
Abstract
Home health aides provide care to homebound older adults and those with chronic conditions. Aides were less likely to receive COVID-19 vaccines when they became available. We examined aides’ perspectives towards COVID-19 vaccination. Qualitative interviews were conducted with 56 home health aides at a large not-for-profit home care agency in New York City. Results suggested that aides’ vaccination decisions were shaped by (1) information sources, beliefs, their health, and experiences providing care during COVID-19; (2) perceived susceptibility and severity of COVID-19; (3) perceived benefits of vaccination including protection from COVID-19, respect from colleagues and patients, and fulfillment of work-related requirements; (4) perceived barriers to vaccination including concerns about safety, efficacy, and side effects; and (5) cues to action including access to vaccination sites/appointments, vaccination mandates, question and answer sessions from trusted sources, and testimonials. Providing tailored information with support to address vaccination barriers could lead to improved vaccine uptake.
• This paper explores the perspectives of home health aides towards COVID-19 vaccination; aides were less likely to receive the COVID-19 vaccine when they first became available despite caring for older adults with chronic conditions. • Aides’ vaccination decisions were shaped by information gleaned from multiple sources, personal experiences and beliefs, perceived susceptibility and severity of COVID-19, benefits and barriers from/to vaccination, and ability to have questions about the vaccine answered by their employers and co-workers. • Aides carefully considered COVID-19 vaccines and based their decision-making on their own perceptions of, and experiences during the pandemic, as well as beliefs about vaccine safety and efficacy.
• Efforts to heighten awareness of COVID-19 risks and deliver information about the COVID-19 vaccine through trusted sources that address aides’ questions and concerns, may be warranted. • Home care agencies can serve as key access points for vaccination by operating centrally-located vaccination clinics and facilitating personalized outreach from agency representatives to answer aides’ questions about vaccines and schedule vaccination appointments.What this paper adds
Applications of study findings
Introduction
Home Health Aides (aides) provide essential services to community-dwelling persons living with functional difficulties and chronic illness, allowing them to safely remain at home and potentially avoid institutional settings. During the COVID-19 pandemic, aides provided hands-on personal care and assistance, as well as emotional support (Bandini et al., 2021; Sterling et al., 2020). Unlike many other healthcare workers who may have been able to work remotely, aides provided care to patients in their homes without being able to socially distance and often without adequate access to personal protective equipment (PPE) at the beginning of the pandemic (Markkanen et al., 2021). Doing so placed them at high risk for infection, and also posed challenges to their own financial, physical, and emotional well-being, exacerbating existing vulnerabilities among a workforce comprised largely of middle-aged women of color who earn low wages and often lack paid time off (Bandini et al., 2021; PHI, 2019; Pinto et al., 2022; Rowe et al., 2020; Scales, 2021; Sterling et al., 2020; Tyler et al., 2021; U.S. Bureau of Labor Statistics, 2021). Many patients with COVID-19 were cared for by aides, and many aides contracted COVID-19 (HCA Policy Team, 2020; Pinto et al., 2022; Sama et al., 2021). Additionally, many home-bound adults were fearful of receiving home care due to the infection risk, which translated into fewer cases and hours for aides and their agencies. These factors contributed to aides’ financial instability during the pandemic relative to other industries and healthcare workers (Bhandari et al., 2021; Sama et al., 2021).
In late 2020, the Food and Drug Administration authorized COVID-19 vaccines as an additional public health strategy to combat the pandemic. Yet the effectiveness of these vaccines is dependent on sufficient uptake by high-risk groups and the general public. Early allocation of COVID-19 vaccines prioritized those at highest risk, including older adults, healthcare workers, residents of long-term care facilities, and persons with chronic health conditions (Dooling et al., 2020, 2021). While vaccination rates among some prioritized groups have been high, others have lagged, including aides. A March 2021 survey found that 26% of home care workers received at least one dose of a COVID-19 vaccine compared to 52% of all frontline healthcare workers, and that one in four home care workers reported they did not plan on receiving a COVID-19 vaccine (Kirzinger et al., 2021). Several factors may drive COVID-19 vaccine acceptance among healthcare workers, including level of education, degree of patient contact, perceived risk of COVID-19 infection, and adherence to infection prevention and control practices (Angelo et al., 2021; Green-McKenzie et al., 2021; Li et al., 2021). Additionally, organizational and policy factors may be at play. Home care agencies, which tend to be smaller and decentralized, may face logistic challenges with acquiring and administering vaccines in their workforce and patient populations (Mohammad et al., 2021). And, while vaccination mandates, such as the one in New York State, hastened the decision-making process for many aides, these policy decisions did not address aides’ personal experiences, beliefs, and unanswered questions about vaccines, potentially leading aides to exit their jobs and worsening an existing workforce shortage (Governor’s Press Office, 2021; Otterman, 2021).
The role of aides in caring for an older and chronically ill population, combined with their lower initial vaccine acceptance compared with other healthcare workers, underscores the need for an investigation into their perspectives towards COVID-19 vaccination. While prior research has explored the attitudes and willingness of staff in nursing facilities to receive a COVID-19 vaccine, there are currently no studies exploring these issues among aides (Harrison et al., 2021; Unroe et al., 2021). This gap is concerning given that vaccination would shield aides and their vulnerable clients from the worst consequences of COVID-19. This study explores the perspectives of aides towards COVID-19 vaccination. Findings can inform workforce safety and ongoing pandemic preparedness efforts.
Methods
Setting and Study Population
This qualitative study was conducted at VNS Health, one of the largest not-for-profit home health organizations in the U.S. In 2020, VNS Health employed 8839 aides who provided more than 43 million hours of home care to adults with chronic conditions and functional limitations in all five boroughs of New York City. Eligible participants included aides who were (1) currently employed; (2) actively caring for clients; and (3) English or Spanish-speaking. Purposive sampling methods were used to recruit vaccinated and unvaccinated aides by contacting those who indicated their interest in participating in research on an earlier survey about their experiences during COVID-19, and by broadcasting announcements about the research to aides via email and text message. At the time of this study, being fully vaccinated meant having received a complete dose of the COVID-19 vaccine.
Data Collection
Four researchers (DR, ML, SV, MM) trained in qualitative research conducted telephone interviews in English or Spanish using a semi-structured topic guide informed by the Health Belief Model (Supplemental Table 1) (Janz & Becker, 1984; Maiman & Becker, 1974). Interviews were conducted between June 15 and October 19 2021. COVID-19 vaccines were widely available during this time and an announcement was made by the New York State Governor on August 16 that mandated vaccination for healthcare workers by October 7 2021. Two researchers (DR, MRS) developed interview questions focusing on (1) perceived risk and susceptibility to COVID-19, (2) perceived benefits of the COVID-19 vaccine, (3) barriers to receiving the COVID-19 vaccine, and 4) facilitators to receiving the COVID-19 vaccine. Demographic and employment characteristics of participants were collected. All participants provided verbal consent and received $25. Study protocols were approved by the VNS Health Institutional Review Board. This manuscript adheres to the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist (Supplemental Table 2) (Tong et al., 2007).
Data Analysis
Interviews were audio recorded and transcribed. Transcripts were uploaded to Dedoose for analysis (Dedoose, n.d.) A thematic analysis was conducted that allowed for flexibility in both pre-established codes from the Health Belief Model, and unique concepts/themes, to emerge from the data (Guest et al., 2011). Five researchers were involved in the analysis (DR, MRS, NO, MM, AS). The researchers began by reviewing six transcripts and applying a combination of in vivo and predefined codes from the Health Belief Model. These codes were refined through discussions during team meetings about content and parsimony, including by grouping similar codes into categories. This refined coding framework was then applied to all interview transcripts. Codes and excerpts were reviewed to identify emergent themes that captured patterns, connections, and distinctions in the data. Descriptive statistics were used to characterize the sample.
Results
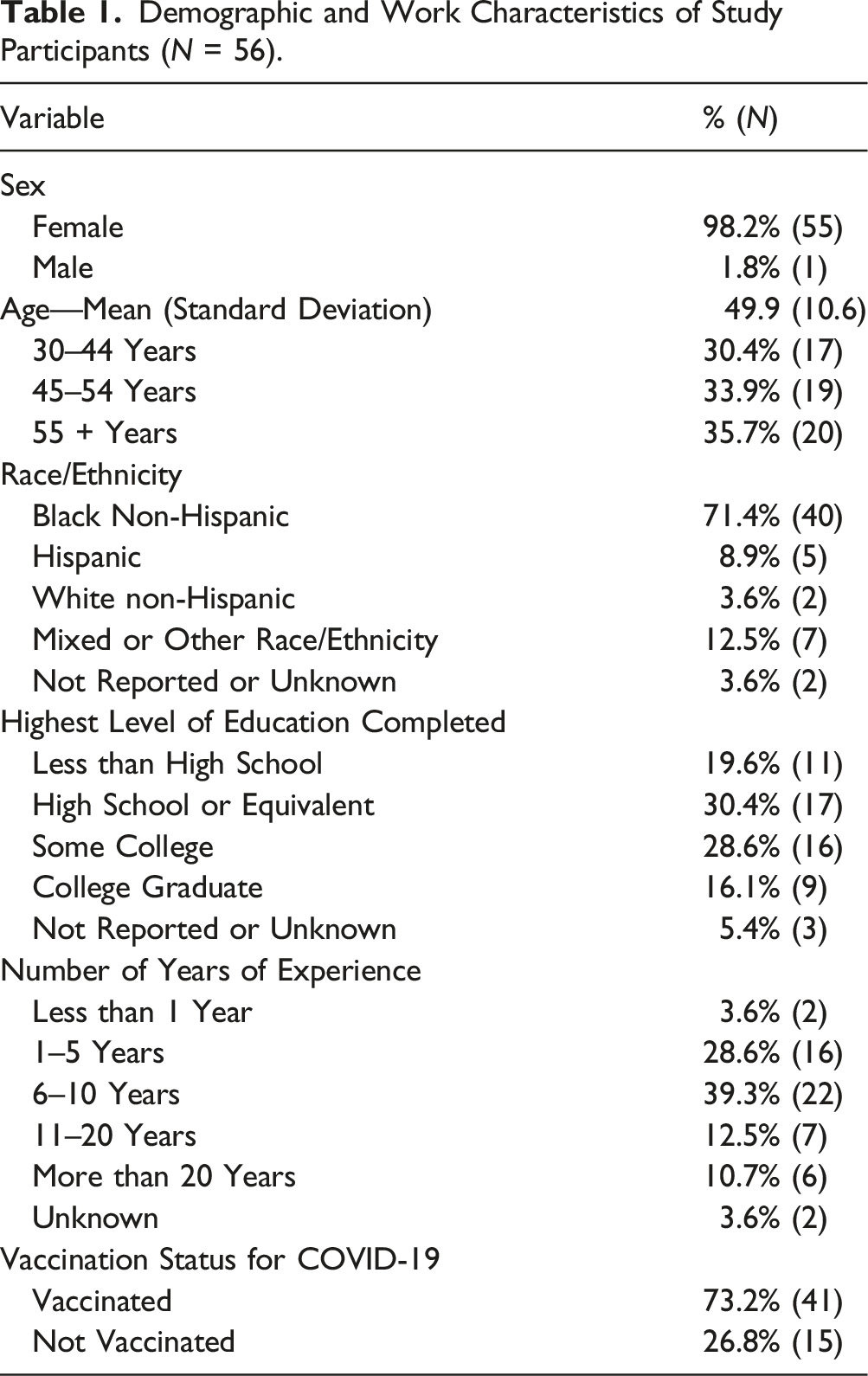
Demographic and Work Characteristics of Study Participants (N = 56).
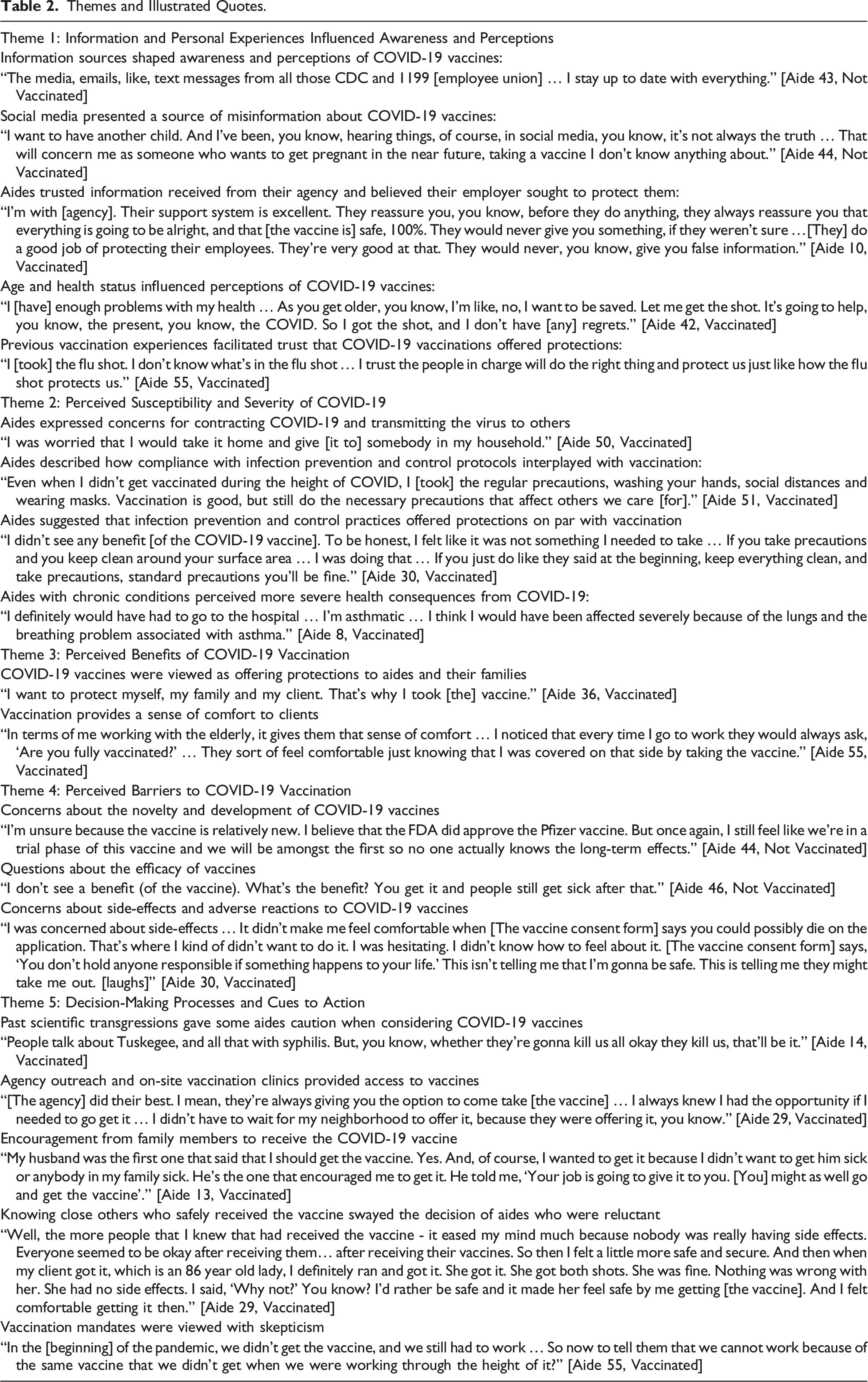
Five themes emerged. Figure 1 demonstrates how these themes fit into the Health Belief Model. Briefly, aides’ decisions about COVID-19 vaccination were shaped by (1) information and personal experiences throughout the pandemic; (2) perceived susceptibility to and severity of COVID-19; (3) perceived benefits of vaccination; (4) perceived barriers to vaccination; and (5) cues to action. Of note, although our sample included aides with different vaccination statuses, we analyzed the data collectively. Table 2 displays Illustrative quotes related to each theme. Conceptual model. Themes and Illustrated Quotes.
Theme 1: Information and Personal Experiences Influenced Awareness and Perceptions
Aides’ awareness and perceptions of COVID-19 and vaccines were influenced by information received, their personal health, and experiences caring for (or having a relationship with) someone who became sick from COVID-19. Aides gleaned information from a variety of sources, including agencies and unions, television, public health organizations, internet and social media, family members, and coworkers. Information gathered from these sources, however, varied in their accuracy. Aides acknowledged that social media could spread misinformation that impacted their vaccine attitudes. Sensational stories shared on social media highlighting deaths among people who received COVID-19 vaccines, false reports linking vaccines to infertility, and FDA statements issued about blood clotting conditions associated with one vaccine, prompted concerns and were hard for some aides to ignore, especially those who were unvaccinated, or who were reluctant about vaccination. Conversely, information gathered from other sources fostered trust among aides, including news about vaccine effectiveness and protections, as well as educational videos and text notifications from their agencies about vaccines, vaccine availability, and appointment scheduling. Aides assigned a greater weight to vaccine information received from their agencies based on a belief that their employer sought to protect them and assure their safety.
Perceptions of COVID-19 were also shaped by aides’ age, health status, personal experiences, and cultural values during the pandemic. Aides who were older and had underlying health conditions such as hypertension, asthma, or diabetes expressed motivation to be vaccinated based on a desire to protect their health. Aides who cared for patients with COVID-19, or who lost family and friends to the virus, had a heightened awareness of the pandemic and its life-altering consequences. Aides’ beliefs about or experience with government entities, employers, healthcare and pharmaceutical organizations, and previous vaccinations also shaped their beliefs about COVID-19 vaccines. Some of these experiences fostered concerns about the vaccination process, whereas for others, trust.
Theme 2: Perceived Susceptibility and Severity of COVID-19
Aides’ attitudes towards vaccination were shaped in large part by their perceived susceptibility to COVID-19 and the potential severity of illness for themselves and others close to them. Aides acknowledged that their job placed them at a heightened risk of infection by way of limited social distancing and greater reliance on public transportation. Additionally, the severity of COVID-19, and its variants, contributed to anxiety among aides that they or their loved ones could become sick.
Aides’ perceived susceptibility to COVID-19 was shaped by their engagement in infection prevention and control practices (e.g. social distancing, wearing masks, washing hands). Aides who described regularly following infection prevention and control practices viewed themselves as less susceptible to COVID-19. These practices were regarded as an important component of safety and were seen as a part of their work responsibilities, regardless of vaccine availability or their vaccination status. Many aides saw infection prevention and control practices as an additional layer of protection against COVID-19. Indeed, some aides questioned the necessity of vaccination in the context of routine testing, training, and compliance with infection prevention and control protocols. Aides underscored that vaccination was not a sufficient substitute for following infection prevention and control practices. Some unvaccinated aides expressed cultural beliefs that their susceptibility to COVID-19 was reduced through herbal medicine practices, and that these practices offered similar protections as vaccines, including a strengthened immune system to ward off infection.
Aides acknowledged that even those who were “healthy” could become very sick if they were to become infected. Others with chronic conditions such as asthma noted they would likely have severe symptoms and need to be hospitalized, which worried them.
Theme 3: Perceived Benefits of COVID-19 Vaccination
Several benefits of COVID-19 vaccination were noted by aides who received a COVID-19 vaccine, including decreased risk of infection, hospitalization, and virus transmission. These perceived protections provided aides with a sense of relief and assurance that they took steps to protect their own health and that of others (i.e., clients, family) against future variants and case surges of COVID-19. Aides also noted social and work-related benefits of vaccination, including the approval and comfort of their clients who preferred to receive services from aides who were vaccinated. Aides viewed vaccination as providing a path for returning to a sense of normalcy and pre-pandemic life. The perspectives of unvaccinated aides differed notably from vaccinated aides on this theme: unvaccinated aides saw fewer (or no) benefits of vaccination and emphasized that even with vaccination, someone could still become infected and sick with COVID-19.
Theme 4: Perceived Barriers to COVID-19 Vaccination
Barriers to vaccination described by aides included concerns about the novelty of vaccines and the speed with which they were developed. Aides questioned whether early adoptees were unknowingly participating in an experiment to test vaccine effectiveness and they did not want to be part of such a process.
Aides questioned the efficacy of COVID-19 vaccines, especially when hearing of vaccinated persons becoming infected. Their questions about vaccine efficacy were also related to new variants, and to recommendations for subsequent “booster” shots to maintain protection. Aides also expressed concerns about side-effects and reactions to COVID-19 vaccines, and they raised questions about the risks vaccines posed to their bodies and overall health, including sickness, allergies, blood clots, and even death. Unvaccinated aides emphasized their concerns about vaccine side-effects and the potential for long-term health consequences associated with vaccination. While vaccinated aides expressed similar concerns, these were outweighed by fears of COVID-19 infection among themselves, family, or their clients, and their trust in governmental agencies and employers to ensure vaccine safety.
Theme 5: Decision-Making Processes and Cues to Action
Aides heavily weighed the decision to get vaccinated, considering perceived benefits, barriers, and risks. Notably, aides’ decisions were shaped by how their concerns and questions about vaccines were being taken seriously and answered by their agency and other sources. Advice from trusted sources, such as their employer(s) and the CDC, played an important role in aides’ vaccination decision. While some aides expressed trust in medical professionals and government officials, others noted how past scientific transgressions such as the Tuskegee Syphilis study gave them caution when considering vaccines.
Several factors served as cues to action among aides that were weighing the decision to get vaccinated. These included trust and approval from clients, participation in support groups with other aides, direct and recurrent outreach from agencies to answer aides’ questions about vaccines, the option to schedule appointments at an on-site agency vaccination clinic, recommendations from co-workers, encouragement from family members, and state vaccination mandates. Among vaccinated aides who initially expressed reluctance towards receiving a COVID-19 vaccine, their decisions were swayed by advice from doctors and medical professionals, as well as by gathering additional information about vaccine side effects and knowing close others who safely received the vaccine (e.g., family members, clients). Vaccine mandates and financial incentives to become vaccinated were viewed with skepticism by aides
Discussion
This study explored the perspectives of home health aides toward COVID-19 vaccination. While aides were among the prioritized groups for early access to vaccines, vaccination rates for this workforce lagged behind that of other healthcare workers early in the pandemic (Kirzinger et al., 2021). Our findings suggest that aides’ attitudes towards COVID-19 vaccination were shaped by information from multiple sources, their health and experiences working during the pandemic, perceptions of their own susceptibility to the virus, and the severity of potential illness. Aides identified the perceived benefits of, and barriers to, vaccination, and acknowledged that certain factors, such as access to vaccination sites, testimonials from colleagues, and impending mandates, motivated them to get vaccinated or not.
This study builds on existing research that examines the perspectives of paraprofessional healthcare workers towards COVID-19 vaccines, which is important given their historically lower vaccination rates compared to other healthcare workers (Centers for Disease Control and Prevention, National Center for Immunization and Respiratory Diseases (NCIRD), 2021; Lee et al., 2021). Similar to studies of healthcare assistants in nursing homes (Niznik et al., 2022; Unroe et al., 2021), we found that aides’ confidence in the safety and effectiveness of COVID-19 vaccines were influenced by their concerns about their rapid development, experimental testing, and potential for causing unwanted side-effects or long-term health consequences. Aides expressed caution towards novel medical research and interventions, including COVID-19 vaccines, which may be shaped by historical abuses and a broader mistrust of medical care (Brandon et al., 2005).
Many aides whom we interviewed, however, embraced vaccination and described how their motivation to protect their own health, and the health of their clients and family members, outweighed any potential risks involved with receiving a vaccine. Indeed, consistent with the Health Belief Model (Zampetakis & Melas, 2021), aides who viewed themselves as being at greater risk of infection or having more severe clinical consequences from COVID-19 viewed vaccines as instrumental in reducing their relative infection risk and illness severity. Interestingly, and perhaps unique to home care, aides viewed vaccination as facilitating trust and approval with their clients and peers. Aides’ motivations to increase their protection of self and others were heavily driven by their work on the frontlines of the COVID-19 pandemic, a context in which aides and their clients were highly vulnerable to infection (Sterling et al., 2020).
Aides received vaccine information and recommendations from multiple sources, including public health guidance, social media, doctors, clients, work colleagues, family, friends, and religious institutions. This finding is consistent with work by Niznik and colleagues, who found that healthcare providers were cited most often as a trusted source of vaccine information for healthcare assistants (Niznik et al., 2022).
Our findings have implications for efforts by agencies, governments, and other organizations to improve vaccination intention and receipt among home care workers. Most notable were the mixed perceptions of aides towards vaccination mandates. Although vaccination mandates were applied early and broadly to the healthcare workforce by the Biden administration, many aides initially occupied a gray area due to the majority working as independent providers, or for agencies with fewer than 100 employees (Campbell et al., 2021; PHI, 2019). Additionally, many aides are employed by agencies funded by Medicaid, which provided states with the authority to impose mandate (PHI, 2019). In New York State, for example, a vaccine mandate was applied to home care workers such that if they did not receive a first dose of the vaccine by October 7, 2021, they would lose their job (Otterman, 2021). Like hospitals and nursing homes, home care agencies and unions were left to navigate this, often weighing the benefits of a vaccinated workforce against an exacerbated workforce shortage. Our findings suggest that aides were resentful of vaccination mandates and financial incentives, explaining that they had worked tirelessly during the pandemic without adequate personal protective equipment, a vaccine, or acknowledgment from the healthcare industry or society at large. Beyond mandates, towards the end of the study period, vaccinated aides began to express reluctance towards receiving “booster” doses of vaccines suggesting the need for ongoing messaging and outreach to aides, even those who met the mandate requirement. Our findings, particularly on the influence of peers and agency-led question and answer sessions on vaccine decision making, underscore that these strategies warrant further attention as the pandemic continues. Beyond opportunities to discuss the vaccine with peers and staff, we found that agencies themselves may serve as key access points for vaccination, a strategy that also warrants further study. Much like frontline hospital employees who were vaccinated at their worksite, the aides in our study also had the opportunity to receive a COVID-19 vaccine through an on-site clinic that operated from January through March of 2021 (Update: VNSNY Frontline Workers Receive the COVID-19 Vaccine, 2021). This on-site and centrally-located vaccination clinic played an important role in reducing barriers to vaccination and increasing equity in vaccine awareness by virtue of personalized outreach from agency representatives who could answer aides’ questions about vaccines and schedule vaccination appointments.
Strengths and Limitations
Strengths of this study included the use of purposive sampling to recruit a diverse group of aides who were vaccinated for COVID-19 and those who were not. For example, a greater share of aides in our study were female (98% vs. 89%) and Black or African American (71% vs. 28%) compared to national profiles of home care workers (PHI, 2019). Recent research has highlighted cultural and cross-national group differences in vaccine intentions and the psychological consequences of receiving COVID-19 vaccines (Bergman et al., 2022; Stojanovic et al., 2021). While our interview sample included both Hispanic, non-Hispanic, and mixed racial/ethnic participants, we did not identify ethnic differences in aides’ perspectives towards vaccination. However, the number of Hispanic aides in our interview sample (n = 5) may not be sufficient to properly examine racial and ethnic differences in perspectives towards the COVID-19 vaccines. Further research is needed to explore how cultural values and ethnicity shape COVID-19 vaccination perspectives. Additionally, data were analyzed using a rigorous approach and an established conceptual framework. However, we note a few limitations. First, because this was a qualitative study at a single agency, findings may not reflect the experiences of aides employed at different agencies or suburban or rural locations. Second, this study does not include the perspectives of the home care agency leadership or other stakeholders; future research should elicit these perspectives. Third, although we recruited sufficient numbers of vaccinated and unvaccinated aides to reach saturation, future studies may benefit from focusing on unvaccinated aides who are not subject to vaccine mandates.
In conclusion, this qualitative study of HHA perspectives towards COVID-19 vaccines identified key themes in their beliefs and attitudes about vaccination. The aides we interviewed carefully considered COVID-19 vaccines as part of a complex process in which they gathered information from multiple sources, considered advice and recommendations from family and work colleagues, and weighed their vaccination decision based on perceived benefits and disadvantages. Delivering tailored information to aides about vaccination through trusted sources that address aides’ concerns may be warranted. Workforce-level policy changes, including enhanced training and stronger supervisory support, could also play an important role in laying a foundation for future vaccination initiatives among aides.
Supplemental Material
Supplemental Material - A Qualitative Study of Home Health Aides’ Perspectives towards COVID-19 Vaccination
Supplemental Material for A Qualitative Study of Home Health Aides’ Perspectives towards COVID-19 Vaccination by David Russell, Nicole Onorato, Alexis Stern, Sasha Vergez, Mia Oberlink, Matthew Luebke, Penny H. Feldman, Margaret V. McDonald, and Madeline R. Sterling in Journal of Applied Gerontology
Supplemental Material
Supplemental Material - A Qualitative Study of Home Health Aides’ Perspectives towards COVID-19 Vaccination
Supplemental Material for A Qualitative Study of Home Health Aides’ Perspectives towards COVID-19 Vaccination by David Russell, Nicole Onorato, Alexis Stern, Sasha Vergez, Mia Oberlink, Matthew Luebke, Penny H. Feldman, Margaret V. McDonald, and Madeline R. Sterling in Journal of Applied Gerontology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the Altman Foundation.
Institutional Review Board
All study protocols described in this article were approved by the Institutional Review Board of the Visiting Nurse Service of New York (Reference Number: I21-003)
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.