
Abstract
Objectives:
To analyze prefrailty’s relationship with limitations in activities of daily living (ADLs) and restrictions in social participation.
Method:
Robust (Fried 0/4; n = 214; Mage = 82.3 years [SD ±2.1]) and prefrail (Fried 1–2/4; n = 191; Mage = 83.8 years [SD ±3.2]) community-dwelling older individuals were included. Frailty scores were obtained from weight loss, exhaustion, gait speed, and grip strength. A total disability index (DI) expressed dependency for basic (b-), instrumental (i-), and advanced (a-)ADLs. Total participation score, being a member, total number of memberships, being a board member, level of participation, membership over time, volunteering, and formal participation represented social participation.
Results:
Logistic regression retained age (OR = 1.224; 95% CI = [1.122, 1.335]), sex (OR = 3.818; 95% CI = [2.437, 5.982]), and a-ADL-DI (OR = 1.230; 95% CI = [1.018, 1.486]) as variables significantly related to prefrailty (68.3%; χ2 = 68.25; df = 3; p < .001).
Discussion:
Subtle limitations in a-ADLs, higher age, and being a man were associated with prefrailty, revealing the possible role of personal and culturally related a-ADLs as red flags for (pre)frailty.
Introduction
Activities and participation are well-known benefits for quality of life in older individuals (Goldberg et al., 2002). The World Health Organization (WHO) promotes active aging in its broadest sense (e.g., physical, social, and functional aspects) by emphasizing the process of optimizing opportunities for health, participation, and security to enhance quality of life as people age and to prevent frailty (WHO, 2015). There is growing evidence that engagement in activities and participation are favorable for the postponement of frailty and morbidity (Fastame et al., 2018; Griep et al., 2017; Huang, 2019). For instance, as an illustration, community-dwelling older persons volunteering in later life showed protection against dementia (Griep et al., 2017), and participation in leisure activity positively influenced the symptoms of depression and well-being (Fastame et al., 2018). According to Huang (2019), active volunteering enhances productive aging by increasing well-being. On top of that, it seems that engagement in social (e.g., playing cards), performance-oriented (e.g., voluntary group), or togetherness-oriented activities (e.g., leisure activities) (Haak et al., 2019; Rizzuto et al., 2012) may lower or influence the risk of mortality among community-dwelling older adults.
Despite the societal emphasis on active aging, not all people grow old in an optimal way, and some become vulnerable and frail. With the aging society, an increasing number of chronic conditions, and multimorbidity, the prevalence of frailty ranges from 5% to 58% in community-dwelling older adults depending on the measurement tool used (Ntanasi et al., 2020; Sternberg et al., 2011). Frailty is a condition or syndrome which results from a multisystem reduction in reserve capacity to the extent that a number of physiological systems are close to, or pass, the threshold of symptomatic clinical failure (Campbell & Buchner, 1997). Screening for frailty is advisable; however, it is a big challenge due to the lack of screening implementations (Walston et al., 2018) and guidance on interventions (Travers et al., 2019). Research is required to develop more efficient screening and intervention methods (Clegg et al., 2013). Frailty is a dynamic state that can revert to robustness, though this is more common in its early stage, the so-called prefrail state (Travers et al., 2019). It is a rather complex state that is influenced by depression (Dos Santos Tavares et al., 2017), exhaustion (Knoop et al., 2019), balance, hearing, low body mass index, living alone, anxiety, and so on (S. J. Gordon et al., 2020). However, to date, little research has been performed on prefrail community-dwelling older adults. To target the negative outcomes of the frailty syndrome properly, it is pivotal to investigate its early determinants. Moreover, older persons are often described and examined as 65 years old and over (Mello et al., 2014), which causes a gap in knowledge of octogenarians, the fastest growing population group. The prevalence of (pre)frailty is more likely in persons aged 80 years and above than in a relatively young age group (Ntanasi et al., 2020), as age is strongly associated with frailty (Mello et al., 2014).
The relationship between limitations in the activities of daily living (ADLs), restrictions in social participation, and (pre)frailty remains ambiguous. First, significant associations have been found between participation restriction and the degree of frailty (J. Y. Liu, 2017), and perceived satisfaction of social participation is associated with lower frailty scores (Kwan et al., 2019). Furthermore, social participation is seen as a protective factor against developing frailty (Hsu & Chang, 2015). Moreover, participants who had not participated in, for example, sports or voluntary work in the last month showed an increased risk of worsening frailty (Etman et al., 2015). However, social participation is rarely involved in proposed frailty interventions (Travers et al., 2019).
Second, frailty is related to limitations in ADLs. ADLs comprise the total package of a person’s everyday activities which allow them to live autonomously and to be integrated in the environment, fulfilling a determined social role (Devi, 2018). Three categories of ADL can be distinguished according to their difficulty and complexity: basic (b-), instrumental (i-), and advanced (a-)ADLs. b-ADLs, such as bathing, are basic physiological and self-maintenance needs necessary to stay alive (Katz et al., 1963). Frailty significantly increases the risk for dependencies in b-ADLs (H. X. Liu et al., 2019), and limitations in b-ADLs increase the odds of being (pre)frail in rural older individuals (Manrique-Espinoza et al., 2016). i-ADLs, needed to live independently, require more high-level skills, such as shopping (Lawton & Brody, 1969), and the risk of limitations is increased when frailty occurs (H. X. Liu et al., 2019). Some studies have indicated the occurrence of limitations in i-ADLs as a predictor and/or characteristic of prefrailty in a new functional classification (Hoogendijk et al., 2019). The most complex activities, a-ADLs, such as hobbies, are unique and specific to each individual, and are influenced by cultural and motivational factors (De Vriendt et al., 2012). Research on the relationship between frailty and a-ADLs is scarce. One study showed that limitations in a-ADLs (e.g., driving), significantly predicted worsened frailty (Alencar et al., 2015).
In conclusion, many studies indicate that engagement in activities and participation could maintain active aging and quality of life. Subsequently, early restrictions in social participation and subtle limitations in daily activities could be early detectors and/or indicators for frailty, although this relationship must be scrutinized initially. Therefore, the aim of this study is to analyze the relationship of prefrailty with limitations in ADLs and restrictions in social participation. This will improve understanding of the relationship, early identification, and, in the future, the prevention of (pre)frailty and its negative health outcomes, such as early mortality, supporting policymakers in developing preventive policies to preserve active aging.
Materials and Method
Study Design
Cross-sectional data from the BUTTERFLY study were analyzed. The BUTTERFLY is a large study of the Gerontopole Brussels consortium directed by the Frailty in Ageing and Belgian Ageing studies research groups of the Vrije Universiteit Brussel (Belgium). The ethical committee of UZ Brussel (B.U.N. 143201421976) gave approval and all participants provided informed consent. All data were collected by a team of researchers with different backgrounds (medical, gerontological, etc.). Recruitment of the study volunteers was through advertisements in day centers, health insurance companies, seniors associations, general practitioners, municipalities, and word of mouth.
A sample of 494 participants was necessary to obtain a minimum of 405 eligible community-dwelling octogenarians, who participated between February 2015 and June 2019. Participants were eligible when they were as follows:
Older individuals aged 80 years and above.
Living independently.
Able to walk (including technical or personal assistance).
Without cognitive disabilities (not unable to understand the test instructions and/or Mini-Mental State Examination [MMSE] ≥ 23/30) (Folstein et al., 1975).
Not diagnosed with cancer within the previous 6 months, and without recent surgery, radiotherapy, and/or chemotherapy.
Not frail—Groningen Frailty Indicator < 4/15 (Steverink et al., 2001), Rockwood Frailty Index < 0.25/10 (Collerton et al., 2012)—and/or the Fried Frailty Phenotype < 3/4.
Similar to Cao Dinh et al. (2018), our approach was based on four frailty characteristics suggested in previous research: weight loss, exhaustion, gait speed, and grip strength (Buchman et al., 2011; Ostir et al., 2004). First, exhaustion was measured according to the original Fried phenotype assessing two questions from the Center for Epidemiological Studies–Depression (CES-D) Scale (Orme et al., 1986) translated into Dutch or French: “How often in the last week did you feel this way?” (1) “I felt that everything I did was an effort” and (2) “I could not get going.” Participants could answer the questions with “rarely or none of the time” (0); “some or a little of the time” (1); “a moderate amount of time” (2); or “most of the time” (3). When participants obtained a score of 2 (a moderate amount of time) or 3 (most of the time) on either of the two questions, one point was granted for the criterion “exhaustion.”
Second, weight loss was evaluated through the self-reported question: “In the last six months, have you lost more than 4.5 kg unintentionally?” which was answered by “yes” (1) or “no” (0). Next, the criterion “gait speed” was assessed using a sex and height stratified timing of a 4.5-m walking distance (Fried et al., 2001). Participants were scored 1 point if their walking time exceeded or was equal to 7 s for men ≤173 cm and women ≤159 cm, and if their time exceeded or was equal to 6 s for men >173 cm and women >159 cm. Finally, grip strength was assessed using the Martin Vigorimeter (Sipers et al., 2016). The cut-off values were ≥71 kPa for men and ≥ 42 kPa for women. Participants who scored lower than the aforementioned values received 1 point. Two groups were identified: a score of 0 indicated robustness, and 1 or 2 signified prefrailty based on previous research (Sirola et al., 2011).
Evaluation of Daily Functioning
Based on the International Classification of Functioning, Disability and Health (WHO, 2001), daily functioning was assessed with the b-ADL, i-ADL (Cornelis et al., 2017), and the shortened version of the a-ADL tool (De Vriendt et al., 2013), together known as “the Brussels Integrated Activities of Daily Living Inventory (BIA).” Six activities were evaluated for the b-ADLs, nine for the i-ADLs, and, at the level of a-ADLs, 15 clusters of activities. The performance of ADLs (what someone actually does) was measured. First, each activity from b-, i-, and a-ADLs was reviewed for relevance by asking participants whether they had performed the activity during the past 10 years. If this was not the case, that activity was not taken into account for further evaluation. If the activity was relevant, participants were asked how the activity was performed. Based on the narratives of the participants, the researcher assigned a score according to a five-point scale ranging from 0 (no difficulty to perform) to 4 (unable to perform), to weigh the quality of the activity’s performance. Through this evaluation of daily functioning, a calculation could be made representing a global disability index (DI) for each ADL level (b-, i-, and a-ADL), expressed as percentages, where higher percentages indicated more limitations (Cornelis et al., 2017).
Evaluation of Social Participation
Social participation was assessed using a structured self-report questionnaire (De Donder et al., 2014). Two questions were asked: if participants held membership of a social organization and if they volunteered.
For the variable “membership,” participants were asked whether they were not a member (1), a former member (2), a current member (3), or a board member (4) of 20 possible social associations or clubs, ranging from environmental organizations to hobby and sports clubs. A total participation score was calculated from a total score of 80, where 20 represented no participation and 80 maximal participation, as the participants could indicate a score ranging from 1 to 4 on 20 options. Second, all items were dichotomized (current and board member, and no and former member). A second variable resulted in being a member of at least one association (1) or not being a member at all (0). Next, each participant’s total number of memberships was counted. These were then dichotomized into the level of social participation (≤3 low or >3 high) according to Lindstrom et al. (2003). Subsequently, a differentiation was made between being a board member in ≥1 organization (1) and not being a board member in any organization (0). Finally, a person’s membership over time was calculated from the overall possible memberships: never having been a member (not a former member and not a member at the moment, 0), having always been a member (a former member and a member at the moment, 1), not a member anymore (a former member and not a member at the moment, 2), and having become a member (not a former member and a member at the moment, 3). For the variable “volunteering,” participants were asked to indicate if and in which of 10 types of voluntary work they participated—for example, recreational, keeping company, and sociocultural. When at least one item was specified, they were classified as volunteers (1) (De Donder et al., 2014).
Finally, the two variables “being a member” and “volunteering” were combined into a new variable, “formal participation” (Buffel et al., 2014), where higher scores represented more participation, the maximum score being 30.
Characteristics
The following data were also collected: sex (man, woman); age (years); education (primary, lower-secondary, upper-secondary, post-secondary-level) (Schneider, 2013); MMSE score (Folstein et al., 1975); Geriatric Depression Scale (Yesavage et al., 1982); self-reported number of medications; self-reported number of comorbidities, counting categories retrieved from Collerton et al. (2012): hypertension, ischemic heart disease, cerebrovascular disease, peripheral vascular disease, heart failure, cancer within previous 5 years, chronic lung disease, chronic joint disease, osteoporosis, diabetes mellitus, thyroid disease, Parkinson’s disease, dementia, eye disease, visual impairment, and hearing impairment; and living circumstances (living together, living alone).
Statistics
A two-staged analysis was performed using IBM SPSS version 26. First, descriptive statistics were presented by percentages and frequencies for categorical variables and means with standard deviation for continuous variables. For the characteristics limitations in ADLs and restrictions in social participation, differences between robust and prefrail participants were evaluated by the χ2 test for categorical variables, and by independent sample t-test for continuous variables. When cells did not contain enough variables, Fisher’s exact tests were performed for categorical variables. Analyses were conducted for sex separately. In addition, a binary logistic regression analysis using the forward likelihood method was carried out to determine which variables were related to prefrailty. Variables that did not show multicollinearity problems (≤r = 0.80) were included. For ADLs, an increment of 10% in ADL limitations was used.
Results
Characteristics
A total of 494 octogenarians volunteered to participate in the study (ranging from 80 to 97 years; 83.0 ± 2.8). After excluding participants with cognitive disabilities (n = 9), missing tests (n = 4), and frailty (n = 76), the final sample consisted of 405 participants (Figure 1).
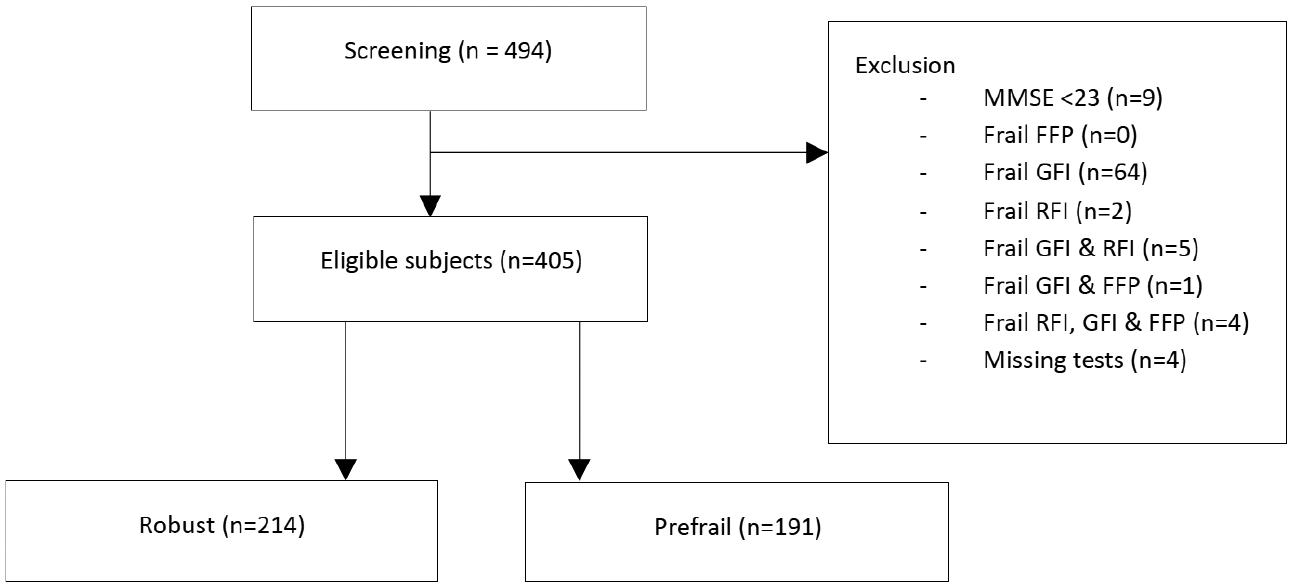
Flowchart.
As Table 1 shows, 214 participants were robust: 91 men and 123 women (Mage = 82.3 ± 2.1 years). The mean age of the prefrail participants (n = 191) was 83.8 ± 3.2 years, with a predominance of men (71.2%). Only sex and age significantly differed between robust and prefrail participants (p < .001). Within men, significantly more robust participants were living with someone compared with prefrail participants (%robust men living together = 76.9; %prefrail men living together = 66.2; p = .03). Prefrail women were significantly older (p < .001) and were taking more medication (p < .05) than the robust women.
Characteristics.

Note. χ2 for categorical variables (when cells did not contain enough variables, Fisher’s exact tests were performed) and independent samples t-test for continuous variables. Bold: significant p-value < .05. M = mean; SD = standard deviation; MMSE = mini-mental state examination; GDS = geriatric depression scale.
Two missing values. bThree missing values.
Participation and ADLs
Table 2 shows the differences between robust and prefrail participants regarding social participation and ADLs. In terms of social participation, there were no significant differences between groups and sexes (Table 2).
Differences Between Robust and Prefrail Participants in Participation and ADLS.
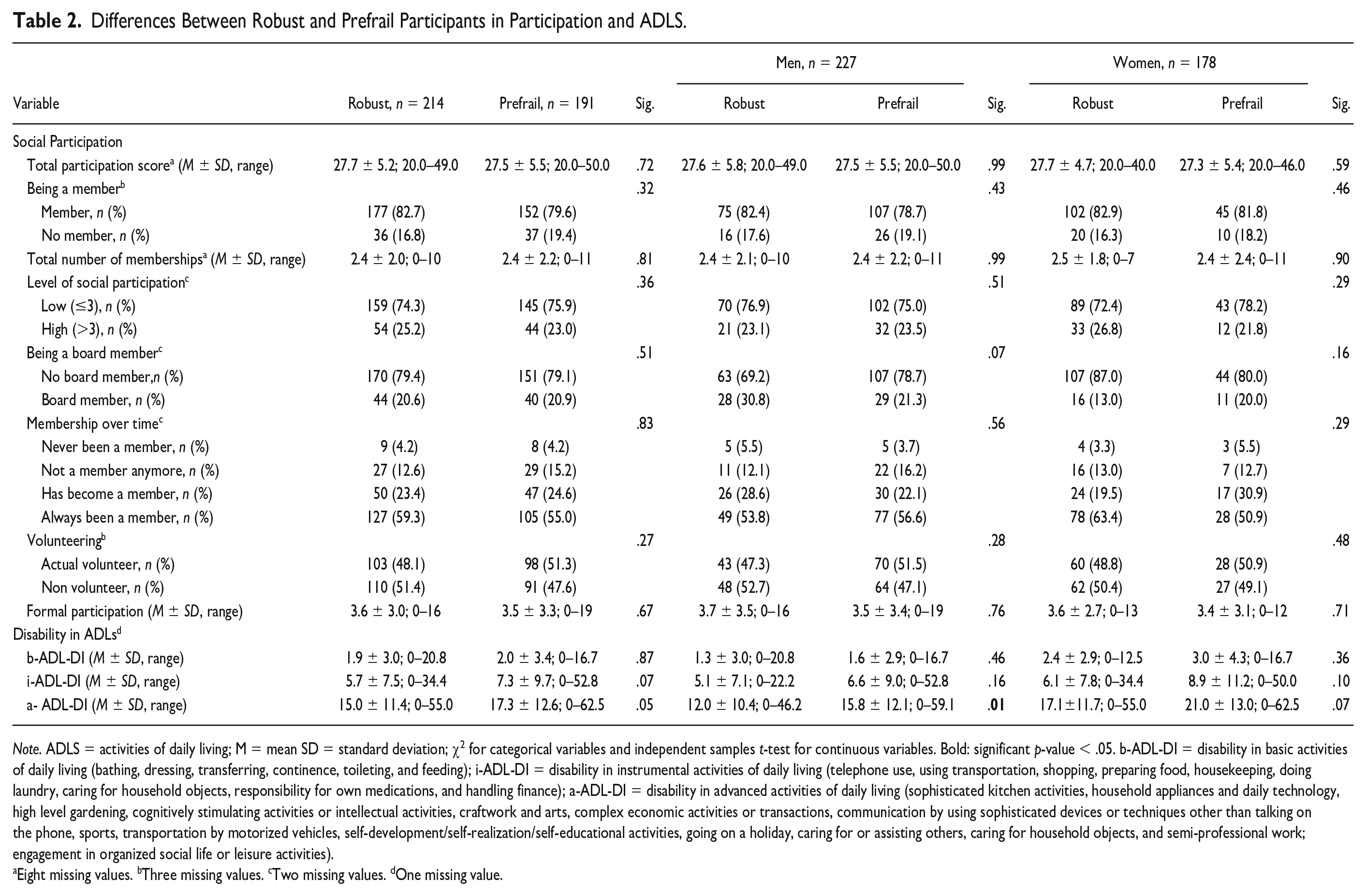
Note. ADLS = activities of daily living; M = mean SD = standard deviation; χ2 for categorical variables and independent samples t-test for continuous variables. Bold: significant p-value < .05. b-ADL-DI = disability in basic activities of daily living (bathing, dressing, transferring, continence, toileting, and feeding); i-ADL-DI = disability in instrumental activities of daily living (telephone use, using transportation, shopping, preparing food, housekeeping, doing laundry, caring for household objects, responsibility for own medications, and handling finance); a-ADL-DI = disability in advanced activities of daily living (sophisticated kitchen activities, household appliances and daily technology, high level gardening, cognitively stimulating activities or intellectual activities, craftwork and arts, complex economic activities or transactions, communication by using sophisticated devices or techniques other than talking on the phone, sports, transportation by motorized vehicles, self-development/self-realization/self-educational activities, going on a holiday, caring for or assisting others, caring for household objects, and semi-professional work; engagement in organized social life or leisure activities).
Eight missing values. bThree missing values. cTwo missing values. dOne missing value.
In terms of ADLs, a-ADL-DI showed more deficits for prefrail than for robust participants (p = .05). At the b- and i-ADL-DI levels, no differences were found between groups. When taking sex into account, prefrail men scored significantly higher on a-ADL-DI (p = .01) than robust men.
Logistic Regression
Sex, age, education, MMSE, medication, comorbidities, living together, formal participation, being a member, level of social participation, being a board member, membership over time, volunteering, b-, i-, and a-ADL-DI, were put into the analysis. Due to multicollinearity problems with formal participation, the total social participation score and the total number of memberships were not inserted. Binary logistic regression (χ2 = 68.250; df = 3; p < .001) indicated that age (odds ratio [OR] = 1.224; 95% CI = [1.122, 1.335]), sex (OR = 3.818; 95% CI = [2.437, 5.982]), and a-ADL-DI (OR = 1.230; 95% CI = [1.018, 1.486]) have a relationship with prefrailty, giving an overall correct prediction rate of 68.3% (Table 3). An increased age shows an increased likelihood of being prefrail. Likewise, men are nearly four times as likely as women to be prefrail, and a 10% in a-ADL-DI increases the odds of being associated with prefrailty by 23.0%.
Logistic Regression Relating Prefrailty/Robustness.
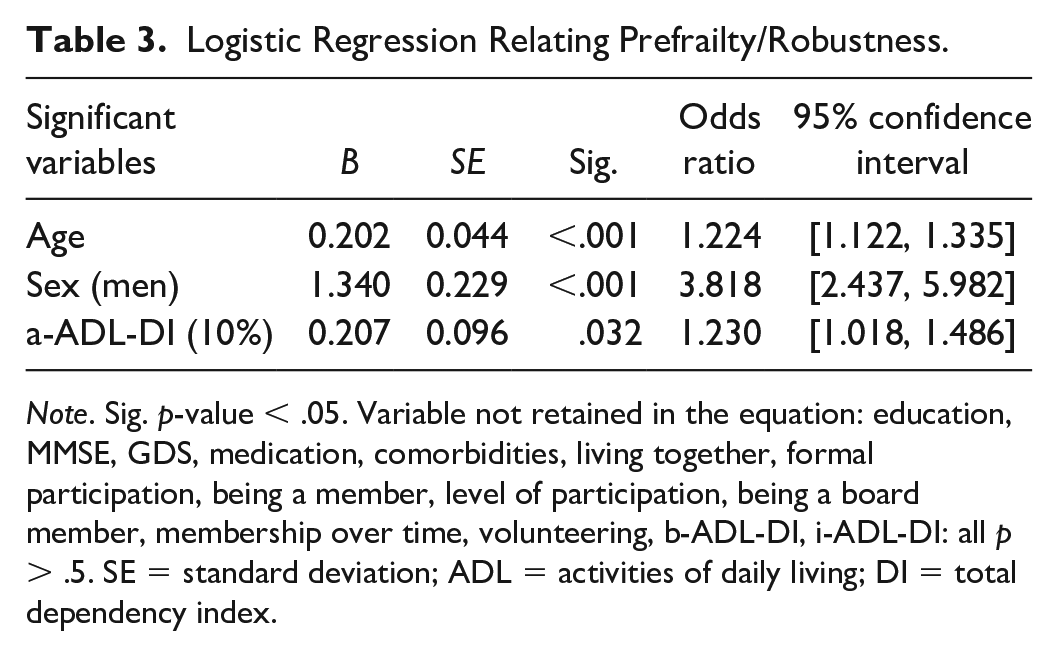
Note. Sig. p-value < .05. Variable not retained in the equation: education, MMSE, GDS, medication, comorbidities, living together, formal participation, being a member, level of participation, being a board member, membership over time, volunteering, b-ADL-DI, i-ADL-DI: all p > .5. SE = standard deviation; ADL = activities of daily living; DI = total dependency index.
Discussion
This study aimed to analyze prefrailty’s relationship with limitations in ADLs and restrictions in social participation. Results indicated that restrictions in social participation were not related to prefrailty, while mild subtle limitations in a-ADLs were. Altogether, in community-dwelling octogenarians, a 10% increase in limitations of a-ADLs (OR = 1.230), combined with higher age (OR = 1.224), and being a man (OR = 3.818), was related to prefrailty with a total accuracy rate of 68.3%.
As far as the authors know, this is the first study investigating activities according to the typology of b-, i-, and a-ADLs and social participation in the same large sample of robust and prefrail octogenarians.
In this sample, 405 older individuals showed no dependency for b-ADLs, while mild dependency occurred for i- and a-ADLs. Although mild and subtle, the a-ADL limitations significantly differed between robust and prefrail men. As shown in the logistic regression analysis, these differences, combined with age and sex, were related to prefrailty. Those findings might act as a first step in the clarification of the complex relationship between frailty and ADLs. This is important since this relationship is highly controversial. Some have stated that ADLs are negative health outcomes (H. X. Liu et al., 2019); others have considered them as predictors (Alencar et al., 2015; Ottenbacher et al., 2006) or characteristics of frailty. Indeed, ADL items (b-, i-, and a- ADLs) are included in more than half of the known frailty measurements (Costenoble et al., 2019).
A key strength of this study was that a-ADLs were also investigated, while other studies have only focused on b- and i-ADLs (Kojima, 2017), and this might help in the clarification. Hoogendijk et al. (2019) presented a model of functional decline in frailty, with limitations in b-ADLs as outcomes of frailty and limitations in i-ADLs as characteristics of prefrailty. We did not find any differences in i-ADLs between prefrail and robust participants, while significant differences were found for a-ADLs. Therefore, based on our findings (with some caution, due to the study’s cross-sectional design), it is hypothesized that limitations in a-ADLs might be predictors of (pre)frailty, and i-ADLs characteristics and b-ADLs negative health outcomes of frailty. This might complete the functional continuum in which a-ADLs are the most sensitive to decline, followed by limitations in i-ADLs and then b-ADLs. As b-ADLs are required for survival, they remain intact the longest (Morris et al., 2013; Reuben & Solomon, 1989). However, this suggestion is only based on the results of this cross-sectional study, which limits the interpretation of the findings, as prefrailty is an unstable condition and reverse causation cannot be excluded. This hypothesis must therefore be investigated longitudinally.
Nevertheless, based on the findings, it might be advisable to evaluate someone’s daily activities and, more specifically, their a-ADLs. As a-ADLs are highly individual personal activities strongly influenced by culture and personal decisions, they are difficult to evaluate and, as far as is known, few tools exist to measure daily functioning in a person-centered approach. However, evaluated in a valid and reliable way, as with the a-ADL tool (De Vriendt et al., 2013), a-ADLs might help to identify older persons at risk for frailty. Research is still scarce: only one study has shown that limitations in a-ADLs—for example, driving—significantly predicts worsened frailty (Alencar et al., 2015).
Next to mild limitations in a-ADLs as the related variable, age and sex are two known influential factors for frailty (Mello et al., 2014). Although most literature refers to women as the risk group for developing higher frailty scores (Ofori-Asenso et al., 2019), this study pointed out that men and higher age were associated factors for prefrailty. There were significantly more men in the prefrail group than women, at 71.2%. Sex differences have already been found in frailty (Alexandre et al., 2018; Zhang et al., 2018). Women live longer but in poorer health, have higher frailty scores based on the frailty index, but tolerate frailty better, with lower mortality scores compared with men (E. H. Gordon et al., 2017). Women might become frail sooner, and as this study solely included persons aged 80 years and above, this might explain the results, as there could be more women in the frail group. In our model, sex (OR = 3.818) made a large contribution to the total accuracy rate (68.3%) implying that other variables in a multidimensional concept of frailty might also play a prominent role.
Furthermore, in the logistic regression analysis, restrictions in social participation were not retained for prefrailty and robustness. This was surprising because a relationship with the progression of frailty has already been shown (H. X. Liu et al., 2019), and engagement in participation has a proven preventive effect on frailty (Hsu & Chang, 2015; Seino et al., 2019). This might be explained by the fact that this study sample had a low degree of participation, where 75% of the participants had three or fewer association memberships, which is lower than the 46.6% found in 20- to 80-year-olds (Lindstrom et al., 2003).
A limitation of the study is that social participation was only measured by indicators (Buffel et al., 2014), mainly by measuring club participation to indicate the frequency of participation, which only serves as a red flag. It is advised to evaluate social participation much more in depth through subjective feelings, frequency of participation, and the environment where the participation takes place (Van de Velde et al., 2018). Duppen et al. (2019) even recommended including all social environment dimensions (e.g., social networks) for further research on frailty. Moreover, selection bias might have occurred due to the inclusion of a select group of possible socially engaged, non-frail, community-dwelling octogenarians, as they were all willing to participate in a study. Generalization of the findings must be done with caution, as this is a selective sample of robust/prefrail octogenarians with a coincidentally high educational level.
Conclusion
To conclude, as the results in this study showed that the occurrence of subtle limitations in a-ADLs were related to prefrailty, a new theoretical model might have emerged, building on the functional classification of Hoogendijk et al. (2019), adding subtle limitations in a-ADLs as possible predictors of (pre)frailty, combined with limitations in b-ADLs as outcomes of frailty and limitations in i-ADLs as characteristics of prefrailty. Although this model should be confirmed in other studies, it is already advised that frailty screening be supplemented with questions on daily activities, specifically the most complex ones such as hobbies, playing cards, and gardening. Prevention of ADLs is still in its infancy, and as yet no improvement in that area (e.g., i-ADLs confidence) has been found (Levy et al., 2020). However, with further research, a-ADLs might offer building blocks for the prevention of frailty by targeting and focusing on preserving daily activities in the form of a-ADLs to support and maintain active aging.
Footnotes
Authors’ Note
Members of the Gerontopole Brussels Study group: Ivan Bautmans (FRIA, VUB), ivan.bautmans@vub.be; Dominque Verté (Belgian Aging Studies BAST, VUB), dominique.verte@vub.be; Ingo Beyer (Geriatric Medicine department, UZ Brussel), ingo.beyer@uzbrussel.be; Mirko Petrovic (ReFrail, UGent), mirko.petrovic@ugent.be; Nico De Witte (Belgian Aging Studies BAST, VUB), nico.de.witte@vub.be; Tinie Kardol (Leerstoel Bevordering Active Aging, VUB), mjmkardol@hotmail.com; Gina Rossi (Clinical and Lifespan Psychology KLEP, VUB), grossi@vub.be; Peter Clarys (Physical Activity and Nutrition PANU, VUB), pclarys@vub.be; Aldo Scafoglieri (Experimental Anatomy EXAN, VUB), aldo.scafoglieri@vub.be; Eric Cattrysse (Experimental Anatomy EXAN, VUB), ecattrys@vub.be; Paul de Hert (Fundamental Rights and Constitutionalism Research group FRC, VUB), paul.de.hert@vub.be; and Bart Jansen (Department of Electronics and Informatics ETRO, VUB), bart.jansen@vub.be.
Author Contributions
A.C. contributed to writing (original draft), methodology, formal analysis, investigation, and visualization; V.K. contributed to investigation and writing (review and editing); A.D. contributed to investigation and writing (review and editing); S.V. contributed to investigation and writing (review and editing); R.V.A. contributed to investigation and writing (review and editing); G.R. contributed to supervision and writing (review and editing); C.S. contributed to investigation and writing (review and editing); K.D.B. contributed to investigation and writing (review & editing); I.B. contributed to conceptualization, funding acquisition, writing (review and editing), project administration, and supervision; D.V. contributed to conceptualization, funding acquisition, supervision, and writing (review and editing); E.G. contributed to supervision and writing (original draft, and review and editing), formal analysis, and visualization; P.D.V. contributed to supervision and writing (original draft, and review and editing), formal analysis, and visualization; on behalf of the Gerontopole Brussels Study Group.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partly funded by an “Interdisciplinary Research Program” grant (number IRP3) from the research council of the VUB.
Statement of Ethics
All subjects have given their written informed consent and the study protocol was approved by ethical committee of UZ Brussel (B.U.N. 143201421976).