
Abstract
The stress of family caregiving may affect many health-related variables, including sleep. We evaluated differences in self-reported sleep quality between incident caregivers and matched non-caregiving controls from a national population-based study. Caregivers and controls were identified in the Reasons for Geographic and Racial Differences in Stroke (REGARDS) study and matched on seven different demographic and health history factors. Caregivers reported significantly longer sleep onset latency than controls, before and after adjusting for covariates (ps < .05). No differences were found on measures of total sleep time or sleep efficiency. Among caregivers only, employed persons reported less total sleep time and number of care hours was
Introduction
Most of the day-to-day caregiving for older adults in the United States is provided by informal/family caregivers, and with the growing size of the older population, the number of caregivers for older adults is large. In 2016, the Committee on Family Caregiving for Older Adults of the National Academies of Sciences, Engineering, and Medicine estimated that there are about 18 million caregivers of older adults with limitations in health or mobility (Schulz & Eden, 2016). A 2020 survey by the AARP and National Alliance for Caregiving estimated that more than 50 million Americans provide unpaid care for adult family members or friends (AARP, 2020). The number of Americans who are 80 years or older is expected to rise from about 13 million in 2015 to about 35 million in 2050 (Redfoot et al., 2013). Therefore, the importance of studying caregivers and the impact of caregiving on their health is unmistakable.
Caregivers can experience high levels of stress, which may affect their physical and psychological health. Research has found that caregivers have higher rates of depression and anxiety compared to non-caregivers (Haley et al., 2020; Pinquart & Sörensen, 2003), greater physical, psychological, and financial burdens, have less time for other family members, and may be less likely to participate in preventive health activities (Collins & Swartz, 2011). Caregiving has also been associated with poor sleep, which in turn can affect quality of life and health generally (Groeger et al., 2014; Mather et al., 2020; McCoy & Strecker, 2011; Narang et al., 2012; Petrov et al., 2018; Spira et al., 2010; Tapp et al., 2017; Tempesta et al., 2015).
Numerous previous studies have compared the sleep of caregivers to non-caregivers. Fonareva and colleagues (2011) compared samples of caregivers for persons with dementia, with non-caregivers who were matched on age and sex and found that the dementia caregivers spent less time in more restful sleep stages and more time in less restful sleep stages than the non-caregivers (Fonareva et al., 2011). A small sample of female veteran caregivers was found to experience higher levels of stress-related sleep disturbances compared to non-caregivers (Song et al., 2020). Similarly, Rowe et al. (2008) found that a convenience sample of older dementia caregivers experienced shorter sleep times, took longer to fall asleep, and reported higher levels of fatigue compared to older non-caregivers, and Fekih-Romdhane et al. (2020) found that caregivers of patients with psychiatric disorders exhibited worse overall scores in the Pittsburgh Sleep Quality Index Scale (PSQI) than age and sex matched non-caregivers. Castro et al. (2009) found no differences between nine female caregivers and 34 non-caregiving women on multiple sleep characteristics, although an association was found between increased levels of depressive symptoms in the caregivers and longer sleep latency.
A recent meta-analysis of dementia caregiving studies found that caregivers got significantly less sleep than non-caregiving controls (Gao et al., 2019). However, all of the studies included in that meta-analysis and the other previous studies reviewed above consisted of comparisons of convenience samples of caregivers, usually identified in clinical settings, and non-caregiving controls, often consisting of healthy volunteers. Such clinical or convenience samples of caregivers are known to report greater behavioral and psychological problems than more representative population-based samples of caregivers (Pruchno et al., 2009), and healthy volunteers recruited through different enrollment methods than caregivers undoubtedly differ from the caregivers in many different ways (Roth et al., 2015).
The present study examined the relationship between caregiving, multiple self-report measures of sleep duration and quality, and demographic covariates, using a national, population-based sample of Black and White adult incident caregivers and matched controls. In addition, within the caregiver sample, we investigated potential predictors of sleep, including depressive symptoms, type of caregiving (e.g., dementia, physical disability, stroke, mental illness, and disabling sensory impairments), caregiver employment status, caregiver co-residence with the care-recipient, and caregiver demographics.
Design and Methods
Regards
The Reasons for Geographic and Racial Differences in Stroke (REGARDS) Study is a population-based study of a national sample of adults over age 45 in the US (Howard, V. J. et al. 2005). The objective of the study is to identify the causes for the high rate of stroke mortality among Black adults and residents of the Southern United States. The REGARDS study sample comprises 30,239 non-Hispanic Black and White adult participants, who were 45 or more years of age when enrolled from 2003 to 2007. The study deliberately oversampled Black adults and residents of the southern United States. The study design, sampling, enrollment, and follow-up procedures have been described in more detail previously (Howard, V. J. et al. 2005). Potential participants were initially sent a letter about the study and then contacted by telephone by trained interviewers. Once eligibility was determined and participants provided verbal consent, a computer-assisted telephone interview (CATI) was conducted to collect demographic, medical history, measures of quality of life, and stroke risk factors. About 4 weeks after the telephone interview, participants were visited in-home to obtain physical measurements (e.g., height and weight) and blood samples. Ongoing brief CATI interviews are carried out semi-annually to assess possible stroke events, and a second comprehensive telephone interview and in-home assessment were carried out between 2013 and 2015, approximately 9 years after the initial in-home visits (Howard, G. et al. 2017).
Caregiving Transitions Study
The Caregiving Transitions Study (CTS) is ancillary to the REGARDS study and examines the health effects of caregiving among the REGARDS participants who have transitioned into a caregiving role between their 1st and 2nd in-home visits. A detailed description of the design, sampling, and participant enrollment for the CTS has been described elsewhere (Roth et al., 2020a). Briefly, the incident caregivers enrolled in the CTS were identified by asking REGARDS participants if they were providing care on an ongoing basis to a family member, friend, or neighbor with a chronic illness or a disability, including any help with basic activities (e.g., dressing, bathing, and grooming), managing bills, arranging for medical care, watching or supervising a person, or providing transportation. Participants who answered “yes” were further questioned regarding their relationship with the person receiving care, whether they lived with that person, the year and month they began providing care because of that person’s health problem, whether or not they provided care to a person with dementia, and the number of hours of care provided per week. REGARDS participants were eligible to be enrolled as incident caregivers in the CTS if they answered “yes” to the caregiving status question and began providing care at least 6 months after the 1st REGARDS in-home assessment and at least 3 months before the 2nd REGARDS in-home assessment. The care recipients for whom the caregivers provided care had to be adults who were not residing in a nursing home, assisted living facility, or another residential care setting. In addition, the caregivers had to live either with or within 50 miles of the care recipients and had to be providing at least 5 hours of care per week in order to be eligible for enrollment in the CTS.
Enrolled incident caregivers were matched to a non-caregiving randomly selected control person in the REGARDS study based on up to seven demographic and health history factors including age, sex, race, education level, marital status, self-rated health at the REGARDS baseline CATI, and self-reported history of cardiovascular disease at the REGARDS baseline CATI. All non-caregiving controls reported no extended family caregiving responsibilities throughout their participation in the REGARDS study. The CTS was reviewed and approved by the Institutional Review Boards of the institutions conducting the study.
Measures
Sleep Variables
During the second comprehensive telephone interview for the REGARDS study, participants were asked the following questions about their sleeping habits: (A) “Thinking about a typical day for you, what time do you usually start trying to fall asleep?”; (B) “How many minutes does it usually take you to fall asleep, after you start trying to fall asleep?”; (C) “How much time, in minutes, do you usually spend awake in between the time you first fall asleep and the time you wake up and start your day?”; and (D) “Thinking about a typical day, what time do you usually wake up?” From the participant’s responses to these questions, we calculated sleep onset latency (SOL: Question B), wake after sleep onset (WASO: Question C), total time in bed (TIB: duration between response to Question A and Question D), total sleep time (TST: TIB - (SOL + WASO)), and sleep efficiency (SE: TST/TIB × 100).
Other Variables
Participants reported sex, race, and date of birth at the baseline REGARDS CATI and current employment status and the 2nd comprehensive interview. Both caregivers and controls completed the 10-item short form of the Center for Epidemiological Studies Depression (CES-D) scale (Andresen et al., 1994), which measures depressive symptoms, at the second comprehensive interview. Body Mass Index (BMI; kg/m2) was obtained from objective height and weight measurements during in-home visits (Howard, G. et al. 2017; Howard, V. J. et al. 2005). Categorical variables for BMI were used in the analyses (< 18.5 = underweight; 18.5–25 = normal; 25–30 = overweight; > 30 = obese).
Participants
A total of 251 incident caregivers and 251 matched controls were enrolled into the CTS. Among the 251 caregivers, seven reported that they started providing care after the second comprehensive telephone interview for the REGARDS study when the sleep questions were administered, and eight additional caregivers reported that they started providing care less than 3 months before that telephone interview. These 15 participants were not included in the present analyses. In addition, seven caregivers did not complete the sleep questions, and eight had missing data on at least one of the covariates (e.g., depressive symptoms and BMI). This left 221 (88%) of the 251 incident caregivers enrolled in the CTS who were included in the present analyses. For the non-caregiving controls, one participant did not complete the sleep questions, and three had missing data on at least one of the covariates. This left 247 (98%) of the 251 non-caregiving controls in the CTS who were included in the present analyses.
Statistical Analysis
Descriptive analyses were performed on the sleep questions to examine distributions and the possibility of individual outliers. No extreme outliers were detected. Linear multiple regression models were used to compare differences in sleep variables between incident caregivers and non-caregiving controls before and after adjustment for participant race, sex, age, BMI category (underweight, normal, overweight, and obese), and the 10-item CES-D score of depressive symptoms. One of these CES-D items asks about restless sleep, and sensitivity analyses were conducted using a 9-item CES-D score with this item removed. These analyses did not differ in any substantive ways from the results using the 10-item CES-D, so only the results with the 10-item measure are further reported.
For analyses of caregivers only, potential predictors of sleep disturbance were examined including whether the caregiver lives with the care recipient, provides care for a person with dementia, the number of caregiving hours provided, and employment status. Statistical significance was set at p < .05, and covariate-adjusted means were interpreted for clinical significance. Statistical analyses were performed using SAS® (version 9.4, SAS Institute Inc., Cary, NC).
Results
Demographic characteristics for incident caregivers and non-caregiving controls.

CED-D = Center for Epidemiological Studies Depression scale; M = mean; SD = standard deviation.
Unadjusted comparisons of self-reported sleep characteristics for incident caregivers and non-caregiving controls.

M = mean; SD = standard deviation.
Multivariable regression of sleep quality in incident caregivers and matched non-caregiving controls.

TST = total sleep time; TIB = time in bed; SOL = sleep onset latency; WASO = wake after sleep onset; SE = sleep efficiency; BMI = body mass index. Outcome variables are scaled in minutes per 1-point change in the predictor.
Multivariable regression of sleep quality among incident caregivers
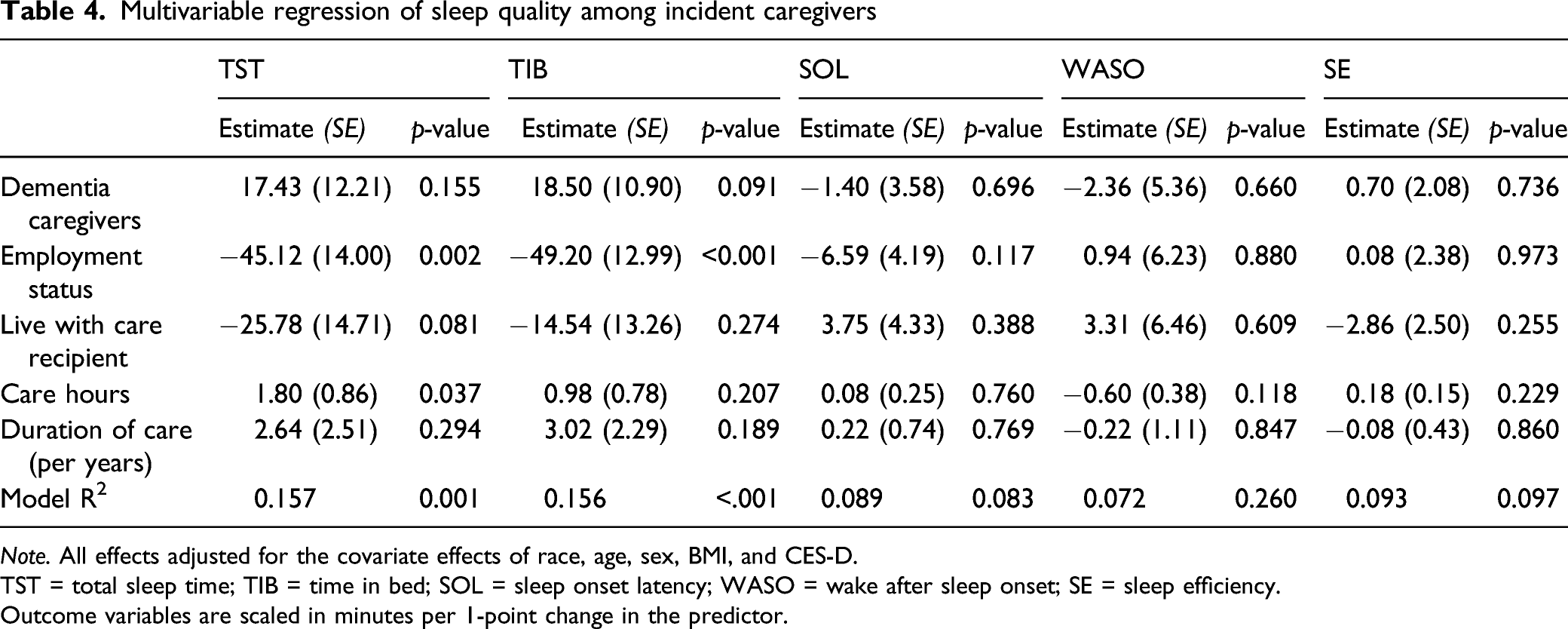
Note. All effects adjusted for the covariate effects of race, age, sex, BMI, and CES-D.
TST = total sleep time; TIB = time in bed; SOL = sleep onset latency; WASO = wake after sleep onset; SE = sleep efficiency.
Outcome variables are scaled in minutes per 1-point change in the predictor.
Discussion
This study compared the self-reported sleep characteristics of incident caregivers and a carefully matched sample of non-caregiving controls using data from a national population-based study. We found that caregivers took significantly longer to fall asleep (i.e., longer SOL) than non-caregivers. Depressive symptoms were found to be related to four of our five sleep measures across both caregivers and controls. Because increased depression is known to be associated with sleep disturbance (Ypsilanti et al., 2018), these effects (TIB, SOL, WASO, and SE) support the validity of the self-reported sleep measures used in the REGARDS study.
To our knowledge, the design of this population-based study is unique compared to previous studies of the association between family caregiving and sleep quality. In our study, the non-caregiving control sample was carefully matched to caregivers based on up to seven factors, whereas other studies utilized convenience samples or matched caregiver/non-caregiver samples with a small number of criteria (e.g., sex, age, and marital status) (Castro et al., 2009; Fekih-Romdhane et al., 2020; Fonareva et al., 2011; Song et al., 2020). In addition, previous studies were focused on caregivers for a specific condition, such as caregivers for dementia (Castro et al., 2009; Fonareva et al., 2011; Gao et al., 2019; Rowe et al., 2008), patients with psychotic disorders (Fekih-Romdhane et al., 2020), or to a particular group—female veteran caregivers (Song et al., 2020) or spousal caregivers (Mills et al., 2009).
Our findings have some similarities to those of other researchers who also found significant differences in sleep quality using convenience samples. Fekih-Romdhane et al., (2020) compared “sleep quality” based on PSQI scores among caregivers, and also found significant differences related to age, but did not measure the specific sleep parameters (TIB and TST) that we identified as significant. Rowe et al. (2008) found differences in objectively and subjectively measured TST, SE, SOL, and WASO, and their results differ from ours in subtle but important ways. In our study, we found that subjectively measured SOL was significantly different between caregivers and controls, whereas Rowe et al. (2008) found that differences in SOL were only significant when measured objectively.
Fonareva et al. (2011) and Rowe et al. (2008) found, using objective measures, that caregivers took significantly longer to fall asleep than did non-caregivers, with relatively small (n = 20 and n = 31, respectively) convenience samples of dementia caregivers. Our study, using self-reported sleep measures, found similar results (longer SOL), but is unique in the literature in that we used a larger and more heterogeneous, population-based sample of caregivers, with both dementia and non-dementia caregivers included in our sample. We also enrolled individually matched non-caregiving controls. Our results confirm the earlier findings with respect to SOL and suggest that they can be extended to other types of caregivers beyond dementia caregivers.
Conversely, our results are not consistent with the meta-analysis findings of Gao et al. (2019). We did not find any differences between caregivers and controls on total sleep time, nor did we find any differences between dementia caregivers and caregivers of other conditions. Explanations for these differences between our findings and those of other studies may be based on differences in sample selection. As noted above, in our study we evaluated incident caregivers from a population-based parent study. The caregivers in the present analyses became caregivers after they were already enrolled in the REGARDS study. Caregiving status, therefore, was not a consideration in the initial enrollment into the REGARDS study, and this may reduce the selection biases that are worrisome when convenience samples of pre-existing caregivers and non-caregivers are compared. In addition, the differences in sleep quality identified in prior studies for specific types of caregivers may generalize to the broader population of caregivers. In our sample, we include a broad range of caregiver characteristics (e.g., multiple care-recipient conditions, co-residing and non-co-residing caregivers, and working and non-working caregivers).
The observed difference between caregivers and non-caregivers on sleep onset latency was just over 4 minutes, on average. At first glance, this might appear to be a small difference. However, additional descriptive analyses indicated that 29.2% of caregivers reported taking 30 or more minutes to fall asleep compared to 21.8% of controls. Thus, caregivers were 34% more likely to have sleep onset latency of a half hour or more compared to controls. Other important effects on sleep quality appeared in the analysis among the caregivers only. We found that caregivers who were employed slept less, and spent less time in bed compared to non-employed caregivers. These findings may reflect the pressures of the time commitments of both working and caregiving (employed caregivers versus non-employed caregivers). Among these caregivers, employment and caregiving demands could reduce the time available for sleep. We also found that depressive symptoms were predictive of sleep quality in both caregivers and controls, which is not surprising since depression has been associated with sleep disturbances (Ypsilanti et al., 2018). Our finding that the underweight BMI group reported lower sleep efficiency than the normal weight BMI group differs somewhat from other caregiver studies (Eleuteri et al., 2018) which found that for caregivers with low depressive symptoms, higher sleep disturbances were associated with higher BMI.
The lack of significant differences between dementia caregivers and other types of caregivers is consistent with other findings from the CTS (Roth et al., 2020b; Sheehan et al., 2020). Sheehan et al. (2020) found that observed differences between dementia caregivers and non-dementia caregivers on levels of stressors, burden, and measures of well-being could be accounted for by the greater number of caregiving hours and total number of care recipient problems encountered by dementia caregivers compared to non-dementia caregivers; after adjustment, no differences between dementia and non-dementia caregivers were found on burden and well-being factors. Similarly, Roth and colleagues (2020) found that dementia caregivers did not exhibit any differences in specific inflammatory biomarkers compared to matched controls (Roth et al., 2020b). This suggests that, to the extent that dementia caregiving is viewed as more stressful than other types of caregiving, this difference is not reflected in corresponding differences between most of the behavioral or biological variables for dementia and non-dementia caregivers measured in the study, including sleep quality.
Our study has some limitations that should be taken into consideration when interpreting the results. The lack of longitudinal data does not allow observations of changes in sleep patterns of caregivers and non-caregivers over time. Thus, our study is a “snapshot” in time comparison of sleep in incident caregivers and non-caregivers. The reliance on self-reported, subjective sleep parameters also does not provide objective measures of the sleep parameters evaluated. Future studies could be improved by employing actigraphy and polysomnography to provide objective measures of sleep quality in population-based samples. Additionally, our study only included Black and White adult participants and may not be generalizable to other racial and ethnic groups.
In our population, caregivers took longer to fall asleep than non-caregivers and we know from prior work (Groeger et al., 2014; Mather et al., 2020; McCoy & Strecker, 2011; Narang et al., 2012; Petrov et al., 2018; Spira et al., 2010; Tapp et al., 2017; Tempesta et al., 2015) that poor sleep quality increases the risk of developing physical and mental impairments. As the population ages, the need for caregivers will rise and addressing caregivers’ poor sleep quality may become a public health imperative, particularly as the physical and mental consequences of poor sleep quality in caregivers could also impact the care recipients they care for. Effective interventions to assess and improve caregivers’ sleep quality are needed.
Footnotes
Acknowledgments
Declaration of Conflict of Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Adam Spira received an honorarium as a consultant to Merck and honoraria from Springer Nature Switzerland AG for guest editing special issues of Current Sleep Medicine Reports.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: This research project is supported by cooperative agreement U01 NS041588 co-funded by the National Institute of Neurological Disorders and Stroke (NINDS) and the National Institute on Aging (NIA), National Institutes of Health, Department of Health and Human Service. The Caregiving Transitions Study is further supported by an investigator-initiated grant [RF1 AG050609] from the NIA. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NINDS or the NIA. Representatives of the NINDS were involved in the review of the manuscript but were not directly involved in the collection, management, analysis, or interpretation of the data.
Research Ethics
The REGARDS and CTS were reviewed and approved by the Institutional Review Boards of the University of Alabama at Birmingham (IRB No. 020925004) and Johns Hopkins University (IRB No. 00096563), respectively.