
Abstract
The fall experiences of older adults living alone lead to restrictions in their social participation. This study aimed to examine the factors that influence functional disability in social participation (FSP) among older adults who live alone and have experienced falls. This study used secondary data of 493 older adults living alone who experienced a fall, which were collected from the 2017 National Survey of Older Koreans. Multiple linear regression analyses were performed. Factors, such as old age, sex, economic status, frequency of drinking, and number of acquaintances, significantly related to functional disability in terms of social participation. In addition, poor muscle strength, depression, and cognitive decline comprised predictors of FSP. The findings of this study revealed that it is important to comprehensively evaluate the social participation of older adults who live alone and have experienced falls.
What this paper adds
Functional disability should consider aspects of social participation. Social participation is an important determinant of how older adults’ function after falling when they live alone. Factors related to functional disability in social participation were verified using the International Classification of Functioning, Disability, and Health (ICF) model.
Applications of study findings
Social resources can be provided, reflecting personal and environmental factors. Tailored intervention programs specific to function in social participation can be developed considering multifunctional factors. Policies can be made to improve older adults’ social participation.
Introduction
Fall experiences may result in disabilities in both personal and social functioning among older adults living alone (Leonardi et al., 2006). Disability in personal functioning involves difficulties in performing personal activities, such as activities of daily living (ADLs) and instrumental activities of daily living (IADLs) (Das Gupta et al., 2020; Kim et al., 2013; Lee & Shinkai, 2003; Wang et al., 2013). On the other hand, disability in social functioning is defined as difficulties in social participation (World Health Organization [WHO], 2001). Evidence shows that limitations in social participation can be the first sign of loss of independence in older adults (Whiteneck & Dijkers, 2009). Functional disability in social participation (FSP) is closely related to one’s ability to perform personal activities (Kim et al., 2012; Tomioka et al., 2017; Tomioka et al., 2018) and is known to predict death (Dale et al., 2012). The functional aspect of social participation is considered one of the key dimensions for older adults to account for their interactions with the world (Bukov et al., 2002). Moreover, social participation may be critical for vulnerable populations, such as older adults living alone with a fall experience (Aris et al., 2009; Stahl et al., 2017; Sun et al., 2011).
Fall experiences have a significant causal relationship with the occurrence of functional disabilities (Gill et al., 2013a). After a fall, older adults are often admitted to long-term care facilities due to functional disability (Gill et al., 2013b; Tinetti & Williams, 1997), and this phenomenon is on the rise worldwide (James et al., 2020; Kannus et al., 2005). In particular, fall experience is related to functional disability in terms of older adults’ ability to perform personal activities (Gill et al., 2013b; Tinetti & Williams, 1998) and social participation (Pin & Spini, 2016). Living alone is one of the significant risk factors for falling (Petersen et al., 2020). In South Korea, 20.6% of older adults who have experienced falls live alone (Ministry of Health and Welfare and Korea Institute of Health and Social Affairs, 2017). Older people living alone are at a high risk of developing functional disability due to falls (Ek et al., 2019; Elliott et al., 2009). However, FSP among older adults living alone with fall experience remains underexplored (Petersen et al., 2020).
Several previous studies have reported that personal factors (old age, low education, and smoking), health conditions (chronic diseases and low level of subjective health status), and environmental factors (weak social support and living conditions) are negatively related to functional disability in terms of performing personal activities or social participation (Fried et al., 2001; Levasseur et al., 2015). In addition, the decline of physical, psychological, and mental functions can act as a factor causing functional disability (Fu et al., 2018; van der Vorst et al., 2016). These factors are also related to disability due to falls (Dionyssiotis, 2012). In particular, it is speculated that FSP may gradually amplify after falls. Pin and Spini (2016) reported that those who fell were less likely to engage in long-term social participation than those who did not, based on a sample of 16,583 people aged 50–95 years. However, few studies have examined the factors that influence FSP among older adults living alone with fall experience.
The term “functional disability” has been used either narrowly or broadly in previous studies (Piškur, 2013; Whiteneck & Dijkers, 2009). It has often been defined and measured only in terms of difficulties in performing personal activities (Kim et al., 2013; Lee & Shinkai, 2003; Wang et al., 2013), while few studies have focused on FSP. However, the International Classification of Functioning, Disability, and Health (ICF) model (WHO, 2001) defines functional disability broadly and explains it according to two aspects: “activities” as the personal aspect of functioning, and “participation” as the social aspect of functioning. Specifically, social participation is defined as the activities required to participate in social life, and personal activity is defined as the execution of a task or action by an individual (WHO, 2001). The ICF model is a revised version of the International Classification of Impairment, Disabilities, and Handicaps (ICIDH) and is developed for the application of a variety of health conditions. It includes various dimensions (physical, psychological, and mental) and components (personal, environmental, health, and body function) that affect disability. Thus, this study aimed to identify the predictors of FSP among older adults living alone with fall experience based on the ICF model.
Methods
Design
This cross-sectional study used secondary data from the 2017 National Survey of Older Koreans (Ministry of Health and Welfare and Korea Institute of Health and Social Affairs, 2017) to identify factors influencing FSP of older adults living alone after falling. The study variables included in the ICF model (WHO, 2001) were background characteristics (personal factors, environmental factors, and health conditions), multidimensional functions (physical, psychological, and mental), and functional disability in terms of performing physical activities and social participation.
Study Participants
The National Survey of Older Koreans is a nationwide survey conducted by the Ministry of Health and Welfare every 3 years. We used the fourth survey data of the National Survey of Older Koreans, which included 10,299 individuals aged ≥65 years in 2017 (Ministry of Health and Welfare and Korea Institute of Health and Social Affairs, 2017). From the 10,299 respondents, 493 older adults living alone with a fall experience (i.e., those who had fallen down, slipped, or flopped down) in the past year were selected and analyzed in this study.
Measurements
Background Characteristics
Personal, environmental, and health conditions were evaluated to determine the background characteristics of the participants.
Demographic and socioeconomic characteristics (sex, age, level of education, and economic status) and lifestyle (smoking, drinking, and exercise) were examined to assess the participants’ personal factors. Age, educational level, and economic status were measured on a continuous scale. Economic status was measured by asking, “What is your total annual income?” Thereafter, economic status was sorted in ascending order by annual personal income and divided into five categories, so that each group contained 20% of the participants. Drinking was measured by the question, “How often have you been drinking in the past year?” Additionally, the average exercise time per week was measured after determining whether the participants exercised regularly or not.
Environmental factors included social support and living conditions. Social support was measured by the number of close acquaintances. The number of close acquaintances was measured by the sum of the number of relatives and friends, including siblings. Living conditions were measured by the enumerator by asking, “Do you think that the senior citizen’s house is comfortable for the senior citizen to live in?” The answers were categorized as “comfortable” or “uncomfortable.”
Health conditions were measured as a continuous variable using the total number of chronic diseases (more than 3 months after the doctor’s diagnosis).
Multidimensional Functions
To measure multidimensional functions, the physical function and structure, psychological function, and mental function were evaluated. The physical function and structure included muscle strength and nutritional status. Muscle strength was measured as the ability to perform the sit-to-stand (STS) movement from a chair or bed five times (Rikli & Jones, 1999) as an ordinal variable. Body mass index (BMI) was used to evaluate the nutritional status. BMI was classified as underweight (less than 18.5 kg/m2), normal (18.5 kg/m2 and more but less than ≺ 25 kg/m2), or obese (25 kg/m2 and more) (Ministry of Health and Welfare and Korea Institute of Health and Social Affairs, 2017).
To measure the psychological functions, the 15-item Geriatric Depression Scale-Short Form Korean Version (GDSSF-K) (Sheikh & Yesavage, 1986) was used. The total score ranged from 0 to 15 points. A score of less than eight points was classified as “normal” and that of eight points or more was classified as “depressed” (Ministry of Health and Welfare and Korea Institute of Health and Social Affairs, 2017). There is evidence supporting the construct and criterion-related validity of the GDSSF-K (Sheikh & Yesavage, 1986); Cronbach’s alpha was 0.88 in a previous study (Sheikh & Yesavage, 1986) and 0.90 in the present study.
The 19-item Mini-Mental State Examination for Dementia Screening (MMSE-DS) (Kim et al., 2010) was used to measure mental function. The total score had a range of 0–30. The cutoff scores for mental function were defined differently by age, gender, and educational level for “normal cognition.” Higher scores indicated higher mental function. There is evidence supporting the validity of the MMSE-DS (Kim et al., 2010); Cronbach’s alpha was 0.82 in a previous study and 0.82 in the present study.
Functional Disability
To assess functional disability, functional disability in terms of social participation and personal activity was measured.
FSP was measured using the following question: “Have you participated in learning or studying activities, social clubs (club activities), networking groups, and volunteering activities?” The response options were as follows: 1 = more than four times a week, 2 = two to three times a week, 3 = once a week, 4 = once a week, 5 = once a month, 6 = less than once a month, and 7 = no participation. In this study, the Kaiser-Meyer-Olkin (KMO = 0.596) value, Bartlett’s chi-square test (p < .001), and scree test (Cattell, 1966) were used to confirm the validity of the questionnaire, and the average scores of the individual items from the raw data were used for analysis. Higher scores indicated higher levels of FSP.
Functional disability in personal activities (FPA) was measured using the ADLs and IADLs. The seven-item Korean ADLs scale and the 10-item Korean IADLs scale were used (Won et al., 2002). When using both scales, respondents were asked to select one of the following responses: completely independent, need partial help, or need help completely. Three questions (deciding to purchase something, calling and receiving calls, and using means of transportation) among the IADLs were categorized as follows: completely independent, requiring little help, requiring a lot of help, and requiring help completely. In this study, factor analysis was performed on the 17 items of the ADLs and IADLs scales while confirming the validity (RMSEA = 0.063, 90% CI [0.060–0.066], CFI = 0.975, TLI = 0.971) of the FPA. The average score for each item from the raw data was used for analysis. Higher scores indicated higher levels of FPA. There is evidence supporting the validity of the Korean IADLs (Won et al., 2002); Cronbach’s alpha was 0.94 in a previous study and 0.86 for IADLs in the present study.
Ethical Considerations
The 2017 National Survey of Older Koreans was obtained without personal identification information after approving from the Korea Institute for Health and Social Affairs. In addition, this study was approved by the Institutional Review Board (IRB No.: E2008/001-004) of Seoul National University.
Data Analysis
IBM’s SPSS Statistics (version 23.0) and MPLUS 7.0 (Muthén & Muthén, 1998–2017) were used for the statistical analyses in this study. To explain the characteristics of the participants, descriptive statistics included means with standard deviations (SDs) for numeric variables and proportions with percentages for categorical variables. To examine the differences in functional disability (in both personal activities and social participation) between participants, an independent t-test and analysis of variance (ANOVA) were used for numeric and categorical data, respectively. For ANOVA, the Bonferroni post hoc test was used. Multiple linear regression was used to identify the factors related to functional disability.
Results
Participants’ Background Characteristics and Functional Disability (N = 493).

Note. FSP, functional disability in social participation; FPA = functional disability in personal activities; KRW = South Korean Won; *average exercise time per week. †Significant level p <.05, p <.01, p <.001.
Differences in Multidimensional Functions Based on Functional Disability
Comparisons of Multidimensional Functions by Functional Disability (N = 493).
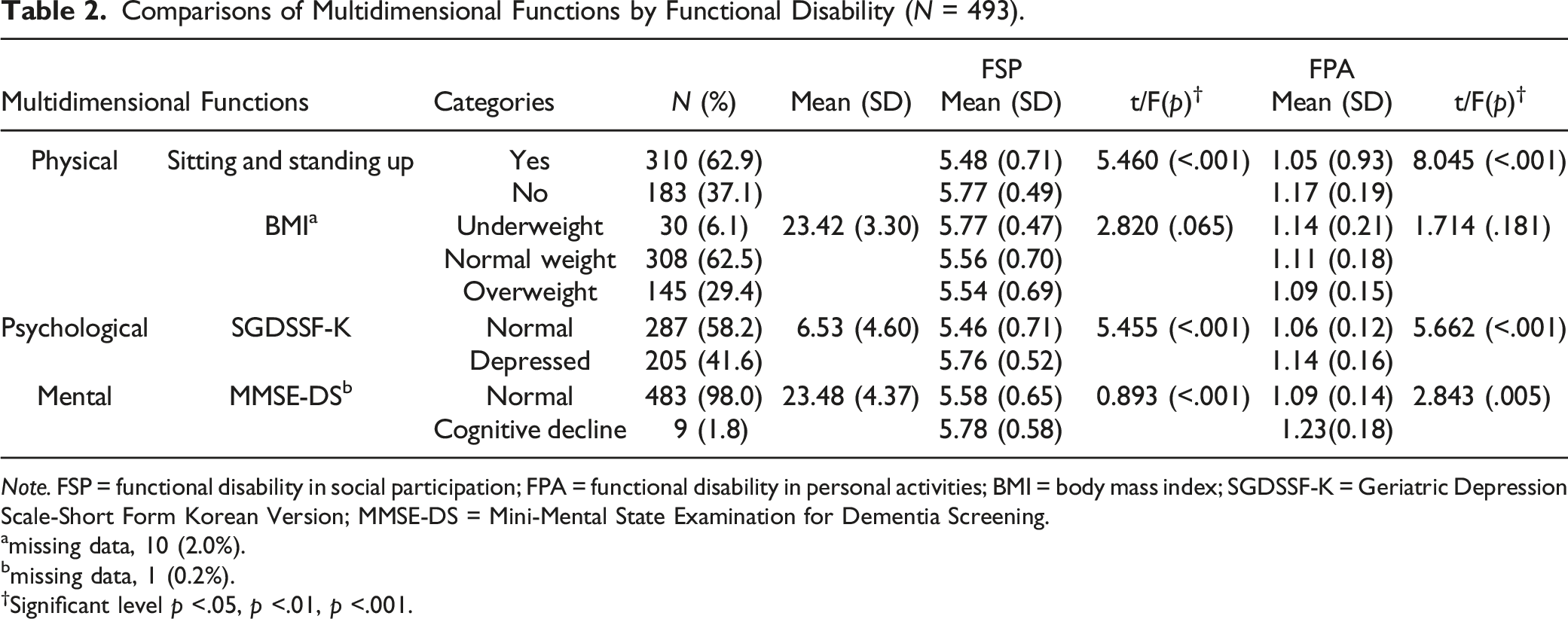
Note. FSP = functional disability in social participation; FPA = functional disability in personal activities; BMI = body mass index; SGDSSF-K = Geriatric Depression Scale-Short Form Korean Version; MMSE-DS = Mini-Mental State Examination for Dementia Screening.
amissing data, 10 (2.0%).
bmissing data, 1 (0.2%).
†Significant level p <.05, p <.01, p <.001.
Factors Related to Functional Disability in Social Participation
Factors Related to Functional Disability in Social Participation (N = 490).
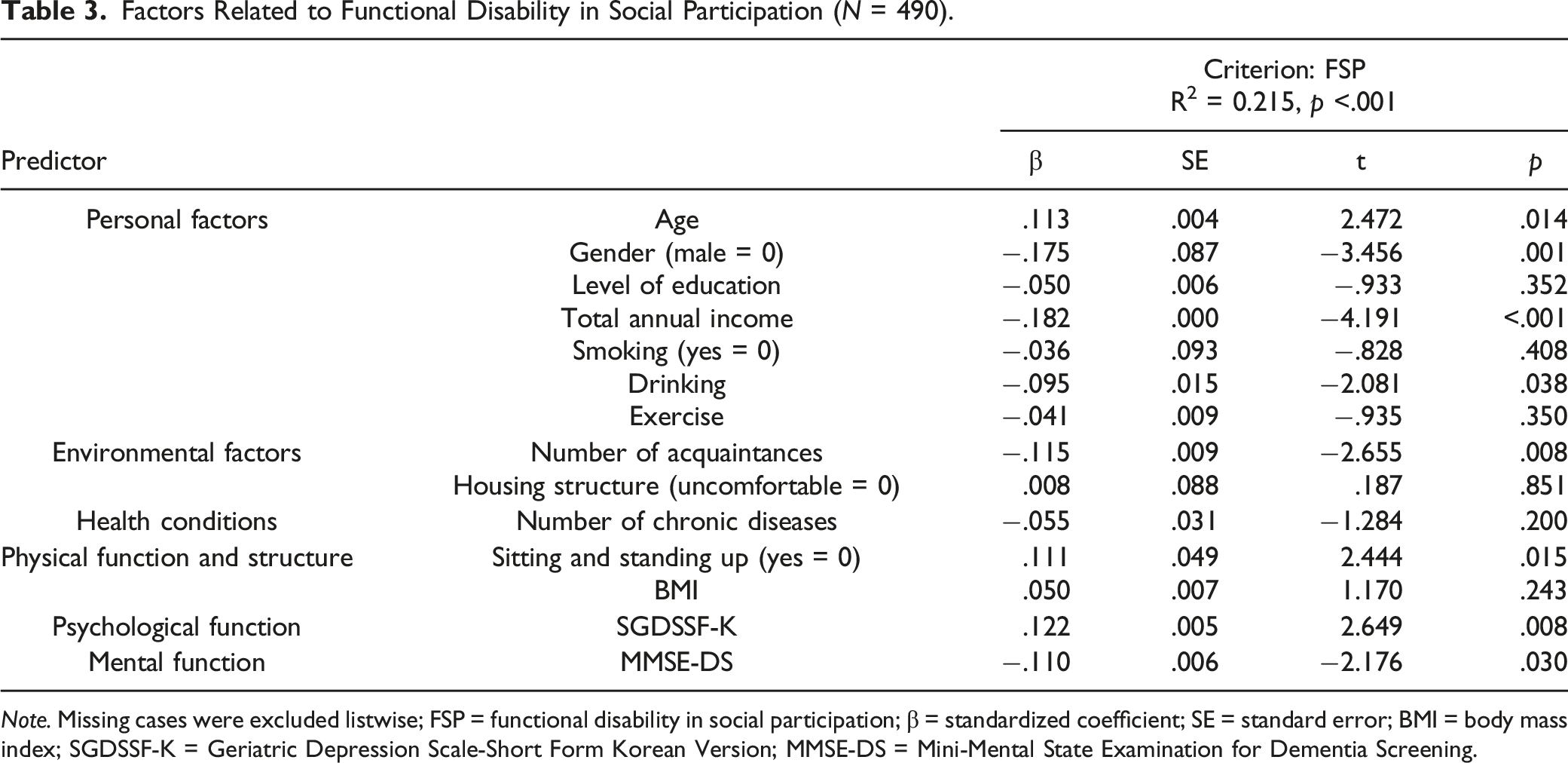
Note. Missing cases were excluded listwise; FSP = functional disability in social participation; β = standardized coefficient; SE = standard error; BMI = body mass index; SGDSSF-K = Geriatric Depression Scale-Short Form Korean Version; MMSE-DS = Mini-Mental State Examination for Dementia Screening.
Discussion
Older adults living alone are vulnerable to falls (Elliott et al., 2009). Previous studies have reported a relationship between falls and living alone in older adults (Petersen et al., 2020). Falls restrict social participation (Pin & Spini, 2016). However, few studies have examined the factors associated with social participation of older adults living alone with a fall experience. This study revealed that personal factors such as old age, low economic status, and male sex were significantly related to FSP. In previous studies, a low frequency of social activities has been observed among older people living alone, especially among those who are older and poorer (Chan et al., 2020; Tong et al., 2019). In addition, evidence suggests that gender influences the level of social participation, depending on the area in which they live (Levasseur et al., 2015; Naud et al., 2019). Older men living alone have shown a lower level of social participation than older women living alone (von Heideken Wågert et al., 2020). The findings demand attention to address the functional disability of economically vulnerable older men living alone with fall experience because they are at a high risk of being disconnected from interactive activities. It is critical to assess their needs and tailor interventions while considering their residential environment.
In this study, environmental factors such as the number of close acquaintances were found to be significantly associated with FSP. Previous studies have also shown that an individual’s acquaintances are significantly correlated with social participation (Nicklett et al., 2017). Using national survey data (Ministry of Health and Welfare and Korea Institute of Health and Social Affairs, 2017), this study found that only 20.6% of participants living alone had a fall experience. Among them, 33.5% did not have close acquaintances. This percentage was slightly higher than that of older adults living alone. The development of interventions is necessary to improve the social networks of older individuals having experienced falls that live alone.
With regard to multidimensional functions, this study found that poor muscle strength, which affects the ability to sit and stand up; depression; and cognitive decline were significant predictors of FSP in older adults living alone with fall experience. According to Tinetti et al. (1995), impairments in multiple domains (poor muscle strength, sensory impairment, and high depression scores) are related to functional dependency. In this study, the level of functional disability (in both personal activities and social participation) was higher in groups with poor muscle strength, depression, and cognitive decline. Therefore, an integrated functional improvement approach to prevent disabilities in personal and social functioning is needed for older adults living alone with fall experience.
In particular, poor muscle strength was observed to be related to FSP in a long-term study conducted on 906 elderly people in the community for 4.9 years (Buchman et al., 2009). Since poor muscle strength is a risk factor for falls, interventions to improve muscle strength are needed to prevent the recurrence of falls (Ambrose et al., 2013). Further research is required to examine the effect of muscle strength training on enhancing the social participation of elderly people living alone, who have experienced falls. In addition, the results of this study are similar to those of previous studies, which found that the psychological function of depression could cause FSP (Cai et al., 2019; Croezen et al., 2015; Liu, 2017). Fu et al. (2018) reported a correlation between cognitive function and social participation in older adults. Older adults living alone were reported to be more depressed than those living with family members (Stahl et al., 2017). It is thus essential to focus on the comprehensive management of multidimensional functions to decrease functional disability and promote optimal performance of older adults living alone with fall experience.
One of the strengths of this study is its large sample size. Functional disability was comprehensively explained and included not only in terms of the personal aspects but also its social aspects. In addition, the findings of this study may help improve interventions that prevent long-term care facility admissions for older adults living alone due to functional disability after falling, thereby reducing medical expenses and the burden of caregiving. However, this study had certain limitations. First, since this study was conducted using a cross-sectional design and secondary data, it does not explain causal relationships, and the findings cannot be generalized to a larger population. Second, although no statistically significant difference in FSP with regard to other personal factors such as health conditions and smoking was found in this study, further research is necessary to examine disability in social functioning among older participants in diverse settings and cultures. Third, the study variables included various dimensions (physical, psychological, and mental) and components (personal, environmental, health, and body functions) affecting functional disability in older adults living alone with fall experience. Other factors (e.g., fear of falling and anxiety) that may influence functional disability were not selected because the study was based on the ICF model, and examining other factors was beyond the scope of this study. Finally, the FSP was conceptualized and measured as a single structure after factor analysis. The findings provide useful clues for understanding the factors related to FSP, but warrant future studies, including longitudinal and clinical trials, to find ways to improve social participation among the older population.
Conclusion
This study aimed to investigate the factors influencing FSP among older adults living alone who experienced falls. For older adults living alone to maintain the remaining function of social participation for a long time despite the experience of falling, assessing and intervening with the identified influencing factors is essential. In particular, tailored interventions that reflect personal, environmental, and multifunctional factors are necessary to address individual needs. In order to improve the size and quality of social participation among the older adults living alone who experienced a fall, it is necessary not only to set up social resources for a tailored program, but also devise policies that increase the accessibility and usability of resources by the population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially funded by the Sigma Theta Tau International Honor Society of Nursing, Lamda Alpha Chapter-at-Large in 2020.
Ethical Approval
The 2017 National Survey of Older Koreans was approved by Statistics Korea (Approval No. 11771). With an approval of the Korea Institute for Health and Social Affairs, raw data without personal identification information was d for this study. The study was approved by the Institutional Review Board (IRB No.: E2008/001-004) of Seoul National University.