerns (Ohayon & Roth, 2001). Empirical evidence shows that insomnia symptoms may present despite sufficient time in bed (Drake et al., 2003); thus, insomnia concerns may be independent of sleep duration. Moreover, those with insomnia concerns may seek an intervention in an attempt to treat potential sleep problems (Murphy et al., 2007). The current study uses multiple sources of data to understand sleep issues among direct-care workers, which has been rarely done in previous research.
The present study examined insomnia concerns and perceived need for treatment in U.S. direct-care workers. First, we analyzed sleep concerns reported by direct-care workers and categorized them into several themes, including insomnia-related themes. We expected a high prevalence of insomnia-related concerns in direct-care workers. We further verified reported insomnia-related concerns against multiple sleep characteristics assessed by 14-day ecological momentary assessment (EMA) and actigraphy. EMA and actigraphy can assess self-reported and objectively measured sleep characteristics, respectively, in participants’ own naturalistic environments. Second, we assessed willingness to participate in a future sleep intervention and the preferred delivery format/content of the intervention in this sample. We expected that direct-care workers with insomnia-related concerns would exhibit more intention to seek help, which can provide information on the validity of reported concerns. Finally, we examined sociodemographic and work characteristics of this understudied group of direct-care workers and their compliance to the study protocol that can provide useful information for future studies. Findings from this study will provide information important to improve the well-being and retention of long-term care workforce that will ultimately benefit the quality of geriatric care.
Method
Participants
Participants were direct-care workers at an assisted-living community. Inclusion criteria for this study required participants to: (a) be at least 18 years of age, (b) work full-time, (c) provide direct care to the residents, and (d) possess a smartphone to use for ecological momentary assessment (EMA) questions. We did not screen individuals for sleep apnea because this study aimed to capture the prevalence of potential insomnia in direct-care workers including those with sleep apnea and those without. Excluding individuals with sleep apnea may result in underestimating insomnia prevalence as previous research reports comorbidity between insomnia and sleep apnea (Benetó et al., 2009). Out of approximately 40 eligible workers, 37 agreed to participate in the study (93% response rate). Data were lost for 1 participant, and 1 person did not complete a background survey, resulting in 35 participants with complete background survey data. The final sample included personal care assistants, medical aides (who dispense medications to residents), and nurses who provided direct care and had regular contacts with residents.
Procedure
Eligible employees were invited to participate in this study. During an information session, investigators distributed recruitment brochures and explained the importance of the study, study protocol, and compensation for participation. Interested employees were instructed to meet the investigators at a designated place in the workplace to complete informed consent. Subsequently, participants filled out a background survey which included questions about sociodemographic characteristics, work characteristics, and questions regarding sleep concerns and a future sleep intervention (see measures section below for details). Background survey completion took approximately 20 min.
Upon completion of the background survey, participants were provided detailed instructions for smartphone-based EMA. The EMA included four prompts (upon-waking, before-lunch, afternoon, and before-bedtime) per day for 14 days, following best practices of previous EMA studies (Scott et al., 2015). Assessing sleep characteristics across 14 days ensures that the data capture participants’ naturalistic sleep patterns with reducing sampling error (data are not collected from unusual days). The upon-waking prompt included questions about the previous night’s sleep. The other three prompts included questions regarding sleepiness and other daily experiences. Responding to questions in each prompt took 5 min or less. All participants received check-in calls from research assistants after second and seventh day of their study to encourage compliance and address questions.
During the same 14-day period as the EMA, participants were asked to wear an Actiwatch Spectrum plus device which measures wrist movement to quantify sleep and wake patterns. Using Actiware software (v6.09, Philips-Respironics Inc, PA, USA), data were computer-scored using a previously validated algorithm (Buxton et al., 2016). A trained actigraphy scoring team used study-specific sleep criteria to determine the validity of each recording. Any intervals with a 15+ min discrepancy between scorers for sleep duration or timing were reviewed by the senior investigator until agreement. Scoring was adjudicated by consensus.
Compensation was designed to encourage active participation in both EMA and actigraphy data collection. Upon study completion, participants received compensation for their participation in each study with a $10 Amazon gift card. To receive compensation for the actigraphy study, participants were required to wear the device for at least 80% (11 of 14 days) of the study period. To receive compensation for the EMA, participants were required to respond to at least 60% (34 of 56) of the prompts. We also provided an additional $20 gift card for those with high EMA compliance defined as ≥80%. Thus, the maximum compensation that participants could receive was $50. All procedures were approved by the appropriate institutional review boards.
Background Survey Measures
Sociodemographic variables
Participants reported their age, sex, race/ethnicity, annual household income, the highest level of education, current marital status, and the number of children living in the household. Participants also provided information about their work schedule, weekly work hours, and secondary workplaces. Secondary workplace information included whether they had a second job and how many hours per week they worked in that job.
Sleep concerns
To assess participants’ main sleep concerns, we included an open-ended question worded “What is your main concern in your sleep that you want to improve?” Responses were coded as texts.
Interest and preferred form of a future sleep intervention were measured by three questions. The first question asked: “If a sleep-focused intervention is offered in the future (without any financial cost on your part), would you maybe be interested in participating or hearing more information?” Participants answered yes or no. Second, we asked, “For the sleep-focused intervention, which form of delivery would you prefer?” Participants were instructed to select all that apply to them of the following responses: group meetings at the workplace, one-on-one meetings at the clinic, online, or other (specify). Finally, we asked, “If you were to take part in a future sleep-focused intervention, which of the following would you like to participate in?” Again, participants selected all responses that applied to them: sleep hygiene education, mindfulness-based stress reduction, cognitive-behavioral therapy for insomnia, or other (specify).
EMA Sleep Measures
We selected five EMA sleep measures that capture qualitative dimension of sleep: sleep sufficiency, sleep quality, sleep onset latency, nocturnal awakenings, and sleepiness. These five measures were adapted from previous studies (Buysse et al., 1989; Lee et al., 2019). Except sleepiness, all the items were asked during the upon-waking prompt, which was participant-initiated to avoid interrupting participants’ sleep. Table 1 shows details of these sleep measures, including each question and response options.
EMA and Actigraphy Sleep Measures and Descriptive Statistics.
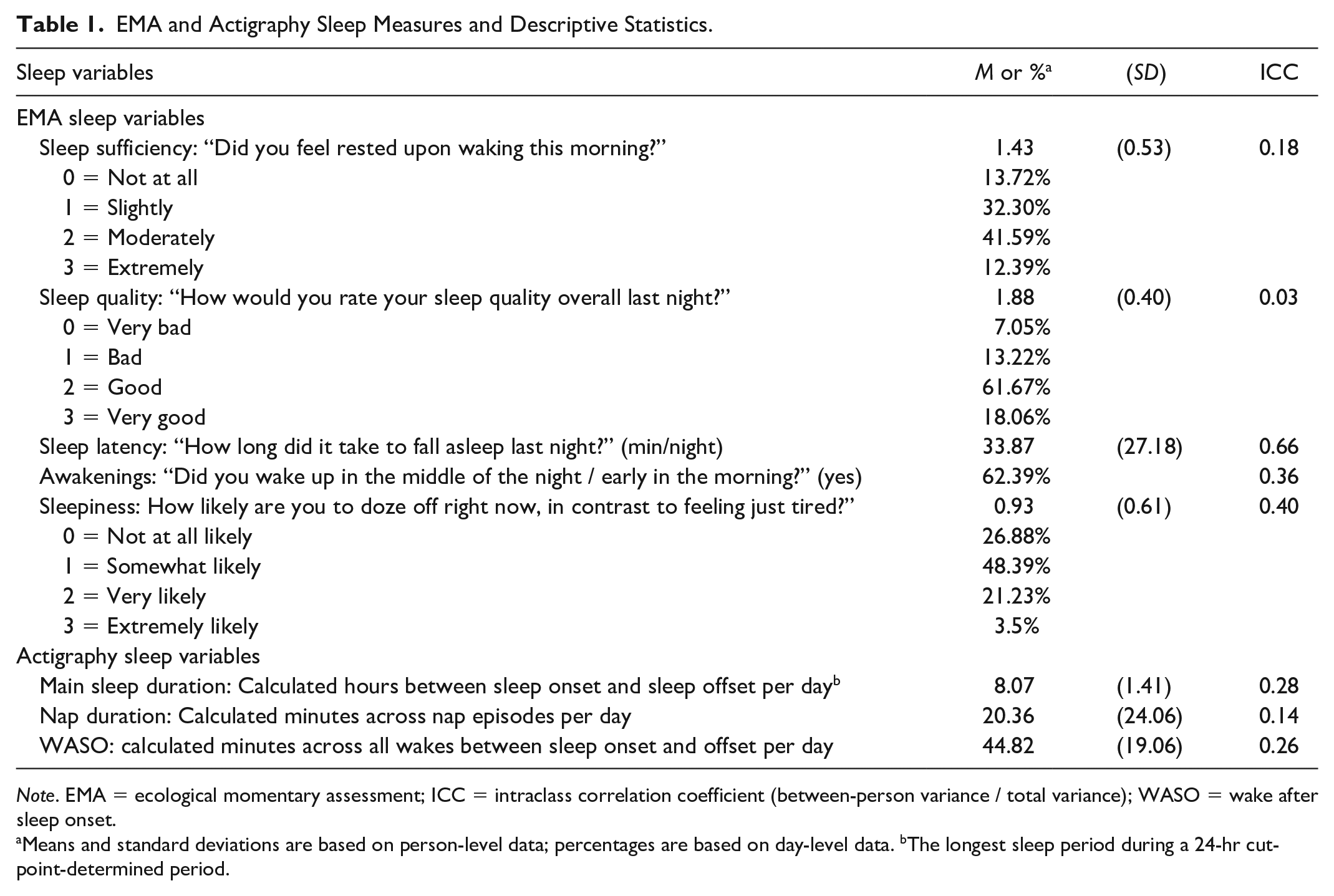
Note. EMA = ecological momentary assessment; ICC = intraclass correlation coefficient (between-person variance / total variance); WASO = wake after sleep onset.
Means and standard deviations are based on person-level data; percentages are based on day-level data. bThe longest sleep period during a 24-hr cut-point-determined period.
Actigraphy Sleep Measures
We selected three actigraphy sleep measures that encompass the duration and efficiency of sleep. Those are main sleep duration, nap duration, and wake-after-sleep-onset (WASO). Table 1 shows how these sleep variables were calculated. The cut-point of each day, which is the time at which a 24-hr period begins and ends, was determined individually for each participant as the clock time closest to 12:00 p.m. that (a) does not cut through a main sleep period, (b) maximizes the number of valid days, (c) intersects the fewest number of naps, and (d) intersects the fewest number of off-wrist periods.
Analytic Strategy
We analyzed open-ended responses with a qualitative content analysis. We used grounded theory (GT) as a guide to the qualitative method of inquiry (Charmaz, 2006). An advantage of the GT method is its systematic approach that provides scientific rigor and trustworthiness in the emerging theory or phenomenon (Burgess et al., 2018). GT follows several steps for a purposive inquiry, including initiating a research question (“what are sleep concerns in direct-care workers?”), developing assumptions (“insomnia-related concerns may be prevalent”), having theoretical sensitivity based on a literature review (e.g., “waking up in the middle of the night, waking up too early, or not feeling rested upon waking” are symptoms related to insomnia), and conducting an iterative data analysis to generate new knowledge.
Following the suggested steps, first, the lead authors (first and second authors) reviewed coded texts and identified key themes that emerged across multiple participants. At this step, seven common themes were identified: not enough hours of sleep, difficulty falling and/or staying asleep, not feeling rested upon waking, sleep disorders (apnea, insomnia, etc.), sleep schedule, overactive and/or stressful thoughts, and other response. Second, using the seven themes, three trained undergraduate-level scorers independently categorized each response into primary and secondary themes. The three scorers had previous experience of coding open-ended responses for a similar project. The individual coding was undertaken remotely without discussing with other coders. Third, the lead authors adjudicated categorization discrepancies between individual scorers. Out of 28 coded cases (28/35 responded to the open-ended question), there were three discrepancies in the categorization into primary themes. These cases were fully discussed by considering both primary and secondary themes suggested by the scorers. Finally, all responses were finally categorized into primary and secondary themes by consensus.
Next, we used descriptive statistics to summarize data and compare sleep characteristics between groups (i.e., those with insomnia-related concerns vs. those without, and those with interest in sleep intervention vs. those without). For sleep variables that have previously defined clinical cutoffs (i.e., sleep onset latency, frequency of nocturnal awakening, main sleep duration, nap duration, and WASO), we made additional group comparisons by the prevalence of suboptimal sleep condition suggested by previous research (Ohayon & Roth, 2001; Watson et al., 2015).
Results
Descriptive Statistics
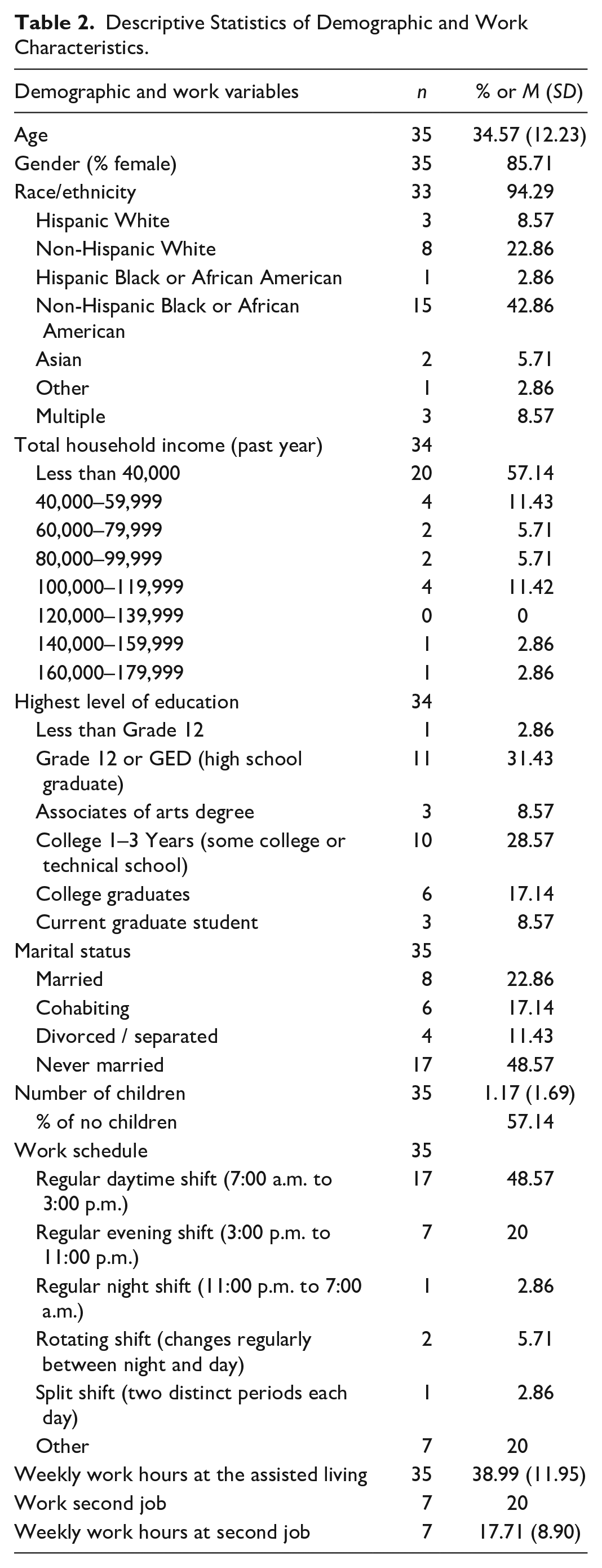
Participants (n = 35) were 35 years old on average, mostly female (86%), and primarily African American (46%). Most participants had a household income below $40,000 (57%). Most (69%) of participants worked the daytime shift of 7:00 a.m. to 3:00 p.m.; 20% worked evening shift of 3:00 p.m. to 11: p.m. and 11% worked other rotating shift (one that changes regularly) or split shift (one consisting of two distinct periods each day). Detailed descriptive statistics for demographic and work characteristics are provided in Table 2. In terms of average sleep characteristics, perceived sleep sufficiency and sleep quality were less than “good.” Sleep onset latency was averaged at 33.87 min. On 62% of the study, participants had nocturnal awakenings. Average main sleep duration was 8 hr 4 min; average nap duration per day was 20.36 min per day. Mean WASO was 44.82 min per main sleep period. Intraclass correlation coefficients (ICCs) for most of these sleep variables (except sleep latency) were less than 0.5, meaning that there was more within-person variability than between-person variability in the sleep variables (Table 1).
Descriptive Statistics of Demographic and Work Characteristics.
Compliance to the Study Protocol
Figure 1 shows the flowchart of study participation across the background survey, EMA, and actigraphy. Of the 35 background survey participants, 33 agreed to participate in the EMA study and 31 completed EMA. Among these, only 23% received additional compensation for high compliance at 80%. Of the 31, 30 participants provided any valid sleep data during the study period. There were invalid upon waking prompts and missingness in some sleep variables, and thus the number of final EMA participants varied by sleep variables (30–26). For the actigraphy study, 32 participants agreed to participate and 30 wore the actigraphy device during the 14-day study period. However, two participants provided all invalid actigraphy days (e.g., >4 hr of off-wrist time), resulting in 28 participants with valid actigraphy data.
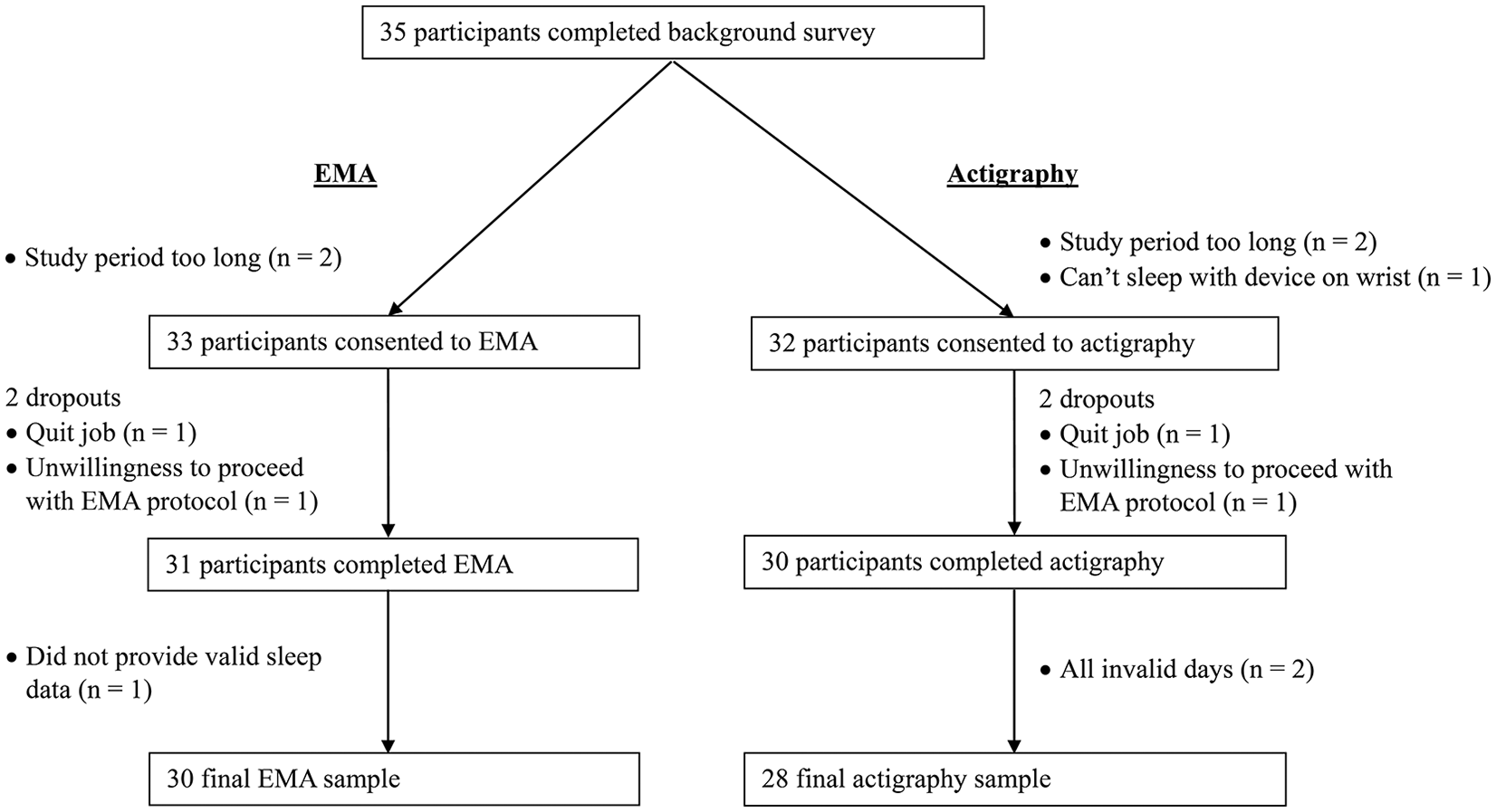
Flowchart of direct-care workers’ participation across background survey, ecological momentary assessment (EMA), and actigraphy study.
Qualitative Themes on Main Sleep Concerns
Of the 35 participants, 28 (80%) responded to the open-ended question asking main concerns in their sleep. Several common themes emerged across responses (Figure 2). Participants’ responses were categorized into the following six primary themes: difficulty falling and/or staying asleep (n = 15), not feeling rested upon waking (n = 3), not enough hours of sleep (n = 3), sleep disorders (e.g., apnea, insomnia) (n = 2), overactive and/or stressful thoughts (n = 1), or some other response (n = 4). Thus, insomnia-related concerns that comprise of difficulty falling and/or staying asleep, not feeling rested upon waking, and sleep disorders (specifically insomnia) were the most prevalent with 57% (n = 20) indicating as their main sleep concern.
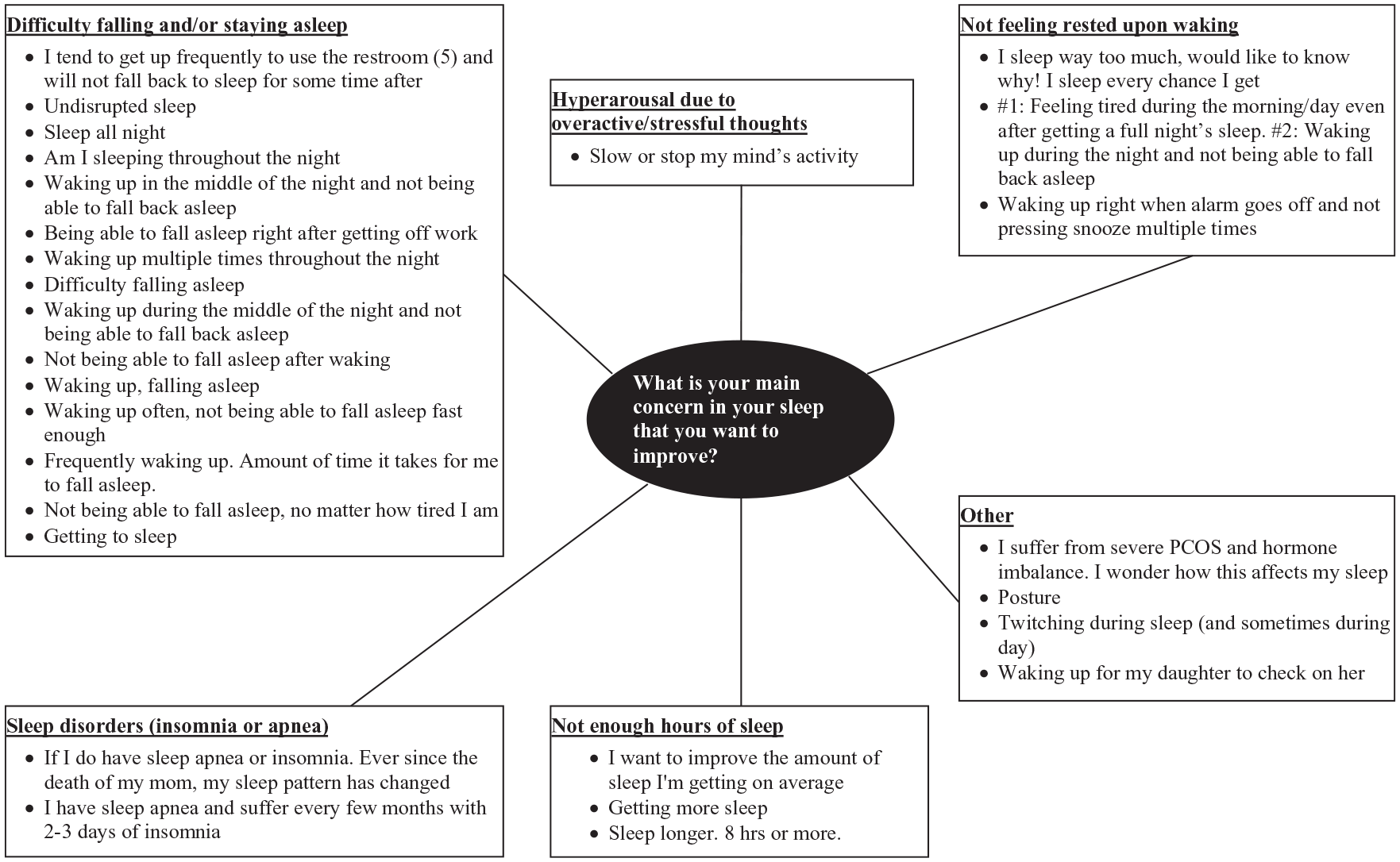
Participants’ main sleep concerns: Qualitative themes and participant narratives.
EMA and Actigraphy Sleep Characteristics
Table 3 shows comparisons of sleep characteristics between those with insomnia-related concerns versus those without. Given the small cell size, formal statistical analyses were not conducted to test for statistically significant differences between the two groups. Participants who indicated insomnia-related concerns tended to have longer sleep onset latency, more frequent awakenings, and suboptimally longer sleep duration, longer naps than those who did not indicate any insomnia-related concern. The two groups did not seem different in perceived sleep sufficiency, sleep quality, and sleepiness, although differences in these sleep variables were apparent on workdays, not on non-workdays (Online Appendix 1). Those with insomnia-related concerns exhibited great variability in most of the sleep variables between workdays and non-workdays.
EMA and Actigraphy Sleep Characteristics by Subgroups.
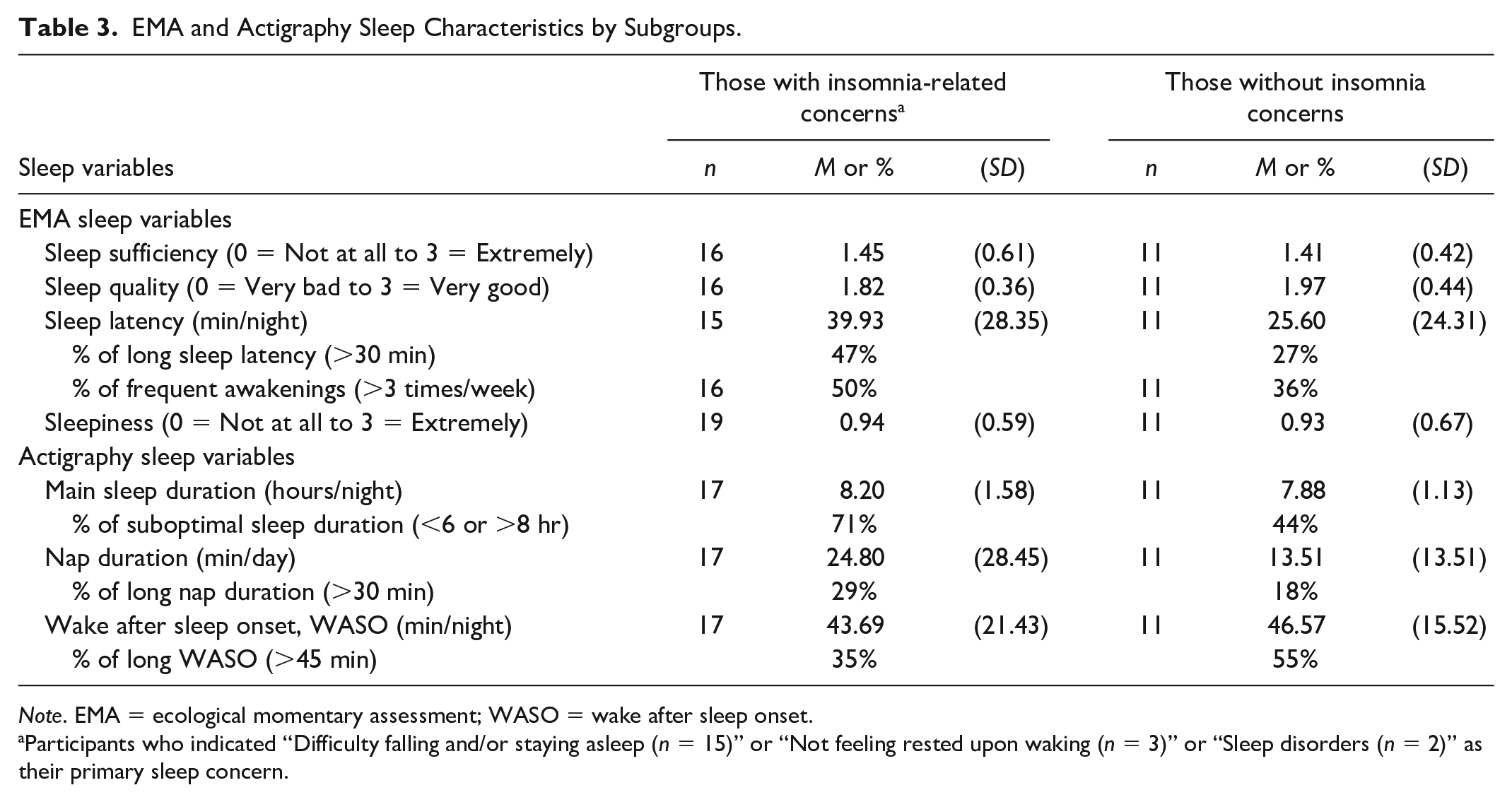
Note. EMA = ecological momentary assessment; WASO = wake after sleep onset.
Participants who indicated “Difficulty falling and/or staying asleep (n = 15)” or “Not feeling rested upon waking (n = 3)” or “Sleep disorders (n = 2)” as their primary sleep concern.
Interest and Preferred Form of a Future Sleep Intervention
Sixty-six percent of the background survey participants (n = 23, out of 35) expressed interest in participating in a future sleep intervention. As expected, the interest was higher among those who indicated insomnia-related concerns (n = 14) versus not (n = 9). Online or group formats were preferred (46% for both) over one-on-one meetings at the assisted living community (14%). As for sleep intervention content preferences, participants preferred mindfulness-based strategies (80%) followed by cognitive-behavioral therapy (14%), and sleep hygiene education (3%).
Table 4 shows the comparison of EMA and actigraphy sleep characteristics between those who expressed interest in participating in a future sleep intervention versus those who did not. Differences between the groups were apparent in EMA sleep quality, sleep onset latency, frequency of awakenings, sleepiness, and actigraphy-measured nap duration and WASO. Participants who expressed interest tended to have poorer perceived sleep quality, longer sleep onset latency, more frequent awakenings, and less sleepiness. Furthermore, participants who indicated interest tended to have shorter nap duration and longer WASO than those who did not indicate interest. The two groups did not seem different in perceived sleep sufficiency and actigraphy sleep duration.
EMA and Actigraphy Sleep Characteristics Between Those Interested in Sleep Intervention Versus Not.
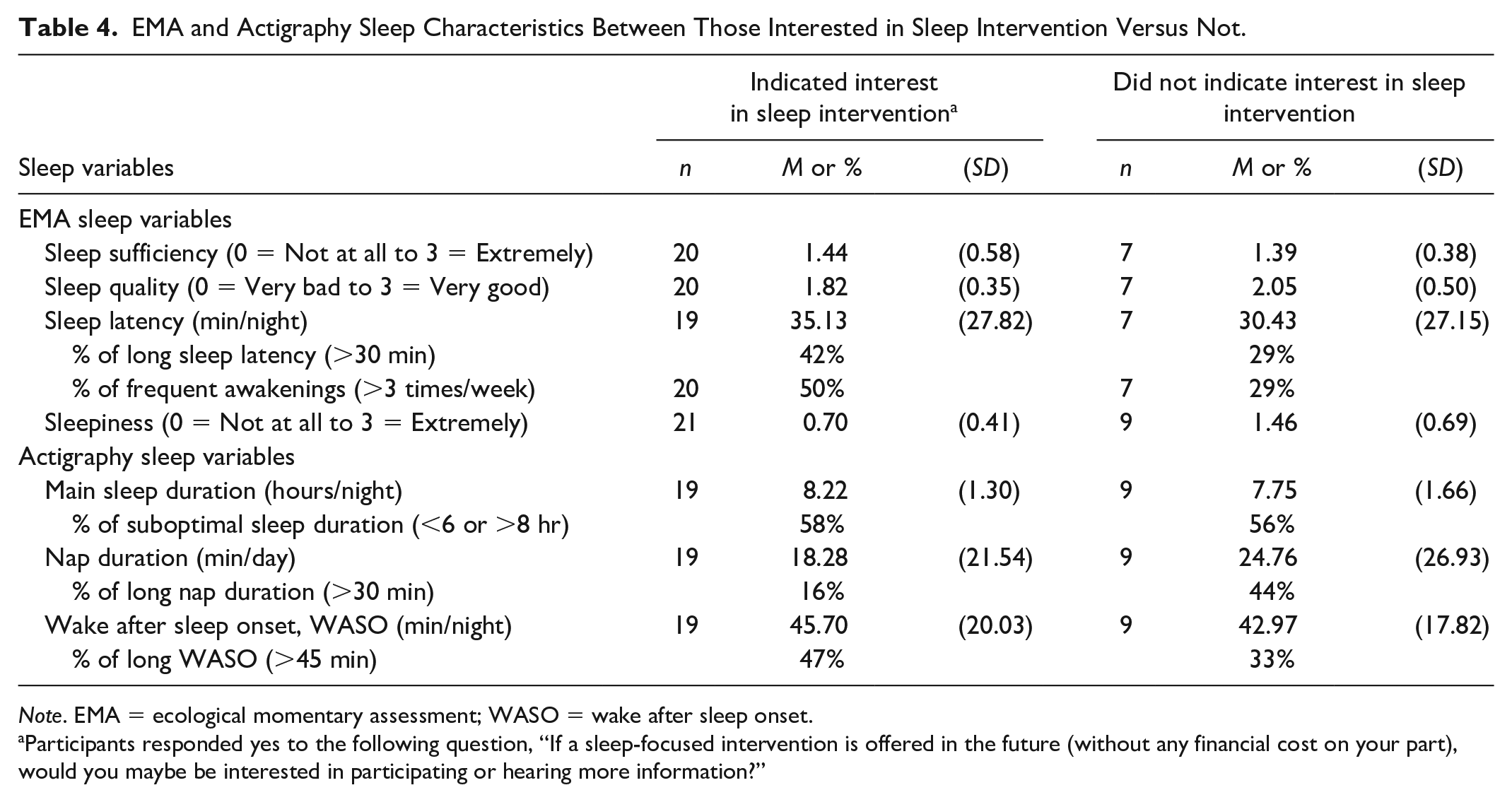
Note. EMA = ecological momentary assessment; WASO = wake after sleep onset.
Participants responded yes to the following question, “If a sleep-focused intervention is offered in the future (without any financial cost on your part), would you maybe be interested in participating or hearing more information?”
Supplementary Analyses
We examined whether reported sleep concerns were reflected in relevant EMA and actigraphy sleep characteristics (Online Appendix 2). For example, we checked whether participants who indicated “difficulty falling and/or staying asleep” as their primary concern exhibited longer sleep onset latency and longer WASO. Generally, EMA and actigraphy supported what participants reported as their main sleep concern. Those who indicated “not enough hours of sleep” as their sleep concern tended to have shorter sleep duration than those without the concern, although their sleep duration was in the optimal range (6 ≤ hr/night ≤ 8). Participants who indicated “difficulty falling and/or staying asleep” as the main sleep concern had longer sleep onset latency, although they did not have longer WASO. Participants who indicated “not feeling rested upon waking” tended to have lower sleep quality than who did not. All of the participants who indicated sleep disorders (specifically insomnia) reported frequent awakenings, whereas this percentage was lower for those who did not indicate sleep disorder concern.
In addition, in our sample, three participants reported ever having physician-diagnosed sleep apnea and all these three participants indicated having insomnia-related concerns. We further examined differences by work schedule. Insomnia concerns seemed more prevalent in those with rotating or split shifts (75%) than in those with day or evening shifts (54%, 57%, respectively). Interest in a sleep intervention seemed higher among those with evening shift (71%) compared with day shift (67%) and rotating or split shifts (50%). There were no differences in preferences for intervention contents. Regarding delivery formats, group meetings were more preferred by day-shift workers; online format was more preferred by evening-shift workers.
Discussion
This study is one of the first reporting the prevalence of insomnia-related concerns and perceived need for a sleep intervention in a sample of direct-care workers in long-term care. Building on the stress-diathesis model of insomnia (Drake et al., 2014), we expected that many direct-care workers would exhibit insomnia-related concerns. Our results supported this expectation. The majority of direct-care workers had a sleep concern, and insomnia was the most prevalent form of their sleep concerns. Most participants expressed interest in participating in a sleep intervention if it is offered in the future. The current study uniquely contributes to the literature on geriatric care by showing the high prevalence of insomnia concerns and high demand for a sleep intervention in direct-care workers. Our findings have implications for the quality of geriatric care and geriatric workforce retention, two important agenda in long-term care. That is, addressing the concerns and symptoms of insomnia in direct-care workers may help improve quality of care delivery and reduce high turnover rates often observed in residential care communities (Bamonti et al., 2019; Choi et al., 2020; Konetzka et al., 2005; Rosen et al., 2011).
In this study, the prevalence of direct-care workers with insomnia-related concerns was 57%. This was similar to the previously reported 54%–58% of clinical insomnia among nursing staff who worked extended shifts (Eldevik et al., 2013). The previous study used a large sample of 1,990 Norwegian nurses, and clinical insomnia was determined by Bergen Insomnia Scale. Our study that used a different method (qualitative open-ended responses) yielded a consistently high prevalence of insomnia-related concerns. Perhaps, this prevalence may have been increased since the COVID-19 disease outbreak. For example, during the COVID-19 pandemic, insomnia prevalence in Chinese hospital staff (medical doctors, nurses, administrative staff, etc.) was reported at 39% (Pappa et al., 2020). Of the hospital staff with insomnia, the vast majority (70%) were nurses (Zhang et al., 2020). Compared with nurses in hospital settings, direct-care workers have less resources and may encounter more challenges to support vulnerable older residents (Choi et al., 2020; Potter et al., 2006). Findings from this study suggest that direct-care workers are a particularly vulnerable group for insomnia, and future studies may need to focus more on assisting this population.
Main sleep concerns reported by direct-care workers were qualitatively examined and compared with EMA and actigraphy-measured sleep characteristics. Compared with those without insomnia concerns, those with insomnia-related concerns tended to have suboptimally longer sleep duration, longer nap duration, longer sleep latency, and more frequent awakenings during the night or early in the morning. Given that insomnia is related to hyperarousal around bedtime and sleep maintenance problems (Drake et al., 2003), longer sleep onset latency and frequent awakenings among those with insomnia concerns are not surprising and consistent with previous research (Ohayon & Roth, 2001). Studies also report that insomnia symptoms may exist independent of sufficient sleep time (Drake et al., 2003), which may explain longer nighttime sleep and longer naps found in those with insomnia concerns. Furthermore, participants with insomnia concerns exhibited greater variability in sleep characteristics between workdays and non-workdays, which may exacerbate their symptoms due to irregular sleep patterns. Taken together, the EMA and actigraphy sleep characteristics of those with insomnia concerns were consistent with the empirically defined criteria for insomnia, providing the validity of self-reported concerns in direct-care workers.
Despite the fact that many direct-care workers in our sample were balancing many roles and demands as found in previous research (DePasquale et al., 2017), most expressed interest in participating in a future sleep intervention study. Participants with insomnia-related concerns expressed a higher interest in participating in a future sleep intervention than participants without insomnia concerns. This indicates that not only are their sleep concerns valid and real, but they are interested in doing something to resolve the issues (Murphy et al., 2007). Moreover, those who expressed interest in a sleep intervention tended to have poorer sleep quality, longer sleep onset latency, frequent awakenings, longer WASO than those who did not. The results indicate that those with more sleep problems (problems related to insomnia) are more likely to seek help. Note that participants who were willing to participate in a sleep intervention also tended to report less sleepiness and have shorter nap duration. This finding is intriguing, perhaps suggesting that help-seeking behavior is associated with more alertness and higher attention. Because our descriptive study cannot determine the statistical significance of these differences, future studies with larger samples may need to replicate our findings.
Among insomnia-related concerns reported by direct-care workers, difficulty initiating sleep and/or maintaining sleep were most prevalent. Future interventions targeting to improve these workers’ insomnia concerns may need to focus on decreasing stress-related arousal around bedtime and improving stimulus control. For example, mindfulness training may reduce hyperarousal by reducing stress and rumination that may interfere with sleep onset (Garland et al., 2016). This also corresponds to the intervention components preferred by the participants, as mindfulness strategies were most preferred, followed by cognitive-behavioral therapy for insomnia, and sleep hygiene education. Considering intervention formats preferred by direct-care workers, an online sleep intervention that includes mindfulness strategies may be promising. It could also incorporate online group discussions, as group discussions were also preferred by these workers and found to be an effective treatment for insomnia with benefits similar to those produced by in-person treatments (Koffel et al., 2015). During global pandemic crises, arranging physical group meetings may be challenging, but facilitating group discussions online may satisfy the needs. Information obtained from this study may guide the design of a sleep intervention for direct-care workers who stand in the frontline during public health crises.
Limitations and Future Directions
The primary limitation of the current study is a small sample size and lack of generalizability. Given that there is a lack of studies examining sleep issues in direct-care workers at assisted living by using multiple sources of data, this pilot study was designed to generate preliminary data for a larger study, and thus only a single assisted living community was sampled. Although we recruited all eligible participants and achieved a high response rate, staff size in the study site was small to begin with and we targeted an even smaller group of the staff who provided direct-care to residents. The high estimated prevalence of insomnia concerns found in this study should be verified in a representative sample of direct-care workers to better guide future research. Specifically, although findings from this pilot study may be limited in generalizability, they still motivate that future research examining sleep issues across multiple assisted living communities is warranted. In addition, when we asked preferred content/format of a sleep intervention, we did not provide detailed information (e.g., success rate) but just provided options to choose. We do not know how lack of information on the options might have influenced their choices. Also, we do not know about factors associated with their preferences. For example, those with high work demands might have indicated no interest in a sleep intervention, even though they are the ones who need it most. Future research could assess preferences on a sleep intervention by considering these issues.
Despite these limitations, our study is unique in examining insomnia concerns in direct-care workers, which has not been done before. Future research could examine whether insomnia and overall sleep problems in direct-care workers are associated with their turnover intentions, and further with factors related to quality of care, including staffing and interactions with residents (Gordon & Chen, 2013). Future efforts may also require structural changes in assisted living (e.g., infrastructure reform), as such efforts are sorely lacking (Choi et al., 2020; Kelly et al., 2020) but may have positive effects on sleep health and retention of workers (Perreira et al., 2019).
Conclusion
This first study found that insomnia-related concerns were common in this sample of direct-care workers, and the concerns were mostly supported by subjective and objective measures of daily sleep. Moreover, this sample expressed interest and willingness to participate in a future sleep intervention study and provided preferred format/content for said intervention. Findings from this study represent initial steps to determining the need, acceptability, and potential format of a future sleep intervention for direct-care workers who need better sleep for their own well-being as well as for the health of their care recipients.
Supplemental Material
sj-pdf-1-jag-10.1177_0733464820978612 – Supplemental material for Prevalent Insomnia Concerns and Perceived Need for Sleep Intervention Among Direct-Care Workers in Long-Term Care
Supplemental material, sj-pdf-1-jag-10.1177_0733464820978612 for Prevalent Insomnia Concerns and Perceived Need for Sleep Intervention Among Direct-Care Workers in Long-Term Care by Soomi Lee, Taylor F. Vigoureux, Kathryn Hyer and Brent J. Small in Journal of Applied Gerontology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported, in part, by the University of South Florida Internal Grant Program (PI: Lee, Grant No. 0134930).
Ethics Statement
The University of South Florida Institutional Review Board (IRB) approved the ethical standard of the study protocol (IRB protocol number: Pro00040338).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.