
Abstract
A significant research gap on socioeconomic determinants of oral health among older persons is that socioeconomic indicators, like employment status, have essentially been problematized and measured using a cross-sectional approach. Based on a life course approach, and using data from a population-representative, face-to-face and longitudinal-retrospective survey focused on older people in Chile (N = 802), we reconstructed representative types of individual employment trajectories and measured their association with different oral health indicators in old age. Our results show that employment trajectories characterized by continuous, formal, full-time employment have a protective effect for multiple oral health indicators among older people. Our study demonstrates the need for public policies on oral health in old age to incorporate a life course approach and to consider the negative impact of constantly working in informal employment or being out of the labor market permanently, particularly in countries like Chile where temporary and informal employment has risen steadily.
Keywords
Introduction
One of the key dimensions of health and wellbeing among the growing proportion of older persons in the world is oral health (Schensul et al., 2020). Adequate oral health in old age not only allows the maintenance of a natural, healthy, and functional dentition, but also contributes to increase life expectancy of older adults, mitigates the risk of suffering non-communicable diseases, and helps to face a healthy aging process with greater self-esteem (Masood et al., 2017; Shokry et al., 2018). Also, oral diseases among older people such as periodontal disease or oral cancer have a high-cost burden for health systems and are unfortunately highly prevalent in some world regions (Kossioni et al., 2018; León et al., 2018).
The literature shows that most old age individuals in developed and high-income countries such as the United States, Sweden, or Germany have optimal levels of oral health indicators, such as high levels of retention of natural teeth or low prevalence of tooth decay. Among other reasons, this is due to high standards of access, prevention, and sanitary conditions throughout their lives, as well as continuously increasing spending on oral healthcare services particularly among individuals who face greater economic adversity (Müller et al., 2007;Thomson, 2014). In developing countries such as those in Latin America, which have shown less progress in oral health prevention programs, there is still very little scientific evidence on oral health of older adults (León et al., 2018).
As in the case of other measures of health, socioeconomic determinants are a substantial source to explain the diversity of oral health conditions among older persons (Amoah et al., 2021; Schensul et al., 2020). What we do know is that people facing adverse social environments have worse oral health on average than those with high socioeconomic status (Gülcan et al., 2015; Tsakos, 2011). The mechanisms that have been proposed to explain this association include contentions that people of lower social status have worse material conditions (e.g., poor nutrition and poor living conditions), worse psychosocial conditions (stress and discrimination), greater health risk behaviors (higher tobacco and alcohol consumption and more sedentary lifestyle), and lower access to health services (Thomson et al., 2004).
One illustrative indicator of socioeconomic status is the presence or absence of paid employment. People who are active in the labor market and have access to remuneration have better oral health conditions (Al-Sudani et al., 2017), for example, in terms of better oral hygiene, greater access to dental care services (Al-Sudani et al., 2016), and less tooth loss (Sato et al., 2018).
A significant gap of the research on socioeconomic determinants of oral health among older persons is that socioeconomic indicators have essentially been problematized and measured using a cross-sectional approach or focusing on a single point in time. However, life course research has highlighted that the health status in old age stem from people’s continuous exposure to social advantages and disadvantages at different stages of life (e.g., childhood, youth, and adulthood), which accumulate and lead to increasing inter-individual inequalities in health as people age (Ayalon, 2018; Kuh et al., 2003; Madero-Cabib et al., 2019a). If we take employment into account, we see only one study based on this perspective conducted in Finland, which demonstrates that employment histories characterized by stable and formal employment are associated with less edentulism, more functional dentition, and better clinically examined oral health (Al-Sudani et al., 2015).
This exploratory study has two objectives. First, to reconstruct representative types of employment trajectories throughout the life course in Chile, and second, to measure the influence of these trajectories on different indicators of oral health in old age.
Chile is a developing country that is highly unequal in socioeconomic terms (Gini Coefficient = 0.55), which has a Health Program for older people to facilitate access, opportunity, and quality in terms of healthcare (Ministerio de Desarrollo Social, 2013). Unfortunately, however, the efforts made in oral health have not been sufficient. The National Health Survey (or “Encuesta Nacional de Salud”) shows that the prevalence of tooth decay among older persons increased from 44.7% to 57.2% between 2003 and 2017 (Ministerio de Salud Chile, 2018). There is, therefore, a great need to understand the life course factors that lead to poor oral health in old age.
Methods
Data
This study used data collected in the population-representative, face-to-face and longitudinal-retrospective survey “Life course and vulnerability among older people in Santiago, Chile.” This is the first survey conducted in Chile to collect retrospective annual information on multiple dimensions of the life course. It was applied to 802 people from 65–75 years of age living in Santiago, the capital of Chile, which is home to approximately 40.5% of the country’s total population. The research project has been approved by the Ethics Committee of the Faculty of Social Sciences at Pontificia Universidad Católica de Chile (institutional review board [IRB] approval number: 190124005), which conforms to the provisions of the Declaration of Helsinki, the Declaration of Singapore, and the Nuremberg Code. All participants in this research signed informed consent.
The survey was conducted between March and August 2019, and the data collection was carried out in accordance with the most recent quality standards defined by the American Association for Public Opinion Research (2016). Based on these standards, the co-operation rate was 88.8%, the response rate was 66.5%, and the refusal rate reached 8.3%. Finally, to avoid possible selection bias, the study sample was weighted by an expansion factor that corrects our estimates according to known characteristics of the 65–75 age group of the population in the city of Santiago (e.g., area of residence, educational level, and gender).
The data collection process involved a retrospective longitudinal instrument called life course calendars, which enabled the participants to recall and chronologically organize various events during their lives, along with the approximate dates of occurrence (Morselli et al., 2016). The life course calendar used in this study was structured in such a way that it would be able to address the three main mechanisms involved in the retrospective exercise of memory: hierarchical order, sequential order, and the interrelated order of life events (Morselli et al., 2016, 2019). This life course calendar also involved constant interviewer-respondent interaction (it was not self-administered), which has been shown to increase the number of events reported in different domains and life stages and allows the information provided by the respondent to be “double-checked,” thus improving the accuracy of the responses (Morselli et al., 2019).
Measures
Independent Variable: Employment Trajectories
In order to reconstruct types of employment trajectories over the life course, we used a variable included in the life course calendar called “labor force status,” which measured three dimensions annually: (i) presence or absence of paid employment; (ii) presence of full-time or part-time paid employment; and, finally, (iii) presence of formal or informal paid employment, which corresponds to being (or not) in a job with which one contributes to social security, an illustrative indicator of labor formality in Chile (Madero-Cabib et al., 2019b, 2019c). The combination of these three dimensions led us to create five mutually exclusive indicators in which people could have been in each year of their lives: “inactive,” “full-time formal employment,” “part-time formal employment,” “full-time informal employment,” and “part-time informal employment.”
Dependent Variable: Oral Health
This study considered five indicators of oral health in old age. Firstly “oral pain,” which was measured with the question “In which parts of the body do you feel pain?” where one of the response options was “Mouth/Teeth.” The second variable is “visit to the dentist,” measured with the question “In the last twelve months, have you been to the dentist or to a dental hygienist?” The third variable is “postponement of dental visits,” measured with the question “In the last twelve months, have you postponed your visits to the dentist in order to reduce expenses?” Dental visits and postponement of dental consultations are considered in this research because they are key indicators that shed light on the possibility of access to oral healthcare.
The fourth variable considered is “out-of-pocket spending on oral health,” which was measured with the question “In the last twelve months, have you paid anything out of your own pocket for your oral health? Please consider spending on diagnostics, treatments and dental prosthetics.” Finally, the fifth variable is “amount of out-of-pocket spending on oral health,” which was measured with the question “How much have you spent out of your own pocket on your oral health each month on average in the last twelve months (i.e., expenses that have not been reimbursed by your health coverage)?” The values for this variable were recoded as “less than 50,000 Chilean pesos” and “50,000 Chilean pesos or more” (equivalent to approximately 65 US dollars). The presence and amount of out-of-pocket healthcare spending is a widely used measure to assess the performance of healthcare systems with respect to the financial protection they provide. In Chile, out-of-pocket spending represents 33.0% of people’s total health expenditure, where a significant part is typically spent on dental attention, which means that the country ranks fifth (highest) among the nations integrated in the Organisation for Economic Co-operation and Development (OECD). As the literature suggests, the high proportion of out-of-pocket spending disproportionately affects people with lower social status, which include older people (Organisation for Economic Co-operation and Development (OECD), 2018).
Control Variables: Sociodemographic and Health Risk Factors
The association between the independent and the dependent variables were adjusted by different factors that typically have an impact on people’s oral health. First, we considered four sociodemographic variables: age, gender (“women,” and “men”), educational level (“primary or none,” and “secondary or higher”), and type of health coverage (“public,” and “private”). Second, we included the following three health risk behavior factors: body mass index (“not obese, ” and “obese”), smoking (“presence,” and “absence”), and alcohol consumption during the last 7 days (“presence,” and “absence”).
Statistical Analysis
There were two stages to our analytical approach. First, we used weighted sequence analysis (SA) to identify different types of employment trajectories over the life course. SA is a longitudinal statistical technique, the main objective of which is to identify representative types of trajectories (in this case employment trajectories) in a population (MacIndoe & Abbott, 2004). To this purpose, first, this tool allows creating a dataset of individual sequences of employment statuses (i.e., any of the five mutually exclusive statuses mentioned above) chronologically experienced by each respondent from birth to the age at the time of the interview in 2019, on a yearly basis.
Then, this technique allows identifying the similarities and differences between every pair of individual employment sequences, which in technical terms is called “distance.” The distance specifically refers to a value that summarizes the modifications needed to convert one individual’s sequence into another. Modifications can be either substitution, insertion, or deletion of statuses composing individual sequences. There are different metrics to calculate distances, for example, optimal matching analysis, hamming distance, dynamic hamming distances, among others. In this study, we used optimal matching analysis metric, which measures distances between individual sequences regarding the minimal number of modifications of statuses for them to become equal (Elzinga, 2007). When using any of these metrics, for each substitution, insertion, and deletion operation between statuses, a cost is attributed. Following the standard recommendations in the field, we set a constant substitution cost equal to two and a constant insertion/deletion cost equal to one, and we used individual’s weights in the calculation of the distance metric (MacIndoe & Abbott, 2004).
Next, the distance between all pair of individual sequences results in a “distance matrix.” Over the distance matrix, we performed a cluster analysis to group similar individual sequences (i.e., with no or low distances between them) into different aggregated trajectory types. To the latter, we used the Ward’s (1963) hierarchical clustering algorithm and four statistical criteria to select the most robust and representative number of employment trajectory types (see Figure 1). Cluster cut-off criteria. Note: In this study, we use Ward’s method to cluster individual trajectories into different types, and four statistical criteria to select the most robust and representative number of employment trajectory types: Average Silhouette Width (ASW), Point Biserial Correlation (PBC), Hubert’ s Gamma (HG), and Hubert’s C (HC). To evaluate these criteria, we use normalized scores since some of them have an index that ranges from −1 to 1, while others from 0 to 1. In addition, while a higher measure in the ASW, PBC and HG indices indicates a better cluster solution, a lower measure in HC indicates a better solution.
Weighted Characteristics of the Sample.
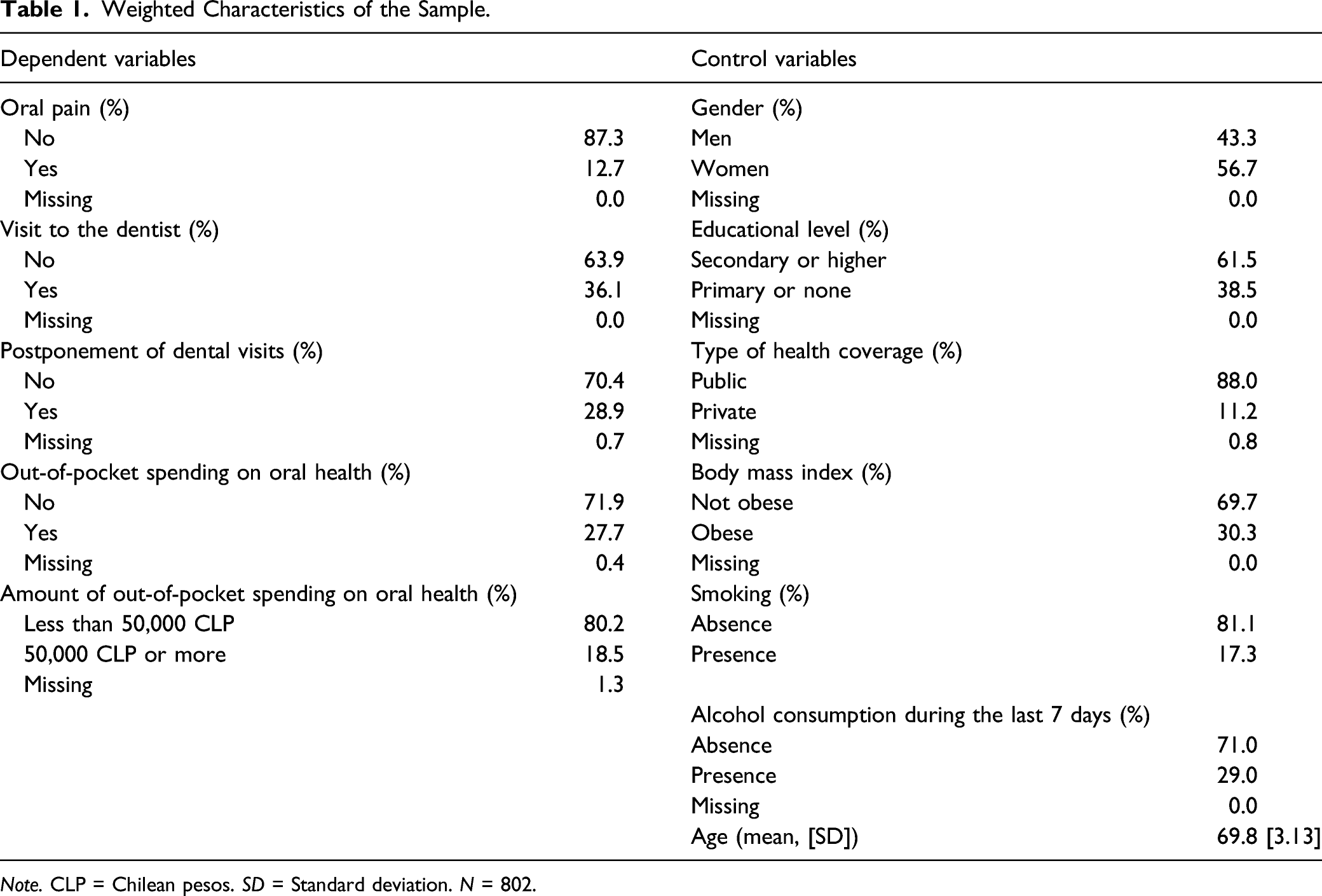
Note. CLP = Chilean pesos. SD = Standard deviation. N = 802.
We used the statistical software package “R” for all our analyses, specifically the packages TraMineR (Gabadinho et al., 2011) and WeightedCluster (Studer, 2013) for weighted sequence analysis, and survey (Lumley, 2011) to work with weighted datasets.
Results
Sample Characteristics
Table 1 shows the weighted distribution of dependent and control variables. As seen, women constituted 56.7% of the sample and men 43.3%. In terms of education, 38.5% of the participants had primary or no education, while 61.5% had secondary education or higher. In terms of health coverage, 11.2% had private coverage and 88.0% had public coverage. Some 30.3% of the sample reported obesity, 17.3% reported smoking, and 29.0% reported consuming alcohol at least once during the last 7 days. With respect to the five dependent variables used, 12.7% reported having oral pain, 36.1% stated they had visited the dentist during the last year, 28.9% said they had postponed a visit to the dentist to reduce expenses, 27.7% had made out-of-pocket spending for oral health, and 18.5% stated that they had spent 50,000 Chilean pesos or more on oral health during the last year.
Employment Trajectories
In Figure 1, we can see that the statistical criteria indicate that between four and seven are appropriate numbers of trajectory types to represent the diversity of employment patterns followed by the older individuals studied (all coefficients of the statistical criteria visibly worsen from eight types onwards). However, after analyzing the different solutions of trajectories, we noticed that the four-, five-, and six-type solutions did not provide enough information on all the key employment patterns among the study sample; thus, minimizing meaningful heterogeneity between trajectories. Therefore, we decided to select the seven-type solution as the optimal choice as it maximizes interpretability of the diversity of employment trajectories.
Figure 2 shows the seven types of employment trajectories in two types of plots: individual sequences and chronogram plots. On the left of Figure 2, we see the names and weighted proportions of each type of employment trajectory, and on the right, the employment statuses used to reconstruct these trajectories with different colors. In the chronogram graph, the x-axis represents the age of individuals, and the y-axis represents the proportion (0 to 1) of individuals in different types of employment statuses over time. In the graph of individual sequences, the x-axis also indicates the age, but the y-axis shows the specific trajectory of each individual classified in a trajectory type (i.e., there are as many lines as there are people classified in each type). Finally, the types are ordered from highest to lowest prevalence. Seven types of weighted employment trajectories.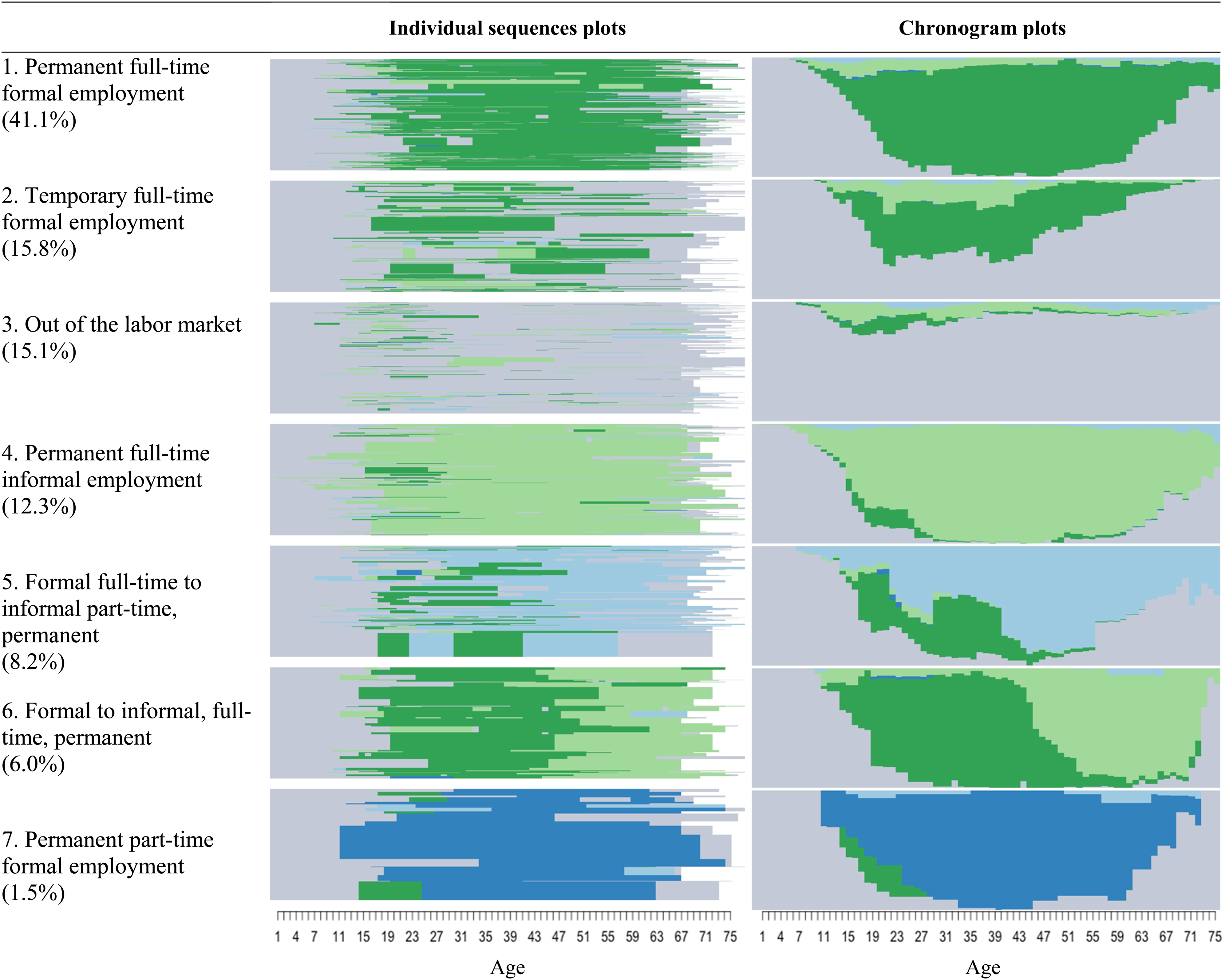
The first type, called “1. Permanent full-time formal employment” (41.1%), is the most frequent trajectory and it groups individuals who remained in formal, full-time jobs continuously through adulthood, contributing to social security. The second type is entitled “2. Temporary full-time formal employment” (15.8%) and includes individuals who also participate in full-time formal jobs, but only for brief periods in adulthood, as most of the time they are out of the labor market. The third type of trajectory, entitled “3. Out of the labor market” (15.1%), groups individuals who have spent most of their lives either inactive or not in paid employment. The fourth type is called “4. Permanent full-time informal employment” (12.3%) and it includes individuals who have been permanently active and working full time, but informally, that is, not contributing to social security.
The fifth type, entitled “5. Formal full-time to informal part-time, permanent” (8.2%), represents people who worked in full-time formal jobs during their early adulthood (18–30 years), but after this stage transitioned to part-time informal employment and remained there most of their lives. The sixth type is called “6. Formal to informal, full-time, permanent” (6.0%) and includes people who remained in full-time formal employment on a stable basis up to around 45 years of age, but after that transitioned to full-time informal employment and remained there until late in life. Finally, the seventh type, called “7. Permanent part-time formal employment” (1.5%), is the least common trajectory and groups individuals who contributed to social security continuously from part-time jobs.
Employment Trajectories and Oral Health in Old Age
Weighted Logistic Regression Models (Odds Ratios).
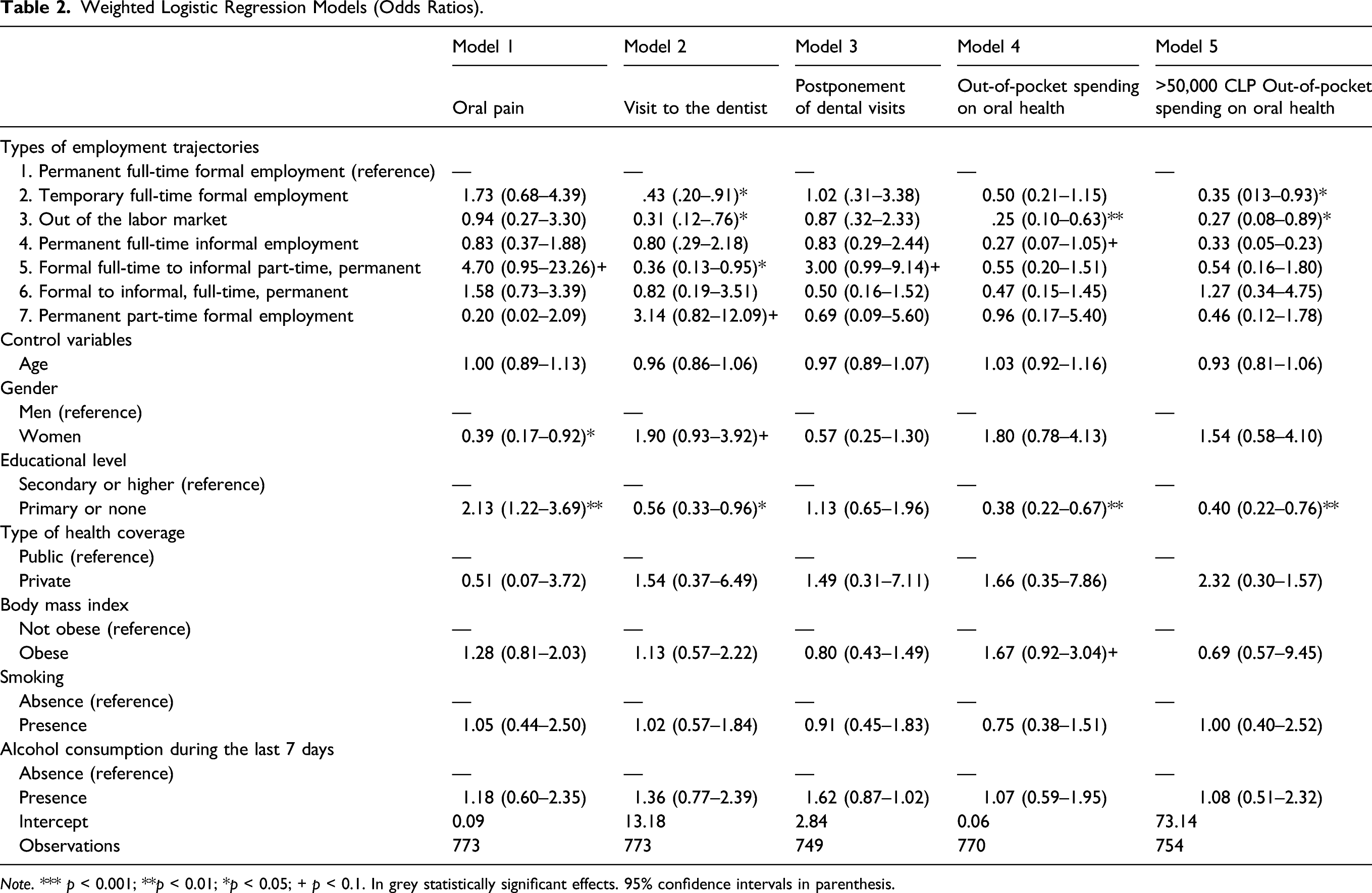
Note. *** p < 0.001; **p < 0.01; *p < 0.05; + p < 0.1. In grey statistically significant effects. 95% confidence intervals in parenthesis.
In Model 1, we can see that, in comparison with people who followed trajectory “1. Permanent full-time formal employment,” those who followed trajectory “5. Formal full-time to informal part-time, permanent” have almost four times the risk (OR = 4.70, p < .1) of suffering oral pain.
Then, in Model 2, we see that people who followed the trajectories “2. Temporary full-time formal employment” (OR = 0.43, p < .05), “3. Out of the labor market” (OR = 0.31, p < .05), and “5. Formal/informal, full-time/part-time, permanent” (OR = 0.36, p < .05) are less likely than individuals in the first trajectory type to have visited a dentist in the last year. In other words, individuals classified in trajectory “1. Permanent full-time formal employment,” are 1.32, 2.22, and 1.77 times more likely to have visited a dentist than those classified in trajectory types 2, 3, and 5, respectively. On the other hand, those classified in type “7. Permanent part-time formal employment” (OR = 3.14, p < .1) are 2.14 times more likely to have visited a dentist in the last year.
Model 3 shows that people classified in trajectory type “5. Formal full-time to informal part-time, permanent,” not only visit the dentist less often than those in trajectory type 1 (as shown in Model 2) but are also twice as likely (OR = 3.00, p < .1) to postpone these visits to reduce expenses.
In model 4, we first see that those who were classified in the employment trajectories “3. Out of the labor market” (OR = 0.25, p < .01) and “4. Permanent full-time informal employment” (OR = 0.27, p < .1) are less likely to make out-of-pocket spending on oral health than those in the first trajectory type. Likewise, Model 5 indicates that the individuals classified in trajectory type “2. Temporary full-time formal employment” (OR = 0.35, p < .05) and “3. Out of the labor market” (OR = 0.27, p < .05) show significantly lower chances of having oral health expenditure of more than 50,000 Chilean pesos than individuals who followed trajectory “1. Permanent full-time formal employment.”
Discussion
The results of this study indicate that, even when controlling for factors that typically affect oral health, life course employment trajectories have a significant association with oral health in old age. Specifically, trajectories characterized by continuous, formal, full-time employment corresponds to a protective factor for multiple oral health indicators for older persons. Also, we observed that for some specific oral health indicators like visits to the dentist, part-time work has a positive association but only when it is combined with uninterrupted and persistent job formality (trajectory type 7). This can be explained because one of the main incentives from the Chilean state for people to work in the formal sector is that regardless of their income level and the work-time basis (i.e., full- or part-time job), as long as workers contribute to social security, they have the right to access comprehensive public healthcare coverage, which is not guaranteed for informal workers. As a matter of fact, we noticed that part-time work combined with persistent job informality (trajectory type 5) led to increased risks of suffering oral pain in old age. This means that although informal work could allow people to increase their monthly income by avoiding social security contributions (a common practice in Chile [Madero-Cabib et al., 2019b]), this occurs at the expense of their health coverage across the life course.
These findings are highly consistent with previous cross-sectional studies which show that people who have access to stable employment have higher out-of-pocket expenditure on oral health services and consequently have better oral health; or, on the contrary, that working in temporary and informal employment, or being out of the labor market, has negative effects on oral health, which is explained by a lower use of oral healthcare services (Al-Sudani et al., 2017; Sato et al., 2018). However, this longitudinal study enables us to extend the previous results and to understand that individuals who participated actively and formally in the labor market during their lives may have accumulated material and socioeconomic advantages, as well as the continuous right to access comprehensive public healthcare coverage, that led them to have better oral health conditions in old age.
The growing proportion of older persons worldwide is leading governments to face an increased demand for health services and to cover high-cost diseases among this age group, such as oral pathologies (e.g., tooth loss, tooth decay, periodontal disease, and oral cancer). Our results also demonstrate the need for public policies on oral health to incorporate a life course approach and to consider, among other factors, the positive effect on oral health of being in continuous, formal, full-time employment throughout life. We recommend promoting public policies that seek to prevent and mitigate in advance the negative impact on oral health in old age of being constantly employed in informal jobs or remaining out of the labor market permanently.
This is particularly relevant in countries such as Chile where temporary and informal employment has risen steadily, leading to increasing precarity of labor conditions, economic vulnerability, and lack of social protection in later stages of life (Madero-Cabib & Biehl, 2021; Madero-Cabib & Cabello-Hutt, 2021). If to this context we add the absence of comprehensive public health programs aimed at facilitating access to oral health treatment and prevention among older persons (Ministerio de Desarrollo Social, 2013), the result is the presence of disproportionately negative effects particularly for those individuals who have accumulated socioeconomic disadvantages during their lifetime and are heavily dependent on public benefits to address oral health problems.
Limitations
This study has limitations that are important to acknowledge when interpreting results. First, the relationship between employment and oral health is not direct, but instead it is explained by characteristics that people who are active in the labor market tend to exhibit, such as better oral health conditions, better oral hygiene, greater access to dental care services, and less tooth loss (Al-Sudani et al., 2016, 2017; Sato et al., 2018). However, none of these characteristics referring to oral hygiene practices were measured in this research. Second, although the life course calendar used in this study was structured to address the three main mechanisms involved in the retrospective exercise of memory, it is important to acknowledge that this type of retrospective questionnaire involves multiple challenges of the autobiographical memory process, which might affect the accuracy of the study findings. And third, we collected our study sample in Chile’s capital and most populated city, Santiago, which is an urban area and therefore limits representativeness of individuals living in rural geographical areas of the country.
Conclusion
This study provides innovative and significant evidence to enable better understanding of the phenomenon of the oral health among older people, who represent an increasing proportion of the population of developing countries in Latin America and other regions of the world. Specifically, our research contributes to better understanding of the types of employment trajectories that are associated with increased risks for oral health in old age. Future research should explore the impacts on the oral health of older persons from life trajectories in other barely explored domains, such as parental, marital, and co-residence trajectories with different family members.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research has been supported by the following grants of the Agencia Nacional de Investigación y Desarrollo (ANID): -ANID/FONDECYT/INICIACION/N°11180360-ANID/FONDAP/Nº15130009-ANID/Millennium Science Initiative/Grant NCS17_062. “Millennium Nucleus for the Study of the Life Course and Vulnerability (MLIV)”
Ethical Approval
This research project has been approved by the Ethics Committee of the Faculty of Social Sciences at Pontificia Universidad Católica de Chile (institutional review board [IRB] approval number: 190124005), which conforms to the provisions of the Declaration of Helsinki, the Declaration of Singapore, and the Nuremberg Code.
Informed Consent
All participants in this research signed informed consent.
Ethical Approval
This research project has been approved by the Ethics Committee of the Faculty of Social Sciences at Pontificia Universidad Católica de Chile (institutional review board [IRB] approval number: 190124005), which conforms to the provisions of the Declaration of Helsinki, the Declaration of Singapore, and the Nuremberg Code.
Informed Consent
All participants in this research signed informed consent.