
Abstract
Ageist attitudes have been associated with negative physical consequences and psychological distress among older adults. Although holding a positive self-image and body image contributes to well-being among older adults, their combined effect on the consequences of ageism has not been examined. Accordingly, the current study examines the moderating role of both variables on the connection between ageism and psychological distress among older adults. Data were collected from 383 older adults (age range = 60–90; M = 71.44; SD = 6.62), who filled out scales assessing ageism, self-esteem, body image, and psychological distress. Psychological distress was associated with reduced self-esteem and body image. In line with the moderation hypothesis, the ageism–distress link remained significant only for individuals with low levels of both self-esteem and body image. The discussion highlights the relevance of both self-esteem and body image as important personal resources which may buffer the connection between ageism and psychological distress among older adults.
Introduction
Ageism, or stereotypical perceptions of older adults, has been associated with various negative physical consequences and psychological distress in old age (see Bodner et al., 2018; Menkin et al., 2020). There are several ways in which ageism may be expressed, either through governmental attitudes which discriminate against older adults, or by negative attitudes demonstrated by younger age-groups (Bodner et al., 2012). Although such negative perceptions can be observed throughout the life cycle (Bodner et al., 2012), it seems that older adults are particularly vulnerable for the negative consequences of internalizing and harboring such attitudes, directed toward their own aging selves (e.g., see Lyons et al., 2018). According to the stereotype embodiment theory (SET; Levy, 2009), older adults may internalize ageist attitudes and views during their life, and as they grow older, these perceptions can become self-definitions through which they see themselves and perceive their own capabilities. Accordingly, such self-ageist individuals demonstrate reduced cognitive, physical, and psychological well-being (see Levy, 2009). Moreover, when such negative stereotypes are targeted against one’s self or one’s age-group, they may compromise older adults’ self-perception (Weiss et al., 2013), as well as their satisfaction with their physical body (see Bergman & Bodner, 2015).
It seems that ageist attitudes are linked with self-esteem throughout the life cycle. From a theoretical perspective, terror management theory suggests that self-esteem may be an important defense for warding off knowledge regarding the inevitability of death (see Martens et al., 2005). Thus, ageism may stem from the fact that older adults can represent a reminder of the physical deterioration linked with the end of life (Martens et al., 2005). As self-esteem is often derived from attributes which diminish in age (e.g., physical strength/beauty), younger individuals may adopt an ageist stance to distance themselves from the older adult age-group, to maintain their positive self-appraisal, and this notion was demonstrated empirically (Martens et al., 2005). Among older adults, longitudinal studies (e.g., Rothermund & Brandtstädter, 2003) and experimental research (e.g., Weiss et al., 2013) have demonstrated how negative age stereotypes affect older adults’ self-concept. Moreover, despite its possible role as a buffer against death awareness in younger cohorts (Martens et al., 2005), ageism is associated with reduced functioning and well-being among older adults (Levy, 2009).
It seems that the major threat to self-esteem vis-à-vis ageism consists of factors relating to physical and body-related changes which occur throughout the aging process. Research has demonstrated that attitudes toward one’s body are linked with self-esteem (see Goldenberg et al., 2000), and that observing older adults who display physical decline elicits increased ageism (Bergman & Bodner, 2015). Interestingly, this issue has not been adequately explored among older adults. Studies examining the connection between older adults’ body image and their perceptions of the aging process demonstrated that the two concepts are linked (Baker & Gringart, 2009), but findings are inconclusive and often conflicting (see Bodner & Bergman, 2019). Moreover, both concepts may contribute together as a personal resource among older adults. More specifically, it is suggested that this age-group may enhance self-esteem in light of age-related changes by physical and/or psychological efforts aimed at maintaining a positive body image (see review by Krekula et al., 2018). However, to date, little is known about the combined utility of both constructs in mitigating the negative effects of older adults’ ageist attitudes on their psychological well-being, despite the importance of both self-esteem (see Weiss et al., 2013) and body image (Bodner & Bergman, 2019) as personal resources, which assist older adults in dealing with age-related attitudes and concerns.
Accordingly, the current study aimed at examining the moderating roles of self-esteem and body image on the connection between ageism and psychological distress among older adults in Israel. Due to the connections between self-esteem and body image among older adults (Baker & Gringart, 2009), and the connections between lower levels of both concepts and negative attitudes toward aging (Bodner & Bergman, 2019; Clarke & Griffin, 2008) and psychological distress (Bergman & Bodner, 2020; Bodner & Bergman, 2019), it was hypothesized that the connection between ageism and psychological distress would be more pronounced among older adults with low levels of both self-esteem and positive body image.
Method
Participants and Procedure
Data were collected from a convenience sample of 383 Israeli community-dwelling older adults (age range = 60–90; M = 71.44; SD = 6.62), of which 168 (48.6%) were women. Most participants stated that they were in a relationship (n = 281, 73.4%), had at least a full high-school education (n = 347, 90.6%), and reported that their economic and health status was at least “pretty good” (n = 318, 83.0%; n = 300, 78.3%, respectively).
Participants were recruited through an online panel company, which targeted community-dwelling older adults, who reported that they were free of cognitive impairments. Anonymity was guaranteed, as personal identifying information was neither required nor given throughout the study. Written informed consent had been obtained from all participants prior to completing the questionnaire. Unless stated otherwise, the scales were back-translated into Hebrew by two experienced bilingual psychologists. The study received ethical approval by an institutional review board of the author’s former university.
Materials
Ageism was assessed using the Hebrew version of the Fraboni Scale of Ageism (see Bodner et al., 2012), which comprises 18 items describing negative age stereotypes and attitudes (e.g., “many old people just live in the past”), rated on a scale ranging from 1 (strongly disagree) to 6 (strongly agree). A mean score is calculated, with higher scores representing higher ageism levels. The Hebrew scale demonstrated high internal consistencies (α = 0.66–0.83; Bodner et al., 2012), and in the current study, Cronbach’s α was 0.79 (see Table 1 for means, SDs, and correlation matrix for the study variables).
Descriptive Statistics and Correlations Among Study Variables.

Note. n = 383. Correlation values represent Pearson coefficients except for coefficients for gender and relationship status that represent point-biserial coefficients, and education, which represent Spearman correlations.
0 = male; 1 = female.
0 = not in a relationship; 1 = in a relationship.
1 = no formal education; 2 = elementary; 3 = partial high-school; 4 = full high-school; 5 = diploma/partial academic; 6 = academic.
p < .05. **p < .01. ***p < .001.
Body image was examined by the Body Appreciation Scale (BAS; Avalos et al., 2005), which requires participants to rate their agreement on a scale ranging from 1 (never) to 5 (always) with 13 statements concerning attitudes toward one’s body (e.g., “I feel good about my body”). The scale has demonstrated high internal consistencies among older adults (α = 0.87–0.89; Meneses et al., 2019), and in the current study, Cronbach’s α was 0.86.
Self-esteem was assessed by the Self-Esteem Questionnaire (Rosenberg, 1965), which requires participants to rate their agreement with 10 statements (e.g., “I take a positive attitude toward myself”) on a scale ranging from 1 (strongly disagree) to 5 (strongly agree). A mean score was calculated, and high scores indicate high self-esteem. This scale was found to be reliable among older adults (α = 0.83; Meneses et al., 2019), and Cronbach’s α in the current study was 0.82.
Psychological distress was assessed by the Hebrew version of the Brief Symptom Inventory (BSI-18; Derogatis, 2001; see Bodner & Bergman, 2019), which requires participants to indicate the degree to which they experienced 18 symptoms over the previous month (e.g., “feeling blue”; “feeling nervous”) on a scale ranging from 1 (not at all) to 5 (a lot). A mean score is calculated, and high scores reflect higher levels of distress. The scale was reliable among older adults (α = 0.95; Kimron & Cohen, 2012); Cronbach’s α in the current study was 0.95.
Participants also provided sociodemographic information, including age, gender, relationship status (not in a relationship/in a relationship), education level (no formal education/elementary/partial high-school/full high-school/diploma or partial graduate studies/academic), and self-rated economic and health status (not good at all/not good/pretty good/good/very good).
Data Analysis
Data were analyzed using the SPSS 24 software (IBM, 2016). Initial correlations between the study variables were calculated, and the hypothesis was examined by a hierarchical regression, with psychological distress as the outcome variable. The first step included the covariates, the second step the main effects, the third included the three possible two-way interactions, and the fourth and final step included the hypothesized Ageism × Body Image × Self-Esteem interaction (see Supplemental Material for additional details regarding the regression analysis and regression coefficients). Significant interactions were probed using Model 3 of the PROCESS 3.4 macro for SPSS (Hayes, 2018), which calculates the regression coefficients for the effects of the predictor (i.e., ageism) on the outcome variable (i.e., psychological distress) for both ±1 SD of the two moderators (i.e., self-esteem and body image).
Results
Initial correlations between the study variables demonstrate that ageism was associated with lower self-esteem levels (r = −.28, p < .001) and increased psychological distress (r = .12, p < .05). Moreover, self-esteem was associated with increased body image (r = .44, p < .001), whereas distress was associated with lower levels of body image (r = −.34, p < .001) and self-esteem (r = −.40, p < .001). The regression analysis (see Supplemental Material) demonstrated main effects of self-esteem (B = −.39, SE = .08, β = −.25, p < .001, 95% CI [−.54, −.23]) and body image (B = −.19, SE = .05, β = −.17, p < .01, 95% CI [−.30, −.08]) for psychological distress. A significant two-way interaction of Ageism × Self-Esteem was discovered, as well as the hypothesized three-way interaction of Ageism × Body Image × Self-Esteem (B = .05, SE = .02, β = .16, p < .01, 95% CI [.09, .14]), which added 1.6% to the model variance (Total R2 = .336). Probing the interaction using PROCESS (Hayes, 2018) revealed that the positive association between ageism and psychological distress was significant only for individuals with low self-esteem and body image (B = .16, SE = .08, β = .14, p < .05, 95% CI [.01, .32]) and was nullified for the three alternative combinations (high/low self-esteem and body image; low/high self-esteem and body image; high self-esteem and body image; see Figure 1), although a near-significant negative association between ageism and psychological distress was found for high self-esteem and low body image (B = −.22, SE = .13, β = −.19, p = .08, 95% CI [−.25, .05]). The significant main effects and interaction remained unchanged when the model was examined both with and without covariates.
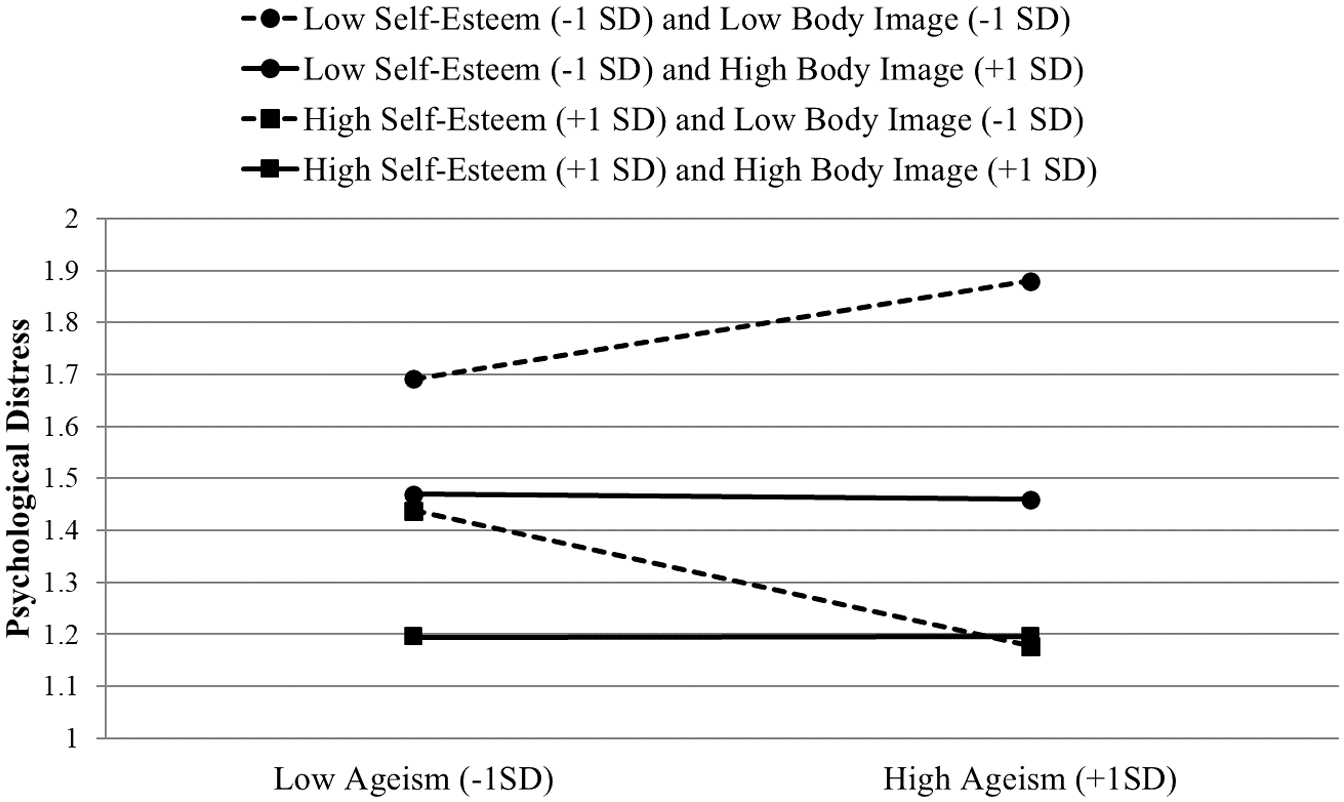
The three-way interaction between ageism, self-esteem, and body image in predicting psychological distress (n = 383).
Discussion
The aim of the current study was to examine whether personal resources, such as maintaining a positive self-esteem and body image, may mitigate psychological distress associated with ageism among older adults, as stipulated by terror management theory (see Martens et al., 2005). The results demonstrate that both self-esteem and body image were associated with lower levels of psychological distress. Interestingly, no main effect was found for ageism in this regard, despite its significant correlation with psychological distress. This could stem from the fact that ageism among healthy older adults was found to be less pronounced in comparison to younger age-groups (Bodner et al., 2012). Nevertheless, this issue requires further investigation in future studies.
In line with the hypothesis, the ageism–psychological distress association was moderated by older adults’ self-esteem and positive body image. More specifically, the negative association between ageism and distress was significant only among individuals with low self-esteem and low positive body image. Accordingly, it can be argued that holding a positive self-esteem and/or a positive perception of one’s body in old age can serve as a personal resource which may mitigate psychological distress associated with ageism. This is in line with the theoretical assumptions of SET, which delineates the particular susceptibility of older adults to ageist stereotypes (Levy, 2009). Previous research has demonstrated the utility of both self-esteem (Bergman & Bodner, 2020) and positive body image (Bodner & Bergman, 2019) with regard to lower psychological distress among older adults. However, this is the first study to examine the notion that self-esteem and one’s physical appearance and capabilities, both of which undergo significant changes during the aging process (Martens et al., 2005), may jointly buffer the connection between ageism and psychological distress in older adults. It should be noted that although the negative association between ageism and psychological distress among individuals with high self-esteem and low body image was not significant, it may nevertheless indicate a surprising and intriguing pattern. This pattern may indicate the relative versatility of self-esteem with regard to ageism and psychological distress, a direction which may be further enhanced by the significant two-way interaction of ageism and self-esteem. However, this issue requires further investigation.
The findings should be seen in light of the study’s limitations. First, the cross-sectional design precludes the ability to establish causality. Although studies have demonstrated a causal connection between ageism and adverse physical (e.g., balance), cognitive (e.g., memory performance), and psychological (e.g., depressive symptoms) outcomes (see Bodner et al., 2020; Levy, 2009), it is possible that a negative self-appraisal of one’s self and/or one’s body may lead to increased ageism and subsequent distress, and these issues need further clarification through longitudinal studies. Second, although it was assumed that the online nature of the study would preclude the participation of older adults with cognitive decline, this was not directly examined. Moreover, although distress levels of older adults in the current work were comparable with those of previous cohorts in Israel (e.g., Shrira et al., 2014) and other countries (e.g., Lyons et al., 2018), research is needed to generalize the findings to additional cohorts of older adults (e.g., older adults living in assisted living facilities), while explicitly assessing physical and cognitive abilities. In this regard, it should also be stated that subjective assessments of health and economic status, used in this study, may be subjected to bias. Accordingly, it is important to examine the results while employing more objective measures of health (e.g., medical history) and economic status (e.g., household income).
Nevertheless, the current study demonstrates the importance of both self-esteem and body image for understanding the link between ageism and psychological distress among older adults. It seems that enhancing older adults’ ability to appraise themselves and their body in clinical settings, by working toward a more balanced view of their personal worth and physical capabilities in light of age-related physical changes, may be important for mitigating detrimental psychological distress associated with internalized stereotypical views of age and aging.
Supplemental Material
sj-pdf-1-jag-10.1177_07334648211009658 – Supplemental material for Ageism and Psychological Distress in Older Adults: The Moderating Role of Self-Esteem and Body Image
Supplemental material, sj-pdf-1-jag-10.1177_07334648211009658 for Ageism and Psychological Distress in Older Adults: The Moderating Role of Self-Esteem and Body Image by Yoav S. Bergman in Journal of Applied Gerontology
Footnotes
Author’s Note
The study was approved by the IRB of the School of Social Work, Ariel University, Ariel, Israel on March 1, 2017.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was partially supported by the author’s former university.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.