
Abstract
Current literature on aging in place highlights the socioemotional components that act as barriers to remaining in the home, but it often neglects actionable safety features of the home which may also pose a threat. Furthermore, this literature often neglects self-reported barriers to aging in place. Utilizing grounded theory, a retrospective review of home safety assessments completed in Philadelphia analyzed older adult reports to determine what factors older adults view as barriers to their aging in place plans. Overarching categories that were discovered through the data analysis process included barriers related to home mobility and safety, personal health, access to community services, home improvement and maintenance needs, general safety concerns, and bathroom safety. Results indicate that older adults can identify many barriers to aging within their home, but that accessing support and services to overcome these barriers requires additional resources and funding.
Keywords
The number of Americans above the age of 65 years will increase to approximately 72 million or 20% of the U.S. population by 2030 (Bonder & Bello-Haas, 2018). Overall, 87% of adults aged 65 years and older want to stay in their current home and community as they age (American Association of Retired People [AARP], 2014). However, many challenges threaten their ability to do so successfully, including changes in functional status as well as the affordability, accessibility, overall safety of their homes, and difficulty with repairs and maintenance of the residence (Fausset et al., 2011; U.S. Department of Housing and Urban Development, 2017).
It is important to recognize that aging in place entails more than residing in the physical space of one’s home. The Center for Disease Control (2009) defines aging in place as “the ability to live in one’s own home and community safely, independently, and comfortably, regardless of age, income, or ability level.” Research by Martin et al. (2019) found that although more than 70% of respondents aged 65 years and older would like to stay in their homes as they age, many did not think their current living arrangements would satisfy their needs in the future.
There are many benefits for older adults to remain within the home environment. Community-dwelling older adults have increased autonomy, control, well-being, and individuality (Martin et al., 2019; Stones & Gullifer, 2016). Their previously established relationships and roles within their communities and neighborhoods, including those of volunteer, work, and social nature, can further foster a greater sense of well-being (Choi et al., 2019; Wiles et al., 2012). The ability to age in place has proven benefits of decreased cost for health care (U.S. Department of Housing and Urban Development, 2020). In addition, aging in place can mitigate other health burdens on individuals such as increased rates of infection and antibiotic resistance noted within facility environments (Montoya & Mody, 2012).
Although the benefits of aging in place are many, they do not eliminate the barriers older adults must overcome to remain in their homes, and current literature lacks information on the true extent of those barriers. Data on the nature of older adult-reported barriers are limited, and much of the literature references the socioemotional aspects of aging such as autonomy, independence, and social connection, rather than actionable home safety, accessibility, or modification needs (Stones & Gullifer, 2016; Wiles et al., 2012). In addition, literature on specific barriers within the home or the safety needs of older adults has almost exclusively been written from the professional’s viewpoint; this fails to account for the lived experience of older adults and may decrease the relevance of recommended home modifications (Blanchet & Edwards, 2018; Grimmer et al., 2015). This project seeks to narrow this literature gap and explore perceived barriers reported by older adults who are aging in place.
Method
This is a retrospective review of qualitative data. Data were analyzed using a grounded theory approach to identify themes related to older adults’ self-reported barriers to aging in place. Data were gathered by retrospectively reviewing reports from older adult home safety assessments. A total of 36 older adults’ reports were analyzed. The assessments were completed gratis through a community-based nonprofit organization serving older adults more than the age of 55 years living in the Mt. Airy, Chestnut Hill, Germantown, and Northwest Philadelphia neighborhoods. The nonprofit organization offers low-cost services including classes, home repairs, transportation, and home care, to its members. Registration is free and entails supplying basic demographic information. The home safety assessments were offered as a complimentary service to current or future members. Older adults were recruited for the assessments via email newsletters from the organization, community flyers, and through classes and programming offered by the nonprofit. Assessments were scheduled by the older adult via phone or email. Following the assessment, some older adults qualified for a grant-funded stipend for low-cost services provided by the nonprofit and/or to cover the cost of desired home equipment. Eligibility for this stipend was determined by the nonprofit, and the interviewers were not involved in any decision-making or distribution of funds.
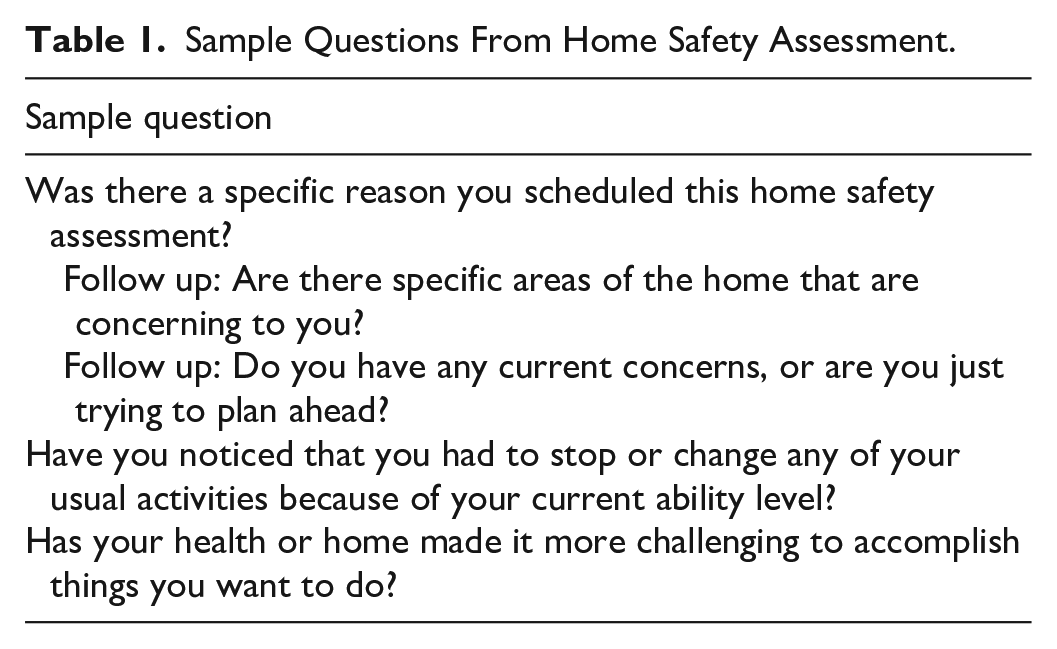
All home safety assessments took place in the older adults’ homes and consisted of a semi-structured interview followed by an older adult-guided tour through the home. The semi-structured interview incorporated a standard list of topics discussed with each older adult including medical history, functional status, and features of the home. See Table 1 for sample interview questions. See Table 2 for a list of topics discussed with each older adult. During the older adult-guided tour, homes were assessed for safety concerns related to falls risk, lighting, fire safety, electrical safety, structural safety, daily activity needs, and functional use of the home. Older adults were given the opportunity to report barriers in any and all topics on the checklist as well as any additional topics they wished to discuss.
Sample Questions From Home Safety Assessment.
Topics Reviewed With Older Adults Receiving Home Assessments.
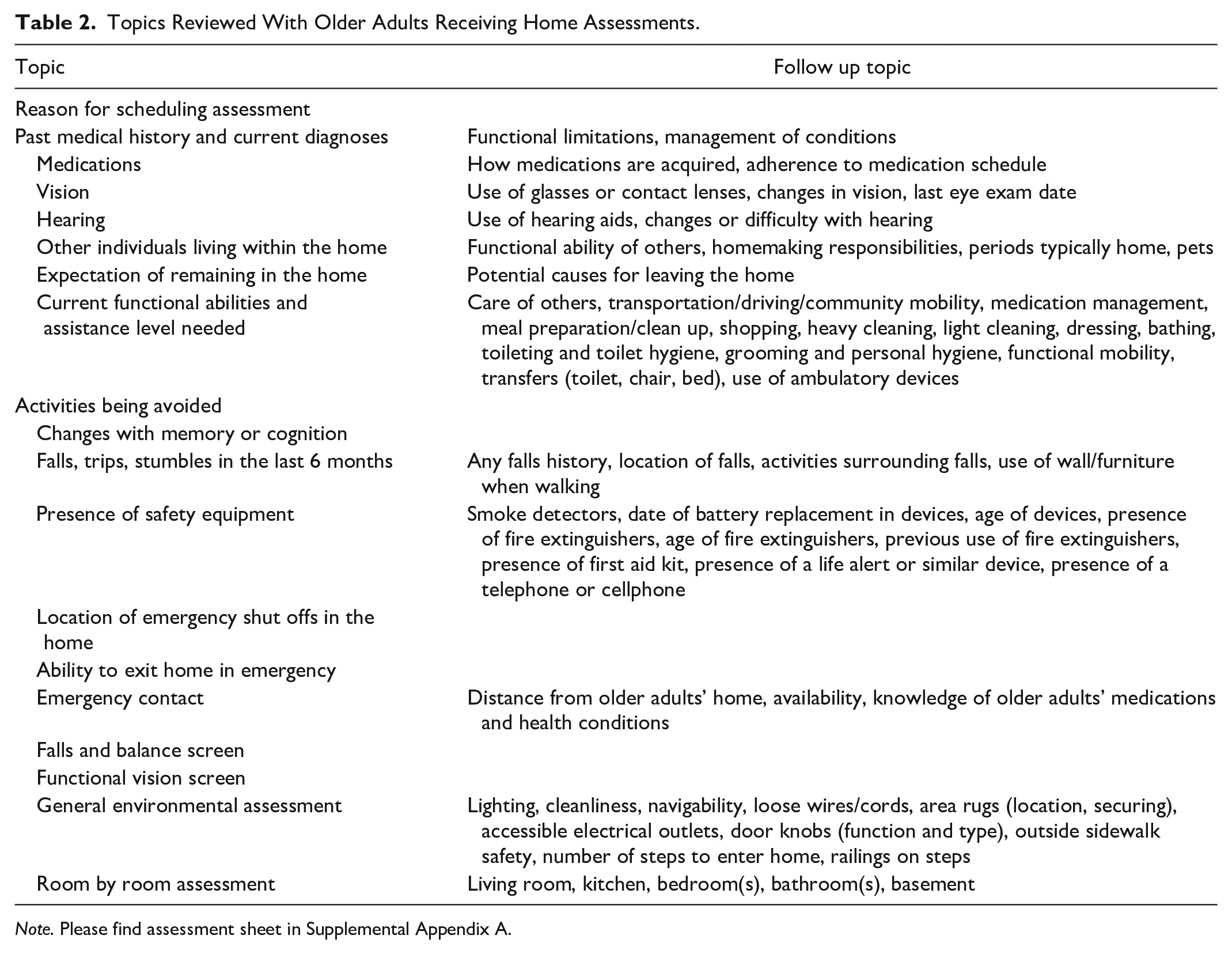
Note. Please find assessment sheet in Supplemental Appendix A.
Data Collection
Interviewers took handwritten notes during each assessment using the form found in Supplemental Appendix A, which were then formatted into individual reports describing current and potential barriers that the older adult reported, as well as barriers that the interviewers observed. Information from each home assessment was used to generate a unique report for the older adult, which included both older adult-identified and interviewer-identified barriers in separate sections of the reports. However, only barriers identified by the older adult were subsequently used for data analysis.
There were three interviewers present for each home safety assessment. The interviewers included one licensed occupational therapist with additional training as a Certified Living in Place Professional (CLIPP; Living in Place Institute, n.d.) and two occupational therapy student practitioners in their final fieldwork rotations. All three interviewers were trained in completing an occupational profile and motivational interviewing and utilized principles set forth in the Occupational Therapy Practice Framework (American Occupational Therapy Association [AOTA], 2014; Resnicow & McMaster, 2012) to fully assess the interaction between older adults and their home environments. A checklist of items was reviewed with every older adult to ensure consistency among the semi-structured interviews. The full checklist can be found in Supplemental Appendix A. Consistency in student training, home assessment, and interview format throughout all 4 years of the home safety assessment program allowed for retrospective analysis of data.
Data Analysis
A grounded theory approach involving constant comparison with existing data from the last 4 years was utilized (Tie et al., 2019). The data coded for analysis were limited to barriers expressed by the older adults and did not include barriers that were identified solely by the interviewers or items noted by older adults that were not seen as problematic. Initial coding included individual line-by-line open coding by two coders, which was then compared to determine consensus. For each report, a barrier was counted only once even if it was mentioned multiple times within the report. For example, if a report showed that an older adult had separate concerns with their first floor stairs and basement stairs, stair safety was only counted once. Discrepancies between the two coders were resolved by a third coder to improve trustworthiness. Initial coding demonstrated an 87% agreement between the two coders. Focused coding was then utilized to consolidate specific codes under a broader theme that best explained the individual codes; for example, original themes coded as “secure rugs” and “clear walkways” were later grouped under the broader theme “falls hazards.” Consensus was established among all three coders to ensure credibility in final themes. Established themes were continuously compared with the most recent data through an iterative process and evolved to incorporate codes from both recent and existing data consistent with methods described by Tie et al. (2019). Themes were then grouped into larger overarching categories. Categories and themes evolved over the course of 2 years through the acquisition of new data and refinement of codes, themes, and categories.
Results
A total of 36 home safety assessment reports were reviewed. Categories that were discovered through the data analysis process included barriers related to home mobility and safety, personal health, access to community services, home improvement and maintenance needs, general safety concerns, and bathroom safety. See Table 3 for a comprehensive list of categories, themes, and counts. The total number of reported barriers to aging in place between the 36 older adults was 143. The number of reported barriers to aging in place ranged from two to nine barriers per home. The average number of barriers reported by each older adult was approximately four.
Summary of Older Adults’ Self-Reported Barriers.
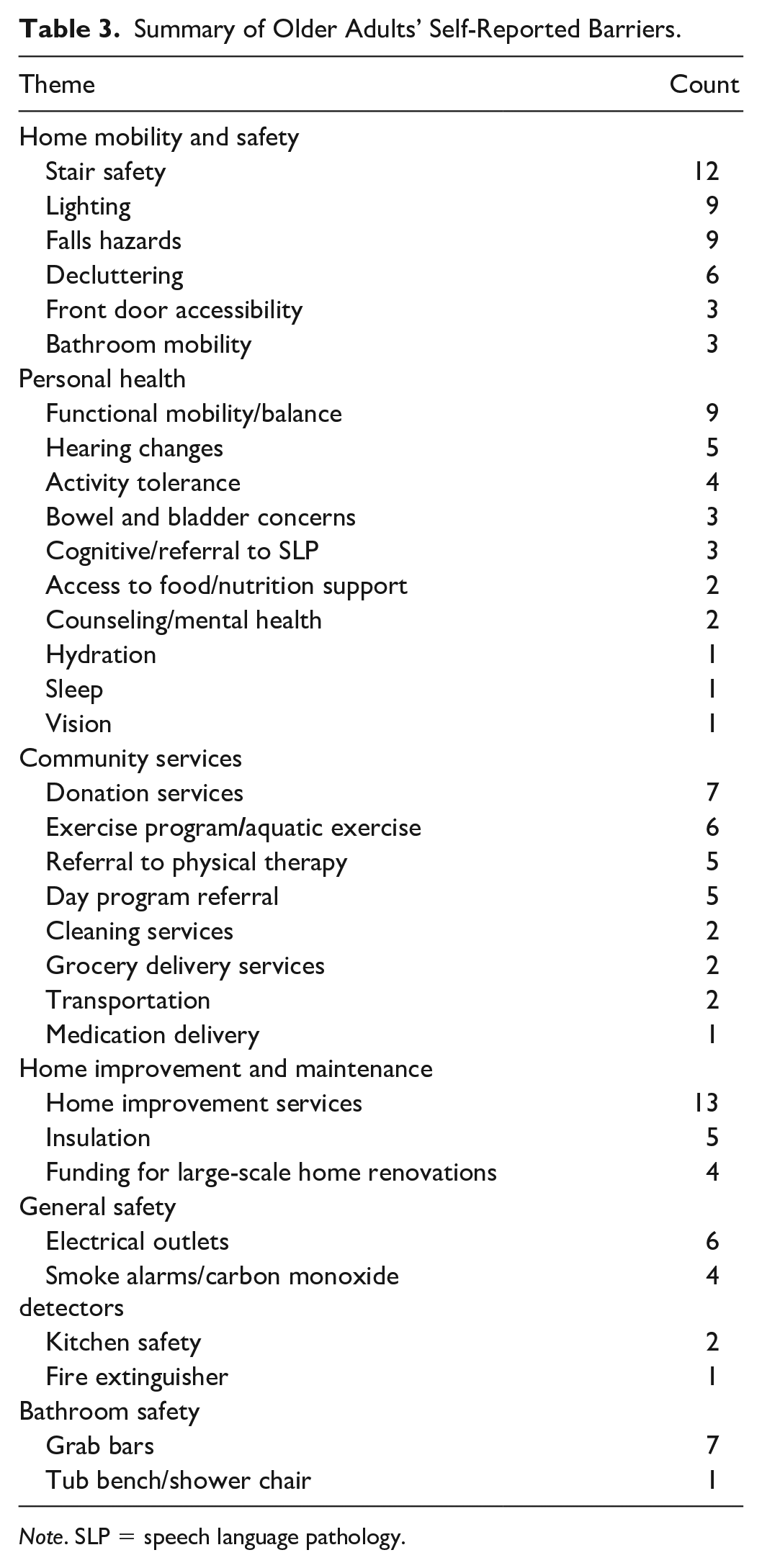
Note. SLP = speech language pathology.
Home Mobility and Safety
The home mobility and safety category included characteristics of the physical environment that older adults recognized as current or potential hazards to moving safely in the home, solely based on the attributes of the space or structure. The themes in this category were stair safety, lighting, general falls hazards not otherwise captured, decluttering, front door accessibility, and bathroom mobility. Stair safety included stairs and railings that were damaged or broken, and general disrepair of the stairwells. General falls hazards included items such as loose area rugs and obstacles in walkways that could pose a risk of falling. Bathroom mobility referred to the features of the existing physical bathroom space that did or could pose a mobility hazard.
The home mobility and safety category was the most commonly reported barrier among older adults. All older adults identified at least one factor in the home mobility and safety category as a current or potential barrier to aging in place. The theme of stair safety was the most commonly reported barrier in this category, with 12 older adults reporting this barrier. Many older adults who reported stair safety as a barrier expressed concerns regarding their basement stairs and a lack of sturdy railings on basement stairs. For example, an older adult who reported falling down her railing-less basement stairs stated that she now travels to a Laundromat to do laundry rather than going down to the basement. Within this category, nine older adults reported lighting, and nine older adults reported falls hazards as barriers to aging in place.
In addition, older adults frequently reported items as falls hazards, either by reporting obstacles they had previously tripped over or an object that may lead to a fall, highlighting an overall awareness of falls risk. Reported falls hazards included loose and damaged flooring and elevated thresholds, which were generally permanent or structural fixtures within the home. Lighting was another common barrier reported by older adults, who often cited dark areas of the home which limited functional use and reported decreased brightness after replacing older incandescent light bulbs with newer compact fluorescent (CFL) or LED bulbs.
The theme of decluttering referenced item accumulation, often referred to as “clutter” or “junk” by older adults, and was reported by six older adults as a concern and possible obstacle. Many older adults reported having unneeded items that they wanted to remove and that interfered with functional use of the home. Of greatest concern were items remaining from individuals who no longer lived in the home such as grown children or deceased spouses. Older adults reported that they were uncertain about how to remove items, especially those of suspected value, or that they felt some level of stress in initiating the decluttering process. Older adults cited the weight, number, location, and anticipated cost to remove items as barriers.
Personal Health
Personal health was defined as any health-related attribute that the older adult felt posed a risk to their ability to remain in the home or that has caused them to require medical care. Themes included functional mobility/balance, hearing changes, activity tolerance, bowel and bladder concerns, cognitive changes or referrals for appropriate cognitive services (speech language pathology), access to food and nutrition, counseling and mental health needs, hydration, sleep, and vision. Within the functional mobility and balance theme, reports of previous falls, stumbles, or trips were included if the older adult deemed them as problematic. These also included reports of decreased balance or unsteadiness and concerns related to physically getting to the bathroom at night. Access to food and nutrition referred to the financial ability to afford food and prepare food. Activity tolerance included difficulties with activities such as walking, climbing steps, and completing kitchen or cleaning tasks.
The most frequently reported personal health barrier reported by nine older adults was functional mobility and balance difficulties, with some resulting in falls, “trips,” or “stumbles.” For example, one older adult reported occasional dizziness and not feeling as stable as she used to be, whereas another reported that her leg sometimes “gives out” and she “stumbles.” In addition, many of these older adults reported previous falls, fall-related injuries, and changes to their daily activities and routines in an attempt to reduce the likelihood of future falls.
Changes in hearing or hearing loss were reported as barriers by five older adults. Activity tolerance, defined as the ability of the older adult to change or maintain body position during an activity (AOTA, 2014), was reported by four older adults as a limiting personal health barrier that interfered with daily activities such as cleaning, walking up and down stairs, and yard work. For example, several older adults reported having difficulty carrying heavy groceries. The underlying cause for decreased activity tolerance varied by older adult, with most due to self-reported musculoskeletal or cardiopulmonary conditions. Within this category, three older adults reported bowel and bladder symptoms, including urgency, frequency, incontinence, and nocturia that they felt pose a risk to aging in place now or in the future, and all thought these changes were permanent.
Access to Community Services
The access to community services category included specific services that older adults reported they currently need or anticipate needing, and without access to these services would potentially impact their ability to age in place. The themes in this category were donation services for unneeded items, exercise programs (including aquatic exercise), referral to physical therapy, adult day programs, cleaning services, grocery delivery services, transportation, and medication delivery services. Donation services were the most commonly reported barrier with seven older adults reporting a need. Older adults who reported clutter as a barrier often requested referrals for donation services for those items. Older adults were especially interested in services that would come into the home to pick up donations due to the size, number, and weight of items. Six older adults reported a lack of access to exercise programs and/or aquatic exercise as a barrier. Five older adults reported the need for physical therapy, and five reported the need for future day program services.
Home Improvement and Maintenance
The home improvement and maintenance category referenced current or anticipated repair services that would limit the older adult’s ability to remain in the home if they were not completed. The themes in this category were general home improvement services needed for routine maintenance, lack of insulation in the home, and funding for large-scale renovations or repairs. This category excluded damage or repairs that the older adult identified as a falls risk.
The need for general home improvement and maintenance services was reported by 13 older adults. Five older adults reported the need for better or new insulation in the home, and four reported lack of funding for large-scale home renovations as a barrier. Older adults expressed concern about cosmetic and structural damage, with roof and ceiling leaks and subsequent damage being the most common. One older adult reported needing a new roof and required “cosmetic attention” due to damage from roof leaks. Often noted in relation to needed home improvement and repair services were reports of decreased access to affordable repairs and concerns related to hiring trustworthy individuals to perform repairs.
General Home Safety
General home safety included features of the home which promote safety or that could pose a hazard to the home. Themes in this category included electrical outlet safety including the use of two-prong to three-prong adapters (cheater plugs), extension cords, proper use of surge protectors, the need for smoke alarms and carbon monoxide detectors, kitchen safety concerns, and fire extinguishers. The kitchen safety theme included reports of problematic or malfunctioning kitchen equipment or kitchen setup that posed a fire hazard. The electrical outlet theme was reported most frequently by six older adults. Some identified hazards such as overloaded outlets due to a lack of outlets in older homes, or a lack of three pronged outlets. Older adults reported use of multiple extension cords and surge protectors to compensate for these issues.
Bathroom Safety
The bathroom safety category was defined by the stated need for a safety device in the bathroom, to safely age in place. This included the themes of grab bars and tub bench/shower chair. Seven older adults reported the need for grab bars, and one reported the need for a tub bench or shower chair. Older adults expressed the need for grab bars both inside and around the bathtub and/or shower stall, and near the toilet.
Discussion
This project aimed to identify factors that older adults perceived as current or potential barriers to aging in place using grounded theory. Data review from home safety assessments of 36 community-dwelling residents of Northwest Philadelphia suggested that older adults are aware of how their own abilities and health, the functionality of their home, community resources, and their preferred activities and habits can all impact their ability to age in place. However, older adults may be unable to access the resources required to address these barriers.
The breadth of topics discussed and reviewed with each older adult, the use of motivational interviewing, and the use of the Occupational Therapy Practice Framework (AOTA, 2014), during the assessment of older adult and environmental interaction, proved invaluable in identifying older adult-reported barriers and may have encouraged open discussion and discourse. In addition, older adults may have been more open to reporting barriers due to the nonpunitive and supportive nature of the home assessment program, which offered a free follow-up visit to highlight available services and solutions to the problems noted by the older adults and interviewers. Further research utilizing these and other methods should be conducted to determine best practices in assessing older adults’ perspectives on barriers to aging in place.
Many older adults reported previous events that were themed as a fall or balance concern. However, the word “fall” was often avoided or denied in favor of other terms such as “stumble,” “trip,” or “become unsteady,” even during instances when the person made contact with the floor or would have made contact if a piece of furniture had not stopped the person from touching the floor. Older adults also identified falls hazards in the home using similar terminology, citing that they “may trip” or “lose balance” due to an object or feature in the home. Research has shown that older adults are hesitant to report falls and often have a different understanding of what constitutes a fall from professionals (Dollard et al., 2014; Freiberger & de Vreede, 2011). Furthermore, research has shown that the word “fall” may be associated with weakness and frailty and not elicit an accurate response from older adults (Hoffman et al., 2018). Older adults who participated in this program frequently reported falls, near falls, trips, stumbles, and falls hazards. This may be due to the phrasing of questions related to falls, the supportive nature of the home safety assessments, and the potential for follow-up supports offered by this program. Despite the interviewers and coders understanding a fall as any event that leads to falling all the way down to the floor or falling and hitting an object such as a chair or stair (Nevitt et al., 1991), interviewers matched the older adult’s chosen language during interviews and avoided using the word “fall” unless it was first used by the older adult. This suggests the importance of utilizing older adults’ chosen language in assessing actual or potential falls and highlights the need for professionals to match their clients’ preferred terminology.
Concerns related to lighting were commonly reported by older adults who reported a general lack of lighting in functional spaces such as the living room, bathroom, stairways, and hallways. This is not surprising due to the fact that older adults receive less light to the retina and, as a result, perceive spaces as darker (Bonder & Bello-Haas, 2018). However, this concern was followed by reports of “new” light bulbs being dimmer than “old” light bulbs. The phasing-out of incandescent “old” light bulbs in favor of newer, more energy efficient, and safer types of light bulbs including LED and CFL (H.R. 6, 110th Congress, 2007) is positive; however, the change in labeling seems to be problematic and may lead to the purchase of suboptimal lighting. Incandescent light bulbs utilize wattage and color as the main labeling components. However, LED and CFL bulbs, often referred as “replacement bulbs,” use additional labeling factors including lumen (brightness) and lifespan (U.S. Department of Energy, 2020). The brightness of a traditional 60-watt incandescent light bulb is usually 800 lumens, but an LED light bulb labeled as a 60-watt replacement bulb may have a lower lumen count, making the bulb appear less bright. These same LED light bulbs may actually only utilize 8 to 10 watts of energy; therefore, a lamp rated for a 60-watt bulb could safely sustain an LED bulb labeled as a 75-watt replacement bulb and receive 1,100 lumens, which is notably brighter and only utilizes 15 watts of energy (U.S. Department of Energy, 2020). Because older adults need up to three times the level of light that younger people do to see clearly, educating older adults on how to safely purchase higher lumen light bulbs and utilize new labeling standards to their benefit may improve the functionality of their spaces (Bonder & Bello-Hass, 2018).
Many older adults reported concerns related to clutter and how to remove items from the home. Clutter outside of a clinical manifestation or hoarding diagnosis has been shown to lead to individuals feeling overwhelmed and correlated with lower quality of life (Ferrari et al., 2017). The frequency of these reports suggests the need for more practical and local resources for decluttering, including providing in-home removal of objects for older adults. Decluttering programs and interventions may be a simple and cost-effective way to help older adults age in place and improve overall quality of life (Canadian Association of Occupational Therapists, 2017).
This review of data suggests that older adults are aware of their need for home repairs but commonly lack funds to complete routine maintenance and repairs, let alone fund projects specific to their aging in place needs. As 80% of aging-related home modifications are paid for out of pocket, this supports the necessity of community and state programming that funds maintenance and repairs for older adults’ homes (Lipman et al., 2012). In Pennsylvania, many such programs exist to support home improvement services for low-income homeowners; however, programs have stringent eligibility requirements and lengthy waitlists that decrease accessibility of the funds (Philadelphia Housing Development Corporation, 2020). These challenges often disproportionately affect older women and women of color. One study found that older African American women are more likely to live in older homes while also allotting at least 30% of their monthly income toward mortgage payments (Johnson & Lian, 2018). Furthermore, the older homes that these older adults inhabit may be increasing their health and safety risks, as the homes may still have lead-based paint and radon (Heller, 2016). Funding needs to include needs-specific modifications for these vulnerable older adults; otherwise, hospitalization and rehabilitation costs for fall-related injuries will continue to rise (Johnson & Lian, 2018).
Three older adults reported bowel and bladder concerns as a barrier to aging in place, with a wide range of symptoms, all of which could be treated with pelvic floor therapy (Academy of Pelvic Health Physical Therapy, 2019). Although this number is overall low for the sample size, the range of symptoms and disruption to functional abilities coupled with older adult attitudes of normality and resignation to bowel and bladder issues is worrisome. Research has shown that incontinence is a leading factor in falls and institutionalization in older adult populations, and it is treatable (Academy of Pelvic Health Physical Therapy, 2019; Foley et al., 2012; Matsumoto & Inoue, 2007). This punctuates the need to improve older adult education and screening surrounding bowel and bladder changes and symptoms to support aging in place and falls prevention.
Overall, these findings support the work of Bercaw (2020), which asserts that older adults’ personal perceptions of need are a key barrier to receiving services, but it also highlights the need for additional older adult education and advertisement of services that exist within the community to allow for better access to services and older adult empowerment. Information about older adults’ perceived barriers should influence programs to address these problems through a person-centered approach and support the independence of community-dwelling older adults.
Limitations
There are limitations in this analysis due to retrospective review of data. This project is part of a public service program and was not designed to be a research study. The reports lacked demographic data including age, gender, race, ethnicity, and socioeconomic status due to the fact that the reports analyzed were intended for the older adults themselves. This decreased generalizability of this study to any one population. The interviews were also not recorded, so it was not possible to analyze the older adults’ statements verbatim. However, the use of three interviewers increased trustworthiness of reports.
It is possible that the residents who requested home safety assessments reported different concerns and barriers than the overall population or older adults outside of the Northwest Philadelphia area. The urban setting in which assessments were completed may also mean suburban or rural older adults may have different barriers to aging in place. In addition, with 36 participants, the sample size is relatively small. All of these factors support the need for additional research within alternative demographics. Despite these limitations, this exploratory work using a grounded theory approach helps fill important gaps in the current literature about aging in place from older adults’ perspectives.
Conclusion
This project fills a gap in the literature as current knowledge on older adults’ perceptions about aging in place tends to focus on the values of autonomy, independence, and social connection (Stones & Gullifer, 2016). This research indicates that older adults can self-identify many actionable barriers that threaten their ability to age in place but are often unaware or unable to access resources to resolve these issues. It has been shown that community-dwelling older adults do not discuss concerns about aging in place with their doctors, as they feel that it is outside the scope of their doctor’s role (Grimmer et al., 2015). This research supports the continued need for an accessible outlet for older adults to discuss their concerns and receive additional support. Professionals, such as occupational therapists and social workers, nonprofit organizations, insurance companies, and government agencies can provide the needed means to intercede and connect older adults to resources. However, more programs, funding, and community outreach is necessary to support long-term independence for older adults (Bercaw, 2020).
This research demonstrates a general knowledge and funding gap to support necessary safety, repair, and service needs of community-dwelling older adults. It highlights the need for comprehensive aging programs and resources to educate older adults on home safety, fire safety, normative and nonnormative aging, disability and fall prevention, available community resources, and funding sources to support aging in place. This research demonstrates the potential role of occupational therapists in providing comprehensive assessment and preventive services, due to occupational therapists’ wide scope of practice and expertise in assessing person, environment, and function (AOTA, 2014). This research also supports the need for future funding and health insurance reimbursement for aging in place initiatives to decrease reactionary spending (Andresen et al., 2006; Hay et al., 2002; Rogers et al., 2016).
Supplemental Material
sj-docx-1-jag-10.1177_0733464820988800 – Supplemental material for Older Adults’ Self-Reported Barriers to Aging in Place
Supplemental material, sj-docx-1-jag-10.1177_0733464820988800 for Older Adults’ Self-Reported Barriers to Aging in Place by Brianna Brim, Stacy Fromhold and Shannon Blaney in Journal of Applied Gerontology
Footnotes
Acknowledgements
The authors thank Eric Wilden, MDiv, of Ralston My Way and the caregivers, contractors, and office staff for their support throughout this project and their continued dedication to serving the older adults of Philadelphia. Brianna Brim would like to thank the past and current fieldwork students who contributed to this project as well as Carrie Knight, PhD CCC-SLP, for her mentorship with qualitative methodology. Additional information related to research materials can be accessed by emailing the primary author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB Approval Number
This study was approved by EBB2003 Salus University Institutional Review Board.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.