
Abstract
Telehealth interventions improve health outcomes by increasing access to care. We conducted a systematic review to synthesize evidence on the effect of telehealth interventions compared with no intervention or usual care for older adults with pre-frailty or frailty for physical function, quality of life (QOL), and frailty. We searched for randomized controlled trials (RCTs) in MEDLINE, PubMed, Embase, CINAHL, Cochrane, PsycINFO, and SPORTDiscus. Two authors reviewed records and assessed risk of bias. A narrative synthesis of findings was conducted. When appropriate, the standard mean difference (SMD) was used to compare telehealth interventions with control conditions. We used GRADE to determine the certainty of the evidence. Twelve RCTs were included. Low certainty evidence highlighted positive effects for the function and mental component of QOL favoring telehealth interventions (SMD = 0.31, 95% CI = [0.15, 0.47]; and SMD = 0.43, 95% CI = [0.22, 0.64], respectively). Despite a small positive effect of telehealth interventions, insufficient, and low certainty evidence precludes making definitive recommendations.
Introduction
Worldwide, the population of older adults, aged 65 years and older, is rapidly increasing and estimated to reach 2 billion by 2050 (Kinsella & Phillips, 2005). One of the most challenging consequences associated with aging is frailty: an “at risk state” caused by an age-associated accumulation of deficits, such as disease and disability (Rockwood & Mitnitski, 2011). Frailty creates functional impairments for community-dwelling older adults (Aihie Sayer et al., 2014), that could lead to difficulties in completing tasks (activity limitation), or problems with involvement in life situations (participation restriction) (Stucki et al., 2002). Based on data from a systematic review, the prevalence of frailty in community dwelling adults aged 65 years and older was estimated at approximately 11% of the population and is more common in older women (Collard et al., 2012).
The two most common measures of physical frailty in the literature (Clegg et al., 2013; Yaksic et al., 2019) are the Clinical Frailty Scale (CFS) (Rockwood et al., 2005), and Fried et al. (2001) phenotype. The CFS is based on clinical opinion and considers older adults’ comorbidities, cognitive impairment, and disability (Rockwood et al., 2005). The Fried et al. (2001) phenotype is based on five pre-defined criteria including, involuntary weight loss, exhaustion, reduced activity, slow gait speed, and lower grip strength. If an older adult demonstrates only one or two of the criteria, he or she is in the pre-frailty stage, a transitional period that may improve with rehabilitation.
A recent scoping review (Puts et al., 2017) identified different approaches, such as exercise-based interventions (Dorresteijn et al., 2016) and nutritional support (Neelemaat et al., 2011), may provide benefits for people with frailty, their families, and society. However, access to such interventions is limited for older adults with physical frailty (Passalent et al., 2010). Telehealth is one means of increasing access to care and improving health outcomes (Ekeland et al., 2010). Telehealth is an umbrella term covering health care delivered remotely, such as telemedicine and a variety of non-physician services, including mobile health (mHealth, e.g., mobile applications) and electronic health (eHealth, e.g., patient education portals) (Weinstein et al., 2014).
To our knowledge, there is only one systematic review on the effect of telehealth interventions for older adults with frailty (Barlow et al., 2007), and one systematic review for the general population of older adults without severe chronic medical conditions (Muellmann et al., 2018). While the review for older adults with frailty and telehealth was promising, it included different study designs in the synthesis (Barlow et al., 2007). The other review compared eHealth interventions with non-eHealth interventions or no interventions on physical activity for older adults in the general population. Therefore, these results may not be generalizable for older adults with frailty (Muellmann et al., 2018).
To address the gap in knowledge for older adults with frailty and telehealth, we conducted a systematic review of randomized controlled trials (RCTs) to identify and synthesize available evidence. We were particularly interested in the effect of telehealth on physical function and health-related quality of life in pre-frail or frail community-dwelling older adults. We further aimed to describe and consider important contextual information such as definition of frailty and type of telehealth intervention.
Methods
We conducted a systematic review following the guidelines established by the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) (Moher et al., 2010), and registered the title and protocol on PROSPERO (CRD42018100504).
Eligibility Criteria
We included peer-reviewed RCTs which met the following criteria: population: community-dwelling older adults, aged 65 years and older, who were identified as pre-frail or frail (Fried et al., 2001); intervention: health programs delivered (alone or in combination) remotely by telephone or smartphones (i.e., audio/video calls, texts, mobile or tablet applications [app]), computers (i.e., website, email), or DVD-based interventions: we did not include interventions that only focused on nutrition; comparator: no training or usual care; outcomes: our primary outcome was physical function, that is, functional ability and behavioral performance, including functional status assessment, functional impairment, and disability measured with either self-reported questionnaires or objective physical performance tests (Paterson & Warburton, 2010). Our secondary outcomes included other functional domains (e.g., mobility, balance, and physical activity) (Fairhall et al., 2011), self-report domains (e.g., health-related quality of life, life satisfaction), falls, and change in frailty status. When outcomes were measured using different methods in the same study, we chose data from the objectively measured tools or instruments to include in the meta-analyses.
Information Sources
We searched the following databases for all languages and years until 18 March 2020: MEDLINE (Ovid), PubMed, Embase (Ovid), Cumulative Index to Nursing and Allied Health Literature (CINAHL), Cochrane Central Register of Controlled Trials (CENTRAL), PsycINFO, and SPORTDiscus. The first reviewer (E. E.) conducted a forward and backward (reference list) citation search for included studies, and two systematic reviews (Barlow et al., 2007; Muellmann et al., 2018) and one scoping review (Puts et al., 2017) to find relevant papers for screening. We performed a focused “allintitle” search for keywords in Google Scholar; and searched Theses Canada Portal, the ProQuest Dissertations and Theses Global, the EthOS, registry of clinical trials (clinicaltrials.gov), and the World Health Organization (WHO) international clinical trials registry platform (http://www.who.int/ictrp/en/). For publications in languages other than English, we contacted the corresponding author for an English version, or used Google Translate.
Search
The Medical Subject Headings (MeSH) terms, and keywords for frailty and telehealth were used to develop our search strategy at MEDLINE (Ovid). The search strategy in Supplementary Figure 1 was used as the foundation for searching the remaining databases.
Study Selection
Covidence (Covidence, Victoria, Australia) was used to remove duplicates and screen at Level 1 and 2. Two authors (E. E., M. C. A.) independently screened the titles and abstracts (Level 1), and excluded citations that did not meet the inclusion criteria; for example, studies with different patient populations, no telehealth interventions, and study designs other than an RCT. A third reviewer (W. C. M.) adjudicated any unresolved discrepancies. We repeated this process for the full text screening (Level 2), and recorded reasons for exclusion only at this level. We emailed the corresponding author if we had any questions.
Data Collection Process and Items
One author (E. E.) extracted data and a research assistant reviewed it for accuracy. We extracted the following information: author, country, study sample, sampling frame and recruitment, mean and standard deviation (SD) for age, sex, gender, outcome measure used to define frailty, description of interventions, data collection timepoints, primary and secondary outcome measures, reported adverse events or withdrawals (with reasons), and main results.
Risk of Bias
We used the Cochrane Collaboration’s Risk of Bias tool for RCTs (Higgins, Savović, et al., 2019). The summary of assessments was reported as “low risk of bias,” “unclear risk of bias,” or “high risk of bias.” The risk of bias for incomplete outcome data was reported as high, if the attrition rate was greater than 20%. Two authors (E. E., M. C. A.) independently adjudicated scores in Covidence and discussed any discrepancies. The third reviewer (W. C. M.) adjudicated any unresolved discrepancies. Concealing group allocation from participants is a challenge in RCTs involving exercise, physical activity, and/or telehealth interventions (Baker et al., 2010). Therefore, we discussed if the knowledge of group allocation for participants and personnel could change behavior, and introduce bias (Higgins, Savović, et al., 2019).
Synthesis of Results
We conducted a narrative synthesis of findings, and meta-analyses when appropriate. We used Review Manager (RevMan) Version 5.3 (Copenhagen, The Nordic Cochrane Center, The Cochrane Collaboration, 2014) for meta-analyses. We used the standardized mean difference (SMD) of change from baseline for continuous variables, due to different scales, and 95% confidence intervals (CIs) (Deeks et al., 2019). We imputed the change from baseline SDs using correlation coefficient if SDs were missing (Higgins, Li, & Deeks, 2019). Random effects models, using the DerSimonian-Laird (DL) method incorporated in RevMan (Cornell et al., 2014), were used with the assumption that the observed differences among studies are due to the intervention effects (Deeks et al., 2019). We reported the effect estimates and CIs for individual studies and meta-analysis with the forest plots. The Chi2 (Q) test and I2 statistic were used to determine the percentage of variability attributable to included studies (Higgins, Thomas, et al., 2019). We set the P value less than 0.1 to determine statistical heterogeneity, due to small number of studies, or an I2 greater than 50% to quantify substantial heterogeneity (Deeks et al., 2019). We planned to conduct a sensitivity analysis to investigate differences noted when SMD of final scores versus change scores from baseline were used. We also planned to inspect the funnel plot to assess risk of publication bias if we included >10 studies and conduct the subgroup analysis based on age groups (65 to 80, and 80 years and older) and frailty status (prefrailty and frailty).
Two reviewers (E. E., M. C. A.) used the Grading Recommendations Assessment, Development and Evaluation (GRADE) rating to summarize the evidence for recommendations (Guyatt et al., 2011); we used GRADEpro GDT Version 3.6 (Evidence Prime, Inc).
Risk of Bias in this Review Process
To manage unconscious risk of bias of team members, we registered the protocol before starting the review, two authors independently (E. E., M. C. A.) screened at Levels 1 and 2, and assessed risk of bias, and none of the team members had publications included in this systematic review.
Results
Study Selection
We identified 2,798 citations based on our search of 7 databases and other sources. After removing duplicates (n = 258), we reviewed 2,540 citations at Level 1, and 114 publications at Level 2. Overall, 12 RCTs were included in this review (Figure 1).

PRISMA flow diagram for study selection into the systematic review: The titles and abstracts were screened at Level 1 and excluded if they did not meet the inclusion criteria, such as different patient populations, no telehealth interventions, or study designs other than an RCT. The full-texts were screened at Level 2 based on the same eligibility criteria.
Study and Participants Characteristics
All studies were in English, and most studies were conducted in the United States (n = 5) (Finkelstein et al., 2011; Gellis et al., 2014; Light et al., 2016; Peterson et al., 2007; Upatising et al., 2013). Studies included older adults with frailty (n = 8) (Dorresteijn et al., 2016; Favela et al., 2013; Finkelstein et al., 2011; Gellis et al., 2014; Laforest et al., 2012; Light et al., 2016; Markle-Reid et al., 2006; Tchalla et al., 2013), pre-frailty (n = 1) (Dekker-van Weering et al., 2017), or a mix of frail and not frail (n = 3) (Comín-Colet et al., 2016; Peterson et al., 2007; Upatising et al., 2013). These included 1,819 community dwelling older adults (65+ years), predominantly women, with frailty, including n = 123 participants considered “pre-frail” (Dekker-van Weering et al., 2017; Upatising et al., 2013). Mean age ranged from 69 to 86 years and older; please see supplementary Table 1. Different methods were used to define frailty, such as aged > 90 years needing caregiver or cut-offs on Barthel index < 90 (n = 1) (Comín-Colet et al., 2016), or Fried classification (Fried et al., 2001) (n = 2) (Peterson et al., 2007; Upatising et al., 2013). Three studies targeted older adults with pre-frailty or frailty with no formal definition for frailty (Finkelstein et al., 2011; Gellis et al., 2014; Markle-Reid et al., 2006); please see supplementary Table 2. Recruitment rate ranged from 1% (Gellis et al., 2014) to 52.5% (Comín-Colet et al., 2016) for all possible participants, and the retention rate for the intervention groups ranged from 68.6% (Dorresteijn et al., 2016) to 100% (Peterson et al., 2007), and between 62.5% (Laforest et al., 2012) to 100% (Dekker-van Weering et al., 2017; Peterson et al., 2007; Tchalla et al., 2013), for control groups. Please see supplementary Table 2.
Description of Interventions
The most common delivery method for health programs was telephone, (n = 8) (Dorresteijn et al., 2016; Favela et al., 2013; Gellis et al., 2014; Laforest et al., 2012; Light et al., 2016; Markle-Reid et al., 2006; Peterson et al., 2007; Tchalla et al., 2013). Interventions were primarily administered by health professionals, and the delivered content varied from falls prevention (n = 3) (Dekker-van Weering et al., 2017; Dorresteijn et al., 2016; Tchalla et al., 2013), increasing physical activity (n = 2) (Light et al., 2016; Peterson et al., 2007), to providing self-management skills for health promotion (n = 7), such as monitoring of health conditions (Comín-Colet et al., 2016; Upatising et al., 2013), social support (Laforest et al., 2012), resolving clinical emergency (Favela et al., 2013), or providing educational resources (Finkelstein et al., 2011; Gellis et al., 2014; Markle-Reid et al., 2006). The most frequently used control intervention was usual care (n = 8) (Comín-Colet et al., 2016; Dekker-van Weering et al., 2017; Dorresteijn et al., 2016; Finkelstein et al., 2011; Gellis et al., 2014; Markle-Reid et al., 2006; Peterson et al., 2007; Upatising et al., 2013). The length of the interventions varied from 3 (Dekker-van Weering et al., 2017; Gellis et al., 2014; Light et al., 2016) to 12 months (Tchalla et al., 2013; Upatising et al., 2013) (Supplementary Table 1).
Risk of Bias Within Studies
The greatest source of bias were blinding of participants and personnel (i.e., the performance bias), where 33% of studies were rated with a high risk of bias (Comín-Colet et al., 2016; Dorresteijn et al., 2016; Favela et al., 2013; Upatising et al., 2013), followed by outcome assessment (i.e., the detection bias), where 25% of the studies were rated with a high risk of bias (Dekker-van Weering et al., 2017; Favela et al., 2013; Upatising et al., 2013) (Figure 2).
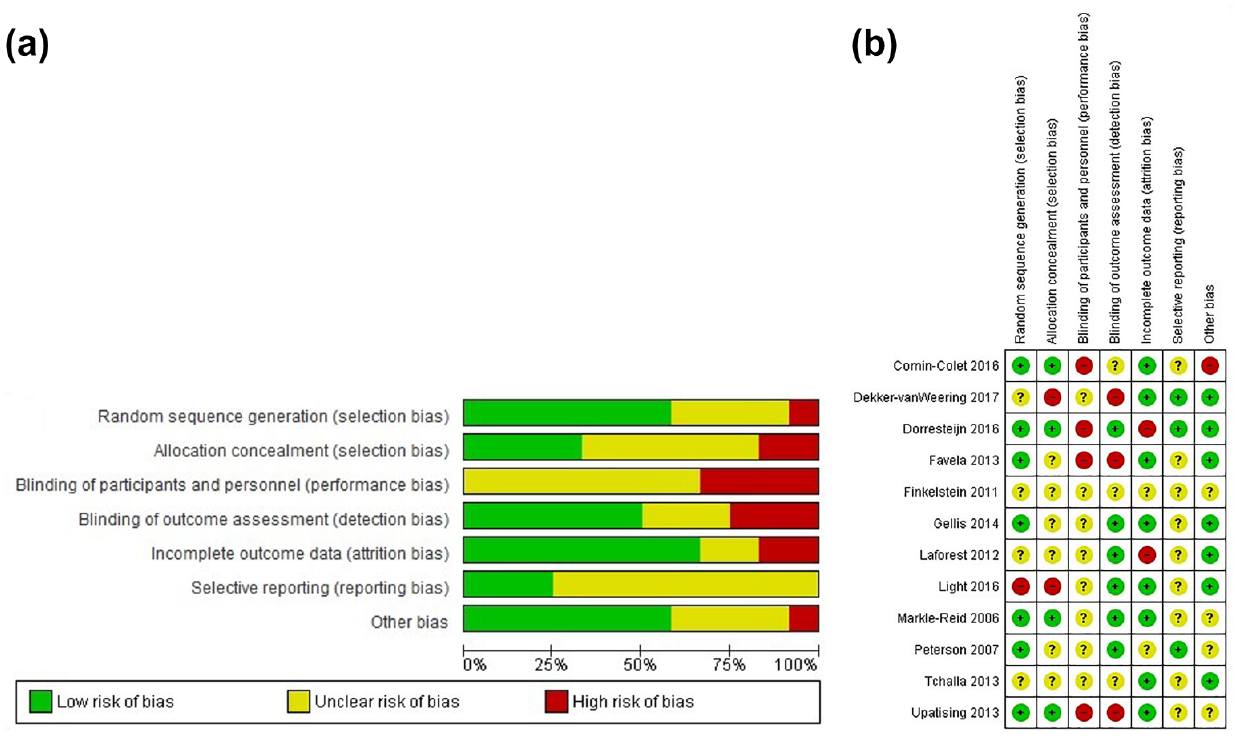
(a) Overall risk of bias. (b) Risk of bias for individual studies.
Synthesis of Results
No study reported measuring adverse events, and only one study reported no adverse events occurred during the trial (Tchalla et al., 2013). One study compared the difference between gender (women vs. men) (Tchalla et al., 2013), and found no significant association between gender and falls in univariate analysis (p = .128) (Tchalla et al., 2013). Improvement in function (Dorresteijn et al., 2016; Gellis et al., 2014; Laforest et al., 2012; Markle-Reid et al., 2006), balance (Light et al., 2016), mobility (Tchalla et al., 2013), physical activity (Dorresteijn et al., 2016), health-related quality of life (Comín-Colet et al., 2016; Dekker-van Weering et al., 2017; Markle-Reid et al., 2006), a decrease in falls incidence (Dorresteijn et al., 2016; Tchalla et al., 2013), or frailty status (Favela et al., 2013; Peterson et al., 2007), were identified in 10 studies. Outcomes of interest were not available for all studies, therefore we could only conduct the meta-analysis for function using four studies (Dekker-van Weering et al., 2017; Dorresteijn et al., 2016; Laforest et al., 2012; Markle-Reid et al., 2006), physical and mental components of quality of life including, two (Dekker-van Weering et al., 2017; Markle-Reid et al., 2006) and three studies (Dekker-van Weering et al., 2017; Gellis et al., 2014; Markle-Reid et al., 2006), respectively. We completed a narrative synthesis of findings for the seven remining studies. Below, we review and tabulate the results by outcome. A detailed summary is provided in supplementary Table 3. Due to the small number of studies it was not possible to conduct subgroup analyses based on age or frailty status.
Primary outcome
Function
Physical function and behavioral performance were reported in seven studies (Comín-Colet et al., 2016; Dekker-van Weering et al., 2017; Dorresteijn et al., 2016; Gellis et al., 2014; Laforest et al., 2012; Markle-Reid et al., 2006; Upatising et al., 2013). Three studies consistently reported telehealth interventions did not improve function (as measured by the European self-care behavior scale, Comín-Colet et al., 2016, or EQ-5D-3L, Dekker-van Weering et al., 2017), or functional decline with frailty and mortality states (Upatising et al., 2013). However, four studies reported telehealth interventions improved function compared with a control group as measured by the Western Ontario and McMaster Universities Osteoarthritis Index (Laforest et al., 2012), 18-item Groningen Activity Restriction Scale (Dorresteijn et al., 2016), Personal Resource Questionnaire 85 (Markle-Reid et al., 2006), or Social Problem-Solving Inventory-Revised (Gellis et al., 2014).
There was low certainty for a small positive change in favor of the telehealth intervention in function, Figure 3(a), 4 studies (Dekker-van Weering et al., 2017; Dorresteijn et al., 2016; Laforest et al., 2012; Markle-Reid et al., 2006), 647 participants: SMD = 0.31 [95% CI = 0.15, 0.47], p =.0001. Results showed little to no heterogeneity between studies (Chi2 = 2.19, p = .53, I2 = 0%). We performed sensitivity analysis on final scores of function; no effect of telehealth interventions compared with control was observed (635 participants: SMD = -0.04 95% CI = [-0.20, 0.12], p = .64). The GRADE summary of evidence is provided in Table 1.
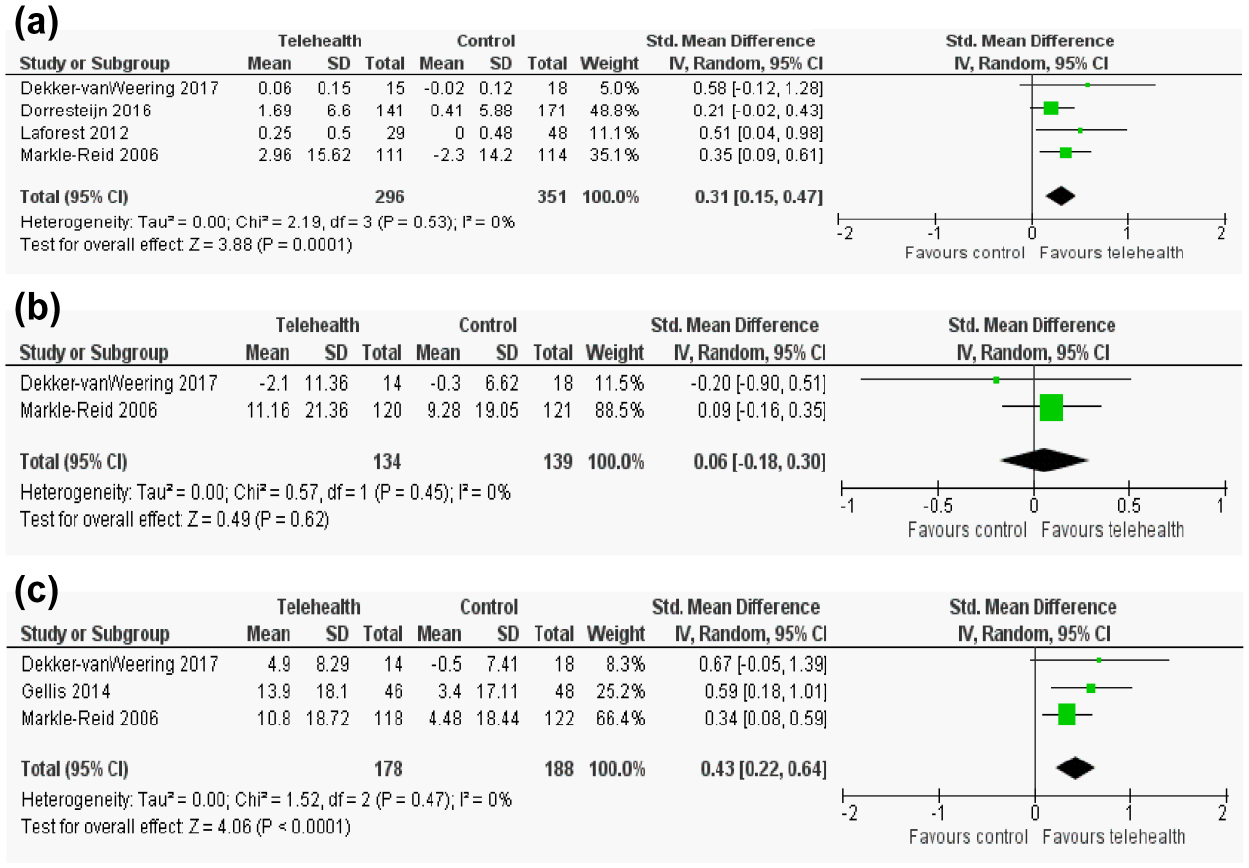
Forest plot of the effect of telehealth interventions on change scores of (a) function/behavioral performance, (b) physical and (c) mental components of health-related quality of life.
GRADE Evidence Profile of Studies Included in the Meta-Analyze.

Note. GRADE: High quality: very confident that the estimate of effect will not be changed by further research. Moderate quality: moderately confident that the estimate of effect close to the true effect and further research may change the estimate. Low quality: limited confident in the effect estimate and further research will likely change the estimate. Very low quality: very little confident in the effect estimate.
The weight and sample of studies were reasonable in quantitative analysis; we downgrade one level due to high risk of bias.
We downgrade one level due to variety of outcome measurement tools including patient reported tools and performance-based tools.
We downgrade one level due to small number of studies.
We downgrade one level due to small number of studies and wide confidence intervals.
Secondary outcomes
Quality of life
Four studies assessed the effect of telehealth interventions on quality of life measured with the Minnesota Living with Health Failure Questionnaire (Comín-Colet et al., 2016), SF-12 (Dekker-van Weering et al., 2017; Gellis et al., 2014), or SF-36 (Markle-Reid et al., 2006). All studies, except one (Gellis et al., 2014) reported enhanced quality of life. The one exception reported a 12-week depression care management program with daily telemonitoring of health conditions and 8-weeks of telephone calls did not improve quality of life for older adults with frailty (Gellis et al., 2014).
The effect of telehealth interventions compared with usual care was equivalent for the physical component of quality of life change score, Figure 3(b), two studies (Dekker-van Weering et al., 2017; Markle-Reid et al., 2006), 273 participants: SMD = 0.06, 95% CI = [-0.18, 0.30], p = .62, very low certainty. Results showed little to no heterogeneity between studies (Chi2 = 0.57, p=.45, I2=0%). Sensitivity analysis, involving final scores, did not change the results (SMD = 0.12 [95% CI = -0.12, 0.36], p = .33). The very low certainty of evidence including three studies (Dekker-van Weering et al., 2017; Gellis et al., 2014; Markle-Reid et al., 2006), highlighted telehealth interventions were better at improving the mental component of quality of life from baseline than usual care (Figure 3(c)), 366 participants: SMD = 0.43 (95% CI = [0.22, 0.64], p < .0001). There was little to no heterogeneity between studies (Chi2 = 1.52, p = .47, I2 = 0%). The sensitivity analysis (conducted by using final instead of change scores) showed no difference between telehealth interventions and usual care (366 participants: SMD = 0.21 95% CI = -0.14, 0.57], p = .24) with substantial heterogeneity among studies (Chi2 = 4.31, p = .12, I2 = 54%). GRADE ratings are provided in Table 1.
Balance
Light et al. (2016) tested the effect of telehealth intervention on balance, (measured with the Berg Balance Test) for older adults with frailty, and reported 12 weeks of telephone (calls to support a home exercise program) increased balance in older adults with frailty.
Falls
Two studies reported the effect of telehealth interventions on reducing fall incidence for older adults with frailty (Dorresteijn et al., 2016; Tchalla et al., 2013). Tchalla et al. (2013) tested the effect of using a nightlight path with telephone calls for assistance to reduce fall rates compared with an in-person fall reduction program. Dorresteijn et al. (2016) explored the effect of a balance exercise DVD, with three home visits and four telephone calls, to address fall incidence reported as number of falls compared with usual care. Though inconclusive, both studies noted telehealth interventions decreased falls occurrence.
Mobility
Tchalla et al. (2013) reported a 54-week study using a nightlight path with telephone calls for assistance, increased walking performance, measured by the Timed-Up and Go test, in older adults with frailty.
Physical activity
Two studies assessed the effect of telehealth intervention on physical activity for older adults with frailty (Dorresteijn et al., 2016; Tchalla et al., 2013). Tchalla et al. (2013) reported physical activity, measured with the Lawton Activities of Daily Living (ADL), did not increase with a telephone call intervention. However, Dorresteijn et al. (2016) reported a home-based balance exercise program, with three nursing home visits and four telephone calls, increased ADLs measured with the Groningen Activity Restriction Scale, after 12 months.
Frailty status
Three studies explored the effect of telehealth interventions on frailty status (Favela et al., 2013; Peterson et al., 2007; Upatising et al., 2013), measured with the Fried theoretical framework (Fried et al., 2001). Favela et al. (2013) noted a 36-week nurse home visit program, along with an alert button and telephone calls decreased frailty progression. Likewise, Peterson et al. (2007) observed a 24-week physical activity counseling group, with follow-up telephone calls, decreased frailty progression in older adults with frailty. Conversely, Upatising et al. (2013) found that 54-weeks of telemonitoring of health conditions resulted in lower frailty status, in older adults with pre-frailty and frailty.
Adherence
Only one study reported adherence. Dekker-van Weering et al. (2017) reported 68% adherence to a 12-week web-based self-management exercise program, measured with completion of the training session by watching exercise videos, for older adults with pre-frailty.
Satisfaction
There were only two studies that explored older adults’ satisfaction with telehealth interventions: (a) a 36-week web-based educational resource with videoconferencing and monitoring, and measured with a 6-item satisfaction questionnaire (Finkelstein et al., 2011), and (b) a 20-week telephone call for monitoring and depression management, as measured with the Home Care Client Satisfaction Instrument (Gellis et al., 2014). Neither study reported significant differences in satisfaction between telehealth intervention and usual care.
Discussion
Summary of Evidence
The aim of this review was to evaluate the effectiveness of telehealth interventions versus control interventions in improving physical function, quality of life, and frailty status among older adults with pre-frailty or frailty. Using technology to support health care in people with pre-frailty and frailty was effective for improving physical function and behavioral performance (four studies [Dekker-van Weering et al., 2017; Dorresteijn et al., 2016; Laforest et al., 2012; Markle-Reid et al., 2006); 647 participants], and the mental component of quality of life (three studies, Dekker-van Weering et al., 2017; Gellis et al., 2014; Markle-Reid et al., 2006); 366 participants] compared with baseline. However, the quality of evidence was very low to low. Our sensitivity analyses identified no effect of telehealth interventions compared with control on final scores. Further research in this area is likely to change the certainty of evidence on the effect estimate. While encouraging, these results must be viewed cautiously, as there is limited evidence overall, and three studies did not report any formal definition for frailty which could affect the overall findings of this review. Furthermore, the generalizability of findings is limited to community-dwelling older women, and insufficient data and heterogeneity of outcome measures and interventions precluded making definitive recommendations.
Laver et al. (2020) in a Cochrane systematic review of telerehabilitation for people after stroke reported no difference in ADLs, balance, and health-related quality of life. However, they suggested telehealth is a reasonable way of service delivery for people with limited access to resources and can improve rehabilitation services for people living in remote areas. Important findings emerging from our review, despite the very low to low certainty of evidence, suggest telehealth intervention is a practical model of health care delivery for older adults with pre-frailty or frailty and has potentially useful clinical applications.
Cost is a potential issue for providing telehealth services (Henderson et al., 2013). However, the COVID-19 pandemic highlighted a clear need for care delivered remotely (e.g., telehealth) (Makhni et al., 2020). There is insufficient evidence to determine the cost-effectiveness of telehealth services for older adults with frailty. Although the cost analysis of videoconferencing fracture clinics showed the savings for health services by limiting the unnecessary hospital transfers (McGill & North, 2012), the implementation and maintenance of telehealth care programs need considerable investment (Makhni et al., 2020). Moreover, the health professionals, patients, and insurance companies need to be aligned and trained to solve the challenges of implementation (Makhni et al., 2020). We recommend future studies determine effective telehealth implementation strategies, and cost-effectiveness of telehealth interventions.
Our review highlighted a high rate of retention for study participants, which is critical to inform practice. Although from our review little can be discerned on the factors, such as the intensity and frequency of program which are attributable to program adherence and study retention; A Cochrane review by McCabe et al. (2020) on telehealth for adults with chronic obstructive pulmonary disease concluded remote delivery improved health-related quality of life and activity, but it is important to sustain engagement with technology over time. As telehealth advances, it is important to focus on implementation factors related to program delivery, adoption, and sustainability.
Limitations
Despite our comprehensive methodology, we may have missed studies including older adults who were frail but did not report a frailty definition, or identify the population as frail (Mohlman & Basch, 2020). Furthermore, we excluded studies using telehealth nutritional interventions for frailty (Neelemaat et al., 2011). As there was heterogeneity in the instruments or outcomes chosen to define frailty, the observed findings cannot be generalized to all older adults with frailty. Moreover, studies did not report collecting and adjudicating adverse events, therefore we cannot comment on harms associated with telehealth interventions. Due to the limited number of studies, with high variability between outcomes, we were not able to include all studies in a quantitative synthesis. Finally, standard deviations for change scores were missing in the majority of included studies; however, it is acceptable to impute this variable (Furukawa et al., 2006).
Conclusion and Implications
We highlight a knowledge and health care gap for telehealth interventions for older adults with frailty. More accessible health care interventions may improve function and the mental component of quality of life compared with baseline. However, evidence is still insufficient to advise health care professionals. This review highlights that telehealth technologies can potentially benefit people with frailty. Moreover, it seems reasonable to suggest that telehealth programs can assist in providing care (remotely) for older adults with functional limitations.
Supplemental Material
sj-pdf-1-jag-10.1177_0733464820983630 – Supplemental material for The Effect of Telehealth Interventions on Function and Quality of Life for Older Adults with Pre-Frailty or Frailty: A Systematic Review and Meta-Analysis
Supplemental material, sj-pdf-1-jag-10.1177_0733464820983630 for The Effect of Telehealth Interventions on Function and Quality of Life for Older Adults with Pre-Frailty or Frailty: A Systematic Review and Meta-Analysis by Elham Esfandiari, William C. Miller and Maureen C. Ashe in Journal of Applied Gerontology
Supplemental Material
sj-pdf-2-jag-10.1177_0733464820983630 – Supplemental material for The Effect of Telehealth Interventions on Function and Quality of Life for Older Adults with Pre-Frailty or Frailty: A Systematic Review and Meta-Analysis
Supplemental material, sj-pdf-2-jag-10.1177_0733464820983630 for The Effect of Telehealth Interventions on Function and Quality of Life for Older Adults with Pre-Frailty or Frailty: A Systematic Review and Meta-Analysis by Elham Esfandiari, William C. Miller and Maureen C. Ashe in Journal of Applied Gerontology
Supplemental Material
sj-pdf-3-jag-10.1177_0733464820983630 – Supplemental material for The Effect of Telehealth Interventions on Function and Quality of Life for Older Adults with Pre-Frailty or Frailty: A Systematic Review and Meta-Analysis
Supplemental material, sj-pdf-3-jag-10.1177_0733464820983630 for The Effect of Telehealth Interventions on Function and Quality of Life for Older Adults with Pre-Frailty or Frailty: A Systematic Review and Meta-Analysis by Elham Esfandiari, William C. Miller and Maureen C. Ashe in Journal of Applied Gerontology
Supplemental Material
sj-pdf-4-jag-10.1177_0733464820983630 – Supplemental material for The Effect of Telehealth Interventions on Function and Quality of Life for Older Adults with Pre-Frailty or Frailty: A Systematic Review and Meta-Analysis
Supplemental material, sj-pdf-4-jag-10.1177_0733464820983630 for The Effect of Telehealth Interventions on Function and Quality of Life for Older Adults with Pre-Frailty or Frailty: A Systematic Review and Meta-Analysis by Elham Esfandiari, William C. Miller and Maureen C. Ashe in Journal of Applied Gerontology
Supplemental Material
sj-pdf-5-jag-10.1177_0733464820983630 – Supplemental material for The Effect of Telehealth Interventions on Function and Quality of Life for Older Adults with Pre-Frailty or Frailty: A Systematic Review and Meta-Analysis
Supplemental material, sj-pdf-5-jag-10.1177_0733464820983630 for The Effect of Telehealth Interventions on Function and Quality of Life for Older Adults with Pre-Frailty or Frailty: A Systematic Review and Meta-Analysis by Elham Esfandiari, William C. Miller and Maureen C. Ashe in Journal of Applied Gerontology
Footnotes
Acknowledgements
We acknowledge doctoral support for Elham Esfandiari from AGE-WELL: Canada’s Technology and Aging Network. Associate Professor Ashe gratefully acknowledges the support of the Canada Research Chairs program. The protocol of this review is registered on PROSPERO [CRD42018100504].
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.