
Abstract
Objectives: Little is known about the contribution of positive psychological factors, such as purpose in life, to healthcare and financial decision making in aging. Here, we examined the relationship between purpose and decision making and tested the hypothesis that purpose benefits decision making, particularly when cognition is limited. Methods: Participants were 1081 community-based older adults without dementia. Healthcare and financial decision making was measured via a 12-item performance-based instrument. Purpose was measured via a 10-item scale. Results: In a linear regression model adjusted for age, sex, and education, higher global cognition was associated with better performance on the decision making measure, as expected. Purpose was not directly related to decision making. However, the interaction of purpose with cognition was significant, such that greater purpose was associated with better decision making among persons with lower cognition. Discussion: Purpose in life may promote better decision making among older adults with lower cognition.
Prior research examining the psychological correlates of healthcare and financial decision making in aging has focused almost exclusively on negative psychological factors while neglecting positive psychological factors.
In this study, we associated a key positive psychological factor, purpose in life, with better healthcare and financial decision making, specifically among non-demented older adults with lower cognition.
Depressive symptoms were not related to decision making; thus, in the current analyses, the positive psychological factor (purpose) entered more prominently into decision making than the negative psychological factor (depressive symptoms).
Purpose in life has promising therapeutic potential because it is modifiable, related to a host of favorable outcomes in older adults, and might be a novel target through which healthcare and financial decision making can be improved.
Because purpose benefited decision making at lower levels of cognition specifically, decision making interventions targeting purpose might be deployed on a selective basis, namely among non-demented older adults with limited raw mental computing power.
Introduction
Many older adults make suboptimal decisions when managing their healthcare and finances, and this can have serious and potentially catastrophic consequences on their health and financial standing (Agarwal et al., 2009; Brown & Ridderinkhof, 2009; Carpenter & Yoon, 2011; Finucane & Gullion, 2010; Lusardi & Mitchell, 2014). For example, debt mismanagement along with a shrinking social safety net has resulted in a record number of older Americans filing for bankruptcy in recent years (Lusardi & Tufano, 2009; Thorne et al., 2020). Thus, there is an urgent need for interventions that bolster healthcare and financial decision making among older adults. An important step toward the development of these interventions is the identification of modifiable factors through which decision making might be improved.
Prior studies of older adults have associated modifiable contextual, social, experiential, and psychological factors with healthcare and financial decision making and related outcomes like financial exploitation (Acierno et al., 2010; Beach et al., 2018; Glover et al., 2020; Hess et al., 2012; Liu et al., 2017; Stewart et al., 2018, 2020; Strough et al., 2015). Much of this work has examined the detrimental effect of negative psychological factors—that is, factors reflecting forms of psychological suffering, such as the sadness, disinterest, and fatigue that is characteristic of depression (Denburg et al., 2009; Lichtenberg et al., 2013, 2016, 2020; Nguyen et al., 2013). By contrast, very little is known about the impact of positive psychological factors—that is, factors reflecting aspects of psychological thriving—on decision making. This is an important gap in knowledge because positive psychological factors promote health and longevity independent of negative psychological factors and might similarly benefit decision making (Diener et al., 2017). In particular, purpose in life, which refers to one’s subjective sense of meaning, investment, and engagement in life experiences and events (Ryff, 2014), is robustly associated with a range of favorable health and financial outcomes (Boyle et al., 2009; Boyle, Buchman, & Bennett, 2010; Cohen et al., 2016; Hafez et al., 2018; Hill et al., 2016; Kim et al., 2014; Kim, Sun, Park, Kubzansky, et al., 2013; Kim, Sun, Park, & Peterson, 2013; Musich et al., 2018). Moreover, purpose can be derived from a wide variety of sources (e.g., volunteering; philanthropic-, educational-, or family-based activities), making it an attractive target through which healthcare and financial decision making might be improved.
In the current study, we investigated the relation of purpose in life with healthcare and financial decision making among 1081 community-based older adults without dementia from the Rush Memory and Aging Project (MAP) (Bennett et al., 2018). We focused on older adults without dementia because they generally continue to make healthcare and financial decisions independently and because older persons with dementia may have difficulty reliably self-assessing aspects of psychological functioning such as purpose. In addition to examining the direct association of purpose with decision making, we hypothesized that purpose interacts with cognition to impact decision making. This hypothesis was based on the notion that psychological and related factors play a particularly important role when cognitive (or other) resources needed for optimal decision making are limited. In the case of purpose, greater purpose might facilitate behavioral or neural mechanisms (e.g., putting forth extra effort, having better brain health) that benefit decision making when raw mental computing power is limited. Conversely, the impact of purpose on decision making might be nominal among older adults who can rely on strong cognitive abilities to make decisions. We also examined whether relations of purpose with decision making persisted after adjusting for depressive symptoms. We did so because depressive symptoms is an important negative psychological factor that has been previously implicated in decision making (Lichtenberg et al., 2013, 2016; Nguyen et al., 2013) and because purpose and depressive symptoms, although conceptually distinct, are negatively correlated (Boyle et al., 2009; Hedberg et al., 2010). Finally, in secondary analyses, we explored whether purpose is associated with decision making via its interaction with five specific cognitive domains (i.e., episodic memory, working memory, semantic memory, visuospatial ability, and perceptual speed).
Methods
Participants
The Rush Memory and Aging Project (MAP) is an ongoing, longitudinal, clinical-pathological study of aging and age-related diseases (Bennett et al., 2018). MAP participants are community-based older adults without known dementia who agree to structured annual clinical evaluations, blood draws, and donation of brain, spinal cord, nerve, and muscles at death. Recruitment occurs in continuous care facilities, retirement communities (i.e., independent living), Section 8 and Section 202 housing subsidized by the Department of Housing and Urban Development, local churches, and other social service agencies. Evaluations are performed as annual home visits. These design features facilitate follow-up participation (approximately 95%) and good representation of common comorbidities. Alzheimer’s dementia is documented annually using the criteria of the National Institute of Neurologic and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association, which requires a history of cognitive decline and impairment in memory and one or more additional cognitive domains (McKhann et al., 1984).
Written informed consent was obtained from participants following a detailed review of the risks and benefits of participation prior to study entry. MAP and the decision making substudy were approved by an Institutional Review Board of Rush (IRB protocol number 07071201).
Memory and Aging Project started in 1997, and a substudy assessing healthcare and financial decision making started in 2010. Of the 2102 participants with a MAP baseline evaluation, 642 died and 77 withdrew before the decision making assessment had begun. Another 68 participants moved or were ineligible due to severe comprehension or sensory limitations; 37 declined the decision making assessment; 87 had not yet completed the decision making assessment; and 3 completed the decision making assessment but had not yet received a clinical diagnosis. Among the remaining 1188 participants, 66 were diagnosed with dementia, and 41 had missing data. This left 1081 non-demented participants available for the current study.
Healthcare and Financial Decision Making
Decision making was measured via a 12-item version of a well-validated instrument that mimics the type of healthcare and financial decisions that older adults face on a fairly routine basis (Finucane & Gullion, 2010). Six items pertained to healthcare decisions and six pertained to financial decisions. On each item, participants viewed tables of information about either HMO plans or mutual funds and answered questions based on the tabulated information. For example, one of the financial items consisted of a table displaying four characteristics of three mutual funds (gross annual return, management fee, minimum investment, and years of activity) and provided participants the following preferences: “You want a mutual fund that has a management fee of less than 1% AND a gross annual return of over 6.5%. Based on the information in the table, which fund should you choose?” For each item, only one of the presented HMO plans or mutual funds met the sought-after preferences; thus, participants’ responses were either objectively correct or incorrect. The number of correct items was summed for each participant (range: 0–12, with higher scores indicating better performance on the decision making measure). The original decision making instrument has good short-term temporal stability and interrater reliability (Finucane & Gullion, 2010), and the current version has adequate internal consistency (α = .77) and has been shown to predict adverse health outcomes among older adults (Boyle et al., 2013; Stewart et al., 2018, 2019).
Purpose in Life
Purpose in life—defined as one’s subjective sense of direction, intentionality, and goal-directedness in current and future events and experiences—was measured using 10 items from Ryff’s Scales of Psychological Well-Being (Ryff & Keyes, 1995). Participants rated their agreement with each item along a 5-point scale (e.g., “I enjoy making plans for the future and working them to a reality”). Items were averaged for each participant (range: 1–5, with higher scores indicating greater purpose). This scale has adequate internal consistency (α = 0.82) and has been shown to forecast adverse health outcomes in aging (Boyle et al., 2009; Boyle, Buchman, Barnes, et al., 2010; Boyle, Buchman, & Bennett, 2010; Wilson et al., 2013; Wilson et al., 2018).
Cognition
Participants completed a neuropsychological battery made up of 19 individual tests, from which measures of global cognition and five specific cognitive domains were derived (Bennett et al., 2018). The five specific cognitive domains were episodic memory (seven tests: Word List Memory, Recall, and Recognition from the CERAD neuropsychological battery; immediate and delayed recall of Logical Memory Story A and the East Boston Story), working memory (three tests: Digit Span subtests [forward and backward] of the Wechsler Memory Scale-Revised and Digit Ordering), semantic memory (three tests: Category Fluency, Boston Naming, and the National Adult Reading Test), visuospatial ability (two tests: Judgment of Line Orientation and Standard Progressive Matrices), and perceptual speed (four tests: the oral version of the Symbol Digit Modalities Test, Number Comparison, Stroop Color Naming, and Stroop Word Reading). Raw scores on individual tests were converted to z scores using the baseline mean and standard deviation of the full MAP cohort. Global cognition was the average of the z scores of all 19 tests; this measure has good internal consistency (α = 0.89). The five specific cognitive domains were the average of the z scores of the tests in each cognitive domain; these measures were conceptually and empirically derived (Wilson et al., 2002).
Covariates
Age was determined relative to the date that participants completed the decision making measure. Participants reported their sex (male or female) and education (years of schooling) at their initial study evaluation. Because depressive symptoms are negatively correlated with purpose in life (Boyle et al., 2009; Hedberg et al., 2010), we also included the 10-item Center for Epidemiological Studies–Depression scale as a covariate; this scale has adequate internal consistency (α = 0.72).
Statistical Analysis
Bivariate associations of purpose in life, cognitive measures, and covariates with decision making were assessed via Pearson correlations, Spearman correlations, or t tests, as appropriate. Next, we examined associations of purpose, global cognition, and the interaction between purpose and global cognition with decision making via a series of multivariable linear regression models. We initially examined associations of age, sex, education with decision making (demographics only model). We then added terms for purpose and global cognition (direct effects model). Next, we added the term for the interaction between purpose and global cognition (core model). Finally, we added terms for depressive symptoms and the interaction between depressive symptoms and global cognition (full model). To determine whether interactions were general or specific with respect to cognition, in secondary analyses, we reran the above models with global cognition replaced by one of the specific cognitive domains. This was done separately for each of the five specific cognitive domains.
Results
Participants’ mean age was 81.0 years (SD = 7.5, range: 58.8–100.8), and their mean score on the Mini-Mental State Examination was 28.3 (SD = 1.7, range: 17–30). Please see Table 1 for additional descriptive information about the participants (also, please see Table S1 in the Supplemental Materials for descriptive information by age group). Younger age, more years of education, greater purpose in life, fewer depressive symptoms, and higher cognitive functions were associated with better performance on the decision making measure (Table 2). Males tended to score higher on the decision making measure than females (Mmales = 8.7, SDmales = 2.4; Mfemales = 7.7, SDfemales = 2.7; t(1079) = −5.0, p < .001). Also worth mention, greater purpose was associated with fewer depressive symptoms (r = −.30, p <.001) (please see Table S2 for bivariate associations between all study variables).
Descriptive Characteristics of the Group.
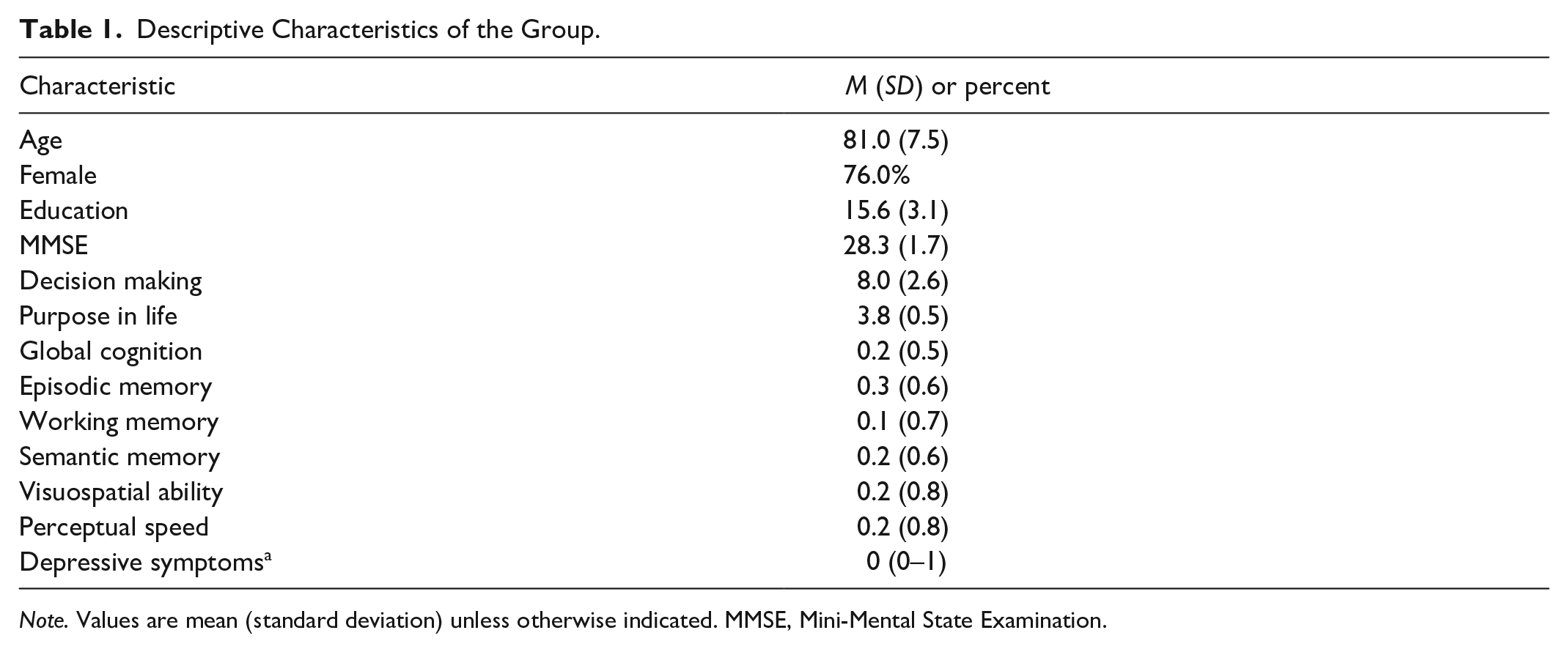
Note. Values are mean (standard deviation) unless otherwise indicated. MMSE, Mini-Mental State Examination.
Median (interquartile range).
Bivariate Associations of Descriptive Characteristics with Healthcare and Financial Decision Making.

Note. Values are Pearson correlation coefficient (p value) unless otherwise indicated.
Spearman correlation coefficient (p value).
Associations of Purpose in Life, Cognition, and the Interaction of Purpose and Cognition with Healthcare and Financial Decision Making
In the demographics only model, younger age, male sex, and more years of education were each associated with better performance on the decision making measure (please see Table S3 for expanded results of all regression models). In the direct effects model that included terms for purpose in life and global cognition, higher global cognition was related to better decision making (β = 2.43, SE = .14, p < .001), but purpose was not related to decision making (β = 0.07, SE = 0.14, p = .61). In the core model that included a term for the interaction between purpose and cognition, the interaction was significant (β = −0.89, SE = 0.24, p < .001; Table 3), such that greater purpose was associated with better decision making among persons with lower global cognition (Figure 1). In the full model that additionally adjusted for depressive symptoms and the interaction between depressive symptoms and global cognition, the interaction between purpose and cognition in relation to decision making persisted (β = −1.02, SE = 0.26, p < .001); however, neither depressive symptoms nor the interaction between depressive symptoms and global cognition were associated with decision making (depressive symptoms: β = −0.02, SE = 0.05, p = .73; depressive symptoms x global cognition: β = −0.12, SE = 0.09, p = .18; Table 3).
Associations of Purpose in Life, Cognition, and the Interaction of Purpose and Cognition with Healthcare and Financial Decision Making.
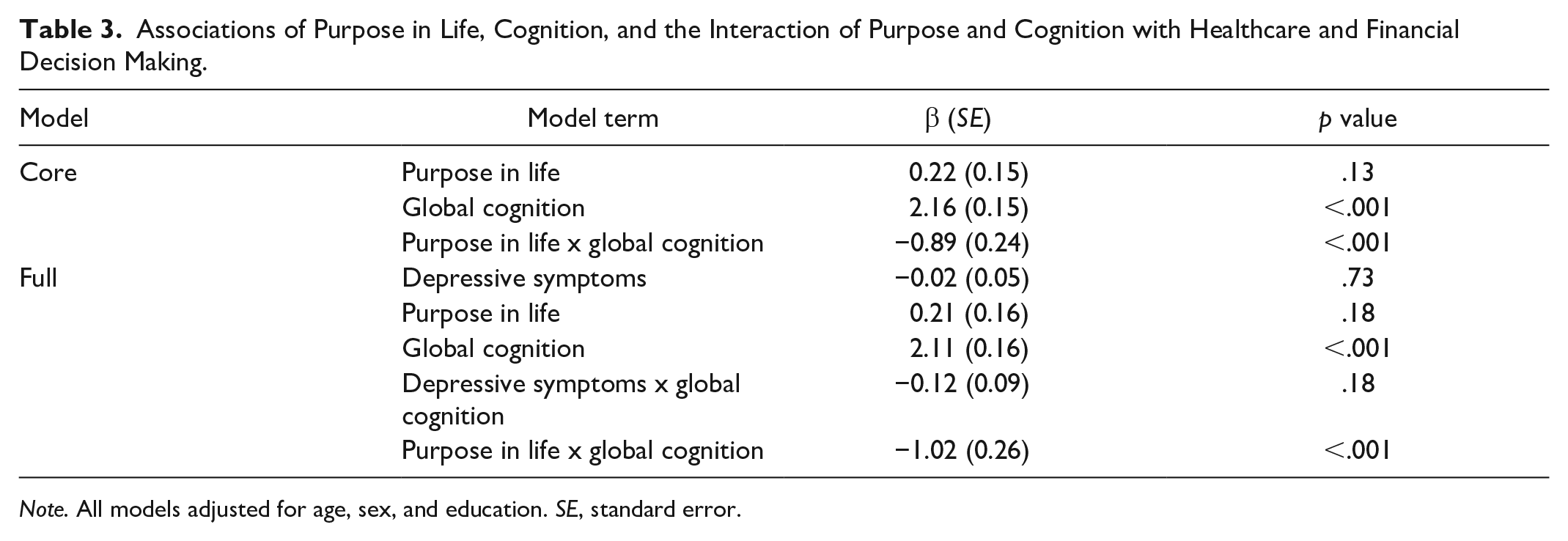
Note. All models adjusted for age, sex, and education. SE, standard error.
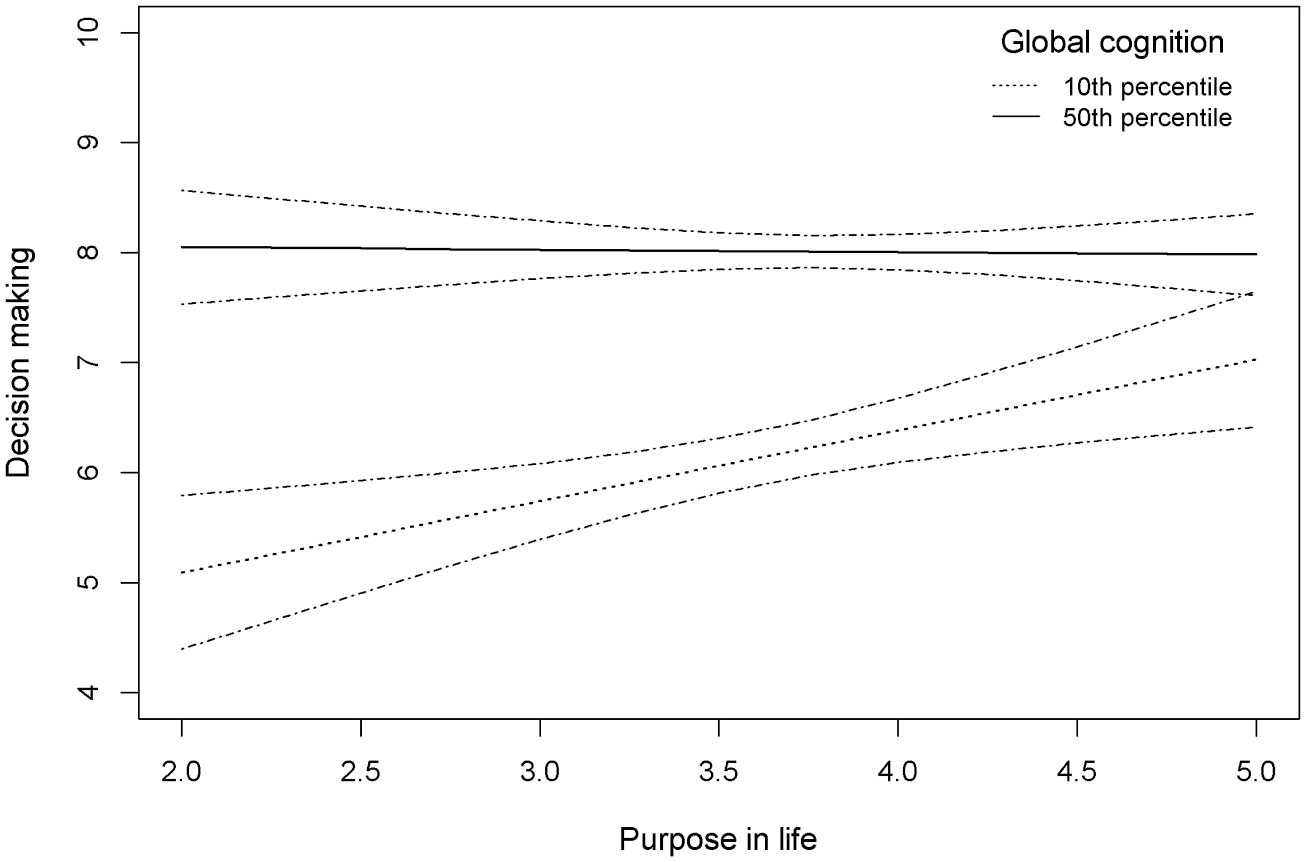
Association of purpose in life with decision making at the 10th and 50th percentiles of global cognition, with 95% confidence bands, adjusted for age, sex, and education.
In secondary analyses that adjusted for age, sex, and education, we examined interactions between purpose and the five specific cognitive domains in relation to decision making. These analyses revealed significant interactions of purpose with episodic memory (β = −0.47, SE = 0.21, p = .03), working memory (β = −0.48, SE = 0.18, p = .01), and perceptual speed (β = −0.58, SE = 0.16, p < .001), such that greater purpose was associated with better decision making among persons with lower episodic memory, working memory, and perceptual speed. Interactions were not found between purpose and semantic memory or purpose and visuospatial ability. The interactions of purpose with episodic memory, working memory, and perceptual speed persisted in models that additionally adjusted for depressive symptoms and the interaction between depressive symptoms and the respective cognitive domain.
Discussion
The current study addressed the relation of purpose in life with healthcare and financial decision making among community-based older adults without dementia. Although purpose was not directly related to decision making, purpose interacted with cognition to impact decision making. Specifically, purpose benefited performance on the decision making measure among persons with relatively low global cognition. This finding persisted after further adjusting for depressive symptoms and the interaction between depressive symptoms and global cognition. We additionally examined interactions of purpose with specific cognitive domains in relation to decision making and found that purpose benefited decision making among persons with relatively low episodic memory, working memory, and processing speed. This study suggests that a sense of meaning, intentionality, and goal-directedness in life promotes better decision making among older adults with lower cognitive function.
Prior research examining the psychological correlates of healthcare and financial decision making in older adults has focused almost exclusively on negative psychological factors while neglecting positive psychological factors (Denburg et al., 2009; Lichtenberg et al., 2013, 2016, 2020; Nguyen et al., 2013). The current study directly addresses this gap, providing clear evidence as to the relevance of purpose in life to decision making. In fact, in our full model, purpose interacted with global cognition in relation to decision making; however, neither depressive symptoms nor the interaction of depressive symptoms with cognition were related to decision making. Thus, in the current analyses, the positive psychological factor (purpose) entered more prominently into decision making than the negative psychological factor (depressive symptoms). The present study also builds upon studies showing that experimentally-induced positive affect facilitates complex decision making (Carpenter et al., 2013; Isen, 2001). Notably, purpose in life and positive affect represent conceptually distinct subcomponents of overall well-being, with purpose reflecting eudaimonia (i.e., pursing and realizing personal virtues) and positive affect reflecting hedonia (i.e., feeling good when satisfying needs). Moreover, eudaimonia and hedonia are psychometrically dissociable, have distinct temporal characteristics (eudaimonia is trait-like; hedonia is state-like), and differentially impact physiology and health (Ryff, 2014; Ryff et al., 2016; Ryff & Keyes, 1995). This raises the possibility that purpose, positive affect, or other positive psychological factors could additively or synergistically benefit decision making among older adults with lower cognition.
The basis of the beneficial effect of purpose on decision making in the setting of low cognition is unknown. One possibility is that, through goal-setting, planning, and regularly engaging their surroundings, individuals with greater purpose establish behaviors that foster good decision making (e.g., maintaining a healthy diet, regularly monitoring financial assets), or they more readily accrue general knowledge or domain-specific knowledge about health/healthcare and finances in everyday life (Pinquart, 2002; Ryff et al., 2016). Another possibility is that purpose enhances motivation-related aspects of information processing during decision making. For example, if individuals with high purpose perceive healthcare and financial decisions as highly self-relevant (e.g., essential to realizing their goals), they might deploy extra mental effort to more thoroughly process available health and financial information or to more fully leverage their health and financial knowledge when making decisions (Hess, 2014; Hess et al., 2012, 2016; Jin et al., 2019). Also worth noting, purpose has been related to important disease biomarkers (e.g., salivary cortisol, proinflammatory cytokine interleukin-6 and C-reactive protein) and therefore might benefit decision making by optimizing biologic systems (Ryff et al., 2016). In particular, emerging evidence suggests that purpose plays a role in reducing cerebrovascular burden and enhancing neural efficiency or compensation despite accumulating Alzheimer’s disease pathology (Boyle, Buchman, Barnes, et al., 2010; Boyle et al., 2012; Kim, Sun, Park, & Peterson, 2013; Yu et al., 2015); thus, purpose might benefit decision making in the face of low cognition through better brain health or brain reserve. While much remains to be learned, the interaction between purpose and cognition in relation to decision making suggests that the underlying mechanism becomes increasingly important as cognitive resources diminish, particularly with respect to episodic memory, working memory, and perceptual speed.
From an intervention perspective, purpose in life has promising therapeutic potential because it is modifiable, related to a host of favorable outcomes in older adults, and might address the essential role of motivation in healthcare and financial decision making and related behaviors (Musich et al., 2018; Pinquart, 2002; Ryff et al., 2016). Regarding the latter, it is well known that low motivation can undermine behaviors that would otherwise improve decision making. For example, even when provided for free by employers, attendance at financial education programs is very low, and motivational barriers are thought to be a primary culprit (e.g., learning to manage complex finances is perceived as uninteresting or not worth the effort) (Duflo & Saez, 2003). Motivational interviewing techniques are specifically designed to address ambivalence to behavior change and could be tailored to target purpose by helping older adults define their life ambitions in concrete terms and then exploring how good healthcare and financial decision making supports their ambitions (Strough et al., 2015). In turn, greater purpose may promote supportive behaviors proximate to healthcare and financial decision making (e.g., attending health fairs and financial education programs, deploying extra mental effort when processing health- and financial-related information). Of note, the interaction of purpose with cognition suggests that purpose interventions should be deployed on a selective basis, namely when cognition is low.
The current study has strengths and limitations. A primary strength is our large and well-characterized group of older adults. In particular, the careful exclusion of dementia is important because older adults without dementia generally continue to make healthcare and financial decisions independently, whereas most (but not all) older adults with manifest dementia have stopped making these decisions on an entirely independent basis. One limitation is that our participants were self-selected and predominantly white, highly educated, and recruited from retirement communities; thus, they are only a proxy of older adults in general. We are collecting decision making data among older African Americans and can begin to address generalization to this group once enough data has accrued. This limitation also underscores the need for population-based studies on decision making in aging. Another limitation of the current study is its cross-sectional design, which precludes the establishment of directional relations between purpose and decision making. We are collecting decision making data longitudinally in MAP and will be able to investigate the issue of directionality as our follow-up interval lengthens. Future research also needs to address how personal values and specific situations interplay with purpose in life (and other psychological variables) to affect decision making, as this will be key in translating the current findings to real world scenarios.
Supplemental Material
sj-docx-1-jag-10.1177_07334648221095514 – Supplemental material for Purpose in Life and Cognition Interact to Impact Healthcare and Financial Decision Making in Old Age
Supplemental material, sj-docx-1-jag-10.1177_07334648221095514 for Purpose in Life and Cognition Interact to Impact Healthcare and Financial Decision Making in Old Age by Christopher C. Stewart, Lei Yu, Crystal M. Glover, David A. Bennett, Robert S. Wilson and Patricia A. Boyle in Journal of Applied Gerontology
Footnotes
Acknowledgements
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Aging at the National Institutes of Health [R01 AG017917 to D.A.B. and R01 AG033678, R01 AG034374, and R01 AG060376 to P.A.B.].
IRB Statement
This study was approved by an Institutional Review Board of Rush University Medical Center (IRB protocol number 07071201).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.