
Abstract
Background:
This study aims to investigate whether regularly active individuals have different levels of mental health and resilience compared to intermittently active individuals.
Methods:
In this 4-year longitudinal study, 180 older people were included. General linear models were used to assess the level of physical activity, psychological resilience, and mental health among regularly and intermittently active older adults.
Results:
Those who maintained regular physical activity were more resilient than those who did not. However, no differences were observed for mental health outcomes. Although those with higher levels of resilience had fewer mental health problems, there were no significant differences between the groups based on their level of physical activity.
Conclusion:
Differences in resilience levels favoring regularly active individuals were found. In both groups, resilience was inversely associated with mental health problems. These findings may help elucidate the underlying mechanisms in the relationship between physical activity and health outcomes.
Greater levels of resilience were found among regularly active individuals as compared to intermittently active individuals.
Better mental health outcomes were associated with greater levels of resilience for both intermittently and regularly active individuals.
No differences in the mental health-resilience relationship were found between regularly and intermittently active individuals.
Gerontologists must be aware of the levels of resilience of their patients.
Interventions promoting physical activity and resilience could be options to promote the mental health of older adults.
Activity engagement can be considered an important determinant of health to these individuals.
Introduction
The World Health Organization (WHO) recognizes physical inactivity as a major risk factor for overall morbidity and premature mortality (Kohl et al., 2012). Similarly, it appears to play a key role in the degenerative consequences that arise from aging (Bauman et al., 2016). There is accumulating epidemiological evidence of the effect of physical exercise on health, with the latest evidence focusing on neurological health and psychosocial and mental well-being (Bauman et al., 2016). A multicenter cohort study with 116,043 participants from 12 European studies found a significant association between healthy lifestyle and disease-free years (Nyberg et al., 2020).
Population aging poses a public health challenge in both the adoption and maintenance of a healthy lifestyle in decelerating the onset of chronic illnesses and effectively managing present illnesses and disabilities (Satariano et al., 2012). Aging is, in fact, a period of potential challenges (e.g., chronic diseases, widowhood, and retirement) and, in order to handle these challenges more appropriately, it is crucial to understand how older individuals maintain healthy behaviors (Satariano et al., 2012).
In this context, continuous physical activity (i.e., maintaining regular activity through the years) seems to be associated with better outcomes such as healthy aging and lower levels of depressive symptoms and inflammatory mediators as compared to irregular/intermittent physical activity (i.e., sedentary or altering moments of physical activity and sedentarism through the years), (Hamer et al., 2009, 2014). Therefore, promoting regular physical activity seems to be an important goal of public health.
For successful aging, the changes associated with the aging process must be accepted, addressed, and adjusted to, which is why resilience is essential. The concept of resilience often involves acquiring the skills and resources that can moderate the adversities faced by older adults in their lives and mitigate the negative consequences of these events or, in some cases, lead to positive growth and development (Lee et al., 2013; B. Resnick, Gwyther, & Roberto, 2011).
Resilience research in gerontology examines why and how some older adults seem to recover or thrive in the face of adversity and setbacks in their lives (Resnick et al., 2011). Evidence indicates that resilience does not exist in isolation and is affected by a variety of social and personal factors such as social support, economic condition, losses and changes, adversities, diseases, and coping strategies (Wermelinger Avila et al., 2017). Resilience influences many aspects of older adults’ lives, including quality of life, successful aging, life satisfaction, morale, lower risk of mortality, and mental health (Resnick et al., 2011; Wermelinger Avila et al., 2017).
Neurological and mental disorders account for 6.6% of the total disease burden in older people (Prince et al., 2015). Physical activity and resilience are among the multiple social, psychological, and biological factors that determine the level of mental health (WHO, 2015). Nevertheless, there is limited information on the association between resilience, mental health, and the level of physical activity in the older population (Siltanen et al., 2020).
Previous theories have highlighted the aforementioned association. Sonstroem (1978) proposed that physical activity may improve an individual’s skills and confidence levels, which, in turn, may promote resilience. In this theory, both resilience and physical activity are related to mental health. The cross stressor adaptation theory (Hegberg et al., 2015) also highlights this relationship, proposing that regular physical activity induces biological changes that promote bodily responses to physical activity as well as psychological stressors and, these responses may improve an individual’s resilience to stressors.
These theories were supported by prior studies that found that physical activity could influence the relationship between resilience and mental health. Kukihara et al. (2018) found that resilience fully mediated the relationship between physical activity and depression in Japanese older adults. Similarly, a Brazilian study (Wermelinger Ávila et al., 2017) and a Spanish study found that physically active individuals have greater levels of resilience and better mental health (Martinez-Moreno et al., 2020).
Nevertheless, most of the evidence relies on cross-sectional designs, which makes it difficult to interpret cause-effect relationships (Kukihara et al., 2018; Martinez-Moreno et al., 2020; Wermelinger Ávila et al., 2018). In a 2020 article on the psychological concepts of resilience in old age and recommendations for future research, the authors stress the importance of prospective longitudinal studies (Infurna, 2020).
In 2022, our group published a 2-year longitudinal study of 291 older adults. In this study, resilience at baseline was a predictor of the older adults’ mental health after 2 years of follow-up care, and the level of physical activity influenced the type of resilience mechanisms used (Wermelinger Ávila et al., 2022). Even with this initial evidence, studies with longer follow-up periods can provide further understanding of the connections of mental health outcomes, resilience factors, and depression and explain the differences between older adults who remain active throughout follow-up and those who do not remain regularly active. The data can orient public policies toward promoting regular physical activity and increasing resilience among the older population (Cosco et al., 2017; Infurna, 2020).
To bridge this gap, we conducted the current study to investigate possible differences in mental health, resilience, and the relationship between mental health and resilience among regularly and intermittently active individuals during a 4-year follow-up period.
We formulated the following hypotheses:
(1) Regularly active individuals would be more resilient than intermittently active individuals.
(2) Regularly active individuals would have better mental health outcomes than intermittently active individuals.
(3) There would be an inverse relationship between mental health symptoms and resilience among participants.
(4) There would be differences in the mental health-resilience relationship between regularly and intermittently active individuals.
Methods
Study design, period, and location
This observational cohort study had a 4-year follow-up period (three waves) and was conducted in the city of Juiz de Fora in the state of Minas Gerais, Brazil, from August 2015 to March 2020. Juiz de Fora is a mid-sized city with a population of 516,247, wherein 13.6% are older persons (SIDRA, 2014). The city is strategically located between the three main Brazilian metropolises: São Paulo, Rio de Janeiro, and Belo Horizonte (Chaves, 2012).
Study participants were older people from the community in the FaMIdade Program at the Instituto Metodista Granbery in Juiz de Fora. This program is offered to the community in an effort to promote education and health through a series of activities and social interactions, such as information technology, pilates, hydrotherapy, literature classes, dance, strength training, functional gymnastics, culture, art discussions, and well-being lectures. Most participants were active older adults (over 60 years old) (Vasconcelos et al., 2016).
Eligibility Criteria
Inclusion criteria: participants must be (1) older persons (60 years or older, according to the WHO classification for developing countries); (2) regularly enrolled in the program’s activities; (3) achieving a score of 25 points (for older adults with 4 years of schooling or more) or 18 points (for older adults with less than 4 years of schooling) on the Mini-Mental State Examination administered at baseline (Lourenço & Veras, 2006).
Exclusion criteria: participants were excluded if they (1) were not available at the follow-up; (2) moved from the city of Juiz de Fora, Minas Gerais; (3) refused to continue their participation in the study; (4) were not found based on the recorded data; (5) passed away during the research period; and (6) were hospitalized and unable to respond to the assessment instruments.
Procedures
Two trained evaluators conducted pre-scheduled, in-person interviews in individual rooms either before or after the Famidade activities or at the participant’s home. Each interview was conducted in a single sitting and lasted approximately 1 hour. The interviews were conducted three times per individual: in 2015 (baseline collection – T0), in 2017 (after 2 years of follow-up – T1), and in 2019 (after 4 years of follow-up – T2).
Instruments
We used the same questionnaire for data collection in the three waves of the study to assess sociodemographic data, cognition, level of physical activity, mental health, and resilience. We have provided descriptions of these instruments below:
Sociodemographic data: We took into account the participants’ sex, age, marital status, years of schooling, tobacco use, family income, and ethnicity.
Number of comorbidities: Based on the sum of all self-reported diseases and was assessed using a predefined list of the most common diseases affecting older persons (e.g., diabetes, hypertension, etc.).
Mini-Mental State Examination (MMSE): The MMSE allows us to examine cognitive function, and is one of the most widely used and studied tests worldwide (Bertolucci et al., 1994; Folstein et al., 1975). The test was developed by Folstein et al. (1975) and has already been translated and validated for the Brazilian population (Bertolucci et al., 1994). As this study was conducted in a city in Minas Gerais, we decided to use the cutoff point specific to this state, which was published in a previous study (Lourenço & Veras, 2006). Therefore, older adults with four or more years of schooling should score at least 25 points, while those with less than 4 years of schooling had to score at least 18 points. Lower scores suggest cognitive impairment and were used as exclusion criteria from the study.
Lawton and Brody Scale: We used this scale to assess the instrumental activities of daily living. This instrument was adapted and translated to Portuguese by dos Santos and Virtuoso Júnior (2008) and has a score ranging from 9 to 27 points, where higher scores are associated with less dependence on other individuals to assist daily living activities.
Physical activity level: We used the International Physical Activity Questionnaire validated for Brazil (Matsudo et al., 2001), which was measured once for each wave. This instrument contains questions that assess the frequency (days per week) and duration (amount of time per day) of physical activity performed in the week prior to the interview. To classify the level of physical activity, we considered the criteria defined in the Guidelines for Data Processing and Analysis of the International Physical Activity Questionnaire (IPAQ) (IPAQ, 2005), which classifies physical activity levels as either Low, Moderate, or High. Participants were divided into two groups based on the following classification: (a) Regularly active individuals—those with Moderate or High levels of physical activity in all three waves of the study (i.e., fulfilling at least one of the following criteria: three or more days of vigorous-intensity activity and/or walking at least 30 minutes per day OR five or more days of moderate-intensity activity and/or walking least 30 minutes per day OR five or more days of any combination of walking or moderate- or vigorous-intensity activities) and (b) Intermittently active individuals—those with low levels of physical activity, as measured by the IPAQ short form, in at least one of the waves of this study (i.e., not meeting any of the criteria above) (IPAQ, 2005). IPAQ has already been validated specifically for older persons in Brazil (mean age=66.6 years old) and shows good agreement with pedometer measures and appropriate reproducibility (Benedetti et al., 2007).
Depression Anxiety Stress Scale (DASS 21): The DASS 21 scale was adapted and validated for the Portuguese language by Vignola and Tucci (2014). This scale comprises 21 questions rated on three 4-point Likert-type subscales. Each subscale contains seven items that assess depression, anxiety, and stress. The final result is obtained by adding the scores of all seven items for each of the three subscales. The scale provides three scores, one per subscale, where the minimum is 0 and the maximum is 21. Higher scores indicate worse mental health (Vignola & Tucci, 2014). In our sample, Cronbach’s alpha was 0.820.
Wagnild and Young’s Psychological Resilience Scale (RS25): Developed by Wagnild and Young (1993) to measure the levels of resilience, it contains 25 items with positive descriptions and Likert-type responses ranging from one (strongly disagree) to seven (strongly agree). The scale scores range from 25 to 175 points, where high values indicate high levels of resilience (Wagnild & Young, 1993). In 2005, Pesce et al. (2005) conducted the cross-cultural adaptation, reliability, and validity of the scale for its application in Brazil. In our sample, Cronbach’s alpha was 0.710.
Statistical analysis
As stated above, the participants were first divided into two groups: regularly active individuals (those who maintained an active IPAQ score for all three waves in the 4-year follow-up) and intermittently active individuals (those who had a sedentary or inactive score in all or at least one of the waves).
We compared the sociodemographic data between the groups using independent t-tests for continuous variables and chi-square tests for categorical variables. Similarly, we compared the scores for resilience and mental health between the groups using independent t-tests in each wave.
To verify the role of physical activity and the period on outcome variables, we performed four separate 2x3 repeated measures analysis of covariance (ANCOVA; physically active individuals [regular vs. intermittent] by the period [baseline, 2 years, and 4 years]) on each dependent variable: DASS 21 Depression, DASS 21 Anxiety, DASS 21 Stress, and Resilience. If the result was significant, we used a Bonferroni test for the subsequent post hoc analyses. Assumptions for this test were investigated and met, including the normality of residuals, sphericity (in the case of violation, Greenhouse–Geisser correction was used) and Homogeneity of variance (using Levene’s test). Covariates were included in the model if there were differences at p≤.10 level in the comparisons between groups using t-tests or chi-square tests.
Finally, to identify differences in the correlations (mental health-resilience) between the groups, we standardized the variables using Z-scores and adopted the methodology for testing the equality or homogeneity of regression slopes through an ANCOVA with these standardized variables, as the regression slopes for the standardized variables represent the correlations (More details of this procedure are available in https://www.ibm.com/support/pages/how-can-i-test-equality-correlations-between-two-variables-different-groups -cases).
We considered a value of p<0.05 to be significant and conducted all analyses using SPSS 21 (SPSS Inc).
Ethical aspects
This study was approved by the Research Ethics Committee of the Federal University of Juiz de Fora under Case no. 1.109.647, and all the participants signed an informed consent form.
Results
From a total of 396 older adults enrolled in the Famidade program, 312 were included at T0 (baseline – 2015), and 180 (58%) remained after 4 years of follow-up (responded to all three waves). Figure 1 illustrates the study flow diagram and demonstrates the losses throughout the follow-up period. The main reason for the loss in follow-up was the COVID-19 pandemic, as it was not possible to conduct interviews during the lockdown.
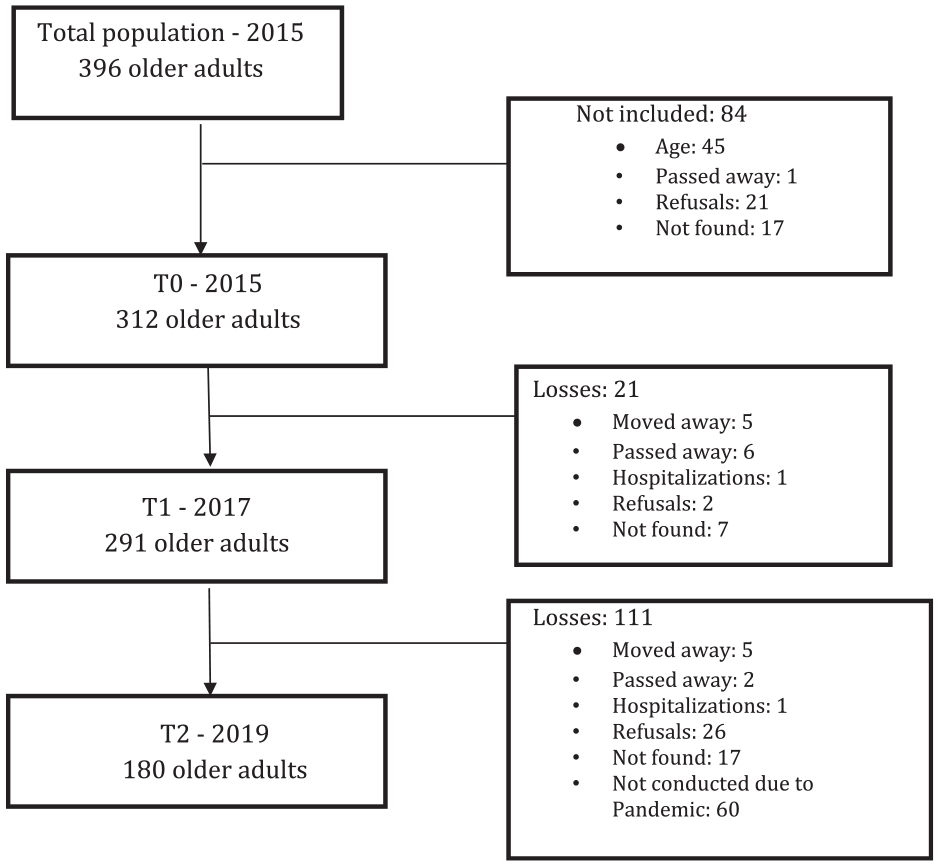
Study flow diagram.
Of the participants, 63 (35.0%) individuals maintained a physically active lifestyle in all 3 waves, 26 (14.4%) remained sedentary in all 3 waves, and 91 (50.6%) were either sedentary or inactive in at least one wave.
Table 1 presents the sociodemographic and clinical data. The majority of the older adults were female, identified ethnically as white, single, had 6 years of schooling, and a mean age of 69.6 years (SD: 6.3, ranging from 60 to 89 years old). There was a trend toward statistical significance for age (p=.074) and a statistically significant effect for instrumental activities of daily living (p=.003) between groups, which were included as covariates in the ANCOVA models. An attrition analysis was carried out comparing mental health, resilience, sociodemographic, and clinical data between those included in the study and those with missing data, which have shown significant results only for sex (greater drop out among women) (see Supplementary tables).
Comparison of sociodemographic and clinical data between regularly and intermittently active individuals.

1 Real (Brazilian currency) = 5 dollars.
Table 2 demonstrates the effects of physical activity and the period on different outcome variables. All assumptions were met, with the exception of Mauchly’s test for DASS Anxiety and DASS Stress. In these cases, Greenhouse–Geisser corrections were used. Concerning resilience, the 2 X 3 repeated measures ANCOVA, had a significant effect for the IPAQ group (F= 5.143,p=.025,η2 =.029), with higher levels for regularly active individuals. However, there was no significant main effect for the period*IPAQ interaction (F=.319,p=.727,η2 =.002), nor a main effect for the period (F=.222, p=.801,η2 =.001). In relation to DASS Depression, there was no significant effect for the IPAQ group (F=.747, p=.389, η2 =.004), the period*IPAQ interaction (F=.250, p=.779, η2 =.001) or the period (F=.426, p=.652,η2 =.002). A similar pattern was seen for DASS Anxiety, in which there were no significant differences for the IPAQ group (F=.384, p=.536, η2 = .002), the period*IPAQ interaction (F=1.507, p=.223, η2 =.008), or the period (F=1.693, p=.186, η2 =.010). This was also the same for DASS Stress, such that there were no significant differences for the IPAQ group (F=.134, p=.714, η2 =.001), the period*IPAQ interaction (F=.183, p=.833, η2 =.001) or the period (F=.626, p=.535,η2 =.004).
Repeated measures ANCOVA - Effects of physical activity and period on different outcome variables.

DASS 21: Depression Anxiety and Stress Scale.
Covariates: Age and Activities of daily living.
Table 3 compares mental health outcomes and resilience between the groups. There were no differences in the depression, anxiety, and stress scores in all three waves. However, resilience presented a significant trend at the baseline as well as 2 years of follow-up, and significance was shown for 4 years of follow-up.
Comparison of mental health outcomes and resilience between groups at baseline, 2 years, and 4 years.

DASS 21: Depression Anxiety and Stress Scale.
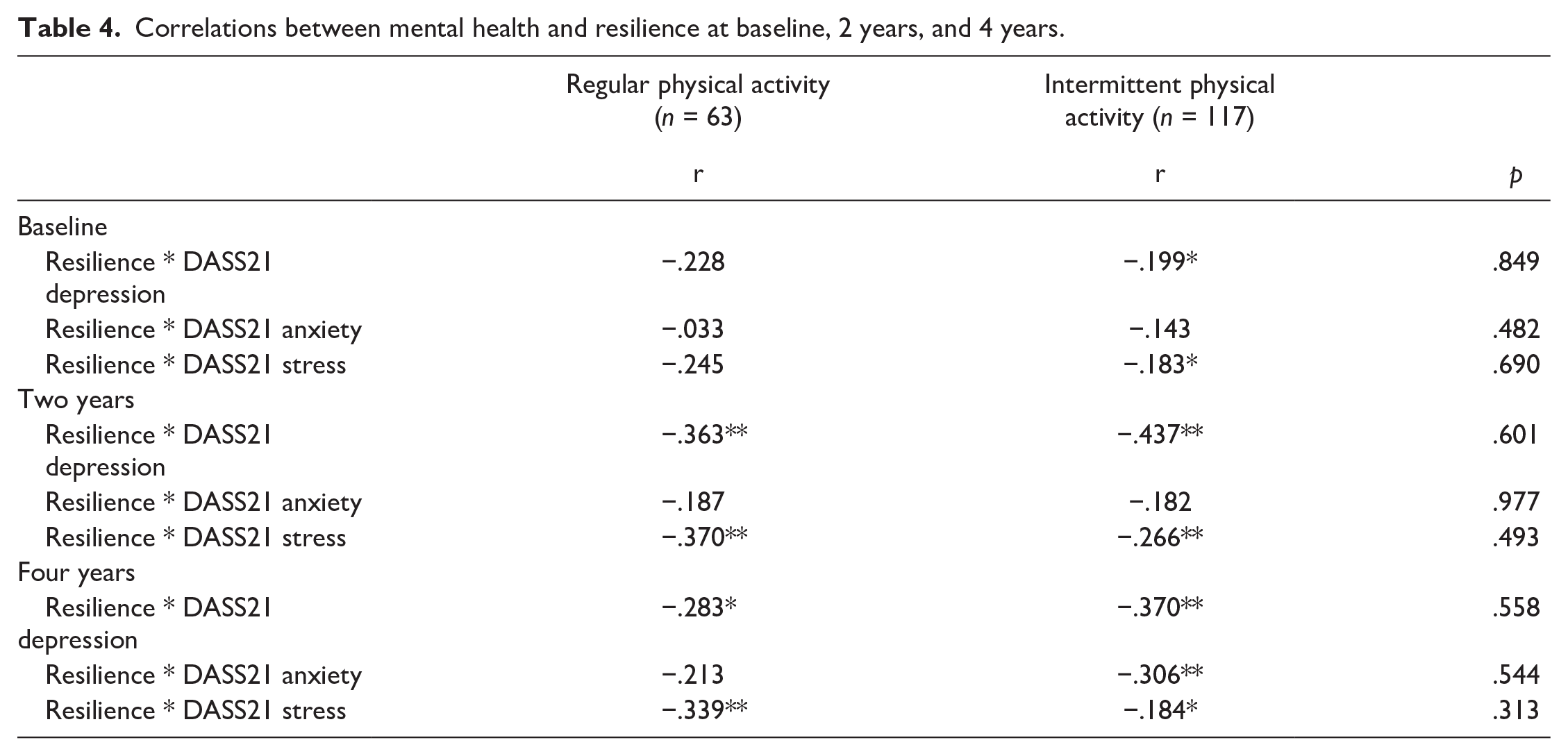
Finally, Table 4 shows the correlations between mental health and resilience. All correlation coefficients were negative, indicating an association between higher mental health problems and lower resilience scores. We observed this for both groups (regularly and intermittently active individuals). Nevertheless, there were no differences in these correlations between the groups.
Correlations between mental health and resilience at baseline, 2 years, and 4 years.
Discussion
The findings of this 4 year longitudinal study reveal some key differences between intermittently and regularly active individuals that should be considered in the assessment of older adults and that could help healthcare professionals develop future interventions and preventive measures.
Regarding our first hypothesis, we found that regularly active individuals were more resilient than intermittently active individuals. These results have been investigated by other studies that report that resilient older adults are more likely to be involved in activities, such as physical activity, which is often associated with successful aging (Resnick & Inguito, 2011B. A. Resnick & Inguito, 2011). This concept provides additional support for the idea that physically active older individuals can maintain their health and adapt to the challenges of aging more successfully (MacLeod et al., 2016; Resnick & Inguito, 2011B. A. Resnick & Inguito, 2011). In a systematic review by Notthoff et al. (2017), two psychological factors—motivation and self-efficacy—demonstrate a consistent association with higher levels of physical activity in the older population, and these factors are also directly related to the concept of resilience.
Our second hypothesis was not supported, as regularly active individuals did not present better mental health outcomes than intermittently active individuals, which contradicts the literature. Data from systematic reviews tend to report the beneficial effects of physical activity on mental health in longitudinal studies. A recent review of 111 studies and nearly three million individuals revealed that physical activity was associated with lower levels of depression. Nevertheless, about 35% of the studies were not significant (Dishman et al., 2021). Another systematic review on the subject, which included only longitudinal studies, evidenced that most studies tend to show the beneficial effects of physical activity on participants’ mental health. However, five of the 30 studies that were reviewed also reported non-significant results (Mammen & Faulkner, 2013). These differences may be related to the participants’ age (in our case, older adults with an average age of 70), the sample size, the instruments used, and the follow-up procedure. Since we compared only two categories—regular versus intermittent—not all of the older adults were inactive the entire period (since they needed to be inactive in at least one wave to be categorized as intermittent), and this may also have influenced our results. Another possible explanation is that, at baseline, only sex was significantly different between those participants with complete data and those who dropped out. Nevertheless, there was a tendency towards higher levels of resilience in participants with complete data. For this reason, the hypothesis that the remaining sample was a more resilient and healthier subset of the original sample should be considered as it may have impacted this hypothesis.
With regard to the third hypothesis, we found an inverse relationship between mental health symptoms and resilience among the participants. In a systematic review and meta-analysis published by our group in 2017, we found a moderate inverse correlation between depression and resilience, indicating the potential protective effect of resilience on depression in the older population, although all the articles included in the study were cross-sectional (Wermelinger Avila et al., 2017). This longitudinal study confirms this finding as it reveals a negative relationship between resilience and mental health, which suggests that older adults with more resilience have better mental health.
Finally, our last hypothesis was not supported, as we did not detect any differences in the mental health-resilience relationship between regularly and intermittently active individuals. These findings differ from those of previous studies that found physical activity to be a mediator in the relationship between resilience and mental health (Kukihara et al., 2018; Wermelinger Ávila et al., 2018, 2022), including one previous study carried out by our group (Wermelinger Ávila et al., 2022). In this particular study, we compared subcomponents of resilience between groups and verified that different subdimensions were used between the sufficiently (i.e., self-sufficiency and perseverance) and insufficiently active groups (i.e., meaning of life and existential) and that these subdimensions influenced the correlations.. However, when we examine the total resilience scores, the findings between that study and this study are similar. Thus, we believe that physical activity has a stronger relationship to the type of resilience used (i.e., equanimity, existential, and meaning of life) than to the relationship itself.
Nonetheless, this study presents some limitations. First, it was conducted through a program for the older population in a city in Brazil and multicenter studies are needed to further generalize the results. Second, programs for older persons, including the site where we collected data, generally have a large presence of functionally independent older individuals, specifically women. Further, the activities of the program itself may have influenced the resilience and mental health of the participants, thereby impacting the study results. Therefore, we recommend including other profiles of older adults in further longitudinal studies on the subject. Third, there was a loss of 59 older adults in the follow-up period between the second and third wave due to the COVID-19 pandemic, which began in Brazil in March 2020, as we were finalizing the third wave of data collection. The older population is considered a high-risk group for COVID-19. As this study evaluates factors that would have been influenced by the quarantine, such as anxiety, depression, stress, resilience, and physical activity, we could not fully complete data collection. Fourth, our analysis is subjected to type I error and should be interpreted with caution, since only the main effect of activity on resilience was found. Likewise, we used listwise deletion for those with missing data, which can be considered a limitation since the attrition rate can impact our statistical power to detect significant differences. Nevertheless, only sex was different between those with and without complete data. Fifth, the generalizability of these findings is limited by sample characteristics, which was mostly composed of white, female, single, and low education individuals. Finally, the IPAQ score evaluated the physical activity performed in the week prior to the interview and, for these reasons, caution should be made concerning inferences about the level of physical activity during a long period of time in these individuals. Within this context, it is possible that, for example, a “regularly active person” became ill somewhere during the first year of a 2-year period and had very little physical activity for a significant period of time, but had recovered to pre-illness levels of activity well before the end of the 2-year period where the IPAQ was administered. However, it is unlikely that a person would re-start physical activity before data collection in the three different waves. Considering “regularly active individuals” as those with moderate or high levels of physical activity in all three waves of the study may denote a consistent pattern of physical activity by the individual. It is also important to note that IPAQ has been already used by previous studies to represent longer periods of time (Li et al., 2020; Lima et al., 2011; Silva et al., 2020).
Despite these limitations, our study also has its strengths. To our knowledge, this is one of the first longitudinal studies at the international level to examine the relationship between resilience, mental health, and physical activity levels for a group of older adults over a 4-year period. By demonstrating that older adults who remained physically active were more resilient than sedentary older adults, this study reinforces the importance of research and interventions that promote physical activity in this age group and to consider its specificities. Finally, this study can contribute both to clinical practice and public policies by providing the basis for future interventions that seek to promote resilient individuals and successful aging.
Clinical Implications
Even with small effect sizes, our results suggest that those individuals who maintain regular physical activity may be more resilient. In fact, studies have shown that resilience and its related factors have implications for the development of public health interventions to maintain healthy behaviors in the older population (Clark et al., 2018). Therefore, it is possible to suggest that the incorporation of physical activity could be an alternative for promoting resilience among older adults (Jeste et al., 2013; Resnick & Inguito, 2011B. A. Resnick & Inguito, 2011). However, interventions designed to test the impact of physical activity and other lifestyle behaviors on resilience among older people are limited (MacLeod et al., 2016; Resnick & Inguito, 2011B. A. Resnick & Inguito, 2011). In 2019, Wiles et al. (2019) demonstrated that the resilience exhibited by older adults helps them maintain their well-being, autonomy, and quality of life, even when faced with challenges such as functional decline and multimorbidity. Another possibility of intervention is to promote coping skills, which may change the way older adults manage or overcome problems and difficulties (Van der Hallen et al., 2020). Previous studies have found that interventions promoting coping strategies have been associated with positive changes in physical activity status among older adults (Evers et al., 2012; Laybourne et al., 2011).
To prevent mental health changes, we need to do more than plan interventions aimed toward affected groups and make an effort to implement programs that prevent these changes and promote mental health (Prince et al., 2015). For instance, previous studies have shown that activity engagement is associated with greater levels of life satisfaction and purpose and lower levels of depression and loneliness (Smith et al., 2020), and leisure time physical activity could be associated with better mental health (Kim et al., 2020). These social activities could be a starting point to an intervention, which may stimulate a more structured and continuous physical activity in the future, thus having public health repercussions.
Conclusions
Individuals who maintained regular physical activity were more resilient than those who were intermittently active. However, no differences were observed for mental health outcomes, which has been shown in previous studies including older persons. One explanation for not finding an association is that the remaining sample (i.e., those with complete data) may be a more resilient and healthier subset of the original sample, which may have impacted our findings.
Although the correlation coefficients between resilience and mental health were negative, implying that individuals with higher levels of resilience had fewer mental health problems, there were no significant differences in the comparison between the groups based on their level of physical activity. These findings could help elucidate the underlying mechanisms of health outcomes affected by physical activity, which should be considered by healthcare professionals and administrators. Additionally, interventions that promote coping skills or increase resilience could be important strategies to implement for older adults, as it may increase the levels of physical activity and mental health altogether.
Supplemental Material
sj-pdf-1-jag-10.1177_07334648221095075 – Supplemental Material for Resilience and Mental Health Among Regularly and Intermittently Active Older Adults: Results From a Four-Year Longitudinal Study
Supplemental Material, sj-pdf-1-jag-10.1177_07334648221095075 for Resilience and Mental Health Among Regularly and Intermittently Active Older Adults: Results From a Four-Year Longitudinal Study by Maria Priscila Wermelinger Ávila, Jimilly Caputo Corrêa, Maria Clara de Castro Furtado Zaidem, Matheus Venancio Passos, Ana Paula Sena Lomba Vasconcelos, Alessandra Lamas Granero Lucchetti and Giancarlo Lucchetti in Journal of Applied Gerontology
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB Protocol
This study was approved by the Research Ethics Committee of the Federal University of Juiz de Fora under Case no. 1.109.647, and all the participants signed an informed consent form.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.