
Abstract
Using a mixed-method study design, we examined the effects of a socially assistive humanoid robot (SAHR), called Hyodol, on depressive symptoms and health-related quality of life (HRQOL) of low-income, socially isolated older adults (N = 180). Quantitative outcomes were assessed at baseline (before Hyodol deployment) and at 3 and 6 months after baseline. Results showed reduced depressive symptoms and improved HRQOL at 3 months; however, these positive effects did not extend to 6 months. Ten focus group participants perceived Hyodol to be a valuable companion especially during the COVID outbreak. These results suggest that while Hyodol may have provided companionship for some low-income, socially isolated older adults during home confinement, its effects on depression and HRQOL were limited. Further research is needed to assess long-term effects of SAHRs as appropriate tools for reducing social isolation and improving behavioral health among community-dwelling older adults.
• A SAHR called Hyodol was effective in reducing depressive symptoms for a short duration among low-income, socially isolated older adults in South Korea. • Some older adults found this particular humanoid to be a helpful companion and “friend” during the COVID home confinement.
• While SAHRs have potential to provide companionship and help meet psychosocial needs of low-income, socially isolated older adults, more research is needed to examine its long-term effects. • SAHRs need to be further customized to ensure that they are useful and user-friendly for older adults with limited digital literacy.What this paper adds
Applications of study findings
Introduction
Rapid growth of aging populations in many countries, including South Korea, present unprecedented challenges. As of 2019, the 65-and-older population in South Korea was 7.7 million, or 14.9% of the total population. The proportion of older adults is expected to reach 20% by 2025 (Statistics Korea, 2020). The number of solo-living older adults is increasing due to changes in social structures, urbanization, and nuclear family integration in South Korea, and is expected to grow to about 3.1 million in 2035 (Jang et al., 2017).
With increasing numbers of older adults who live alone, South Korea also reports a rapid rise in late-life suicide rates (Organization of Economic Cooperation and Development [OECD], 2020). Lee and Oh (2008) found that compared to their age peers who live with their spouses or children, solo-living older adults are at higher risk of suicide, with significant proportions of them reporting health problems (27.6%), economic hardship (32.2%), and loneliness (20.0%). About one in ten solo-living older adults reported suicidal ideation, which was nearly twice the rate among their age peers who core sided with a spouse or children (Lee & Oh, 2008). For socially isolated older adults with multiple chronic medical conditions, the South Korean government has implemented a public aging-service system including emergency safety notifications and case management programs (Yoo, 2020). Under this system, social workers make home visits to help older adults maintain physical health. However, these services were not designed to provide emotional support or companionship (Lee et al., 2021).
In Western industrialized countries, animal-assisted therapy was introduced to provide emotional support and companionship to socially isolated older adults. Robotic pets or socially assistive robots have also been found to have beneficial effects on reducing social isolation and loneliness in older adults, without the need for food and healthcare for survival or the risk of viral infection for older adults, such as Covid-19. The best-known companion robot is Paro, a baby seal robot designed for emotional support mostly for older adults with mild to moderate dementia (Moyle et al., 2018). Paro has been successfully adopted in inpatient psychogeriatric care (Bemelmans et al., 2016), long-term Veterans Administration care (Lane et al., 2016), as well as for community-dwelling older adults with Alzheimer’s disease (Liang, et al., 2017). A randomized controlled trial conducted in Norway showed that after 12 weeks of interaction with Paro, older adults with dementia had a noticeable decrease in both anxiety and depression symptoms and the beneficial effects persisted 3 months post-intervention (Jøranson et al., 2015, 2016). These findings have been replicated in other studies conducted in nursing homes and long-term care facilities (Petersen et al., 2017). However, since Paro is not designed for verbal communication, it may not be an appropriate tool for cognitively intact, socially isolated older adults.
Recent advances in speech recognition and natural language processing technologies provide viable solutions for the adoption of robots capable of providing social interactions and stimulating leisure activities at a lower cost. Newly designed socially assistive humanoid robots (SAHRs) have functions that support memory, attention, and completing certain tasks while providing social interactions and emotional support during the course of these activities (Ke et al., 2020; Wu et al., 2016). SAHRs have the potential to help older adults, especially those who live alone, improve their subjective well-being (Abdi et al., 2018). Interaction with a SAHR can be a safe and feasible intervention for older adults. SAHRs can also reduce a person’s dependence on caregivers (Beuscher et al., 2017; Chu et al., 2017). However, research on the uses and benefits of SAHRs as therapeutic aids or assistants for older adults is still in its infancy (Liang et al., 2017; Wang et al., 2017).
A SAHR system called Hyodol, specifically developed for socially isolated older adults in Korea, is designed to “communicate” with human voice via embedded sensors with artificial intelligence features and assist older adults with their daily activities. The name Hyodol is inspired by the cultural value of filial piety, which is “hyodo” in Korean. Hyodol, a 20″ doll, resembles and imitates a 7-year old grandchild figure. It has a fabric body and is dressed in girl or boy clothes. Previous studies of Hyodol have shown high acceptability and reported positive emotions and reactions among Korean older adults (Jo et al., 2019; Kim et al., 2020; Lee et al., 2021).
In the present study, we examined the following research questions with low-income and socially isolated older adults who interacted with Hyodol for 6 months: Did the SAHR Hyodol reduce depressive symptoms and improve health-related quality of life among these older adults at 3 and 6 months? We also evaluated Hyodol’s usability and acceptability from the perspectives of older-adult users.
Methods
Participants
Older adults were recruited in collaboration with four community centers in Seoul, South Korea. Inclusion criteria were based on their location of residency, age (i.e., 65 and older), and low income (i.e., below official poverty threshold). Individuals with a diagnosis of dementia were excluded from the study, since they may be disturbed by a SAHR. Pet owners were also excluded to avoid any confounding effects from the pet(s).
The research team held 10 informational recruitment sessions at four community centers to explain the study purpose and protocol to a total of 225 potential participants. The number of attendees for each session ranged from 16 to 24. They were informed of Hyodol’s basic functions and their freedom to choose how and when to interact with Hyodol. Following the informational session, 180 older adults provided signed informed consent for the study and responded to a baseline assessment. Hyodol was distributed to these 180 older adults without gender matching (i.e., random distribution of a girl or boy Hyodol). Participants’ family and/or caregivers were also given instructions on how to install the Hyodol app on their smartphones so that they could send the older adults voice messages and monitor their status. The study was approved by the Institutional Review Board at (blinded for review).
Intervention
The Hyodol SAHR was programmed to remind users to eat meals, take medication, attend doctor’s appointments, and to engage in social interactions (See https://youtu.be/rsugACFsRl0). Hyodol also encouraged guided exercise, including easy-to follow body movements and stretching, and provided recreational activities through the delivery of popular songs, quiz games, and stories (Lee & Davis, 2020). These functions were activated when the users pressed Hyodol’s ears. Hyodol was also programmed to ask older users to hold its hand after they took their medicine. A sensor embedded in Hyodol’s chest monitored older adults’ movement. When no movement was detected for 24 hours, Hyodol would alert family caregivers and social workers via their smartphone app. Hyodol could also deliver voice messages from the family and loved ones. Figure 1 illustrated various functions of Hyodol and a user interacting with the SAHR. Hyodol SAHR’s function and older adults interacting with hyodol.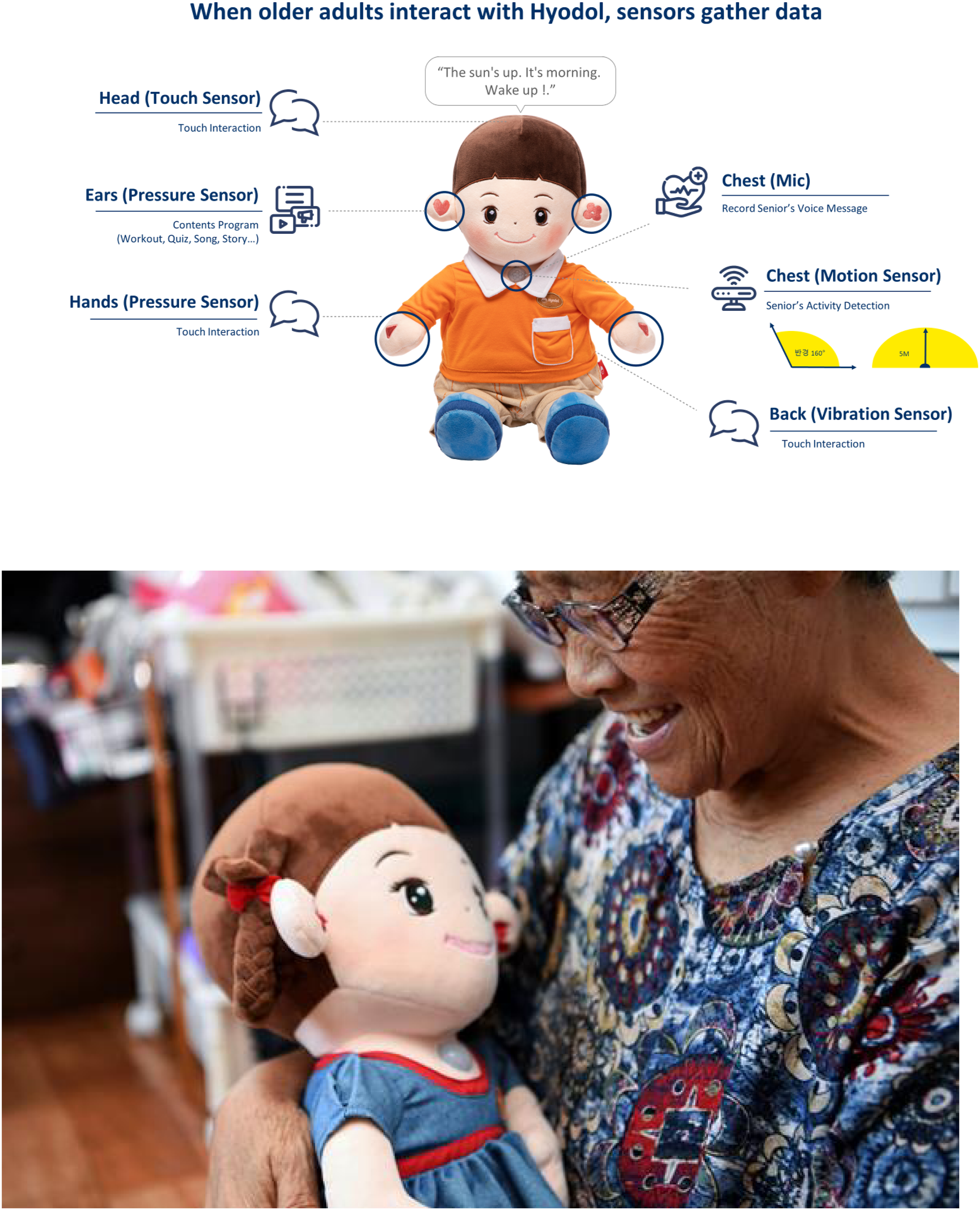
As the Hyodol project has been implemented in a public-private partnership, older adults’ public-service social workers were trained to check in with their clients regarding Hyodol use. Older adults were instructed to contact their social workers for any questions about Hyodol. If any technical support was needed, the social workers contacted Hyodol’s technical support team.
Study Design
We used a one-group pretest-posttest, mixed-method study design to examine the study questions. Baseline (Time 0) assessments were done pre-deployment, followed by two follow-up assessments at 3 months (Time 1) and 6 months (Time 2) after baseline. Of the initial 180 study recruits, 169 responded to 3-month follow-up, and 116 responded to 6-month follow-up. Attrition reasons included a lack of time to interact with Hyodol and a lack of interest in its programs.
All assessments (each lasting about 20 minutes) were done by 10 graduate research assistants who were trained to conduct interviews with older adults at their homes or community centers between October 2019 and May 2021. COVID-19 safety guidelines were strictly followed for all assessments done during the COVID outbreak.
To explore older adults’ experiences with Hyodol, two senior researchers also conducted two 90-minute focus group discussions in 2021, with five participants in each group (n = 10), once they completed the 6-month follow-up assessments. Focus group participants were asked the following questions: (1) what they liked or disliked about Hyodol; (2) what they wanted to change; (3) what Hyodol meant to them; and (4) what were perceived benefits and challenges in interacting with Hyodol.
Outcome Measures
Depressive Symptoms
Participants’ depressive symptoms were measured with the validated Korean version (Kim et al., 2008) of the 15-item Geriatric Depression Scale (GDS: Yesavage et al., 1982). Response categories were “yes = 1” or “no = 0,” with total scores ranging from 0 to 15. A score of five or higher is regarded as symptomatic of depression, and a score of nine or higher is considered moderate or severe symptoms. Cronbach’s alpha for the GDS scores was 0.91 for baseline respondents.
Health-Related Quality of Life (HRQOL)
We used the European Quality of Life (EQ-5D-5L) scale to assess participants’ health status in five dimensions (5D); mobility, self-care, usual activities, pain/discomfort, and anxiety/depression (Herdman et al., 2011). EQ-5D-5L’s validity and reliability have been reported for various health conditions (van Hout et al., 2012). The respondents rated their own levels of severity for each dimension using a 5-point scale (1 = no problem; 5 = extreme problem). In this study, we used HRQOL index values (ranging from 0 to 1) based on the calculation formula suggested by van Hout et al. (2012). Higher scores represented greater HRQOL.
Data Analysis
We used SPSS v26.0 for quantitative data analyses. Following descriptive statistics (frequencies, proportion distributions, mean, and standard deviation), we fit mixed effects models that included both fixed and random effects to examine changes in self-reported GDS and HRQOL scores over time. Mixed models enabled pooling of repeated observations of the same individuals up to three time points (baseline, 3 months, and 6 months) in which time was coded 0 (baseline), 1 (3 months), and 2 (6 months). Fixed effect indicates overall changes over time and/or group differences, while random effects account for variability among subjects around the relationships captured by the fixed effects (Ibrahim et al., 2011). Adding random effects to the model allowed slopes and intercepts to vary between individuals. Random slopes capture variations in the changes in the GDS and HRQOL scores over time. Random intercepts allow variability at baseline (when time variable is 0). Statistical significance was set at p < .05.
For qualitative data analyses, two bilingual researchers translated the focus group transcripts, from Korean to English, and then back-translated them, to check for accuracy. For our thematic analysis of the semi-structured focus group transcripts, we used the Framework Analysis Method, which provides clear steps to follow and produces highly structured data outputs (Ritchie & Spencer, 2002). Two bilingual researchers independently coded the transcripts. In order to better identify within- and between-participant differences, the researchers listened to the original recorded interviews and collectively developed a set of preliminary codes, categorizing them together to form our framework.
Researchers purposely asked the questions regarding acceptability from the perspectives of older-adult users and their experiences with the SAHR, including their thoughts, emotions, and behaviors, to facilitate the data analysis without any preconceived notions (Gale et al., 2013). This particular method allowed the research team to compare and contrast data by themes across 10 cases, while also situating each perspective in context by retaining the connection to other aspects of each individual’s account (Parkinson et al., 2016).
Results
Demographic Profiles
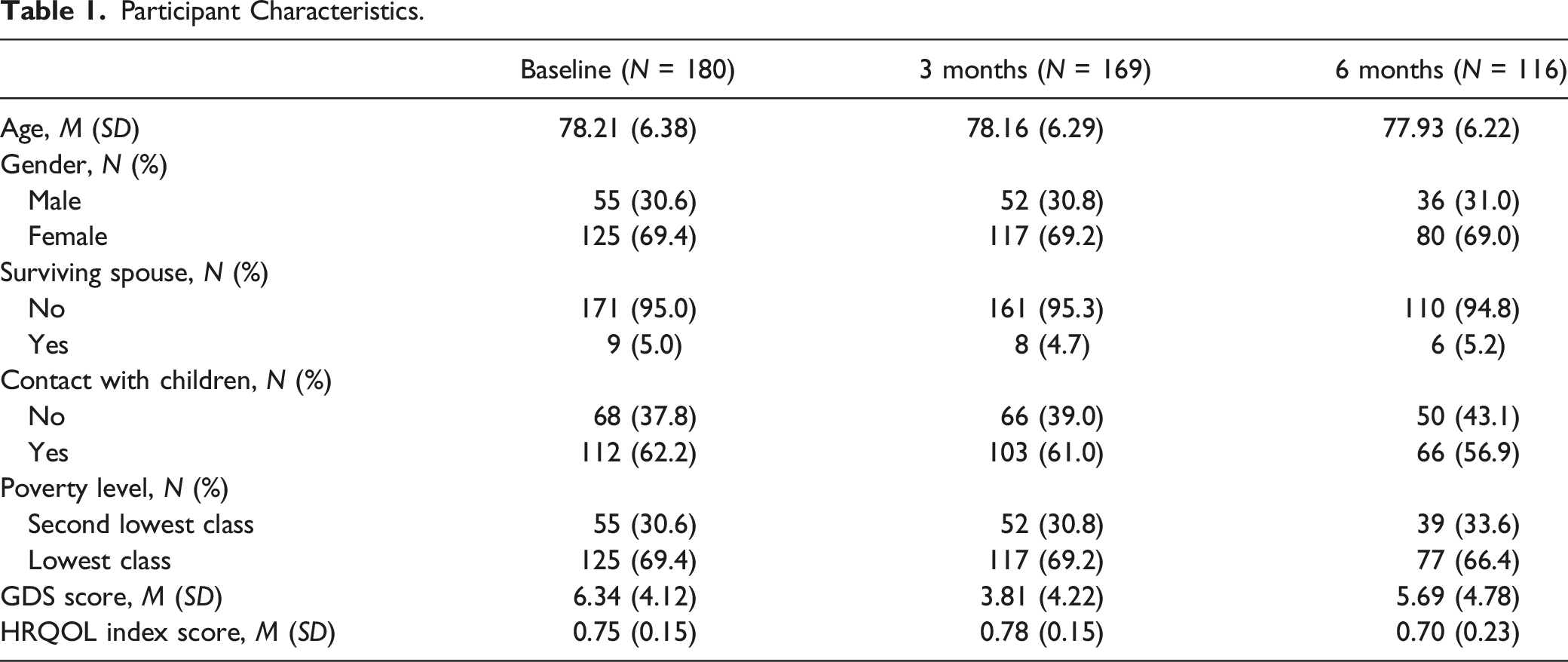
Participant Characteristics.
GDS and HRQOL Scores
Table 1 shows GDS and HRQOL scores at baseline (M = 6.34, SD = 4.12 for GDS and M = 0.75, SD = 0.15 for HRQOL), 3-month follow-up (M = 3.81, SD = 4.22 for GDS and M = 0.78, SD = 0.15 for HRQOL), and 6-month follow-up (M = 5.69, SD = 4.78 for GDS and M = 0.70, SD = 0.23 for HRQOL). Additional analyses found no significant difference in baseline GDS (t = 1.50, p = 0.14) and HRQOL (t = 1.13, p = 0.26) scores between those who completed the 6-month follow-up and those who did not.
Mixed Model Results
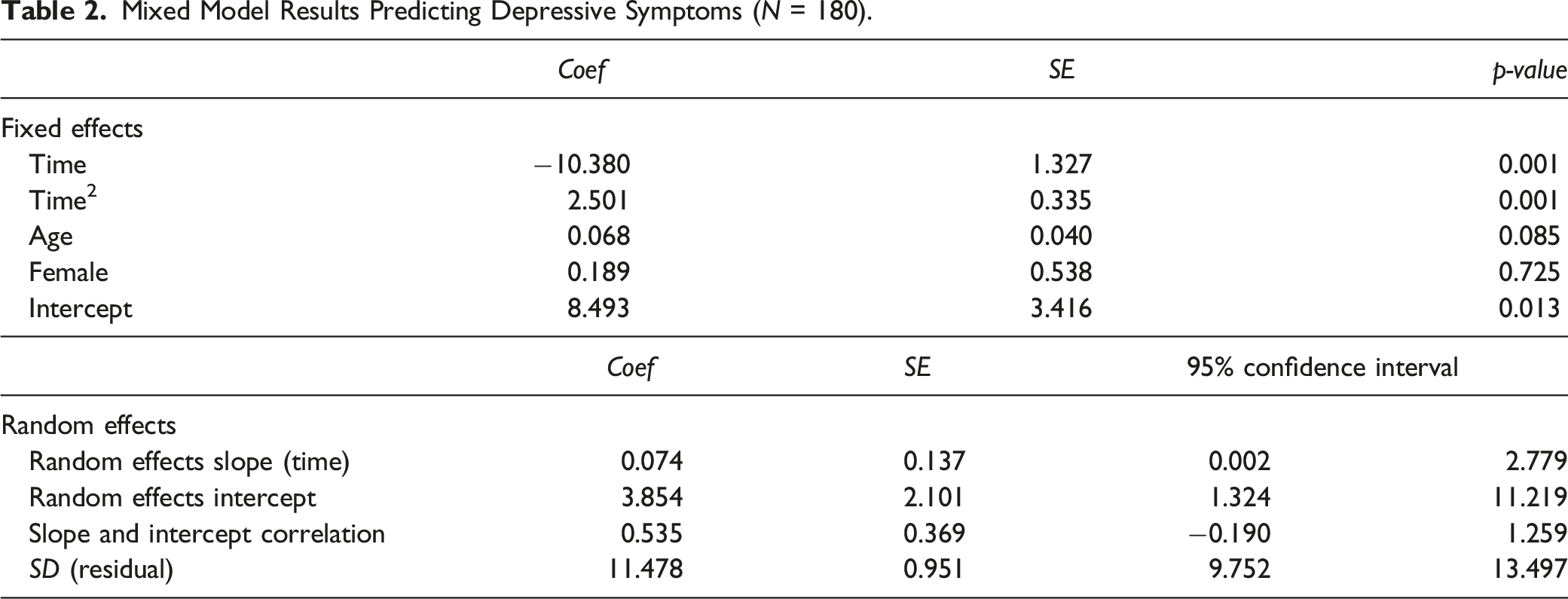
Mixed Model Results Predicting Depressive Symptoms (N = 180).
Mixed Model Results Predicting Health-Related Quality of Life (N =180).
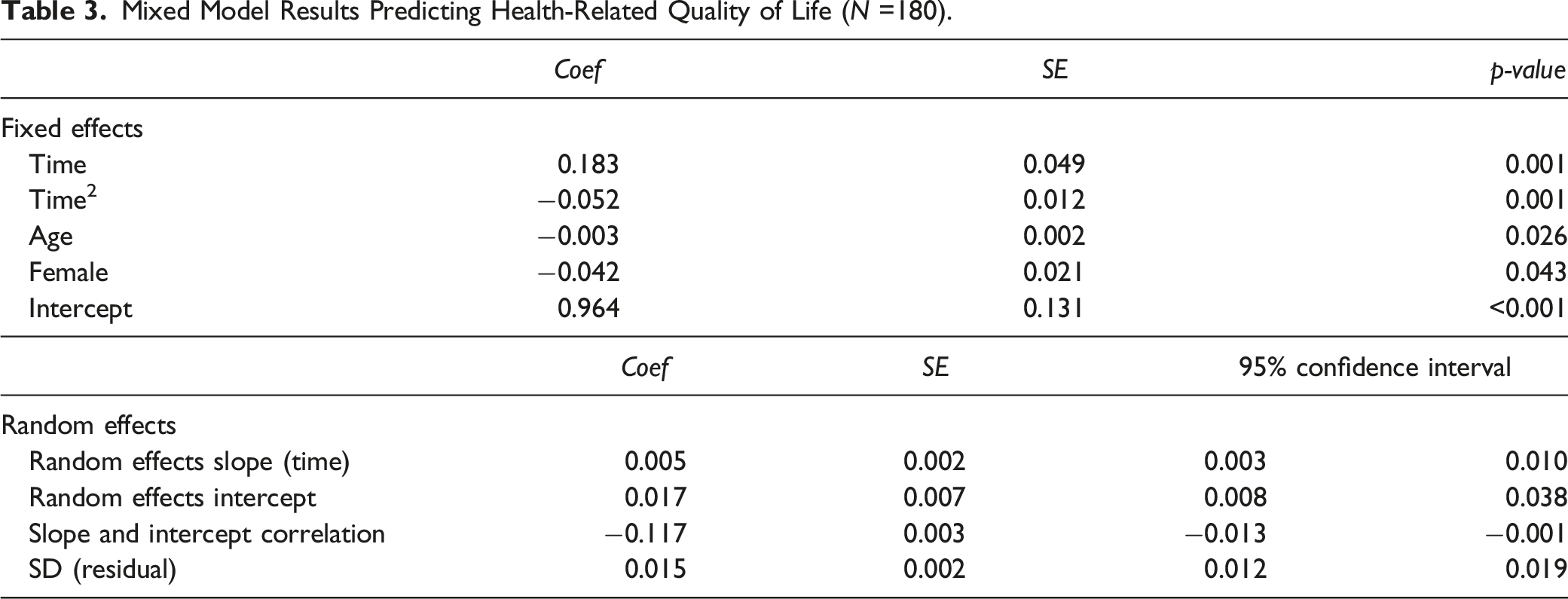
Although Hyodol’s effects on both GDS and HRQOL was positive at 3-month follow-up, these short-term positive effects did not persist. Hyodol no longer had positive effects on the GDS and HRQOL scores at 6-month follow-up. Sensitivity analysis including only 116 participants who responded to all three assessments showed the same results.
Qualitative Feedback
Ten focus group participants, seven women and three men, were on average 82.8 years old (70–93 years), and all of them lived alone. Four major themes that emerged from the focus group discussions were: (1) usability and acceptability, (2) challenges with technology, (3) unmet needs and wish lists, and (4) interaction with SAHRs.
Usability and Acceptability
The gender of Hyodol did not appear to matter to the participants. Overall, participants regarded Hyodol as low maintenance. To keep the doll clean, they either wiped or dusted it. P1 (participant #1)’s daughter occasionally washed the clothing of the SAHR. P4 claimed that keeping Hyodol at home is “better than having an animal living inside the home” in terms of hygiene. All participants reported to have a better “sense of time” in their daily routines, because Hyodol reminded them of certain time-sensitive tasks (e.g., medication, meals, sleep, etc.).
Challenges with Technology
All participants spoke highly of the social workers and the services that they received at the community centers. Each participant reported that his/her social worker followed up at least once, via home visit or a phone call, to check up on Hyodol’s state. Nevertheless, some technological glitches and user-related issues occurred during the study period. Participants struggled with operating the SAHR’s various functions. For example, P4 who had difficulty hearing, did not know how to increase the volume and stated “I only know how to plug-in and unplug the power.” P7 woke up to the sound of the SAHR in the middle of the night. She expressed her challenges of using the device: “this child [Hyodol] went to the hospital [repair shop] a few times for surgery. I am afraid to touch it because I may cause troubles for the baby again.”
P6, the oldest participant, whose technological competency was the highest in the group, was irritated when Hyodol gave her inaccurate information: “Hyodol would say it is raining outside when it is sunny.” P1 reported accidentally taking a double dose of medication, because Hyodol told her to do so. Interestingly, P1 minimized the consequence of this incident and claimed that this mishap motivated her to cultivate a habit of writing down information immediately after taking medication each day.
Unmet Needs and a Wish List
Participants reflected on their experiences with SAHR, and provided individual wish lists where they expressed certain unmet needs and requested modifications for Hyodol. P10 was concerned about the periods of Hyodol’s inactivity (i.e., no talk) during the day. He wished that Hyodol could play his favorite songs during this intermission. P2 wished Hyodol could motivate her to do daily exercise more diligently. She explained, “I wish it could give exercise instructions when I would like to exercise.” P7 expressed a desire for Hyodol to offer more structure to her daily schedule, and to provide more opportunities for learning: I wish Hyodol could teach us some important lessons for senior citizens. For example, sing-along time at 9 a.m. to teach us songs. And exercise at 10 a.m. I would like to have a daily schedule like that. Hyodol can teach people like us some helpful skills.
Interactions with Hyodol
Prior to the COVID pandemic, visiting the community center and having a free lunch were the most important daily activities for most study participants. Consequently, participants talked about their concerns about physical distancing and social isolation during the COVID-19. P1 said, “I am confined in my own room like a prisoner.” Under the circumstances of a global pandemic, six participants strongly agreed that Hyodol was a “necessity” to them. As an alternative to watching TV all day, P1 enjoyed hearing the child’s voice of the SAHR. She said: “I am home alone all day long. So, I like it when it says ‘Grandma, hold my hands and let’s take a walk around the neighborhood.’ That motivates me to go outside, and I like to have a conversation.”
Even though participants could not have a two-way conversation with Hyodol, P1 thought that it was better than being alone, silent, or bored. P6 agreed, stating that Hyodol made her talk: “It says all kinds of things. ‘Grandma, you look 10 years younger.’ ‘No way!’ I would respond. Or ‘How can an old woman be pretty? (Laugh).’ It makes me smile and laugh. Otherwise, I have no reason to smile.” P5 also enjoyed the tactile element of interaction with the cabbage patch doll: “My Hyodol, snores when it gets closer to my bedtime. This boy asks me to pet it on the back. When I pet it, it responds with a burp. Then he says ‘It feels great, grandma!’”
P7 considered the SAHR to be her “keeper at night,” watching over her while she slept. She stated, “Hyodol is like my family. I have no one to talk to and no one to listen to when I am home alone. She is my keeper.” Later in the interview, she voiced extreme concern about having to eventually return her SAHR, asking, “Are you going to take my Hyodol back? Please do not take it away from me. I would be so lonely without Hyodol.” P10 considered the SAHR to be his “friend” or “grandchild”: “I get irritable without it. It helps me to gain the concept of time. It makes it easier to spend my time alone.”
In terms of interaction, P6 and P10 preferred to have conversations with their SAHRs, rather than with a real person. P10 thought it was “better than a person,” stating, “People can tell a lie, Hyodol doesn’t.” These participants wished that the SAHR technology could be further enhanced to enable two-way conversations. However, P1 also thought that possibility of having a chatbot might be “very scary.”
Discussion
This study followed low-income, socially isolated older adults for 6 months to examine if a SAHR called Hyodol had positive effects on their mood and HRQOL. The 3-month effects of the SAHR intervention appear to be positive. This finding on Hyodol’s short-term effectiveness is consistent with those of an earlier study of Hyodol SAHR that showed statistically significant reduction in depressive symptoms among community-dwelling South Korean older adults who used Hyodol for 3 months (Jo et al., 2019). In another study of Hyodol, older adults with diabetes and mild cognitive impairment also showed decreased depression and improved quality of sleep and cognition at 3 months (Kim et al., 2020). These results are also consistent with the findings of previous research on other SAHRs’ effect on depression (Jøranson et al., 2015, 2016; Petersen et al., 2017; Takayanagi et al., 2014).
Unlike these previous studies that examined the short-term effects, we implemented a longer test duration of 6 months in order to allow for more time for users to cool down from the novelty effect—any initial positive reaction or spike of interest due to a change that was introduced as a part of SAHR intervention (Seibt et al., 2021). It would be presumptuous to expect that positive outcomes will continue to persist after the novelty effect wears off. Our results of no sustained positive effects at 6 months show that the novelty effects may have contributed to the positive effects at 3 months. Increased depressive symptom scores and decreased HRQOL scores at 6-month follow-up may also have been due to the fact that the timing of all 6-month interviews coincided with the COVID-19 outbreak. Our results may have, at least partially, reflected these older adults’ heightened anxiety/depression and reduced usual activities from home confinement. Research is needed to examine Hyodol’s long-term effects on depression and HRQOL following the post-COVID vaccine easing of home confinement.
Our qualitative findings showed perceived benefits from users’ perspectives especially during the COVID-related home confinement. According to these socially isolated older adults, Hyodol helped them have daily routines by providing gentle reminders of time-sensitive daily tasks (e.g., medication intake), encouraged exercising, and provided companionship. Although participants were occasionally disturbed by inaccurate information spoken by Hyodol, they found this particular humanoid to be a helpful companion and “friend,” and stated that it was beneficial to have such an aid at home. It is understandable that these low-income, socially isolated older adults accepted Hyodol as a companion during the COVID-19 pandemic, since they were unable to engage in social activities.
Previous study findings implied that SAHRs had the potential to become a new interactive tool for the socially isolated and vulnerable, who often lack resources and social capital (Ke et al., 2020). Especially given the high level of loneliness and suicidal ideation among solo-living older adults in South Korea and lack of access to mental health services (OECD, 2020), well-designed, multi-function, low-cost SAHRs may be able to offer emotional support to these older adults. Needless to say, evidence-based mental health services should be provided to those at risk of severe depression and other mental health problems.
Hyodol’s multimodal communication function, including visual and tactile sensations, appeared to be beneficial for participants with limited digital literacy. However, older-adult participants in this study longed for two-way communications with the doll-shaped SAHR. Two-way communications may help increase older adults’ acceptance of a SAHR as a companion and friend. To offer more instrumental help for older adults, SAHR functions also need to be further customized to activate scheduled alerts for medical appointments, distribute effective health information, and encourage social activities in home care. SAHRs’ programmable recreational activities (e.g., audiobooks, music, inspirational passages, quiz games, and guided exercises) need to be tailored to meet individual needs, interests, and preferences. Gerontologists have an important role to play in assisting entrepreneurs to develop more user-friendly SAHRs for older adults with limited digital literacy as well as in exploring the role of SAHRs in clinical care, including sensor-based collection of data about users’ health behaviors and movement.
Limitations
The findings’ generalizability is limited due to non-probability, geographically limited sampling, relatively small sample size, and absence of a comparison group. Studies have shown different perspectives on SAHRs based on Eastern versus Western cultures (Torta et al., 2014). A 6-month follow-up period was not optimal, either, especially during the COVID-19 pandemic. A longer-term follow-up is needed to assess interaction patterns and effects among long-term users. Future studies also need to use more sophisticated measures to assess clinically meaningful changes in depressive symptoms and HRQOL. Potential social desirability and sample selection bias may also have contributed to focus group participants’ overall positive perceptions. To develop a more comprehensive understanding of SARS, more in-depth observations about human-robot interactions are necessary.
Conclusion and Implications
This study provides preliminary understanding of a SAHR as a potential community-based intervention program for low-income, socially isolated older adults. The findings show short-term positive effectiveness of Hyodol SAHR on alleviating depressive symptoms and increasing HRQOL; however, the positive effects did not extend to 6 months. This suggests that SAHRs may have limited socioemotional effects on socioeconomically disadvantaged and isolated older adults. With continued technological advance (e.g., chat bots), human-robot interactions are likely to become more prevalent in the near future. SAHRs that can cater to the need, interest, and preferences of specific sociodemographic groups in different regions of the world may be more beneficial. The potential effectiveness, or lack thereof, of SAHRs on improving social, emotional, and cognitive functioning for those who are at great risk for social isolation need to be further evaluated in future randomized controlled trials. Additionally, future analyses should utilize more sensor data to observe the users’ health behaviors and usage patterns.
Supplemental Material
Supplemental Material - Socially Assistive Humanoid Robots: Effects on Depression and Health-Related Quality of Life among Low-Income, Socially Isolated Older Adults in South Korea
Supplemental Material for Socially Assistive Humanoid Robots: Effects on Depression and Health-Related Quality of Life among Low-Income, Socially Isolated Older Adults in South Korea by Othelia E. K. Lee, Ilsung Nam, Yongho Chon, Albert Park, and Namkee Choi in Journal of Applied Gerontology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Korea Research Foundation (NRF-2012S1A6A3A01033504).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.