
Abstract
Function after acute hospitalization is mostly operationalized by Basic Activities of Daily Living (BADL), a limited concept that overshadows a wide range of instrumental, social, and recreational activities, otherwise referred to as participation. Participation is important for patients’ health and quality of life after hospitalization. This study focuses on high-functioning older adults, examining functional recovery after hospitalization by comparing BADL assessment with assessment of participation at one and three months following discharge relative to pre-hospitalization. Quantitative data were collected from 72 participants divided into two age groups of hospitalized older adults (age 65–74, n = 38; age ≥75, n = 34), followed by home visits after 1 month and telephone interviews 3 months after discharge. Both groups experienced a significantly greater decline in participation, compared with BADL, which were mostly preserved. A comprehensive assessment of participation better captures functional changes in high-functioning older adults. Early identification of participation withdrawal is crucial for preventing disability.
Keywords
High-functioning older adults hospitalized for acute medical illness are at risk of losing meaningful health-promoting activities such as leisure and social activities in the months post-hospitalization, even when basic function is preserved.
The traditional definition of hospital-associated functional decline overshadows the subtle changes experienced by high-functioning older adults in higher-level activities.
Adopting a broader perspective on function after acute hospitalization, using assessment of participation that can capture functional changes in multiple domains will help promote active lifestyles in older adults, possibly preventing future healthcare utilization.
The assessment of participation should begin during hospitalization to improve the transition process from hospital to the community.
Introduction
Functional decline after acute hospitalization is a common, unintended outcome experienced by up to 60% of older patients during and after discharge (Boyd et al., 2008; Covinsky et al., 2011; Zisberg et al., 2011, 2015). It is associated with many adverse outcomes such as re-hospitalization and nursing home placement (Berian et al., 2016; Boyd et al., 2008; Depalma et al., 2013) and can last up to 2 years post-discharge (Boyd et al., 2009). The first 3 months after hospitalization represent a critical period of high vulnerability, presence of geriatric syndromes, and risk for adverse health outcomes, which may result in a failure to return to baseline functioning, referred to as post-hospital syndrome (Krumholz, 2013; van Seben et al., 2020).
In recent years, studies highlight the necessity to examine hospital-associated functional decline as a multidimensional concept that sensitively assesses multiple domains of functioning, such as social and leisure activities, in older adults transitioning from hospital to home (Brown, 2020; Liebzeit, et al., 2018). Most studies, however, continue to quantify function through the narrow lens of Basic Activities of Daily Living (BADL) that focuses on self-care, such as dressing and bathing (Buurman et al., 2012; Fimognari et al., 2017). Few studies additionally assess Instrumental Activities of Daily Living (IADL), such as shopping and financial management (Dharmarajan et al., 2020; Zisberg et al., 2016), and yet a meaningful life consists of participation in many activities that go far beyond BADL or IADL.
It has been well established that lower preadmission function in BADL, IADL, and cognitive impairment, as well as frailty and older age, are predisposing risk factors for hospital-associated functional decline (De Saint-Hubert et al., 2009; Hoogerduijn et al., 2012). However, lesser attention has been paid to the functional recovery of a sub-group of high-functioning older adults who are independent in basic function and with no severe cognitive impairments (i.e., dementia or delirium). BADL and IADL assessments of high-functioning older adults often indicate to preserved functional abilities. Indeed, because such traditional assessments do not take into account the subtle changes in the daily operation of high-functioning older adults, BADL and IADL assessments may overshadow the decline and difficulties experienced by these patients in other areas of life following hospitalization for acute illness, resulting in a ceiling effect (Fieo et al., 2011). For example, participation in outdoor social and leisure physical activities requires higher cognitive and physical abilities, compared with BADL that are performed mostly in the home space (Liebzeit et al., 2018; Toglia & Foster, 2020). Therefore, such higher-level activities may be affected and often ignored in this sub-group following hospitalization.
According to the World Health Organization’s Interna-tional Classification of Functioning, Disability, and Health (ICF) model (WHO, 2001), the traditional assessments of basic functions address activity limitations (i.e., limitations in independent execution of daily tasks such as self-care). In contrast, participation provides a broader concept of functional recovery that takes into account a variety of activities and is defined as a person’s “involvement in life situations” and the extent to which they engage in societal contexts (WHO, 2001, p.10). It encompasses a wide range of purposeful and meaningful activities, including IADL, leisure, recreation, socio-cultural, and religious activities. Participation is considered a key factor of a person’s well-being during the aging process (Amagasa et al., 2017; Levasseur et al., 2010; Sowa et al., 2016) and has positive effects on preventing cognitive decline, functional disability, and depressive symptoms in older adults (Chiao et al., 2011; Gao et al., 2018; Tomioka et al., 2018). In line with the WHO’s call for “active aging” (WHO, 2002), the concept of participation illustrates the difference between living a meaningful life as opposed to the reduction of life to basic and instrumental functioning. Changes in participation are considered part of the aging process, becoming more prominent in people aged 75 years and older (Arnadottir et al., 2011; Yang et al., 2018).
Although researchers acknowledge the dramatic effect of hospitalization with acute illness on declines in participation (Covinsky et al., 2011), there is a scarce body of literature examining how leisure, productive, and social activities are affected. Few studies addressed limited aspects of participation, such as community mobility (Brown et al., 2009; Loyd et al., 2018; Wells et al., 2020), and studies tend to overlook potential differences between various age groups of high-functioning older adults in terms of resumption of social and leisure activities and levels of participation following acute hospitalization.
The current study aimed to fill these two main gaps by characterizing and comparing dimensions of functional recovery: participation (i.e., IADL, social, and leisure activities) and BADL in two age groups of high-functioning older adults up to 3 months after acute hospitalization. We hypothesized that differences in the relative recovery will be found between the concept of participation and BADL at 1 and 3-months, such that the participants experience greater decline in participation, as compared with BADL. This decline would be more pronounced among older adults aged 75 years and older.
Methods
Participants and Setting
This study is part of a larger, prospective research project, Hospitalization Process Effects on Mobility Outcomes and Recovery (HoPE-MOR) (Gur-Yaish et al., 2021). In the current study, we recruited community-dwelling older adults who were admitted to one of three internal medicine units at a medical center in Israel for a non-disabling diagnosis. High-functioning older adults were recruited as participants between February 2019 and February 2020 if they met the following criteria: (1) age 65 years or older, (2) self-reported ability to walk with or without personal or assistive devices prior to admission, (3) independence in BADL 2 weeks prior to admission defined by the accepted Modified Barthel Index (mBI) cutoff of >80 (Sinoff & Ore, 1997), (4) able to speak, read, and write Hebrew, and (5) able to sign an informed consent form as determined by a health professional. Exclusion criteria were (1) admission diagnosis of acute stroke or other acute or chronic neurologic disorder, (2) need for mechanical ventilation, (3) admission for end-of-life care, (4) prescribed isolation (e.g., patient in isolation due to highly communicable disease), (5) diagnosis of dementia as obtained from medical records, and (6) diagnosis of delirium during the hospital stay. Patients were assessed for the presence of delirium at admission and daily during hospitalization using the 4'A’s Test (4AT) (Bellelli et al., 2014).
A total of 138 participants were approached for participation in the current study, 45 declined, leaving 93 eligible participants. Eight withdrew consent during hospitalization or 1 month after discharge, three were transferred to another ward or discharged less than 24 hours within admission, two were unavailable during the 1-month follow-up, and one was discharged to a rehabilitation facility, leaving 79 participants who completed the 1-month follow-up. At the 3-month follow-up, one participant withdrew consent and one died. Five of the 3-month follow-ups were scheduled during the outbreak of COVID-19, and therefore participants were excluded from the analysis, leaving a total of 72 participants who completed the 3-month follow-up. Study participants (n = 72) were divided into two age groups, “younger” (ages 65–74, n = 38) and “older” (ages 75–90, n = 34), according to the median age of the sample of 74 years.
Data Collection
Participants were recruited within 24 hours of admission to the internal medicine ward. After obtaining informed consent, a trained research assistant administered the assessment measures and questionnaires during the first 48 hours of hospitalization on the ward. Follow-up assessment took place at participants’ homes 1 month after discharge and follow-up assessment at 3 months was conducted by telephone interview. All assessments and questionnaires were conducted in Hebrew.
Measurements
Participation was measured using the Activity Card Sort (ACS) version one (Baum & Edwards, 2001). An interview version was used to compare the individual’s activity and participation levels with those prior to hospitalization to determine the impact of illness on participation. The ACS consists of 88 daily activities divided into four main areas: (1) IADL (e.g., grocery shopping, household care, meal preparation, financial management, driving, and using public transportation), (2) sociocultural leisure activities (e.g., meeting family and friends, going to the cinema, theaters, and restaurants, and engaging in religious activities), (3) leisure activities with low physical demands (e.g., reading, watching television, listening to music, and painting), and (4) leisure activities with high physical demands (e.g., walking, swimming, exercising, travelling, and gardening). During hospitalization, participants retrospectively rated whether they participated in each activity relating to the period of 2 weeks preceding their current hospitalization (no=0; yes=1). At the 1- and 3-month follow-ups, participants were asked whether they performed the activities to a similar extent (=1), to a lesser extent (=0.5), or not at all (=0). The ACS provides an overall “retained activity level” score (0–100) calculated as a percentage, that is, the sum of the weighted values of the activities a person is currently engaged in divided by the activities they were engaged in before hospitalization. Accordingly, baseline participation level before hospitalization was defined as 100%, and at follow-up after one and 3 months, participation was calculated as a percentage of activities maintained. Lower percentages represent greater withdrawal from previous participation. The ACS is used worldwide and has been translated, adapted, and validated in Israel (Katz et al., 2003). The original ACS has good test–retest reliability (r = 0.90) among community-dwelling adults (Baum & Edwards, 2001); and has good construct validity as evidenced by studies comparing activity levels across different age groups and populations with neurological disabilities (Katz et al., 2003; Sachs & Josman, 2003).
BADL were measured using the Modified Barthel Index (mBI) (Shah et al., 1989) that consists of individuals’ subjective assessment of their independence level in 10 items of BADL: feeding, grooming, bathing, dressing, bowel and bladder care, toilet use, ambulation, transfers, and stair climbing. The total score ranges from 0 to 100 and reflects the amount of care needed, with lower scores indicating increased disability. BADL were assessed at admission, retrospectively for 2 weeks before admission (baseline mBI), and at one and 3 months after discharge. A functional decline in BADL was defined as a decrease of five points or more on the mBI from baseline pre-morbid status to follow-up at one and 3 months, expressing a loss of independence in one of the BADL domains (Palleschi et al., 2011). Similar to ACS, the current study used a retained mBI total score, that is, the sum of post-hospitalization mBI divided by total pre-hospitalization mBI, calculated as a percentage of preserved activity level.
Additional sample characteristics were measured at admission. Depressive symptoms were assessed using the Hospital Anxiety and Depression Scale (HADS) that categorizes symptoms of depression as normal, borderline, or positive (Zigmond & Snaith, 1983). Cognitive status was assessed using the Mini Mental State Examination Telephone version (MMSET) (Roccaforte et al., 1992). Symptom severity was assessed using 11 self-rated common symptoms (Kroenke et al., 1999), comorbidities using the Charlson Comorbidity Index (CCI) (Charlson et al., 1987), and severity of illness using the National Early Warning Score (NEWS) (Jones, 2012). Length of Hospital Stay (LOS) was obtained from the patients’ medical records.
Statistical analysis
Descriptive data were presented as frequencies for categorical variables and as mean and standard deviation for continuous variables. All study variables were normally distributed except for mBI (right skewed) and ACS (left skewed). A log10 transformation was performed to normalize the distribution of the overall main ACS score. The transformation of the mBI data did not correct the non-normal distribution. Independent sample t-test and Mann–Whitney tests for continuous variables and chi-square tests for categorical variables were used for sensitivity analysis to test for significant differences in study variables between participants who completed the study and those who withdrew, and between the two age groups. A mixed-model repeated measures ANCOVA was used to compare time by group effects in ACS total scores, while controlling for group differences in study variables. Wilcoxon test was used to compare between the ACS and mBI total retained scores within the age groups. For all analyses, significance was accepted at level p <.05. Analyses were performed using IBM SPSS Statistics for Windows, version 25 (IBM Corp., Armonk, N.Y., USA).
Results
Study group characteristics for the total sample and by age groups are presented in Table 1. Of the 72 participants, 38 (53%) were women, and the mean age was 75.9 years (SD ± 7, range 65–90). The most common referral diagnoses were pneumonia, congestive heart failure, and chronic obstructive pulmonary disease. Sensitivity analysis revealed no significant differences (p > .05) in basic characteristics (age, gender, years of education, LOS, mBI, illness severity, and comorbidity) between the 72 participants who completed the 3-month follow-up and the 21 participants who withdrew. The younger group had significantly shorter LOS compared with the older group.
Characteristics of study sample by age groups.

Notes. p-Values from chi-square tests for categorical and t tests for continuous variables. p-Value from Mann–Whitney for the Modified Barthel Index.
Abbreviations: MBI: Modified Barthel Index, NEWS: National Early Warning Score, CCI: Charlson Comorbidity Index, MMSET: Mini-Mental State Examination Telephone version, HADS: Hospital Anxiety and Depression Scale.
Participation and BADL
When compared with participants’ pre-hospital basic function and participation levels, results showed that the basic function in the older group was preserved at 98% after 1 month (SD = 4.7, range = 77–100) and 3 months (SD = 3.5, range = 84–100). However, they reported participation withdrawal to a level of 81% (SD = 19.8, range = 36–100) after one month and 86% (SD = 18, range = 50–100) after 3 months. Results among the younger group showed that basic function was preserved at 99% (SD = 2.7, range = 86–100) at both 1 month and 3 months. However, participation withdrawal was to a level of 89% (SD = 15.5, range = 56–100) at one month and 92% (SD = 13, range = 58–100) after 3 months.
For the total retained activity level of the ACS, a mixed-model repeated measures ANCOVA (controlling for LOS) revealed that the main effect of time (between 1 and 3 months) and the interaction effect (time X group) were not statistically significant (F[1,69] = .036, p = .850, η2 = .001),)F[1,69] = .379, p = .549, η2 = .005), respectively. Similarly, the main group effect had no statistical significance (F[1,69] = [4.9], p = .051, η2 = .054).
No significant differences were found between mBI retained scores at 1 and 3 months in the younger age group (z = −1, p = .317) and the older group (z = .001, p = 1). No significant differences were found between age groups in the mean retained mBI score at 1 month (z = −1.5, p = .114). However, a statistically significant difference was found in the mean retained mBI score at 3 months (z = −2.4, p = .014), with the younger group having higher retained scores (mean = 99, SD ± 2.7) compared with the older group (mean = 98, SD ± 3.5). An additional mBI analysis showed that 18% of participants in the older age group had a clinically significant decrease of 5 points, whereas a similar decline was seen in only 8% of participants in the younger group.
Participation vs. BADL over time
When comparing mBI and ACS retained scores, statistically significant differences were found in the younger group at 1 month (z = −3.9, p = .001) and 3 months (z = −4, p = .001), and in the older group at 1 month (z = −4.6, p = .001) and 3 months (z = −4.1, p = .001). Both groups had lower retained ACS scores compared with the retained mBI scores. The functional trajectories are further demonstrated in Figure 1.
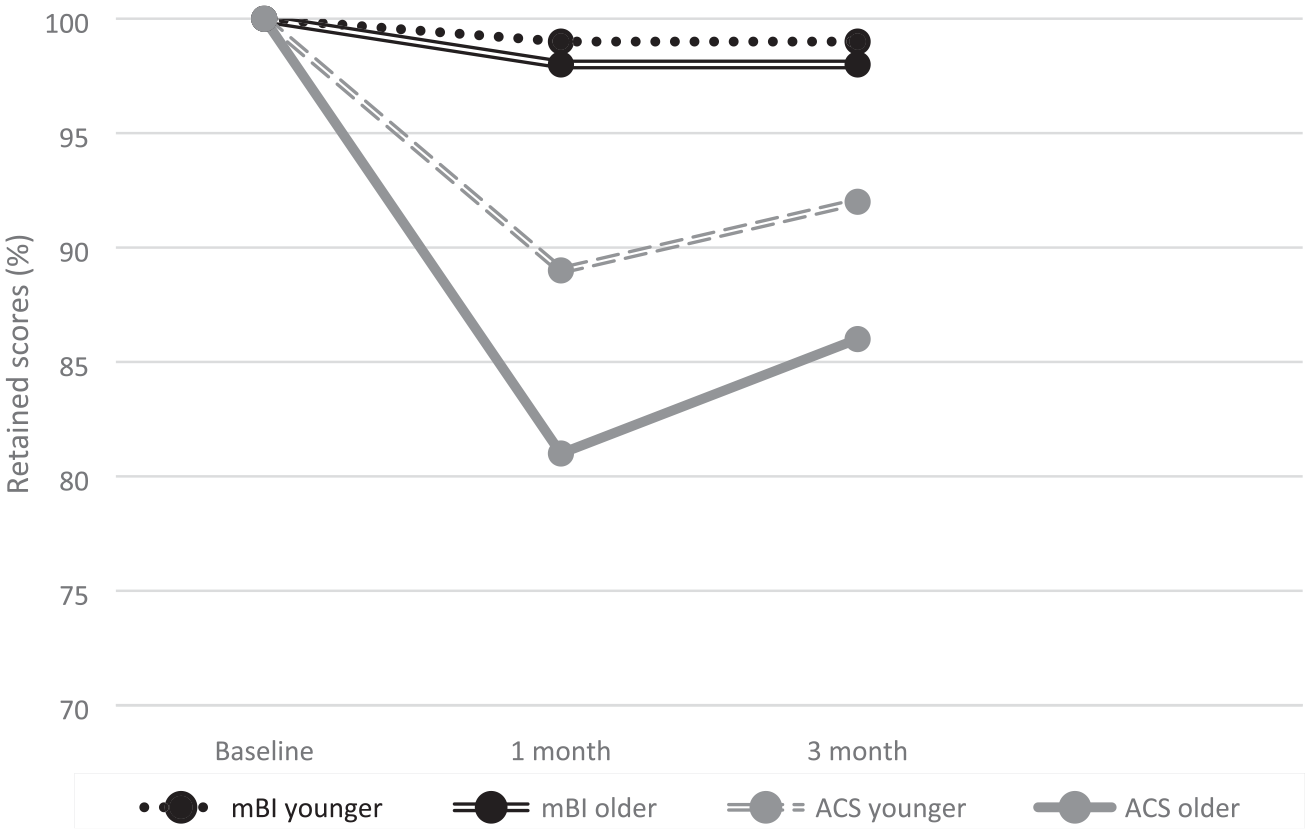
Functional trajectories: Activity Card Sort (ACS) and Modified Barthel Index (mBI) retained scores (%) by time and age groups.
Discussion
The primary aim of this study was to characterize and compare functional recovery captured by two distinct concepts (i.e., BADL and participation) among two age groups of high-functioning hospitalized older adults. Contrary to our hypothesis, no significant differences in recovery of participation were found between the younger and older age groups. While both groups showed a decline in participation level in the first month, followed by a recovery trend at 3 months, neither group returned to baseline levels of participation after 3 months post-discharge. While their basic functions were mostly preserved, participants reported giving up outdoor physical recreational activities such as walking, exercising, and going to the gym, as well as social activities such as attending concerts and participating in a bridge club. We found that the older group experienced a significantly greater decrease in BADL after 3 months. Nevertheless, the percentages of their functional decline were lower than reported in the literature (Loyd et al., 2020), and overall they remained independent in their basic function after discharge. The average comorbidity score of both age groups in the current sample was lower than reported in previous studies of acutely hospitalized older adults supporting a sample of high-functioning and less comorbid older adults (Frenkel et al., 2014; Zisberg et al., 2015). Thus, the novelty of this study is in focusing on two age groups of high-functioning older adults, and illustrating that they are at risk for decreased participation in meaningful activities beyond BADL.
The decrease in participation in both age groups warrants attention as participation in social, leisure, and physical activities has a great impact on subjective well-being and is highly effective as a health promotion strategy for community-dwelling older adults (Adams et al., 2011; Bherer et al., 2013; Yamashita et al., 2019). Participation in social activities has been found to reduce the risk of functional decline in BADL (Gao et al., 2018) and is associated with a lower risk of depression (Choi et al., 2021). High levels of participation in leisure activities were associated with a decreased risk of cognitive impairment in community-dwelling older adults (Zhu et al., 2017). This is consistent with the call in recent decades for “active aging” which encourages older individuals to remain active in their communities and participate in meaningful social and productive activities (WHO, 2002). Therefore, examining participation in the context of acute hospitalization is of great importance because a decline in participation after discharge can lead to secondary negative outcomes.
The improvement in participation between 1 and 3 months was not significant in either age group, suggesting that the recovery process in IADL and social leisure activities extends beyond the first few months. A study by Boyd and her associates (2009), for example, showed that recovery in IADL activities after acute hospitalization can take up to 2 years, while other studies that operationalized participation as community mobility highlighted a recovery period of several months to 2 years following acute hospitalization (Brown et al., 2009; Dharmarajan et al., 2020; Loyd et al., 2018). It is noteworthy that these studies are limited to one aspect of participation and ignore the quantification of a wide range of meaningful daily activities, such as social and leisure activities.
The difference between the relative decline in participation and BADL was significant at 1 and 3 months in both age groups. This different pattern, showing a greater decrease in participation compared with the relatively preserved BADL, supports the notion that the assessment of participation in high-functioning older adults better captures functional changes. Because BADL were largely preserved, we can assume that they often overshadow the decline in other, less mundane, but no less meaningful activities. As demonstrated in the current study, high-functioning older adults may be unrecognized by the traditional assessment of basic function. Hospitalization is a significant event, and after discharge, older adults may invest their efforts in survival-related activities such as BADL at the expense of other activities that are easier to abandon, such as social and leisure activities outside the home—as our findings confirm.
Because functional decline is still a common negative outcome of hospitalization in older adults, efforts should be made to prevent it (Brown, 2020). An important step is to adopt a broader perspective on function and use instruments that can capture changes in multiple domains of function. The current study demonstrates the multidimensional nature of hospital-associated functional decline beyond the well-documented BADL (Loyd et al., 2020) and is consistent with recent recommendations of reconceptualize and assess function after acute hospitalization (Liebzeit et al., 2018). A comprehensive assessment of participation would lead to a better understanding of the ability of older adults to live independently and reintegrate into the community after hospitalization. Such an assessment would allow identification of which activities are meaningful and important for the patient in recovery to set personal functional goals. The assessment of participation should begin during hospitalization to enable early identification and to improve the transition process from the hospital to the community. Indeed, goal-directed transition interventions that are designed to meet older patient’s unique needs were previously recommended (O’Donnell et al., 2021), and maintaining participation can serve as their ultimate goal.
Limitations
The limited follow-up period of 3 months is a limitation of this study, as it may have masked a positive trend in recovery. Of note, several studies that examined functional recovery after acute hospitalization focused on longer follow-up periods and found similar trends (Brown et al., 2009; Dharmarajan et al., 2020). Second, the sample of the present study is relatively small and participants were recruited from a single medical center, which limits the generalizability of the results. Third, because the ACS measures participation through a variety of activities, its administration during hospitalization takes a relatively long time. Furthermore, administration of the mBI and ACS included retrospective recall. Limitations of self-report measures administered at different time points (e.g., during hospitalization and in follow-up assessments) such as recall bias are well-described, including patients' overestimation or underestimation of their level of independence. Future longitudinal studies examining participation after acute hospitalization with larger and diverse samples using different participation measures may help generalize the current findings. In addition, it is recommended to examine factors associated with recovery of participation after acute hospitalization to plan targeted interventions.
Conclusions
Even for high-functioning older adults, acute hospitalization can result in significant changes in a wide range of activities beyond basic functions, affecting their ability to live rich and meaningful lives. To promote active aging, adoption of a broader perspective of function and recovery following hospitalization that includes participation is required. Early recognition using a comprehensive assessment is crucial for planning transitional and post-acute care services to prevent participation declines.
Footnotes
Acknowledgements
We thank the contribution of the HoPE MOR team and the teams in the Internal medicine units at Bnai Zion Medical Center for their assistance in data acquisition.
Author Contributions
All authors contributed to concept and design, and/or data acquisition, and/or analysis and interpretation of data. All authors were involved in the manuscript preparation, revision, and final approval of version to be published. Dr. Kizony and Dr. Agmon had equal contributions to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially funded by the Israel Science Foundation (Mobility ISF1216/17). The funding agency had no role in the design and conduct of this study, in the collection, analysis and interpretation of the data, or the preparation, review, and approval of the manuscript.
Ethical Approval
The study was approved by the University of Haifa Ethics Committee (Approval no. 324/17) and by the Bnai-Zion Medical Center institutional review board (0099-18-BNZ).
Informed Consent
A written informed consent was obtained from all participants of this study.