
Abstract
We examined whether Medical Marijuana Legislation (MML) was associated with site of death. Using state-level data (1992–2018) from the National Vital Statistics System (NVSS), we employed difference-in-differences method to compare changes in death rate among older adults at four sites—nursing home (NH), hospital, home, hospice/other—over time in states with and without MML. Heterogeneity analyses were conducted by timing of MML adoption, and by decedent characteristics. Results show a negative association between MML implementation and NH deaths. Among early adopters (states with weakly regulated programs) and decedents with musculoskeletal disorders, there was a positive association between MML implementation and hospital deaths, whereas among late adopters (states with “medicalized” programs), there was a positive association between MML implementation and hospice deaths. Decline in NH deaths may reflect increased likelihood of transfers due to threat of Federal enforcement, penalties for poor outcomes, and liability concerns. Future studies should examine these associations further.
Introduction
Where people die is a key determinant of care quality at the end-of-life (EOL). Despite documented preferences for dying at home, a substantial share of Americans die in a hospital or a nursing home (NH) (Teno et al., 2018). Hospital deaths are expensive, associated with aggressive interventions, and linked with high levels of stress among bereaved family members (Wright et al., 2010). In nursing homes, studies show insufficient pain and symptom management (Teno et al., 2004; Hanson et al., 2008) as well as frequent and often unnecessary terminal hospitalizations (Temkin–Greener et al., 2013; Xing et al., 2013). While institutional death rates have decreased over the past two decades (Teno et al., 2018), there exists limited evidence on the association between public policy and site of death patterns in the U.S.
The legalization of medical cannabis represents a relevant policy in this context. Although prohibited at the Federal level, most states have adopted laws allowing therapeutic use of cannabis for several “qualifying” symptoms and conditions including pain, nausea/vomiting, cachexia, muscle spasms, cancer, and multiple sclerosis. Recent research shows that “medical marijuana legislation” (MML) is associated with a surge in medical cannabis use among older adults (Martins et al., 2016). Studies using data from patient registries also find older adults to represent a substantial share of all registered medical cannabis users in MML states (Kaskie et al., 2017). In this study, we provide the first evidence on the association between MML passage and site of death patterns in the United States.
Medical Marijuana Legislation passage can influence site of death in several ways. First, MML increases access to a new medical treatment to terminally ill patients who experience multiple distressing symptoms that overlap with common qualifying symptoms listed in state MMLs as well as symptoms for which there exists strong evidence of cannabis efficacy (NASEM, 2017). Studies demonstrate that MML passage leads to improvements in pain scores among older adults (Nicholas & Maclean, 2019) and induces substitution of cannabis for prescription opioids (Bradford & Bradford, 2017). Further, there is growing support in palliative medicine for the use of cannabis as an adjuvant therapy. Specifically, studies find that cannabis when co-administered with opioids, produces opioid-sparing effects and reduces the rate of opioid use (Pawasarat et al., 2020). Improved palliation of troubling symptoms may increase the likelihood of death at hospice or home.
Alternatively, cannabis may lead to harmful outcomes. Cannabis use (smoked and ingested) has been found to increase the risk for lung disease, pneumonia and chronic bronchitis (Tetrault et al., 2007; Vozoris et al., 2019). Cannabis is linked to an increased risk of drug-drug interactions and there are concerns about its effects on cognitive functioning, particularly decreases in neurocognitive reserve, dizziness, and memory impairment (Minerbi et al., 2019). Late-life cannabis is associated with increased risk for injury and emergency department use (Choi et al., 2018). A recent study also showed that MML passage is linked with an increase in cardiac-related mortality, with stronger effects in states with a more lenient approach towards cannabis dispensing (Abouk & Adams, 2018). Potential adverse effects of cannabis use may increase the likelihood of hospital deaths. This may occur directly or indirectly through nursing home transitions. With regard to the latter, previous work shows that top conditions associated with frequent hospitalizations among nursing home residents include falls, pneumonia, and bronchitis (Grabowski et al., 2017). As described above, these conditions are also associated with potential harmful effects of cannabis use, which may be magnified in states with weakly regulated MML programs.
Medical Marijuana Legislation passage may also relate to site of death through mechanisms other than clinical efficacy and safety. Specifically, the discordant legal status of cannabis imposes regulatory and financial burdens on institutions, particularly nursing homes as these are regulated by both state and Federal laws. Conflicting state and federal policies on cannabis use may create incentives for nursing homes to reduce the numbers of nursing home deaths by transferring residents to hospitals and other locations. Nursing homes have behaved similarly in the past, increasing nursing home-to-hospital transfers in response to government reimbursement policies and the increasing burden of litigation (Temkin–Greener et al., 2013; Intrator et al., 2007; Perry et al., 2010).
Given this complex set of pathways, the association between MML passage and site of death is unclear. We use aggregate state-level panel data (1992–2018) on mortality from the National Vital Statistics System (NVSS) and estimate event study and difference-in-differences models to examine this question. We also investigate how heterogeneity in MML regulatory environment across states and variation in decedent characteristics moderate our results.
Methods
Outcome
We employed public-use NVSS mortality data from 1992–2018 to identify deaths at different locations in each state in each year. The NVSS collects death certificate records for all deaths occurring within the U.S., which provide information on site and year of death, gender, age, and underlying cause of death. The NVSS aggregates these data to the state-level. From 1992–2002, NVSS identified a decedent’s site of death as either nursing/residential facility, hospital, home, or other/unknown. Before 2003, deaths at inpatient hospice facilities were included in the “other/unknown” category. From 2003 onwards, inpatient hospice facility was included as a standalone category. For consistency, we combined deaths at hospice and those in other/unknown locations in one category for all study years. We restricted our analysis to deaths among those aged 65 years and older and excluded deaths due to external causes (e.g., homicide) as these are less likely to be impacted by MML-induced cannabis use.
For a given state-year, outcomes were defined as the number of deaths at four sites (nursing home, hospital, home, hospice/other) per 100,000 residents in the age 65 and older population. In heterogeneity analyses by age group (65–74 years, 75–84 years, 85 years and above) and gender, we identified these outcomes in the same age/sex group. We also examined site-specific death rates associated with 11 common underlying causes of death. Other causes of death were excluded due to small cell sizes.
Exposure
The state of California adopted the first MML in November 1996. As of June 2018, 29 states and DC had enacted an MML (Supplementary Table S1). These 30 states comprised the “treatment group” in the main analysis. For each MML state, exposure is coded as “1” commencing from the effective year of passage if the policy was implemented by June 30th of that year. If MML was effective on or after July 1st of a given year, the next year is considered as the beginning of the treatment period. Exposure is coded “0” throughout for states that did not enact an MML during 1992–2018.
We also explore whether differences in state MML programs influence our outcome of interest. We do so because previous work cautions against the empirical treatment of MMLs as dichotomous choices as it ignores significant heterogeneity across state programs (Pacula & Smart, 2017). In particular, the release of the “Ogden Memo” in 2009 (Ogden David, 2009), which directed U.S. Department of Justice attorneys to deprioritize prosecuting users and suppliers in states with MMLs, represented a key shift in the cannabis policy landscape (Pacula & Smart, 2017). The characteristics of MMLs passed after 2009 (N = 17) differ considerably from those of MMLs in earlier adopting states (N = 13).
Given threats of federal prosecution, early MMLs rarely required patients to register with a state authority. Early laws were also ambiguous with reference to regulating cannabis supply through state-licensed dispensaries (Pacula & Smart, 2017). Instead, these states allowed approved patients (or their legally designated caregivers) to grow a specific number of cannabis plants at home. However, allowance for home cultivation has several drawbacks including the lack of adequate quality control measures in processing and producing cannabis (e.g., high THC levels [the chemical that regulates cannabis potency] in home-made edibles and concentrates, use of pesticides, contaminants such as bacteria and mold, and inconsistency in product strength) (Borodovsky & Budney, 2017; Carlini, 2017).
In contrast, MMLs passed after 2009 established comprehensive regulatory controls over cannabis supply and did not allow personal cultivation by patients or caregivers (except Oklahoma and Missouri). Later programs are also far more stringent and medicalized, reflecting the practices of medical care, and pharmaceutical regulation (Pacula & Smart, 2017; Williams et al., 2016). For example, late adopters limit smoking, require testing and labeling of cannabinoid profile, and necessitate a bona-fide clinical doctor-patient relationship for continued management of qualifying condition(s)/symptom(s) (Williams et al., 2016). In light of these differences, we test for heterogeneity in response among early (MML passage before 2010) and late adopting states (MML passage in 2010 or later).
Statistical Analyses
We estimated the association between MML and death rate among older adults at four sites (nursing/residential facilities, hospitals, homes, hospice/other) using Difference-in-Differences (DD), an approach that entails comparing mean changes in an outcome in a treatment group (states with MML) before and after a policy change with mean changes in a control group (states without MML). For the main analysis, we estimated four linear regressions (separately for each outcome) with a binary indicator for effective MML, with state and year fixed effects, and with controls for a state’s racial, ethnic, and gender distribution in the age 65 and over population, percentage of population over 85 years, unemployment rate, per capita income, Medicaid expenditures per capita, Home and Community Based Services (HCBS) expenditures per capita, and the presence of a Personal Care Services State Plan Option. Standard errors were clustered at the state-level and all regressions were weighted by the 65 and older population. To examine heterogeneity by regulatory environment, we tested for differences in response among early and late adopting states. We conducted 2 separate DD analyses with early and late adopting states comprising the treatment group in each analysis, respectively. The control group in both cases comprised of non-adopting states. To examine heterogeneity by decedent-level characteristics, separate DD regressions were conducted for subgroups defined by cause of death, age, and gender.
DD requires that baseline temporal trends (but not absolute levels) of the outcome are equivalent in states with and without MML; with the corollary that trends in both groups would have continued to be the same in the absence of a policy change. We tested this assumption by estimating “event studies” for all models. An event study is a modification of the original DD regression equation that decomposes the overall treatment effect into a series of leads and lags (or pre- and post-relative time periods with respect to MML implementation year). States that did not implement an MML during 1992–2018 are coded as 0 for all leads and lags. There is a minimum of 5 years of pre-event data for all treatment states. The coefficients on lead terms capture the difference in trends between the treated and comparison units before the treatment occurs. Inability to reject the hypothesis that the lead coefficients are statistically indistinguishable from 0 provides suggestive support for the DD assumption. The event study also demonstrates the evolution of the treatment effect after policy passage. The coefficients on lag terms detect regression-adjusted trends in the post-period informing how the impact of MML implementation changed over time. All DD and event study regressions controlled for the same set of covariates as the main model, were weighted by the 65 and older population, and included standard errors clustered at the state-level.
Results
Summary statistics.

*p < .05. **p < .01. ***p < .001.
a30 states including the DC.
b“Difference” represents statistical significance associated with the difference between the two means/proportions and were assessed using t-tests. Standard deviations (SD) in parenthesis.
cPer capita Medicaid expenses, per capita HCBS expenses, and per capita income are expressed in 2018 dollars.
Association of MML a Passage with Death Rate at Four Sites.
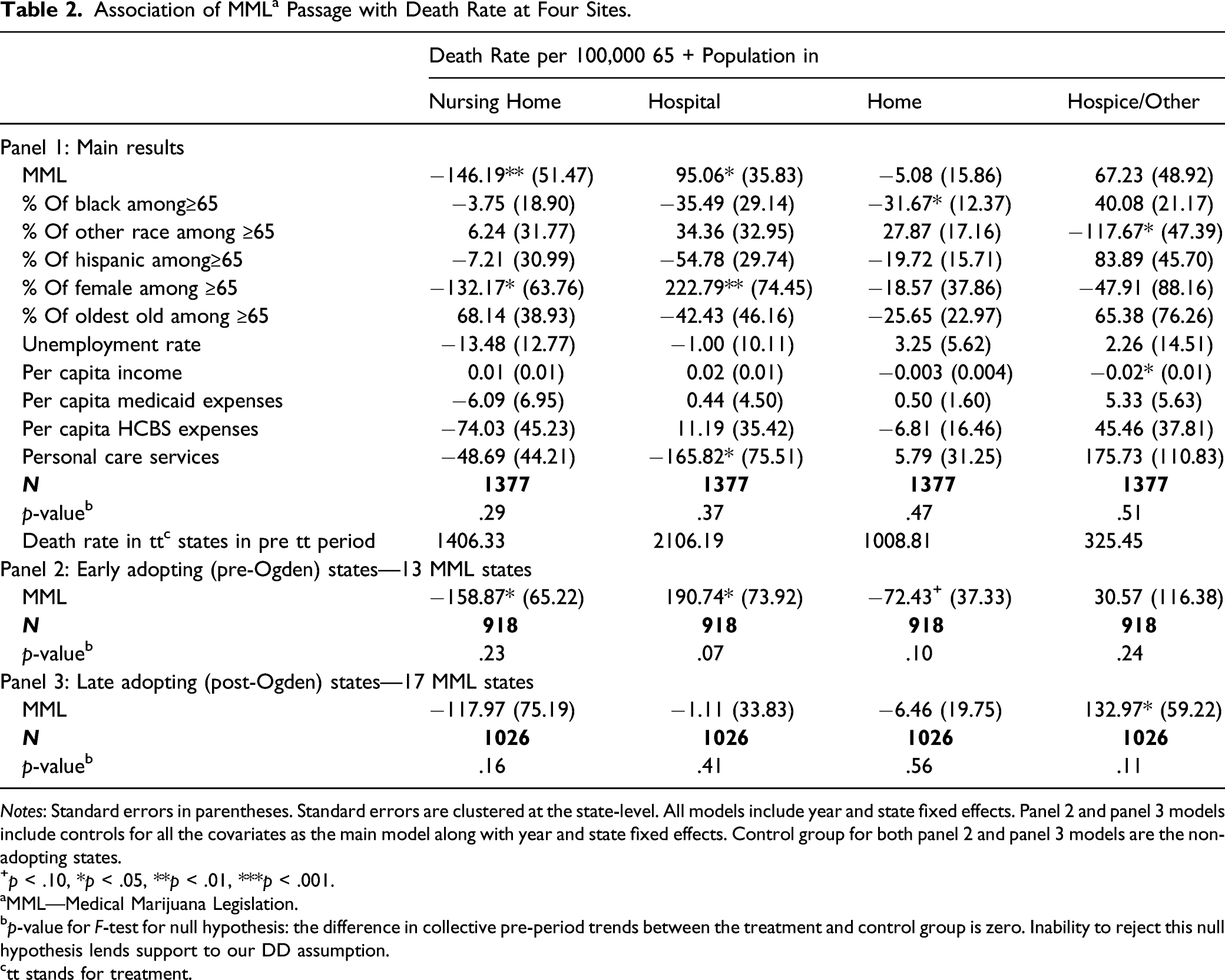
Notes: Standard errors in parentheses. Standard errors are clustered at the state-level. All models include year and state fixed effects. Panel 2 and panel 3 models include controls for all the covariates as the main model along with year and state fixed effects. Control group for both panel 2 and panel 3 models are the non-adopting states.
+p < .10, *p < .05, **p < .01, ***p < .001.
aMML—Medical Marijuana Legislation.
bp-value for F-test for null hypothesis: the difference in collective pre-period trends between the treatment and control group is zero. Inability to reject this null hypothesis lends support to our DD assumption.
ctt stands for treatment.
Table 2, panels 2 and 3, show considerable heterogeneity across early and late adopting states. The pattern of main results—a decrease in nursing home deaths and an increase in hospital deaths—was mirrored only in early adopting states (those with weakly regulated MML programs). In late adopting states, event study models—Figure 1—demonstrate that MML passage was associated with a decrease in nursing home deaths approximately three or more years post MML implementation (though the overall effect on death rate in nursing homes among late adopters is statistically insignificant) and a corresponding increase in deaths at hospice and other facilities. Among late adopters, post-implementation coefficients for hospital deaths were relatively flat and statistically insignificant (Figure 1). Event study results for early and late adopting MML states. 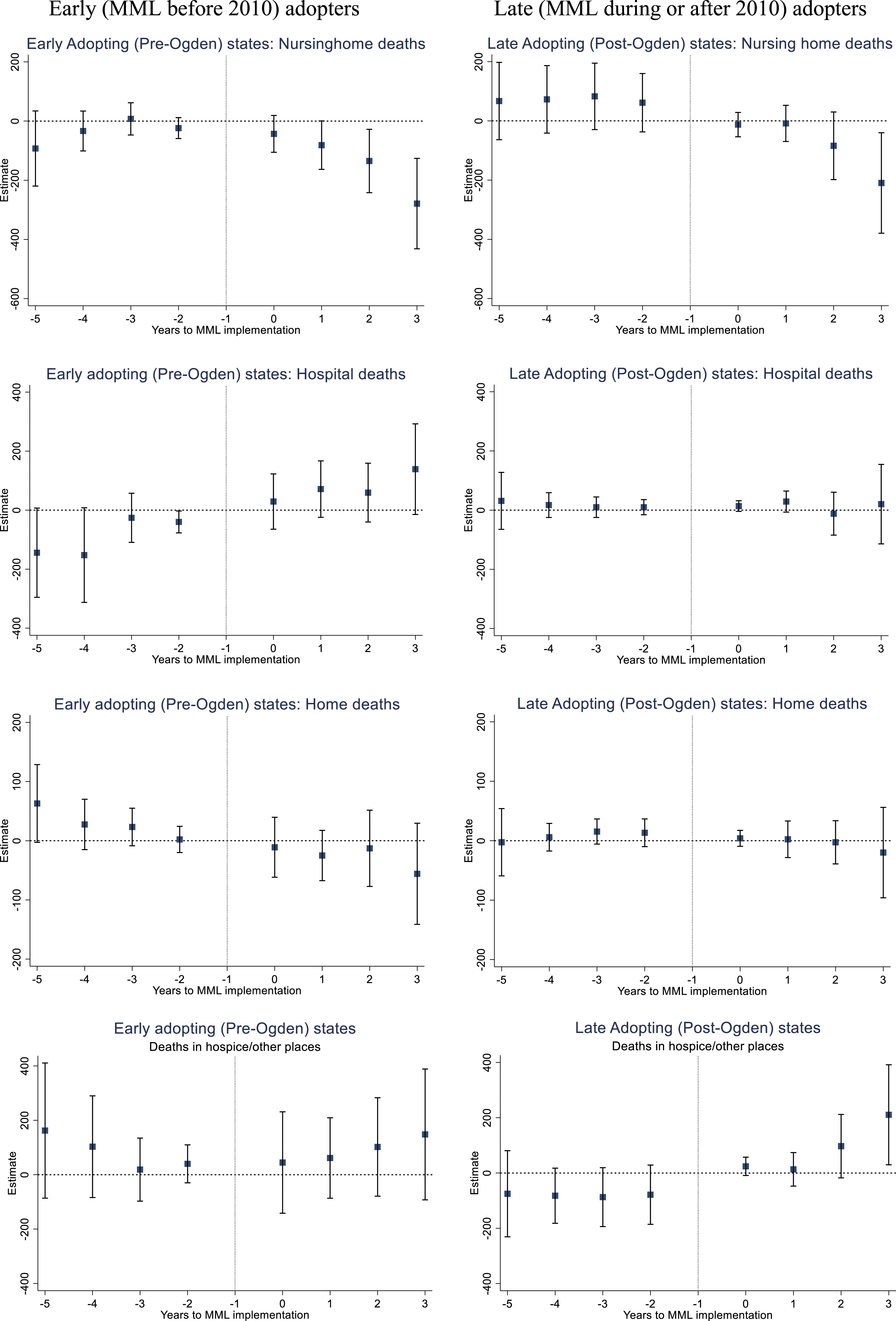
Association of MML a Passage with Site of Death by Underlying Cause of Death.

Notes: Standard errors in parentheses. Standard errors are clustered at the state-level. All models include all covariates included in the main model, state and year fixed effects. Underlying causes of death not examined due small cell sizes: diseases of the eye and adnexa, diseases of the ear and mastoid process, diseases of the skin and subcutaneous tissue, congenital malformation, deformation and chromosomal abnormalities.
+p < .10, *p < .05, **p < .01, ***p < .001.
aMML - Medical Marijuana Legislation.
bp-value for F-test for null hypothesis: the difference in collective pre-period trends between the treatment and control group is zero. Inability to reject this null hypothesis lends support to our DD assumption.
Association of MML a Passage with Site of Death by Age Groups and Gender.
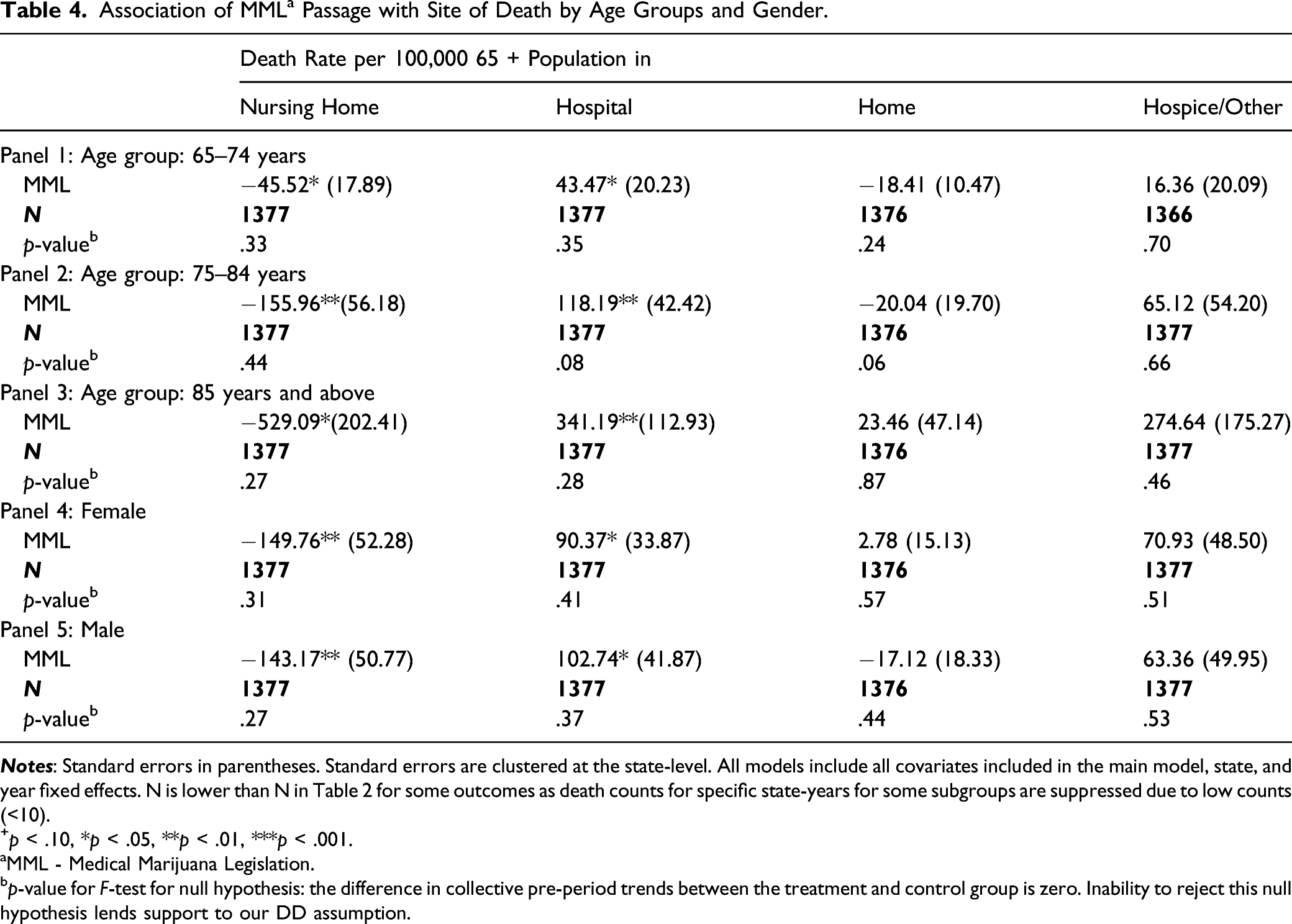
+p < .10, *p < .05, **p < .01, ***p < .001.
aMML - Medical Marijuana Legislation.
bp-value for F-test for null hypothesis: the difference in collective pre-period trends between the treatment and control group is zero. Inability to reject this null hypothesis lends support to our DD assumption.
We conducted several sensitivity checks. We checked the robustness of our findings by employing another dataset. Specifically, we used state-level panel data [1994–2018] on inpatient health care utilization at EOL (last 6 months of life) from the Dartmouth Atlas (2021) dataset. We examined the association between MML passage and number of ICU/CCU days and inpatient days per decedent during terminal hospitalization. Estimates from Poisson regressions show that among early adopters, MML passage was associated with an increase in the number of ICU/CCU days; while among later adopters the coefficient was negative and statistically insignificant. Inpatient days during terminal hospitalization followed a similar pattern, however the coefficients were not statistically significant. These results are provided in Supplementary Table S2. We included a control for presence of recreational cannabis policy in the main model. We utilized an alternative measurement of the outcome—percent of deaths at each site with the denominator defined as total deaths in the age 65 and over population. We separated hospice deaths from the “other/unknown” category and conducted DD analysis for 2003–2018 time period for this outcome. In all cases, the pattern of results was similar to our main results (Supplementary Tables S3–S5). In another robustness test, we restricted the event study to include only those states with three or more post-implementation time periods. Thus, we excluded six states that implemented MML during or after 2016 thereby ensuring that the remaining 24 treatment states contributed to all policy leads and lags. Results followed a similar pattern and pre-trends continued to be statistically insignificant. This indicates that the treatment effect is due to changes in impact over time and not due to temporal changes in group composition (Supplementary Figure S2).
Discussion
We provide the first evidence on the potential association between MML passage and site of death in the U.S. In the aggregate, MML implementation was associated with an increase in hospital deaths and a decrease in nursing home deaths. However, subgroup results demonstrate that this aggregate finding is masked by heterogeneity in MML regulatory environment and underlying cause of death.
This study has three main findings. First, we find robust evidence that deaths at nursing homes decrease following MML implementation. Compared to the pre-treatment mean in treatment states, the decrease of 146 deaths per 100,000 older adults in our main results accounts for a 10% relative decrease in the death rate in nursing home settings. This decline was observed across multiple decedent-level characteristics and for both early and late adopting states. The consistency of this result potentially reflects the uniqueness of the nursing home industry, which is highly regulated (i.e., subject to frequent quality assessments/inspections and reporting requirements) and exposed to substantial litigation threat (Konetzka, 2006). The salience of these dimensions is magnified in the context of cannabis use—a Schedule I controlled substance with paucity of evidence on safety consequences. In this context, a decrease in nursing home deaths may reflect an increased likelihood of transfers of terminal nursing home residents (who either use cannabis or indicate an interest in doing so) to hospitals and hospices. Specifically, fear of enforcement actions from the Federal government, penalties for poor quality outcomes, and additional liability concerns (associated with cannabis storage, disposal, dispensing and diversion as well as objections from other residents) may incentivize nursing homes to transfer certain terminal patients to other locations. Hesitancy surrounding this issue is reflected in a recent position paper from the American Medical Directors Association (AMDA) formally cautioning against routine use of cannabis in post-acute and long-term care settings (AMDA, 2019).
Second, among early adopters, the potential MML-associated decline in nursing home deaths appears to be compensated by an increase in hospital deaths. The aforementioned pattern of results—that is, a decrease in nursing home deaths and an increase in deaths at other locations, suggesting increased likelihood of transfers—is also stronger among early-relative to late adopters. A combination of ambiguity in MML laws in early adopting states and heightened threat of federal prosecution before 2010 may account for this finding. An increase in hospital deaths may be linked to potentially harmful effects of cannabis use as early adopting states paid relatively little importance to dosing levels, guidance for new users, regulation of cannabis potency, or a system for addressing food safety and contamination issues for home grown cannabis (Ghosh et al., 2015). Previous research shows states with loosely regulated systems experienced large increases in cannabis use and cannabis-associated adverse outcomes that persisted even after amendments were made to these MML programs following federal guidance in 2009 (Ghosh et al., 2015; Powell et al., 2018). In addition to early adopters, the finding of a decline (increase) in nursing home (hospital) deaths is reflected among decedents with musculoskeletal diseases. There is a high prevalence of cannabis use in this population due to pervasiveness of chronic pain (Leroux et al., 2020). Cannabis use and musculoskeletal pain are also independent risk factors for falls (Choi et al., 2018; Leveille et al., 2009), and this supports the proposed mechanism of increased nursing home transfers to hospitals due to higher potential for adverse effects. Additional analysis (available on request) demonstrates that the finding related to musculoskeletal diseases is mainly attributable to early adopting states, which is consistent with prior discussion on the consequences of lenient cannabis regulation in these states.
Third, among late adopters, MML-associated decline in nursing home deaths (although smaller in magnitude relative to early adopters) occurs concurrently with an increase in deaths at hospices and other locations. An absence of change in hospital deaths may possibly relate to the presence of more regulated and medicalized cannabis programs in these states.
Even though hospice is largely funded with Medicare/federal dollars, MML-associated increase in hospice deaths may reflect growing acceptance of cannabis in palliative medicine where the focus of care is on patient choice and autonomy, comfort, and quality of life as defined by individuals and their caregivers (Carter et al., 2011). This result may also reflect the inclusion of “hospice enrollment” as a distinct qualifying condition for medical marijuana use in several state MMLs (ProCon.org, 2021). Additionally, nursing homes and hospices experience different quality regulation burdens. As compared to nursing homes, hospice quality measures and standards are relatively newer and subject to less frequent inspections and quality monitoring efforts. For nursing homes, regular surveys are required every 9–15 months, whereas hospices are surveyed every 3 years. The Centers for Medicare and Medicaid Services (CMS) publicly reports detailed inspection data, penalties for violation, and star ratings for individual nursing homes. In contrast, public reporting on hospice quality measure scores began only recently (in 2017). Further, star ratings for hospice quality are not provided, and federal inspection quality deficiencies are not publicly reported (Harrington et al., 2017). These differences suggest that hospices may be less sensitive to the potential risk of losing federal funding. Indeed, in contrast with AMDA apprehension, a recent survey of palliative care providers finds overwhelming support for the use of medical cannabis in hospice settings regardless of its legal status (Costantino et al., 2019).
There are several limitations to this study. NVSS does not include other outcome indicators for assessing quality of care at the EOL. Our data only allows us to examine where a person was at the moment of death. Patients with the same site of death can have vastly different EOL experiences depending upon the duration of their stay at a particular site. While we address this limitation to some extent with the robustness check using the Dartmouth Atlas data on inpatient utilization during EOL, we cannot assess other EOL quality indicators. Additionally, the underlying cause of death in NVSS is selected from conditions entered by the medical certifier in the cause of death section of the death certificate and coded according to the most current International Classification of Diseases (ICD) revision (Kochanek et al., 2019). Thus, accurate classification of causes of death may vary based on training and qualifications of these professionals as well as ICD revisions over time (Becker et al., 2021; Kochanek et al., 2019). Further, the coding of underlying cause of death may not comprehensively reflect death certificate information when multiple causes of death are present (Kochanek et al., 2019). Beyond limitations associated with NVSS data, it is likely that our analyses did not account for all possible variables that could influence MML passage and site of death. While our methods try to address this through various mechanisms, omitted variables may still potentially lead to spurious correlations.
Despite these limitations, this study sheds light on an important and novel question relating to public policy and site of death patterns. The results point to potential unintended consequences of MML passage—greater likelihood of nursing home transitions, particularly to hospitals among states with weakly regulated programs—that warrant further study. In states with more recent MMLs, the positive association with increased deaths at hospices reflects an encouraging trend. These results underscore the importance of examining heterogeneity in state MML programs in relation to various health outcomes. They also draw attention to the consequences of the long-standing conflict between state and federal positions on cannabis legalization. Enhanced policy harmony may decrease transfer incentives and encourage greater provision of palliative care and hospice services within nursing homes.
Supplemental Material
sj-pdf-1-jag-10.1177_07334648211058720 – Supplemental Material for Legalization of Medical Cannabis and Site of Death: Evidence From National Vital Statistics Mortality Data
Supplemental Material, sj-pdf-1-jag-10.1177_07334648211058720 for Legalization of Medical Cannabis and Site of Death: Evidence From National Vital Statistics Mortality Data by Divya Bhagianadh and Kanika Arora in Journal of Applied Gerontology
Footnotes
Author Contributions
K. Arora and D. Bhagianadh conceptualized the study. D. Bhagianadh conducted the data analysis, wrote the first draft, and assisted with revising the manuscript. K. Arora supervised the data analysis, wrote the final draft, and revised the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Dartmouth Atlas End-of-Life Inpatient care dataset used in the robustness check section was obtained from Dartmouth Atlas Data website, which was funded by the Robert Wood Johnson Foundation, The Dartmouth Clinical and Translational Science Institute, under award number UL1TR001086 from the National Center for Advancing Translational Sciences (NCATS) of the National Institutes of Health (NIH), and in part, by the National Institute of Aging, under award number U01 AG046830.
Supplementray Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.